
Abstract
Severe pyogenic soft-tissue infections (SSTI) are a frequent cause of morbidity among people living with HIV (PLHIV) in resource-limited hospitals. Drawing on five months of frontline work in a district surgical unit in South Sudan, this field report distills practical lessons into a simple, resource-adapted algorithm for triage, source control, antibiotics, and wound care. Core steps include bedside sepsis screening with qSOFA, prompt empiric antibiotics aligned with the WHO EML/AWaRe approach, and decisive operative debridement without waiting for advanced diagnostics when necrotizing infection is suspected, followed by planned re-look procedures. Low-cost wound-care options (eg, diluted hypochlorite/povidone-iodine transitioning to saline gauze) and loss-to-follow-up–aware discharge practices are emphasized. The aim is to standardize care and shorten time to debridement in district-level services rather than report outcomes. Keywords: pyogenic soft-tissue infection; HIV; resource-limited settings; necrotizing fasciitis.
Introduction
Severe pyogenic skin and soft-tissue infections (SSTIs) remain an important cause of morbidity among people living with HIV (PLHIV), particularly in resource-limited settings where delayed presentation, advanced local disease, and restricted access to surgical care are common.1,2 In many district-level hospitals across sub-Saharan Africa, clinicians must make urgent bedside decisions with limited diagnostics, narrow antibiotic formularies, constrained peri-operative support, and uncertain patient follow-up. 3 Although current guidelines emphasize early source control and empiric antimicrobial therapy, much of the available literature assumes access to imaging, microbiologic cultures, intensive care support, and structured postoperative follow-up that may not be consistently available in low-resource surgical environments. 4
In these settings, management often depends primarily on clinical recognition, pragmatic operative decision-making, and simplified treatment pathways that can be implemented despite infrastructure limitations. This manuscript presents a field-derived perspective from five months of frontline surgical care at a mission-run district hospital in South Sudan. Rather than proposing a validated protocol, we describe how repeated bedside decision-making under operational constraints evolved into a pragmatic management workflow for severe pyogenic SSTIs in PLHIV. Our aim is to highlight how triage, operative timing, empiric antibiotic therapy, wound care, and discharge planning were adapted to a setting with limited diagnostics and constrained follow-up, and to provide a practical framework for clinicians working in similar resource-limited environments.
Clinical Setting and Operational Constraints
This field report draws on bedside experience from a mission-run district hospital (146 total beds; surgery 40) in South Sudan. One operating room with two tables supported twice-weekly elective lists and 24/7 emergency access. Water supply was stable; electricity was reliable via solar with generator backup. An autoclave was available; apart from disposable scalpel blades, instruments were re-sterilized between uses. Routine postoperative care occurred on standard wards (no HDU/ICU). In practice, this meant that many critical decisions had to be made quickly at the bedside, often before confirmatory testing, and with a low threshold to intervene when delay could cost tissue, limb, or life. These constraints shaped every stage of care, from triage and operative timing to wound dressing selection and discharge planning.
Diagnostic capacity was limited but clinically useful when available. Ultrasound was available; plain radiography twice weekly; no CT. Laboratory capacity comprised CBC and rapid antigen tests (HIV, hepatitis B/C, typhoid, and malaria); there was no culture service. Given limited laboratory support, a simple bedside sepsis screen (qSOFA) was applied at triage to flag high-risk patients. 5 Point-of-care ultrasound aligns well with low-resource workflows.6,7 However, imaging and laboratory tests were treated as adjuncts rather than prerequisites for operative decision-making when necrotizing infection or uncontrolled sepsis was suspected.
Anesthesia and peri-operative support were also adapted to local capacity. Minor procedures used spinal anesthesia or ketamine procedural sedation; major laparotomies proceeded under general anesthesia with basic monitoring. Ketamine remains a critical enabler of anesthesia care across sub-Saharan Africa. 8 Transfusion relied on warm whole blood from family/replacement donors; component therapy was not available. In limited-resource settings, whole blood is an appropriate option when component processing and storage are not feasible. 9
The formulary typically included benzylpenicillin, ampicillin, gentamicin, ceftriaxone, metronidazole, and intermittently vancomycin. These map to the WHO Model List of Essential Medicines and permit stewardship within an AWaRe framework. 10 Because microbiologic cultures were unavailable, antibiotic decisions had to balance empiric coverage, toxicity, drug availability, and early de-escalation once the patient stabilized.
Local wound care relied on povidone-iodine, saline, gauze, and bandages; negative-pressure wound therapy was not available. Dressings were changed daily. Core surgical instruments, including suction and standard debridement sets, were available. As a result, wound plans had to be simple, reproducible, inexpensive, and feasible for ward nurses, patients, and families after discharge.
The catchment included remote communities; neighboring facilities lacked a functioning operating room. Life-threatening emergencies were treated free of charge; elective surgery cost approximately US$15 and outpatient visits approximately US$1. Distance, transport barriers, and out-of-pocket costs likely contributed to late presentation and frequent loss-to-follow-up. 11 These realities shaped bedside decision-making: whenever possible, we favored early source control, simple wound plans, and discharge instructions that patients and families could realistically carry out. ART services operated on-site with good drug availability, yet many patients remained untreated due to non-uptake/refusal; regionally, treatment gaps persist despite expanded access. 12
Field Experience and Key Management Challenges
Over five months in a mission-run district surgical unit, severe pyogenic SSTIs in PLHIV were encountered repeatedly, often after several days of symptoms, home treatment, or delayed referral. Patients commonly presented with advanced local infection, systemic illness, or wounds that had already progressed beyond the stage at which outpatient treatment alone was realistic. In this environment, the central challenge was not simply choosing the ideal investigation or antibiotic regimen, but making timely surgical decisions with incomplete information and limited capacity for rescue if deterioration occurred.
Several recurring challenges shaped the management approach. First, delayed presentation meant that local disease was frequently extensive at the time of surgical evaluation. Second, diagnostic support was limited, and neither CT imaging nor microbiologic cultures were available to guide early decisions. Third, the antibiotic formulary was narrow and variable, requiring empiric regimens that were both clinically reasonable and locally available. Fourth, postoperative wound care had to be feasible on standard wards without negative-pressure therapy or advanced dressings. Finally, follow-up after discharge was uncertain because many patients lived far from the hospital and faced transport and financial barriers.
These realities required a management strategy that prioritized early recognition of sepsis, rapid operative source control when necrotizing infection or uncontrolled purulence was suspected, and simple wound-care plans that could be continued after discharge. The pathway described below therefore did not originate as a formal protocol. It evolved from repeated bedside decisions under operational pressure and was later organized into a pragmatic workflow intended to support similar frontline surgical settings. Representative clinical findings from these presentations are shown in Figure 1. Representative clinical images of severe pyogenic soft-tissue infections in PLHIV. (A)-(C) Groin-thigh infection before and after debridement. (D)-(E) Cervical infection with fistula formation after debridement. (F) Anterior leg wound with exposed tibia after delayed presentation. (G) Necrotizing fasciitis of the lower limb with skin and subcutaneous tissue necrosis. All images show non-identifiable body areas only
Pragmatic Algorithm Derived From Frontline Care
The management pathway that emerged from this setting is summarized in Figure 2. It was organized around five practical priorities: early recognition of sepsis, empiric antimicrobial therapy based on local availability, timely operative source control, low-cost wound care, and discharge planning adapted to limited follow-up. The purpose of the algorithm is not to replace existing guidelines or serve as a validated protocol, but to translate core principles into a workflow that can be applied when advanced imaging, microbiologic cultures, intensive care support, and structured outpatient follow-up are not consistently available.4,10,13,15 Pragmatic algorithm for managing severe pyogenic SSTIs in PLHIV in a resource-limited district hospital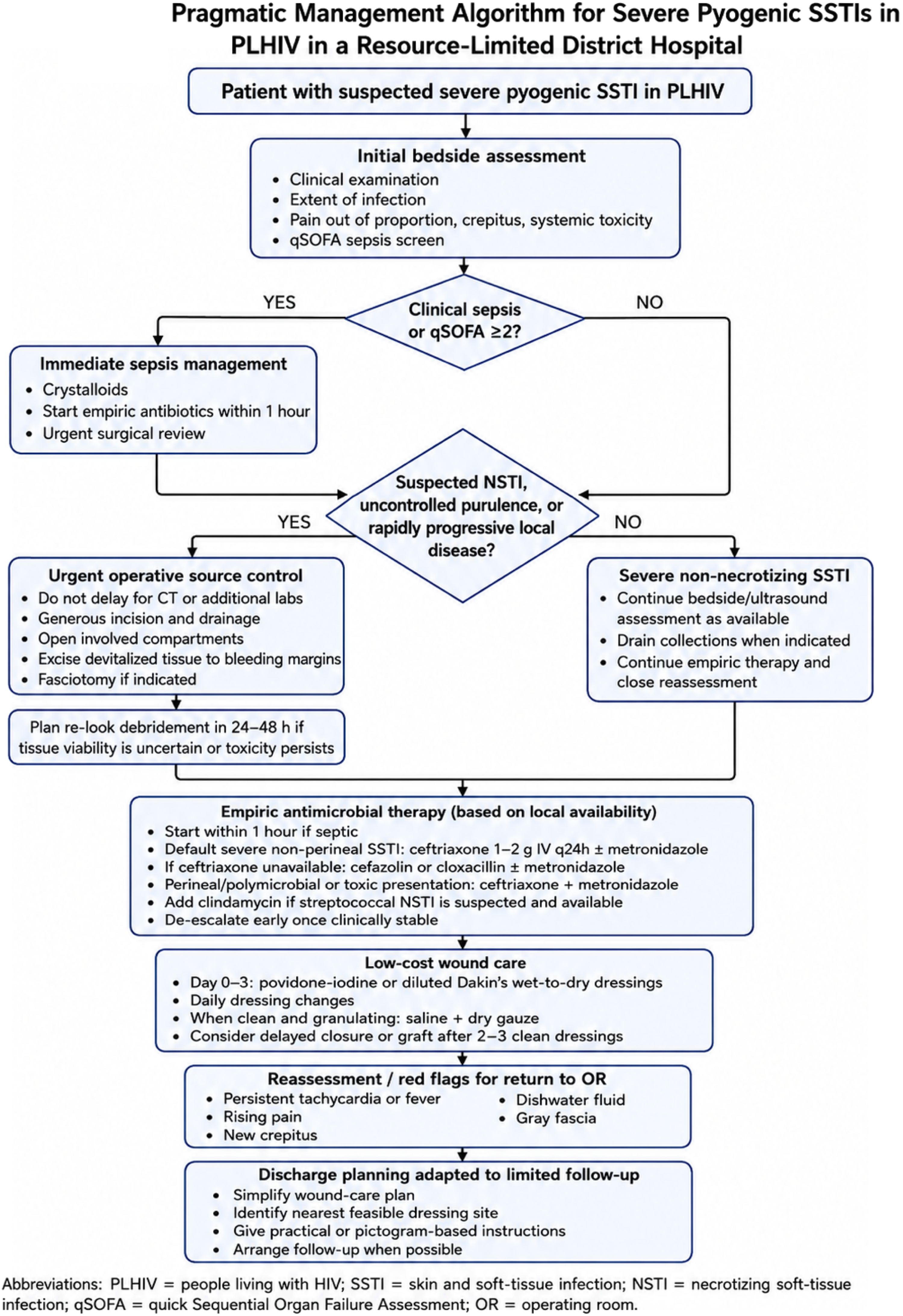
At presentation, patients were assessed clinically, with qSOFA used as a simple bedside screen to identify high-risk patients. 5 When sepsis was suspected, resuscitation, empiric antibiotics, and surgical review were initiated without delay. 13 When necrotizing infection, uncontrolled purulence, or rapidly progressive local disease was suspected, operative exploration and debridement were not delayed for CT imaging or additional laboratory confirmation.4,14
Antibiotic selection was guided by local availability and the suspected clinical syndrome, with early de-escalation once the patient stabilized.10,15 Operative management emphasized generous drainage, opening of involved compartments, and excision of devitalized tissue to bleeding margins, with planned re-look debridement when tissue viability remained uncertain 4,14. Wound care followed a simple progression from antiseptic or wet-to-dry dressings toward saline gauze, delayed closure, or grafting once the wound was clean and granulating. 16 Because return visits were often uncertain, discharge planning focused on simplified wound-care instructions and the nearest feasible site for dressing changes. 11
Discussion
This field-derived workflow differs from standard SSTI management less in its underlying principles than in how those principles are operationalized under constraint. In well-resourced settings, severe SSTIs are commonly supported by cross-sectional imaging, microbiologic cultures, broad antimicrobial availability, intensive care capacity, advanced wound therapies, and structured outpatient follow-up. In the district-level setting described here, these supports were limited or unavailable. As a result, management depended heavily on bedside recognition, early operative judgment, formulary-based antibiotic selection, simple wound-care methods, and discharge planning that anticipated loss-to-follow-up.
The most important adaptation was the threshold for operative source control. When necrotizing infection, uncontrolled purulence, or rapidly progressive local disease was suspected, clinical findings were prioritized over confirmatory imaging or laboratory testing. This approach is consistent with the principle that delays in debridement worsen outcomes in necrotizing soft-tissue infection, but it becomes especially important where CT, ICU rescue, and repeat specialist review are not readily available.4,14 In this context, early exploration was often the safest diagnostic and therapeutic step.
Antibiotic management also required adaptation. Without culture support, empiric therapy had to be selected from a narrow formulary and guided by clinical syndrome, severity, and anatomic site. The workflow therefore emphasizes practical regimens that align with available essential medicines and stewardship principles, followed by early de-escalation once systemic signs and wound findings improved.10,15 This approach accepts diagnostic uncertainty while avoiding unnecessary escalation whenever clinical stabilization allowed.
Wound care and discharge planning were equally central. In settings without negative-pressure wound therapy or advanced dressings, daily low-cost dressings and repeated bedside reassessment became the foundation of postoperative care. Because many patients lived far from the hospital and could not reliably return for frequent review, discharge planning was treated as a clinical intervention rather than an administrative step. Simplified instructions, feasible dressing locations, and early identification of red flags were necessary to make source control durable beyond the operating room.
The broader lesson is that resource-limited surgical care requires more than simplified versions of high-resource protocols. It requires workflows that explicitly account for diagnostic uncertainty, limited rescue capacity, constrained drug availability, and fragile continuity of care. The proposed algorithm is therefore best understood as a pragmatic framework derived from repeated frontline decisions, rather than as a validated protocol or substitute for local clinical judgment.
Limitations
This manuscript reflects frontline surgical experience from a single mission-run district hospital and was not designed as a prospective observational study. Standardized patient-level data, microbiology, outcomes, and long-term follow-up were not systematically collected. Therefore, the proposed workflow should not be interpreted as a validated protocol or as evidence of improved clinical outcomes.
Culture services, CT imaging, advanced wound therapies, and reliable follow-up were limited or unavailable, and these constraints shaped both the clinical decisions described and the level of evidence that could be generated. Nevertheless, the report provides a pragmatic synthesis of repeated bedside decision-making in a resource-limited surgical environment and may help inform care in similar settings.
Conclusion
In this resource-limited district hospital, management of severe pyogenic SSTIs in PLHIV depended on bedside sepsis recognition, early operative source control, formulary-based empiric antibiotics, simple wound care, and discharge planning adapted to uncertain follow-up. The proposed algorithm translates these recurring frontline decisions into a pragmatic workflow for similar constrained settings. It should be interpreted as a field-derived framework rather than a validated protocol, and future prospective work is needed to evaluate outcomes and refine its applicability.
Footnotes
Acknowledgments
We thank the surgical, nursing, and anesthesia teams of Mary Immaculate Hospital in Mapuordit, South Sudan, the community health workers, and the staff of the on-site HIV clinic for their dedication and partnership. Our deepest thanks go to the patients and their families, whose trust made this work possible.
Ethical Considerations
The approval of the ethics committee was not necessary as the article is a completely anonymized and no experiments were performed.
Consent to Participate
Not required. All clinical data in this report are fully anonymized, and all images depict non-identifiable body areas only. Faces and unique features (eg, tattoos, birthmarks, jewelry) are not shown; dates and locations have been removed or generalized to prevent re-identification. No individual can be identified and no personal health information is disclosed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.