
Abstract
Background
Patients undergoing surgical repair of penetrating cardiac injury are routinely evaluated postoperatively with a transthoracic echocardiogram (TTE). We hypothesized that patients undergoing a single operation for penetrating cardiac injuries without the need for cardiopulmonary bypass (CPB), coronary artery bypass grafting (CABG), or additional staged procedures do not benefit from routine postoperative TTEs.
Methods
A retrospective chart review of patients presenting with cardiac injuries to a level I trauma center from January 2018 to March 2025 was performed. Patients with a blunt mechanism, age <18 years, or no identifiable penetrating cardiac injury were excluded. Demographic data, injury characteristics, postoperative care and complications, and TTE findings were analyzed.
Results
Thirty-eight patients with penetrating cardiac injuries were identified. Twenty-one patients died within 4 hours of arrival, and 2 patients underwent advanced procedures (ie, CPB and CABG), leaving 15 patients for analysis. Thirteen (87%) were male with an average age of 36. The Median Injury Severity Score (ISS) was 26, with a median American Association for the Surgery of Trauma (AAST) heart injury grade of 3. Fourteen (93%) patients survived to discharge. Eight (53%) of the fifteen patients underwent postoperative TTEs, none of which revealed clinically significant findings relative to their procedure.
Discussion
Routine postoperative TTE demonstrated low clinical utility in this cohort. These findings support a selective approach to TTE based on injury complexity and clinical indicators. Postoperative TTE may be deferred in asymptomatic patients following uncomplicated repair but remains indicated in patients with new cardiac symptoms, higher-risk injury patterns, or complex operative repair.
Key Takeaways
• Routine use of postoperative TTE following surgical repair of penetrating cardiac injury may not be necessary in patients who do not undergo CPB, CABG, or staged procedures. • Multi-center studies may provide additional evidence, as well as other subsets of patients who do not benefit from routine imaging.
Introduction
Due to their high lethality, patients with penetrating cardiac injuries form a unique subset of trauma admissions. Such injuries account for 0.1% of all trauma admissions, with fewer than 10 cases expected annually at most institutions. 1 This is likely due to the fact that an estimated 94% of individuals with such injury die before reaching the hospital, often due to hemorrhagic shock or cardiac tamponade. 2 Additionally, 58% of those who make it to the hospital alive will likely die before discharge. 3 The few that successfully undergo surgical repair are routinely evaluated postoperatively with a transthoracic echocardiogram (TTE) to assess the adequacy of repair and potential additional injuries.
Transthoracic echocardiography is a non-invasive, bedside imaging tool with the ability to provide a real-time assessment of cardiac function, pericardial effusion, and extent of cardiac injury after trauma. However, its convenience may lead to overuse and unnecessary spending. A 2022 study based in Portland, Oregon, found that only 7.6% of TTEs recorded over 2.5 years in a surgical and trauma intensive care unit resulted in clinical management change. 4 Moreover, TTEs generate greater Medicare spending than any other cardiovascular imaging procedure. 5 Although the American College of Cardiology’s Appropriate Use Criteria successfully reduced inappropriate TTE ordering in certain cohorts, similar evidence-based guidelines do not exist for trauma or surgical patients. 4
Despite frequent usage, there is limited research regarding the utility of TTE within a trauma and surgical setting. More specifically, no studies to our knowledge have evaluated the role of routine postoperative TTE in the management of penetrating cardiac injuries. Rates of cardiac complications detected on postoperative echocardiography in these patients vary in the literature from 17% to 31%.6,7 These studies consist of heterogenous patient populations varying in injury severity, cardiac chamber involvement, operative complexity, and timing of performed echocardiogram. Because these factors can influence postoperative findings, differences in cohort composition may contribute to variability in clinically significant TTE findings. This study aims to identify which patients appear low risk for clinically significant postoperative TTE findings and which postoperative features may warrant mandatory imaging. We hypothesized that routine postoperative TTE provides limited clinical benefit after a single uncomplicated repair for penetrating cardiac injury without cardiopulmonary bypass (CPB), coronary artery bypass grafting (CABG), or additional staged procedures, supporting a selective, risk-stratified approach.
Methods
American Association for the Surgery of Trauma Cardiac Injury Scale 10
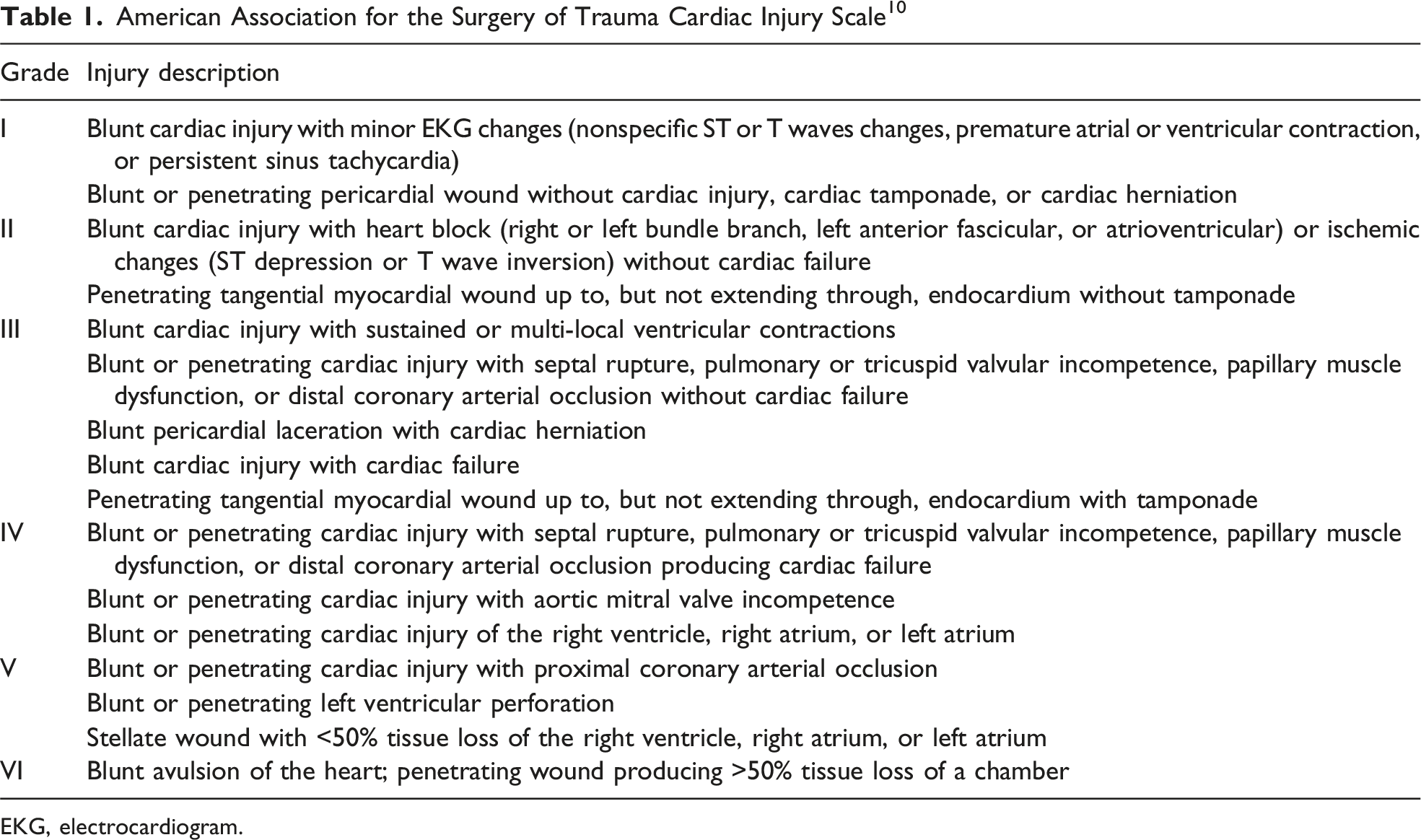
EKG, electrocardiogram.
Data analysis was performed using Microsoft Excel (Version 16.105.2, Microsoft Corporation). Patient age, length of ICU stay, and length of hospital stay were calculated and reported as a mean with standard deviations. Injury Severity Score and AAST grade were calculated and reported as a median with interquartile range. Categorical values were reported as a percentage. No statistical analysis was performed.
Results
General Demographics and Clinical Characteristics
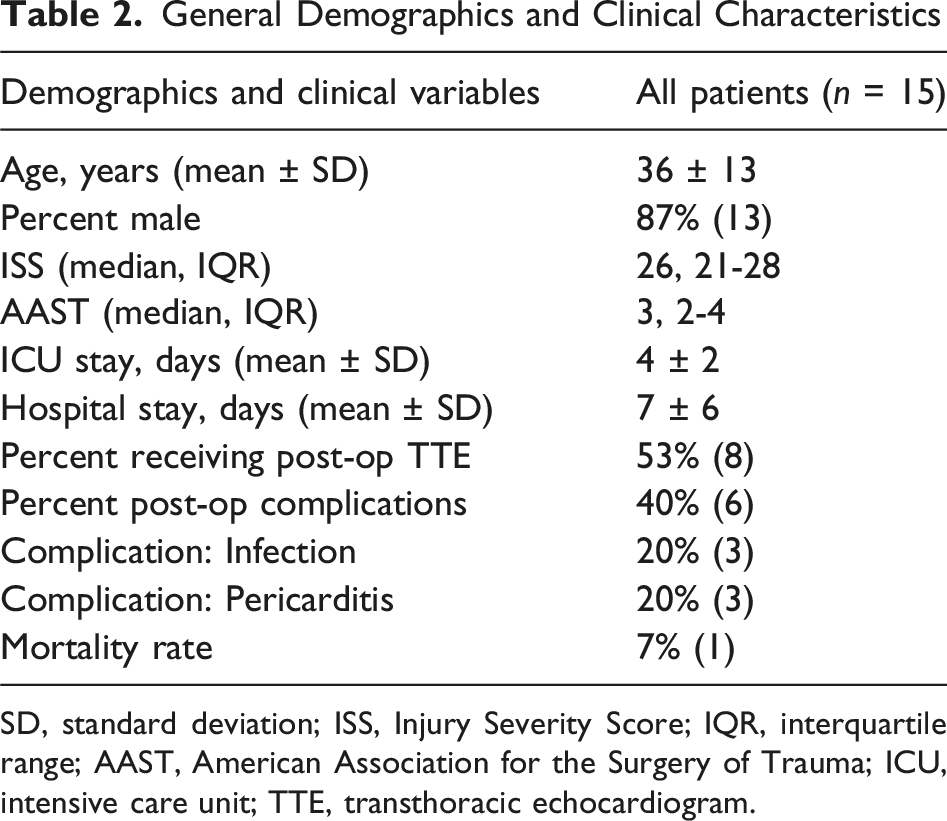
SD, standard deviation; ISS, Injury Severity Score; IQR, interquartile range; AAST, American Association for the Surgery of Trauma; ICU, intensive care unit; TTE, transthoracic echocardiogram.
Description of Patients With Penetrating Cardiac Injury
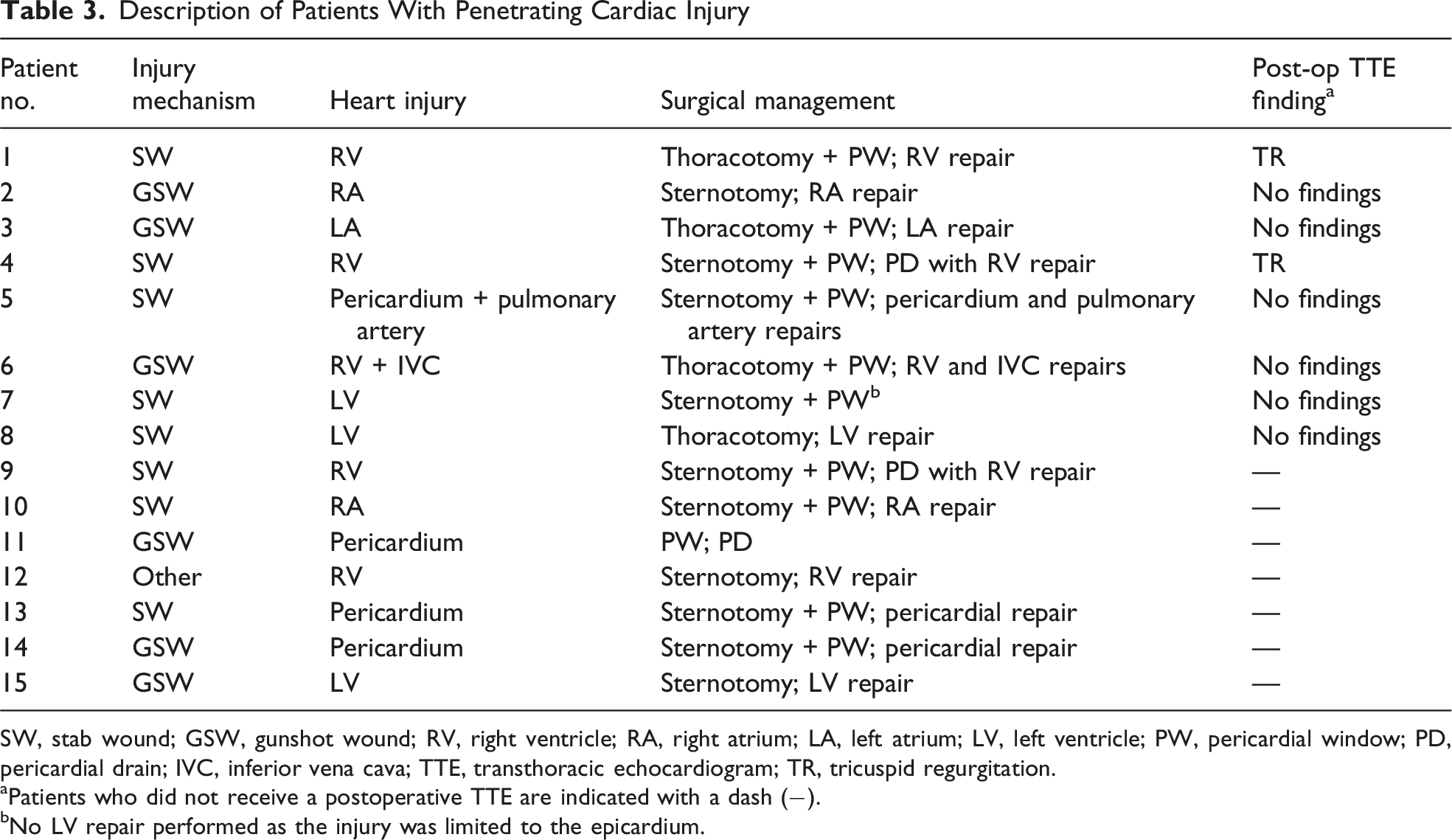
SW, stab wound; GSW, gunshot wound; RV, right ventricle; RA, right atrium; LA, left atrium; LV, left ventricle; PW, pericardial window; PD, pericardial drain; IVC, inferior vena cava; TTE, transthoracic echocardiogram; TR, tricuspid regurgitation.
aPatients who did not receive a postoperative TTE are indicated with a dash (−).
bNo LV repair performed as the injury was limited to the epicardium.
A total of 10 TTEs were performed on 8 (53%) patients. Seven patients underwent a single TTE, while one patient underwent three TTEs. The initial postoperative TTEs were performed on average of 0.9 days following surgical repair. In total six patients had a completely normal postoperative TTE, while two were found to have mild to moderate tricuspid regurgitation. No postoperative TTE identified any missed cardiac injury, pericardial effusion, or new-onset wall motion abnormalities. The two patients with mild to moderate tricuspid regurgitation were deemed clinically insignificant, so none of the ten postoperative TTE resulted in a change in postoperative management.
After repair, all patients were admitted to the ICU for an average length of stay of 4 days. Mean hospital length of stay was 7 days. Six patients experienced infectious complications (two bacteremia and one pneumonia), while three patients were diagnosed with pericarditis. Ultimately, 93% (14 of 15) of the individuals that survived beyond 4 hours and did not undergo complex procedure survived to discharge. The lone mortality died due to anoxic brain injury.
Discussion
Following repair of penetrating cardiac injury, routine postoperative TTE is used to assess adequacy of repair and detect missed cardiac injury. However, a clinically driven approach may be more appropriate than routine use in a subset of low-risk individuals. In our cohort, routine postoperative TTE performed in the index hospitalization demonstrated very low diagnostic yield. Among patients undergoing a single, uncomplicated surgical repair without the need for cardiopulmonary bypass, coronary artery bypass grafting, or additional staged procedures, no clinically significant abnormalities were identified. Seventy-five percent of patients that underwent postoperative TTE were considered normal, and the remaining studies had findings that were deemed clinically insignificant. Importantly, no TTE changed postoperative clinical management. These findings support a selective approach to postoperative TTE, guided by injury complexity and clinical indicators, particularly in otherwise low-risk patients.
Given the low diagnostic yield in this subgroup, our findings suggest that postoperative TTE may be safely deferred in patients who remain asymptomatic throughout their hospital course following a single, uncomplicated repair. In contrast, TTE is indicated in patients who develop clinical signs suggestive of cardiac dysfunction in the postoperative period, including new-onset murmur, chest pain, or symptoms of congestive heart failure. Early postoperative TTE remains appropriate in higher-risk scenarios, including multi-chamber injury, as well as patients requiring more complex operative management such as cardiopulmonary bypass, coronary artery bypass grafting, additional staged procedures, or resuscitative thoracotomy.
To our knowledge, there is one other case series available regarding echocardiographic findings during the index hospital admission following surgical repair of penetrating cardiac injury. Tang et al 8 reported that 17% of 109 survivors had abnormal postoperative echocardiograms post-discharge. The most common complications included pericardial effusions, abnormal wall motion, and decreased ejection fraction, while less frequent findings included intramural thrombus, valve injury, cardiac enlargement, conduction abnormality, pseudoaneurysm, aneurysm, and septal defects. 8 Nearly 80% of patients with abnormal echocardiograms were symptomatic at the time of imaging. 8
Although injury severity between the two cohorts is comparable (mean ISS 26 in Tang et al 8 vs median ISS 27 in our cohort), several differences in injury characteristics and operative complexity may explain the lower diagnostic yield in the present study. Our cohort demonstrated fewer left-sided injuries and several cases limited to pericardial involvement. Although gunshot wounds made up a larger proportion of our cohort than previous studies,6–8 these injuries were predominantly isolated and lacked multi-chamber involvement. In contrast to prior studies,6–8 none of our group had a resuscitative thoracotomy in the emergency department. Furthermore, all patients underwent definitive repair without the need for CPB, CABG, or additional staged procedures. Lastly, none of our cohort presented with any cardiac symptoms that prompted echocardiographic evaluation. These factors suggest our cohort represents a narrower population of patients with relatively uncomplicated injury patterns and straightforward surgical repair, which may account for the lower rate of abnormal postoperative echocardiographic findings.
Both the present study and Tang et al 8 reported low rates of structural defects such as ventricular septal defects, aneurysms, and pseudoaneurysms during the initial hospital admission. This observation could be explained in that some intracardiac lesions may not be immediately detectable in the early postoperative period due to tissue edema or an occluding coagulum plug. 9 As a result, some structural abnormalities may become apparent days to weeks following surgical repair. Consistent with this possibility, studies have reported higher rates of delayed complications during extended follow-up. Cha et al 7 identified abnormal echocardiograms in 23% of their cohort within 2 months of surgical repair, with several ventricular septal defects detected within 4 days following surgery in patients who developed symptoms such as a new-onset holosystolic murmur and signs of congestive heart failure. 7 Demetriades et al 6 reported abnormal echocardiographic findings in 31% of their cohort at a mean follow-up of 23 months. Importantly, this study demonstrated that symptoms and physical exam alone may fail to detect a substantial proportion of delayed complications.
Taken together, these findings suggest that timing and clinical context of echocardiographic evaluation are important considerations when assessing survivors of penetrating cardiac injury. Based on our findings and existing literature, postoperative TTE appears to be clinically useful in patients with cardiac symptoms or higher-risk injury patterns. Potential indicators for routine postoperative TTE evaluation include multi-chamber involvement, complex surgical repair, and history of resuscitative thoracotomy. Patients in the early postoperative period who develop new cardiac findings such as, but not limited to, new-onset murmur, chest pain, or congestive heart failure symptoms should be evaluated with an echocardiogram. In contrast, routine early postoperative TTE in asymptomatic patients with an uncomplicated surgical repair may have limited diagnostic yield.
The present study evaluated echocardiograms obtained in the initial hospital admission and therefore cannot assess delayed complications that may develop after discharge. Previous studies report that routine late follow-up is important in identifying delayed cardiac complications, regardless of whether a patient is symptomatic.6,7
Conclusion
While use of TTE after surgery for penetrating cardiac injury is common, it did not impact the postoperative management of any patient in our study. However, this should be interpreted in the context of several limitations, including small sample size, single-center retrospective design, incomplete uptake of postoperative TTE within our cohort, and lack of follow-up beyond the index hospitalization. Within these constraints, our data suggests that patients who undergo a single uncomplicated operation for penetrating cardiac injury without the need for more advanced procedures or additional staged procedures appear unlikely to reveal clinically significant routine postoperative TTE findings. This study is in support of a selective risk-stratified approach to postoperative echocardiograms in higher-risk scenarios. As our results are observational, further multi-institutional studies with longitudinal follow-up are required to better define optimal imaging strategies.
Footnotes
Ethical Considerations
The Ethics Committee of the USA Health University Hospital waived the need for ethics approval and patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on request.