
Abstract
Background
Ultra-radical cytoreductive surgery is frequently performed for patients with advanced ovarian cancer (OC). However, anastomotic leakage (AL) is a serious complication of such surgeries and the risk factors remain unclear. This study identified early postoperative C-reactive protein (CRP) and albumin were the strongest predictors of leakage.
Methods
This multicenter retrospective study involved 305 patients with ovarian cancer who underwent primary anastomosis following enterectomy, spanning January 2018 to June 2023. Comprehensive clinical and demographic data were used to develop predictive models. Feature selection was performed using LASSO and univariate logistic regression. Machine learning algorithms were subsequently applied, with model interpretability assessed using SHapley Additive explanations (SHAP).
Results
The study revealed an AL prevalence of 14.1%, with 46.5% of affected patients requiring reoperation. Five predictors were identified, including postoperative CRP, serum albumin levels, Eastern Cooperative Oncology Group score, N stage, and blood urea nitrogen. The Lasso-Logistic model demonstrated the best predictive performance with an area under the curve of 0.828 (0.119). SHAP analysis highlighted early postoperative CRP, albumin, and N stage as major contributing factors. Economic analysis revealed a significant correlation between AL and hospital stay, hospital costs, and time to chemotherapy.
Discussion
Early postoperative inflammatory and nutritional biomarkers, particularly CRP and albumin, demonstrated significant predictive value for anastomotic leakage, providing an early warning for risk stratification and intervention. The investigation also bolstered the evidence supporting the restrictive surgical scope approach advocated in clinical guidelines.
Introduction
Ovarian cancer (OC) is among the most common gynecological malignancies, significantly affecting women’s health globally. According to the International Agency for Research on Cancer’s (IARC) Global Cancer Statistics 2022 report, OC accounted for 3.4% of all female cancers and 4.8% of cancer-related female deaths in 2022. 1 Aggressive surgery improves postoperative survival, and optimal cytoreduction linked to higher 5-year survival compared to cases with residual tumors over 1 cm. 2 Consequently, ultra-radical cytoreductive surgery, which often involves resecting adjacent abdominopelvic tissues invaded by the tumor (eg, bowel and bladder), is commonly employed in advanced OC. Rectosigmoid resection (RSR) is the most frequent procedure, followed by colon and small bowel resections. 3 Intestinal anastomosis is necessary for bowel reconstruction but poses a high risk of postoperative anastomotic leakage (AL)—a severe complication with reported incidences of 5.3-16.9% among OC patients undergoing bowel resection.4,5 AL significantly increases health care costs, prolongs hospital stays, and raises the likelihood of secondary surgeries, with associated mortality rates ranging from 3% to 21%. 6 Additionally, AL can delay adjuvant chemotherapy, adversely impacting survival outcomes. 7
Given the detrimental impact of AL on patient outcomes and the financial burden it imposes, some studies have aimed to identify its risk factors, including the American Society of Anesthesiologists (ASA), renal disease, advanced cancer stage, and multiple bowel resections.8,9 Machine learning (ML) emphasizes not only the non-linear relationships of the variables themselves, but also the non-linear interactions between variables when dealing with structured and unstructured data, and ML models have gained increasing recognition in health care settings due to their ability to develop robust risk models and improve predictive accuracy. 10 We conducted a search of PubMed for ML-based studies on predicting anastomotic leakage (AL) and identified 21 relevant studies, with all focusing on colorectal and gastroesophageal cancers. However, most studies were limited by single-center data and overlook psychosocial factors, and other AL-related variables.11,12
The objective of this study was to develop an ML-based predictive model to identify high-risk factors contributing to AL, facilitating early assessment of AL risk in OC patients during the perioperative period.
Methods
Ethics approval was obtained from the IEC for Clinical Research of Zhongda Hospital, Affiliated to Southeast University (Approval No. 2024ZDSYLL077-P01).
Data Source
This machine learning-based predictive model was developed using data sourced from three medical research centers in China, spanning January 2018 to June 2023. The study encompassed all inpatients diagnosed with ovarian cancer who underwent primary anastomosis following bowel resection. Demographic, clinicopathological, and medical expense data were retrospectively extracted from electronic medical records (EMR). AL diagnostic criteria included abdominal pain, fever, abdominal distension, tenderness, rebound pain, or muscle tension within 2 months after OC surgery, combined with at least one of the following: (1) feculent fluid from drains, wounds, or the vagina; (2) definitive radiographic evidence of extravasation at the anastomotic site; or (3) AL detected during reoperation. 8
Study Measures
Allostatic load, a cumulative measure of physiological damage from cognitive-emotional responses to socio-environmental stressors. 13 The study utilized biomarkers routinely collected in clinical practice and extensively cited in the literature related to allostatic load, spanning four physiological systems including cardiovascular; metabolic; renal, and immune. Patients were assigned a point for each biomarker in the worst quartile, with higher scores indicating greater physiological dysregulation. 14 An adapted Aletti Surgical Complexity Score was used to assess the complexity of the surgical procedure, with procedures assigned scores from 1 to 3 based on complexity, and surgeries categorized as simple or complex (Supplemental Table S1).15-17
Model Building Process
Statistical Analysis
Continuous variables were expressed as mean ± SD or median (interquartile range, IQR), depending on distribution, and compared using t-tests or nonparametric tests. Categorical variables were compared using χ2 or Fisher’s exact test. Statistical analyses and model development were conducted using R software (version: 4.4).
Results
Patient Characteristics
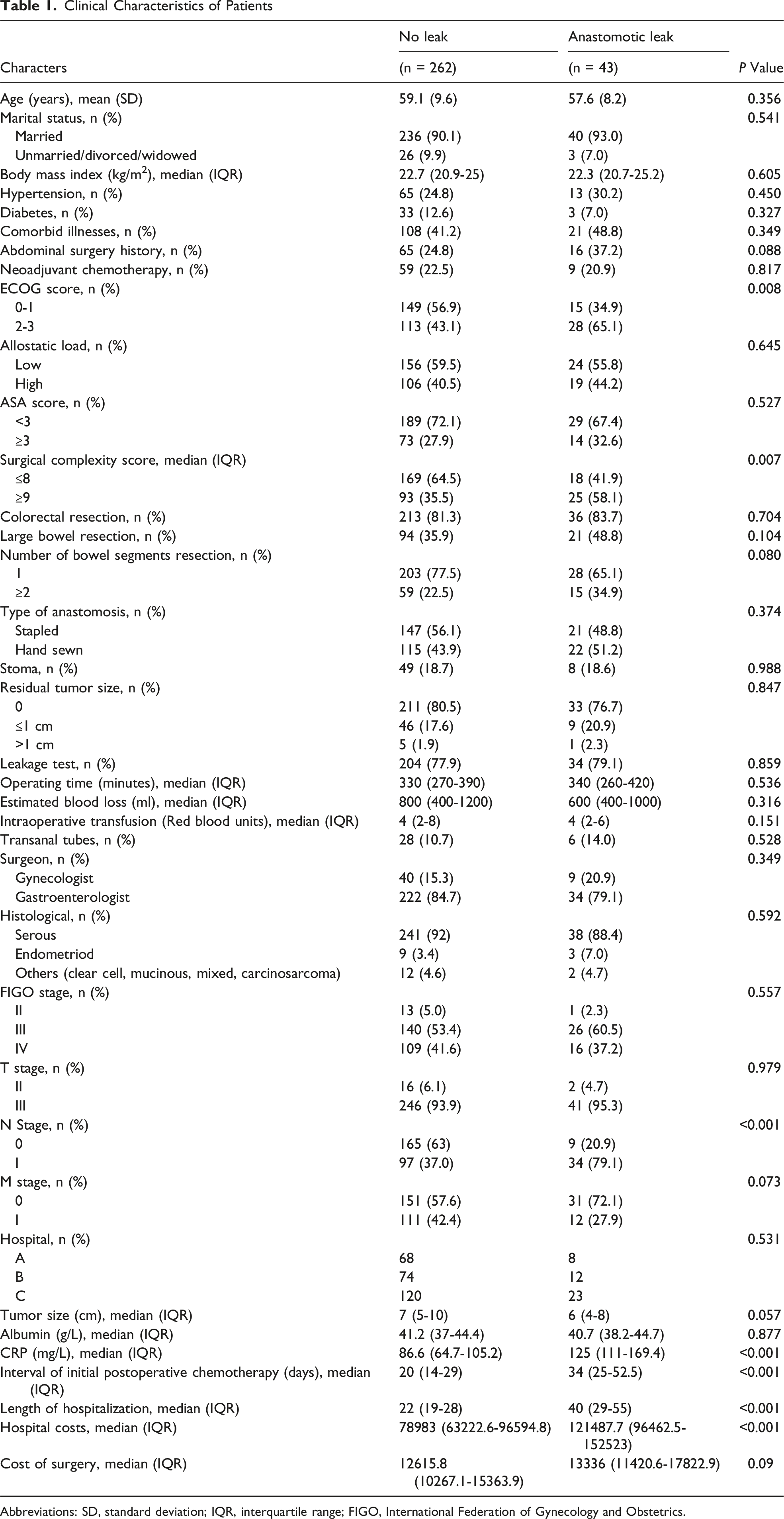
A total of 401 eligible patients were initially screened, with 96 patients excluded based on the exclusion criteria, resulting in a final cohort of 305 patients (Figure 1). Of these, 43 patients (14.1%; 95% CI: 10.4%-18.5%) developed AL. The median time of occurrence was 11 days (interquartile range (IQR): 7.5-15.5) post-operation, and with 46.5% requiring a second surgery. The characteristics of patients who developed AL differed significantly from those who did not. For example, those with AL had higher ECOG scores (65.1% vs 43.1%, P = 0.008), greater surgical complexity (58.1% vs 35.5%, P = 0.007), increased lymph node positivity (79.1% vs 37.0%, P < 0.001), and higher postoperative CRP levels (125 [111-169.4] vs 86.6 [64.7-105.2], P < 0.001). Detailed differences in patient characteristics between AL and non-AL groups are provided in Table 1 and Supplemental Table S2. The flow chart of the study Clinical Characteristics of Patients Abbreviations: SD, standard deviation; IQR, interquartile range; FIGO, International Federation of Gynecology and Obstetrics.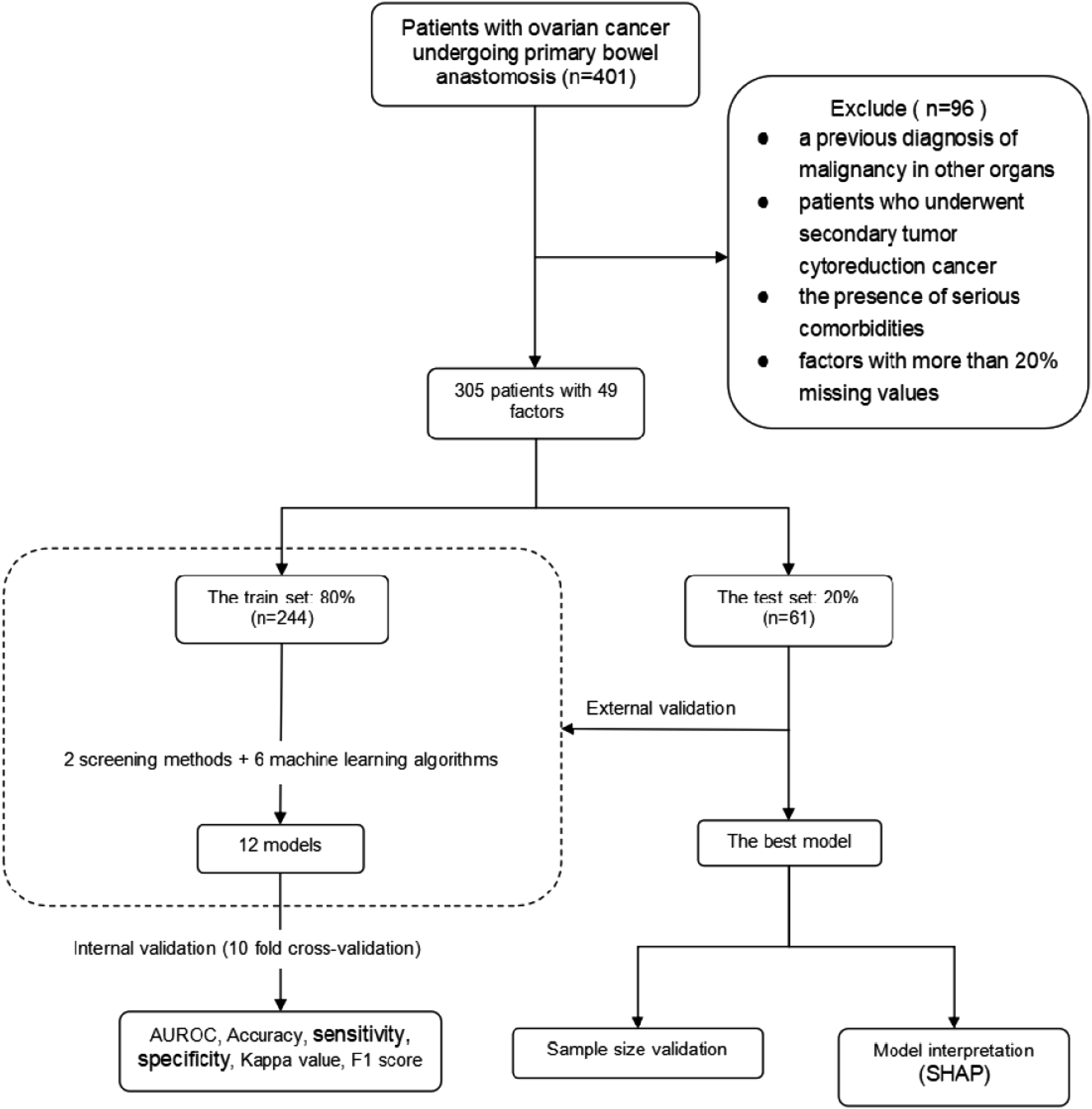
Economic Analysis
As shown in Table 1, patients who developed AL experienced significantly longer hospital stays (40 [29-55] vs 22 [19-28] days), higher hospital costs (121,487.7 [96,462.5-152,523] vs 78,983 [63,222.6-96,594.8] RMB), and longer time to chemotherapy initiation (34 [25-52.5] vs 20 [14-29] days) compared to patients without AL. A rank correlation analysis further revealed statistically significant associations between AL and hospital stay (r = 0.466, P < 0.001), hospital costs (r = 0.399, P < 0.001), and time to chemotherapy (r = 0.313, P < 0.001). However, there was no statistically significant association between AL and surgical costs (r = 0.107, P = 0.09).
Feature Selection
Following data preprocessing and feature selection, five variables were retained in the LASSO regression analysis: ECOG score, N stage, blood urea nitrogen (BUN), postoperative CRP, and postoperative albumin. Additionally, univariate logistic regression retained eight variables: history of laparotomy, ECOG, surgical complexity score, type of intestinal resection, N stage, blood urea nitrogen, and postoperative albumin.
Comparisons of Model Performance
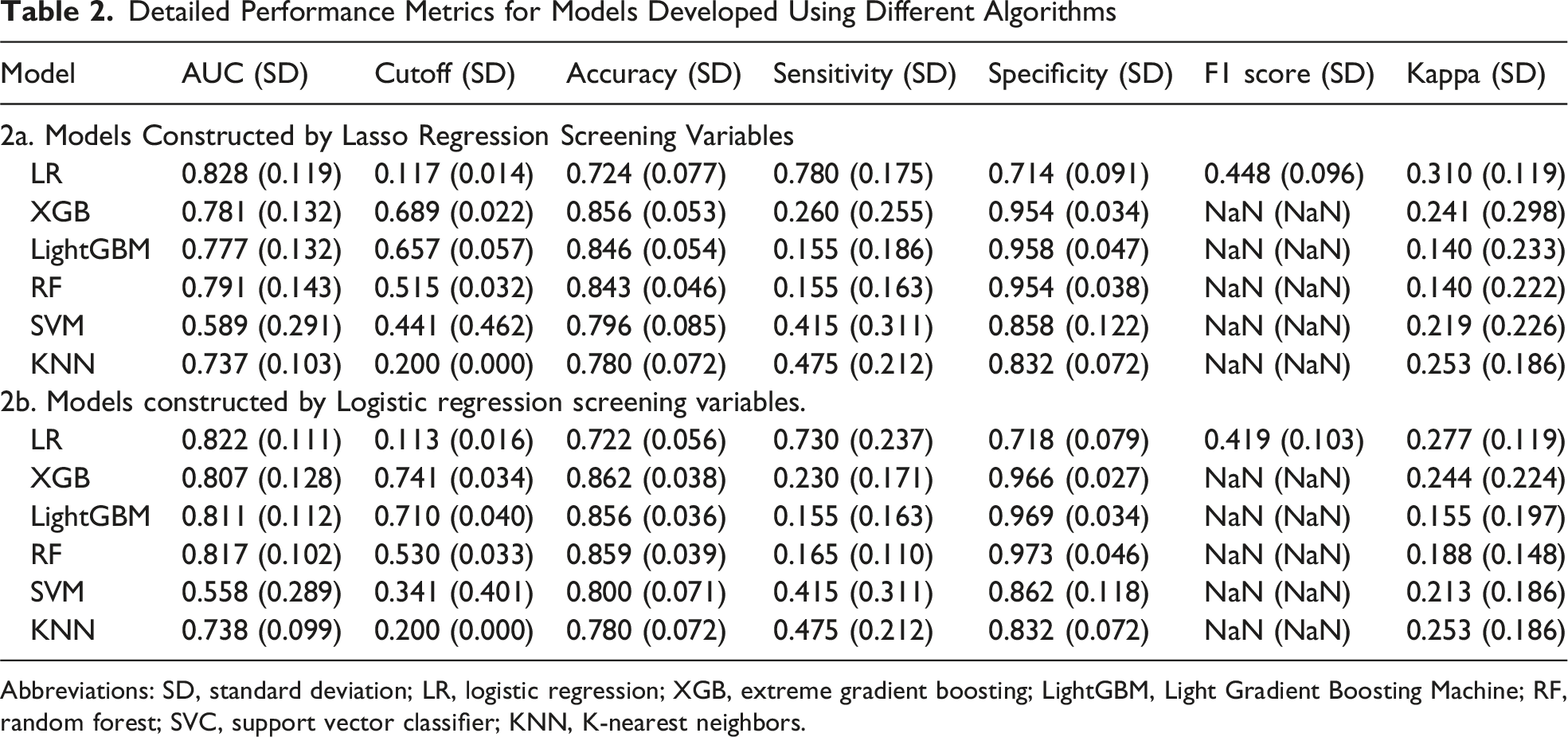
A total of 12 models were developed and validated using the test set, with performance metrics calculated for each. Figure 2 illustrates the predictive effectiveness of these models through receiver operating curves (ROC) and AUC values. The logistic regression model that employed LASSO for feature selection exhibited the highest predictive performance, achieving an AUC of 0.861 (±0.011) in the training set and 0.828 (±0.119) in internal validation. Detailed performance metrics for models developed using different algorithms are presented in Table 2. Summary of model performance: (A) Area Under the Curve (AUC) results for the six models constructed by Lasso regression screening variables. (B) Decision Curve Analysis (DCA) results for the six models constructed by Lasso regression screening variables. (C) AUC results for the six models constructed by Logistic regression screening variables. (D) DCA results for the six models constructed by Logistic regression screening variables. Abbreviations: XGBoost, extreme gradient boosting; LightGBM, Light Gradient Boosting Machine; SVC, support vector classifier; KNN, K-nearest neighbors Detailed Performance Metrics for Models Developed Using Different Algorithms Abbreviations: SD, standard deviation; LR, logistic regression; XGB, extreme gradient boosting; LightGBM, Light Gradient Boosting Machine; RF, random forest; SVC, support vector classifier; KNN, K-nearest neighbors.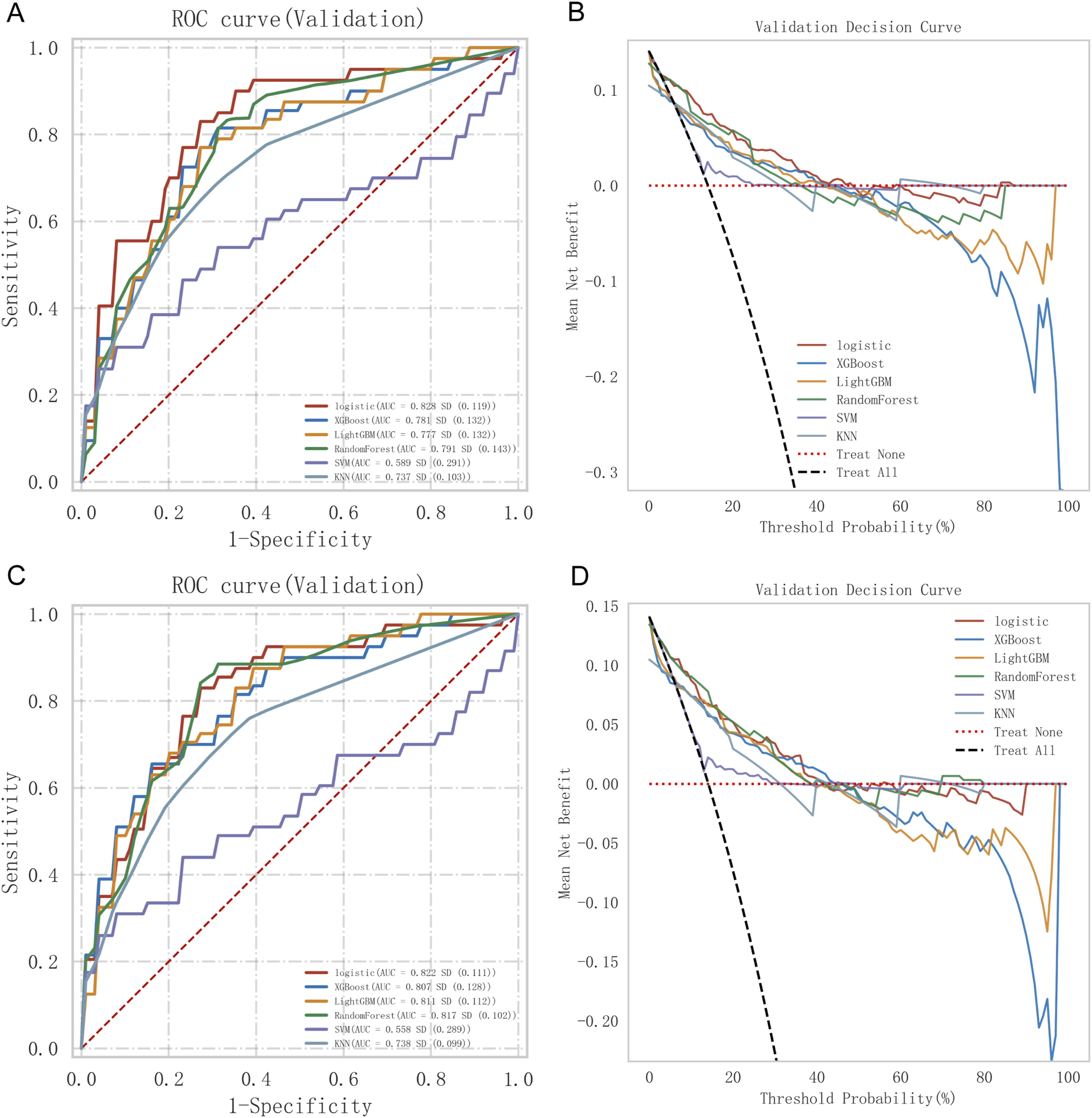
Model Interpretation
During external validation, the predictive model was evaluated using SHAP values to elucidate feature impact on AL prediction. Figure 3 shows that postoperative CRP, albumin levels, and N stage were the top three most influential factors in AL risk. A higher concentration of red samples in the region with positive SHAP values for CRP indicates that elevated CRP values contribute substantially to predicting AL. Variable contribution to the model by SHAP Value. (A) Summary of SHAP value of each variable. (B) Contribution of each feature value in one sample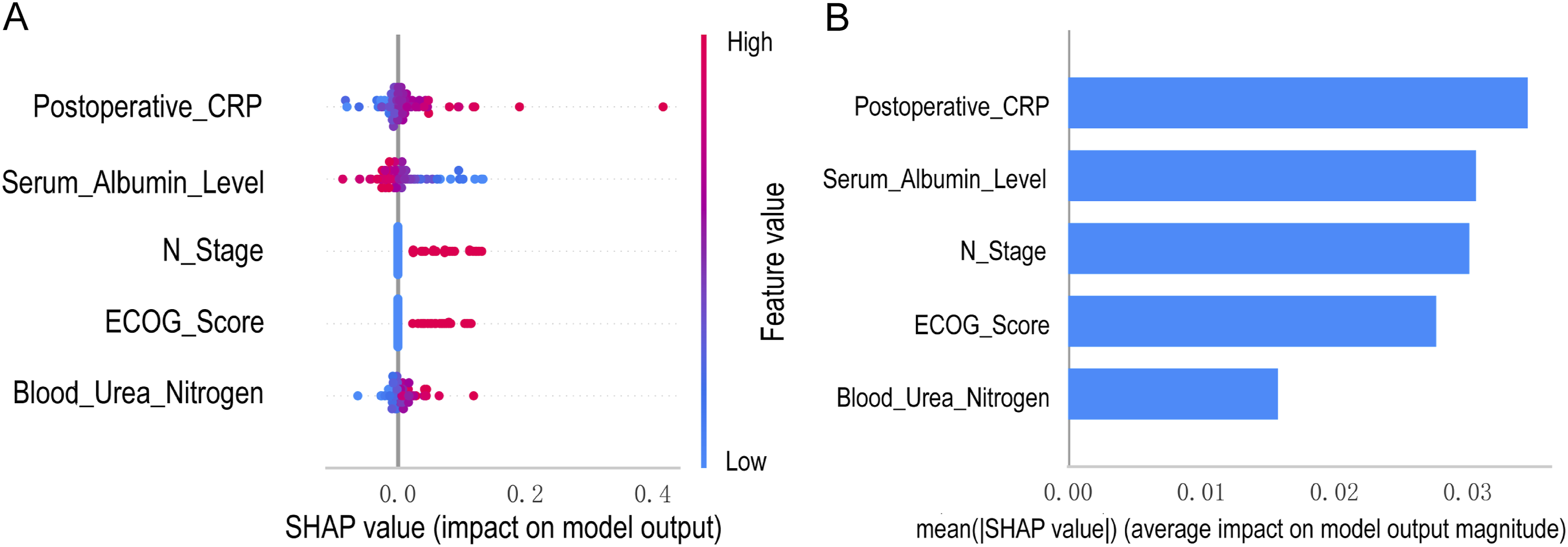
Discussion
At present, there is still a lack of consensus on the risk factors for anastomotic leakage following ovarian cancer surgery, which may be due to the low incidence rate and the heterogeneity of surgical techniques. 19 Our study emphasizes that postoperative CRP, albumin levels, N staging, ECOG score, and BUN are key factors in predicting AL, as confirmed by univariate and multivariate logistic regression analyses (Supplemental Table S3). Among these factors, postoperative CRP and albumin emerged as the most influential predictors, indicating that early postoperative inflammatory and nutritional status plays a dominant role in the development of anastomotic leakage. CRP is an acute phase reactant protein synthesized by the liver in the human body. Its plasma concentration increases with acute inflammation, infection, tissue injury, and cancer. CRP levels typically rise within 6 to 12 hours and reach a peak approximately 48 hours after the inflammatory stimulus, with the increase usually being proportional to the extent of tissue damage. 20 As a localized inflammatory complication, AL triggers a pronounced systemic inflammatory reaction, characterized by a rapid and persistent elevation in CRP levels among affected patients. In some clinical studies, CRP has been reported as an early predictor of postoperative infectious complications and anastomotic leakage following rectal resection surgery. 21 Serum albumin is a widely utilized biochemical marker in clinical practice that reflects both nutritional status and systemic inflammatory burden. It plays a critical role in postoperative tissue repair and the maintenance of immune function. Serum albumin levels typically decrease after inflammatory events such as surgery or acute stress. Low albumin levels usually indicate poor nutritional status, leading to tissue edema which is detrimental to wound healing. Studies have shown that a decrease in serum albumin concentration of ≥10 g/L is associated with a three-fold increase in overall postoperative complication risk. 22
Early postoperative CRP and albumin as dominant predictors of AL has important implications for clinical practice. These routinely available biomarkers facilitate early risk stratification following ovarian cancer cytoreductive surgery. Patients with elevated CRP and reduced albumin in the early postoperative period should be prioritized for enhanced surveillance, including timely imaging and closer clinical monitoring. In addition, these markers may guide postoperative management strategies, such as delayed oral intake, intensified nutritional support, and individualized recovery pathways.
Lymph node positivity typically reflects a more advanced depth of tumor invasion and a greater number of lymph nodes to be resected. This is often associated with increased surgical complexity and prolonged operative time. The latest clinical research has found that systemic lymphadenectom does not improve survival outcomes, but increases the risk of anastomotic leakage after ovarian cancer surgery by nearly four-fold, emphasizing the importance of limiting the scope of surgery. 23 The ECOG performance status is widely used in clinical settings to assess a patient’s physical function and ability to perform daily activities. Clinically, a high ECOG score often reflects underlying issues such as malnutrition, chronic comorbidities, impaired immune function, and delayed postoperative recovery-all of which may contribute to impaired tissue healing and reduced resistance to infection, thereby increasing the likelihood of AL occurrence. 24 To our knowledge, this was the first study to find that abnormal blood urea nitrogen is associated with an increased incidence of AL in ovarian cancer patients. BUN is a major end product of protein metabolism and is commonly used as a clinical indicator of glomerular filtration function. In the context of malignancy, higher BUN levels may indicate renal function damage and subclinical organ dysfunction, which is similar to the conclusions of colorectal cancer researches. 25
While evidence on the use of indwelling anal tubes in ovarian cancer is limited, previous studies in rectal cancer have demonstrated that anal tube placement may help prevent AL possibly by reducing intraluminal pressure at the anastomotic site. 26 In our study, neither protective stomas nor transanal tubes significantly reduced the incidence of AL, but they may still mitigate the severity of complications. However, protective stomas can be associated with additional risks, such as malnutrition, dehydration, severe psychological burden and a decreased quality of life. For these reasons, indwelling anal tubes have been proposed as an alternative to protective stomas. 27
Economic analysis revealed that AL significantly correlated with increased hospital stay length, higher hospitalization costs, and chemotherapy delays. However, no statistically significant association was observed with surgical costs, suggesting that the financial burden in AL cases primarily arises from medication and nursing care. Compared to patients without AL, the time from surgery to the first chemotherapy is significantly prolonged (20 days vs 34 days). The interval between surgery and adjuvant chemotherapy may provide an opportunity for micrometastasis to proliferate, Tewari conducted a randomized controlled study found that when the initiation of chemotherapy exceeds 25 days, the risk of death in patients with advanced ovarian cancer increases. 28
This study developed machine learning models from 305 ovarian cancer patients undergoing bowel resection, using 2 feature selection methods and six algorithms. The best-performing model achieved an AUC of 0.828 (SD: 0.119), demonstrating robust generalization. DCA indicated superior net clinical benefit. Compared to existing models (AUC: 0.64-0.78), our model exhibits competitive or superior performance.29,30
Study Strengths and Limitations
This study has several notable strengths. First, the multicenter design and relatively large sample size enhance the representativeness and generalizability of the findings within the context of ovarian cancer surgery. The relatively high rate of AL observed in this study may be attributed to the inclusion of patients undergoing ultra-radical cytoreductive surgery with bowel resection (a surgical approach proposed in 2013) as well as the high proportion of advanced-stage disease. Second, we incorporated a comprehensive set of clinical and laboratory variables, including novel and underexplored predictors such as indwelling transanal tubes, allostatic load, and BUN. By applying diverse ML techniques, we enhanced the statistical robustness of the analysis and developed a predictive tool applicable across the continuum of patient care, from preoperative evaluation to postoperative surveillance.
Nevertheless, several limitations should be acknowledged. First, although the model was developed using multicenter data, differences in institutional data structures and the limited sample size may still affect its stability. Second, some potential AL predictors, such as anastomotic tension, blood supply, and distance of the anastomosis from the anal verge, were not available in our data set and could not be evaluated.
Supplemental Material
Supplemental Material - Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage After Ovarian Cancer Surgery: A Multicenter Study
Supplemental Material for Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage After Ovarian Cancer Surgery: A Multicenter Study by Lianjie Miao, Bo Ding, Shanhu Qiu, Jingru Zhang, Ying Zhou, Zhen Shen, Yunxia Zhang, Yan Wang, and Yang Shen in The American Surgeon™.
Supplemental Material
Supplemental Material - Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage After Ovarian Cancer Surgery: A Multicenter Study
Supplemental Material for Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage After Ovarian Cancer Surgery: A Multicenter Study by Lianjie Miao, Bo Ding, Shanhu Qiu, Jingru Zhang, Ying Zhou, Zhen Shen, Yunxia Zhang, Yan Wang, Yang Shen in The American Surgeon™.
Supplemental Material
Supplemental Material - Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage After Ovarian Cancer Surgery: A Multicenter Study
Supplemental Material for Postoperative Inflammatory and Nutritional Biomarkers for Predicting Anastomotic Leakage Aftter Ovarian Cancer Surgery: A Multicenter Study by Lianjie Miao, Bo Ding, Shanhu Qiu, Jingru Zhang, Ying Zhou, Zhen Shen, Yunxia Zhang, Yan Wang, Yang Shen in The American Surgeon™.
Footnotes
Acknowledgments
We are grateful to the staff in Biobank of Zhongda Hospital Affiliated to Southeast University for technical assistance.
Ethical Considerations
Consent to Participate
Given the study’s retrospective design, informed consent was not required.
Author Contributions
LM was responsible for developing the models and drafting the manuscript. BD, JZ, YZ, ZS, and YXZ undertook data collection. YS and YW contributed expertise in clinical study design and provided primary oversight of the analyses. SQ participated in the literature review and validation of statistical results. The initial draft was viewed by all the authors, who subsequently approved the final manuscript. LM, BD, SQ, JZ, YZ, ZS, YXZ,YW and YS had access to and verify the underlying study data. YS had final responsibility for the decision to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (grant numbers 2025ZD0545600), The National Clinical Key Discipline Construction Funds (grant numbers Gynecology czxm-zk-40), National Natural Science Foundation of China (grant numbers 82372126, 82072078), Zhongda Hospital Affiliated to Southeast University, Jiangsu Province High-Level Hospital (grant numbers 2023GSPKY11), and Xinjiang Uygur Autonomous Region Natural Science Foundation (grant numbers 2021D01A43).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset, code, and algorithm files used in this study are not publicly available. However, the data generated in this study are available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.