
Abstract
Work-related musculoskeletal (MSK) pain is frequent in surgeons, but factors associated with it are not well studied. Methods: Repeat surveys were sent to general and subspecialty surgeons in the evening of their operating room (OR) days in one month. Age, sex, BMI, weekly exercise, NASA Task Load Index (NASA-TLX: a composite measure of workload), and pain scores were collected. Operating room case length and approach were collected from a registry. All variables were analyzed for their independent association with mean pain score changes in 12 body regions (with 95% CI). Results: There were 29 surgeons who performed a total of 537 operative cases on 228 OR days. Increases in NASA-TLX by 100 were associated with increased pain in neck +0.23 (0.10-0.35), hands/fingers +0.22 (0.11-0.33), upper back +0.22 (0.10-0.34), lower back +0.31 (0.18-0.44), buttocks +0.07 (0.02-0.13), hips +0.10 (0.03-0.18), legs +0.14 (0.06-0.21), and feet +0.15 (0.05-0.24). Longer total case length increased pain in neck and upper back (+0.15 and +0.13 for every increase in 4 hours, respectively). An OR day with higher proportion of robotic time was associated with increased pain in wrists +0.32 (0.10-0.54) and lower back +0.36 (0.02-0.70). Higher proportion of lap/endo time was associated with increased pain in upper back +0.33 (0.08-0.58). Conclusion: Workload was the strongest contributor to musculoskeletal pain during operating days, with associations seen across most body regions. Case length and approach contributed to pain in a smaller number of regions. Targeted ergonomic strategies may reduce the burden of MSK pain among surgeons.
Keywords
Musculoskeletal Pain on Operating Days Take away Points
• This study extends work exploring surgeon musculoskeletal pain by engaging a large multi-disciplinary cohort over real operating days and different surgical modalities and utilizing NASA-TLX as a standardized scale in surgeon workload assessment. • Surgeons’ perceived workload, not case length or surgical approach, emerged as the strongest contributor to musculoskeletal pain.
Introduction
Work-related musculoskeletal disorders (WRMSDs) are highly prevalent among surgeons and represent a major source of occupational injury, lost work time, and reduced clinical productivity.1,2 Prior reviews report on WRMSD rates ranging from 66 to 94% in open surgery, 73 to 100% in conventional laparoscopy, 54 to 87% in vaginal surgery, and 23 to 80% in robotic-assisted procedures.1–4 A survey of 260 surgeons found that 22% missed work and 35% reduced their case load during recovery from musculoskeletal (MSK) injuries. 2 Cross-sectional data suggest an increase in pain prevalence with greater case volume and longer operative duration. For instance, in an international study surveying laparoscopic surgeons, 90% reported pain attributed to their work. Additionally, those operating more than 4 hours per day were significantly more affected than those performing shorter cases. 3
The pattern and distribution of MSK pain varies by surgical modality, reflecting the distinct biomechanical demands of each approach. Laparoscopic surgeons often experience neck, shoulder, back, and hand pain. This aligns with biomechanical factors such as restricted motion, static postures, and poor visual-motor coordination.5–7 Robotic surgery generally results in lower self-reported discomfort and reduced objective muscular strain compared to laparoscopy.8–10 However, robotic systems still impose strain, notably static neck posture and wrist load. 8 With open approaches, broader physical movements are allowed, but there are ergonomic risks associated with equipment use (ie, loupes and headlamps), awkward postures, and static load bearing activities.11,12 Across all modalities, MSK pain contributes to cumulative strain with potential for long-term consequences for surgeon performance, endurance, and career longevity.
Despite increasing recognition of ergonomic risks in surgery, several important gaps remain. Much of the existing literature presumes that case volumes, operative duration, and complexity contribute to MSK burden, yet few studies quantitatively link these exposures to validated, region-specific pain outcomes. Additionally, current research rarely integrates surgeon-level characteristics or day-to-day variability in workload, limiting the ability to identify actionable contributors to MSK strain. A more comprehensive understanding of how patient characteristics and intraoperative factors shape daily MSK pain is essential for developing effective, evidence-based ergonomic strategies and to promote surgeon well-being.
Accordingly, this study evaluated surgeon characteristics and operating room factors associated with anatomic region-specific MSK pain among surgeons. Specifically, the aim was to quantify the relationship between daily workload, surgical modality, operative characteristics, and body region MSK pain in practicing surgeons.
To evaluate this aim, we employed the National Aeronautics and Space Administration Task Load Index (NASA-TLX), a multidimensional workload assessment tool that quantified perceived workload across 6 domains: mental demand, physical demand, temporal demand, effort, frustration, and perceived performance. 13 It was originally developed for human performance research, and the tool has been adopted in fields ranging from aviation to health care to assess cumulative demands associated with complex tasks.13,14 Unlike isolated ergonomic measurements, the NASA-TLX captures both the physical and the cognitive components of workload, making it relevant for evaluating the demands of surgical practice. 15
Methods
This prospective cohort study involved only surgeon participants, and the surgeon daily operating schedule was accessed from the electronic registry. No patient charts were reviewed. The Kaiser Permanente Southern California-Hawaii Institutional Review Board was consulted and it exempted the study from review. Repeat electronic surveys were sent digitally to general and subspecialty surgeons at Kaiser Permanente Los Angeles Medical Center in the evening of their operating room (OR) days over the course of a single month. Age, sex, BMI, and hours per week of moderate to vigorous exercise were collected on day 1 of the study period. NASA Task Load Index and pain scores on a scale of 0-4 (none to severe) were collected each evening. The NASA-TLX is a validated instrument designed to quantify perceived workload across 6 domains: mental demand, physical demand, temporal demand, effort, frustration, and performance. Each domain is scored on a 0-100 scale and combined into a composite workload score. Higher values indicated greater perceived workload. 13 Total adjusted OR time per day (case length in registry adjusted by surgeon reported scrubbed-in time), surgical approach (open, laparoscopic/endoscopic, or robotic), and daily proportions of time of these approaches in each OR day were collected from an electronic registry and all variables were analyzed for their independent association with surgeon pain scores in 12 body regions including neck, shoulder, elbow/arm, wrist, hands/fingers, upper back, lower back, buttock, hip, knee, leg, and feet.
Descriptive statistics were used to summarize surgeon demographics and baseline characteristics. Linear mixed-effect models were constructed to evaluate the association between NASA TLX measures, case length, operative approach, and region-specific pain scores on operative days from individual surgeons. The mixed-effects modeling was selected to account for within-surgeon variability. Models were also adjusted by age (condensed into 3 categories), sex, BMI, and exercise frequency. Regression coefficients with 95% confidence intervals were reported, with statistical significance defined as P < 0.05. Analyses were performed using SPSS (IBM Corp).
Results
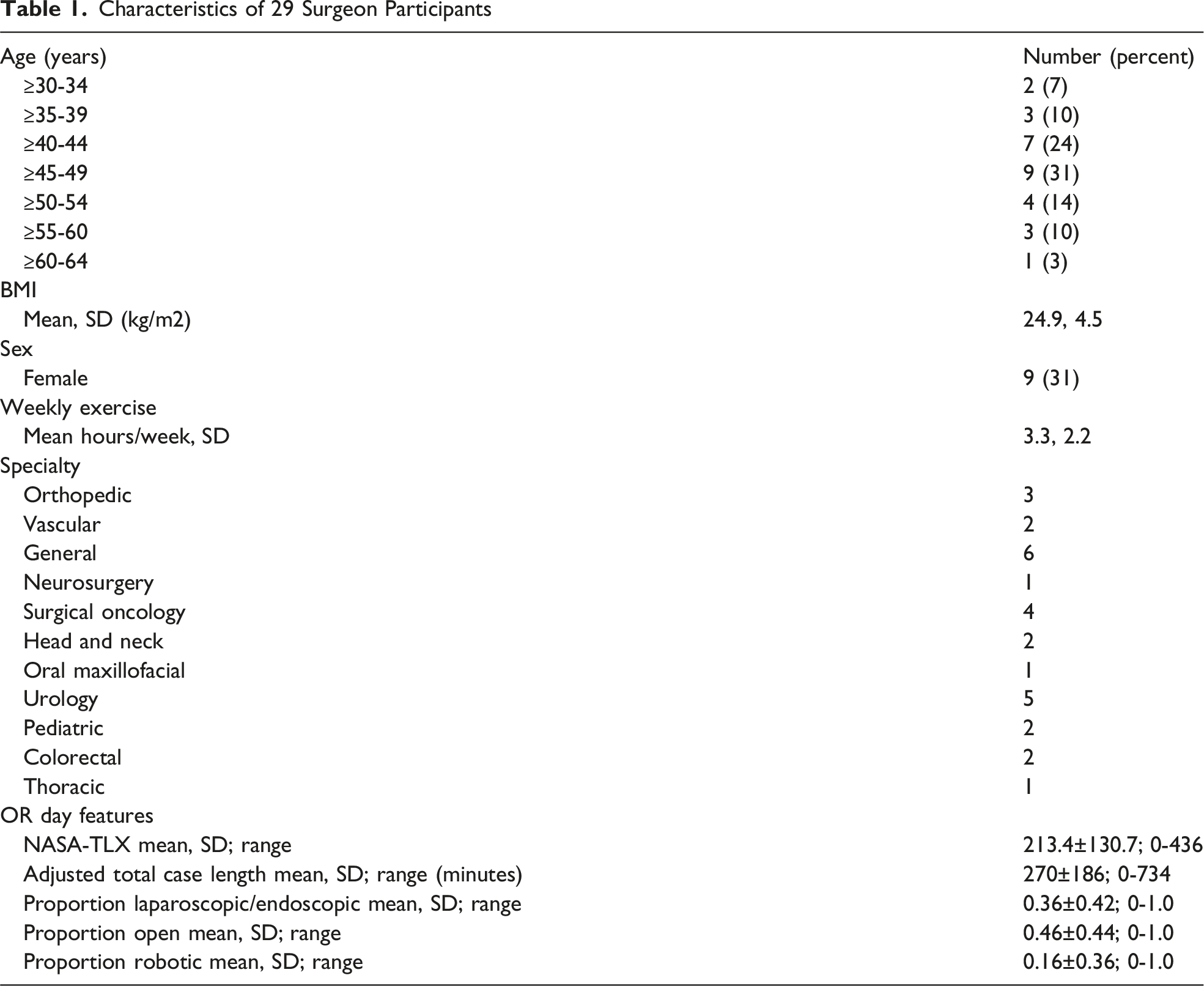
Characteristics of 29 Surgeon Participants
Pain Scores in the 12 Anatomic Regions for all 228 OR Days
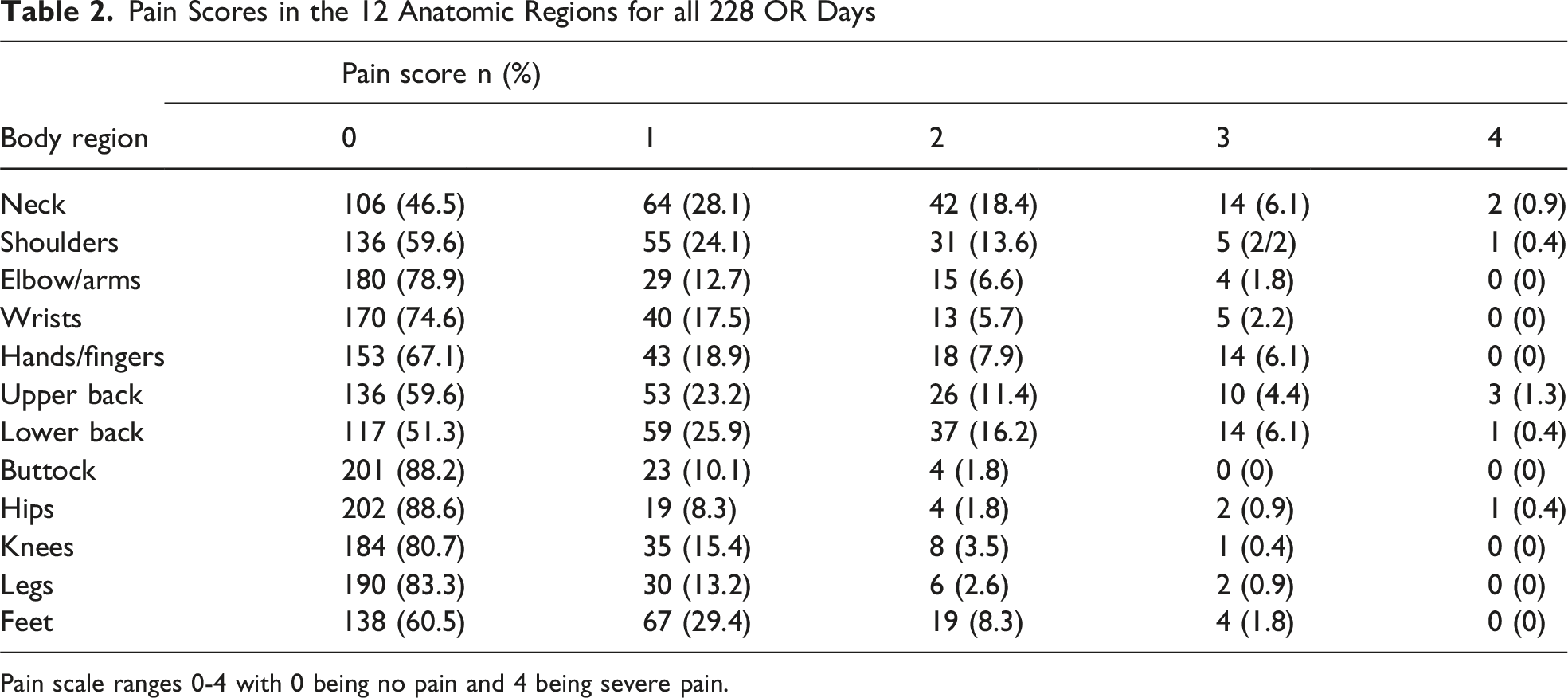
Pain scale ranges 0-4 with 0 being no pain and 4 being severe pain.
Significant a Factors Associated With Body Region Pain Score
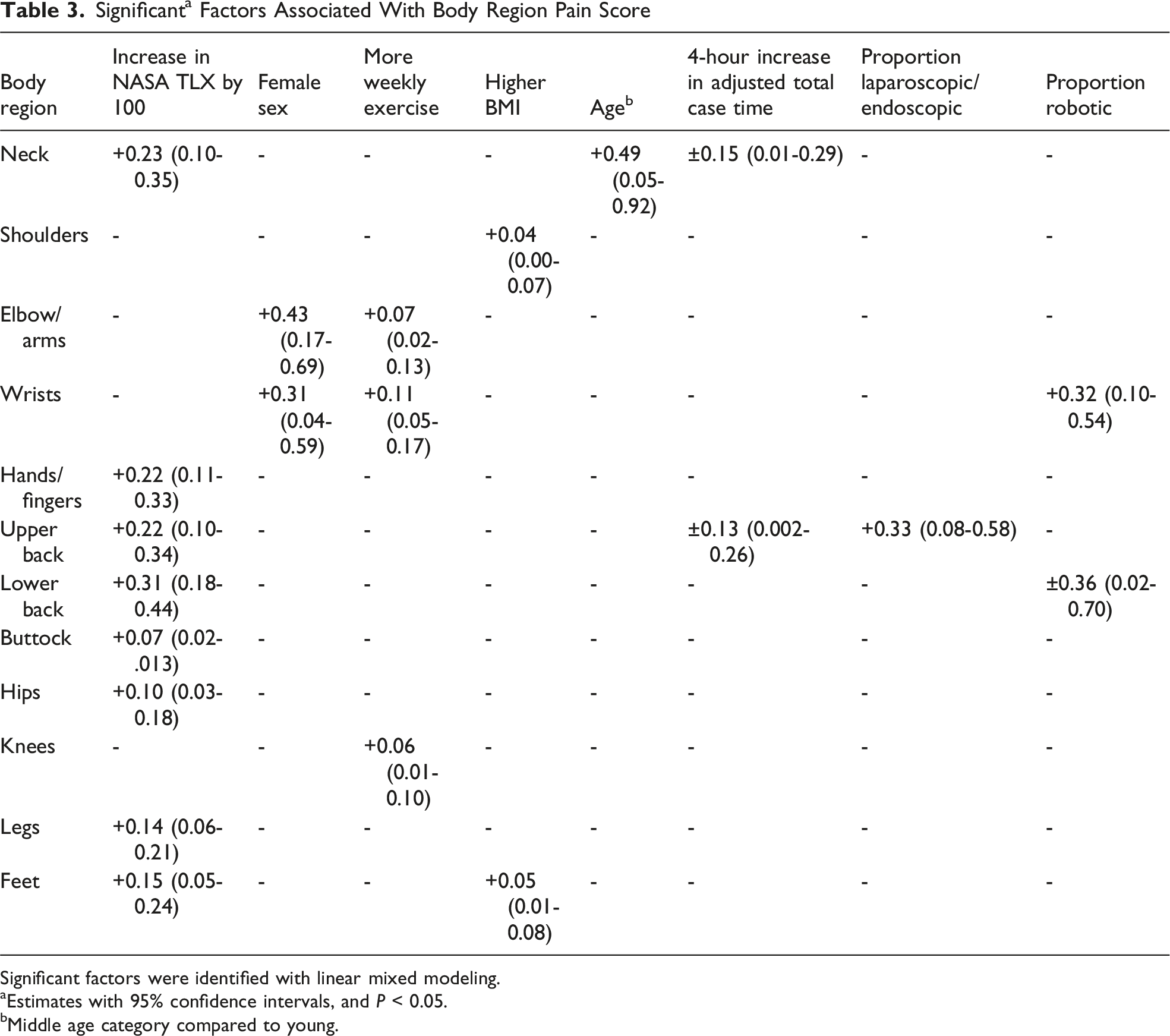
Significant factors were identified with linear mixed modeling.
aEstimates with 95% confidence intervals, and P < 0.05.
bMiddle age category compared to young.
Discussion
In this study, workload emerged as the strongest contributor to musculoskeletal (MSK) pain on operative days, demonstrating significant associations across nearly all body regions studied. NASA-TLX serves as a more sensitive indicator of operative strain by capturing dimensions of workload that are not reflected in traditional operative and ergonomic metrics. For instance, operative duration quantifies exposure time, but it does not account for cognitive complexity, time pressure, technical difficulty, frustration, or perceived effort. By integrating these domains into a single quantitative measure, the NASA-TLX may better reflect the cumulative physiologic and psychologic burden experienced by surgeons during an operative day.
Operative factors such as total case length and surgical approach were associated with pain in fewer anatomical regions. This indicates that duration and technique alone do not fully explain ergonomic stress, and that subjective workload may be a more sensitive measure of real-time operator strain. For example, a short but cognitively intense case may generate higher NASA-TLX scores—and correspondingly greater MSK discomfort—than a longer yet less demanding operation.
Interestingly, increasing age was not commonly associated with MSK pain, nor was less moderate to vigorous exercise during the week. Although counterintuitive, exercise outside of the workplace has been shown to be less effective as workplace group exercise in mitigating MSK pain in health care workers. 16 Likewise, increasing BMI was not associated with an increase in MSK pain. With these findings in mind, there are preventative measures that can be taken in the workplace to minimize surgeon MSK pain. The benefits of the intraoperative micro-break (ie, short breaks between tasks while remaining within the sterile field) have already been described, though have yet to become standard practice. 16 Non-medical industries with high physical demands investigated exercise-based injury prevention strategies with low-time commitment. The findings suggest that low-cost interventions focused on flexibility and conditioning may represent promising strategies for reducing musculoskeletal strain among surgeons as well. 17
Work-related musculoskeletal disorders (WMSDs) are highly prevalent among surgeons and a significant contributing factor in surgeon job dissatisfaction. Many studies to date rely on heterogenous, non-validated pain scales, making cross-study comparisons challenging and obscuring the relative contribution of biomechanical demands across surgical modalities. This is not the first study to utilize NASA-TLX as a standardized scale in surgeon workload assessment. For instance, in the study by Stewart et al, the NASA-TLX was used to assess ergonomic outcomes in open vs robotic cases. 18 Other studies with smaller cohorts have also utilized NASA-TLX, looking at subspecialty-specific surgeon perceived workload in plastic surgery and colorectal surgery.19,20,21 However, our study extends this work by engaging a large multi-disciplinary cohort over real operating days and different surgical modalities.
Strengths of this study include its prospective design, repeated daily measurements across real-world-operative practice, inclusion of multiple surgical specialties, and use of a validated workload instrument paired with region-specific pain outcomes. These features allowed evaluation of day-to-day variability in surgeon workload and musculoskeletal symptoms, providing a more granular assessment than prior cross-sectional surveys.
Several limitations should be considered with this study. Firstly, the study was conducted at a single institution over a 1-month period. This may limit generalizability to other practice environments. Secondly, both pain scores and NASA-TLX scores were self-reported and therefore susceptible to reporting bias. Thirdly, unmeasured factors such as sleep quality, operating room staffing, and psychosocial stressors, among others, could have influence workload and pain reporting.
In summary, this study demonstrates that surgeon-perceived workload, measured using the NASA-TLX, is more consistently associated with musculoskeletal pain than traditional operative metrics such as case duration or surgical approach. These findings suggest that workload captures import dimensions of operative strain that are not reflected by procedure characteristics alone. Therefore, strategies aimed at reducing surgeon injury should not only focus on operative technique and duration, but also on modifiable contributors to overall workload. Incorporating workload assessment into future ergonomic initiatives may aid in identification of surgeons at greatest risk for musculoskeletal injury and guide targeted interventions to improve surgeon well-being and career longevity.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.