
Abstract
Background
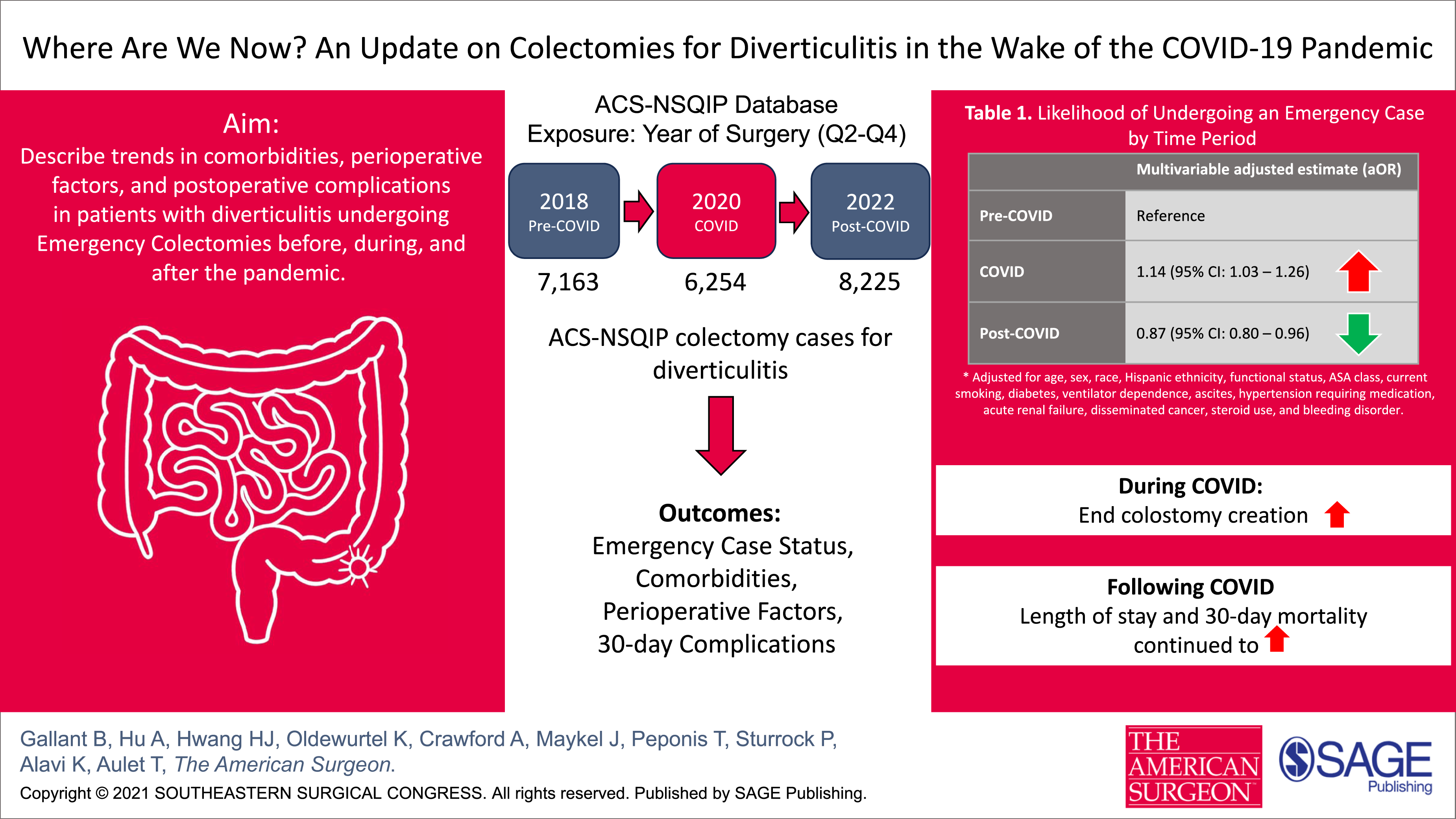
The COVID-19 pandemic strained hospital systems and post-pandemic data on colectomy trends for diverticulitis are limited. We aimed to describe trends in colonic resections in patients with diverticulitis before, during, and after the pandemic.
Methods
This retrospective cohort study queried the American College of Surgeons NSQIP database, analyzing patients who underwent a colectomy for diverticulitis during quarters 2-4 (April 1-December 31) in 2018 (“pre-COVID”), 2020 (“during COVID”), and 2022 (“post-COVID”). The primary study outcome was emergency case rates during the 3 time periods. Secondary outcomes included trends in patient comorbidities, severity of presenting illness, 30-day postoperative complications, and disposition status.
Results
A total of 21,642 patients were studied (7163 pre-COVID, 6254 during COVID, and 8225 post-COVID). Emergency cases of diverticulitis increased to 21% during the COVID period but remained at 17% and 18% during the pre-COVID and post-COVID periods, respectively (P < 0.001). Similarly, end colostomy creation rates rose to 20% during COVID and returned to baseline levels (18%) after the pandemic (P < 0.001). Hospital length of stay and 30-day mortality increased during the COVID period and remained slightly elevated post-COVID.
Conclusions
The COVID-19 pandemic was associated with a temporary increase in emergency colectomies and end colostomy creations for diverticulitis, with operative urgency returning to pre-pandemic levels in the post-COVID period. Short-term postoperative outcomes also shifted modestly during and after the pandemic. These findings offer a national perspective on trends in the surgical management of diverticulitis during and after the pandemic and may help guide surgical practice during future health care disruptions.
Key Takeaways
• Emergency colectomy and end colostomy creation rates for diverticulitis increased during the COVID-19 pandemic but returned to near pre-pandemic levels in the post-pandemic period. • Several short-term postoperative outcomes differed during and after the pandemic, including modest changes in length of stay, mortality, and readmissions related to the index surgery. • These findings offer a national perspective on trends in the surgical management of diverticulitis during and after the pandemic and may help guide surgical practice during future health care disruptions.
Introduction
The World Health Organization officially declared COVID-19 a global pandemic in March 2020. By August 2020, COVID-19 had become the third leading cause of death in the United States, with daily fatalities exceeding 1000 and nationwide cases surpassing 5 million. As of July 2025, COVID-19-related deaths have exceeded 7 million worldwide and 1.2 million in the United States. 1
Not surprisingly, the COVID-19 pandemic placed a substantial strain on health care institutions across the United States. 2 There was considerable concern among health care professionals that these constraints would result in significant delays in care and worse outcomes for patients with various disease conditions. Nationwide, non-emergency surgeries were canceled, leading to immediate and long-term impacts on access to surgical care and worse patient outcomes.3,4
During the acute phase of the pandemic, several studies reported a decrease in hospitalizations and surgical volume among patients with diverticulitis, accompanied by a significant increase in the severity of presenting illness and rates of emergency surgeries compared with pre-pandemic levels.5,6,7,8,9 Furthermore, patients requiring emergency surgeries during the pandemic were more likely to have significant comorbidities at baseline, suggesting that limited access to timely care may have led to more severe presentations. 6
Previous studies have demonstrated an increase in both emergency operations and the severity of presenting illness related to diverticulitis during the pandemic; however, less is known about trends following the pandemic. This study aimed to describe nationwide trends in colectomies in patients with diverticulitis before, during, and after the pandemic, using the NSQIP database. We hypothesized that compared to the pandemic period, post-pandemic years would demonstrate a return to pre-pandemic distributions of emergency vs elective colectomy and postoperative outcomes among patients undergoing surgery for diverticulitis.
Methods
Study Design
We performed a retrospective cohort study utilizing data from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP). Adult patients who underwent a colectomy for diverticulitis during quarters 2-4 (April 1 to December 31) of 3 representative calendar years, namely, 2018 (“pre-COVID”), 2020 (“during COVID”), and 2022 (“post-COVID”), were included. These specific months and years were selected to reflect surgical practice patterns for colectomies performed for diverticulitis before, during, and after the peak impact of the COVID-19 pandemic on hospital systems in the United States.
Setting
The ACS NSQIP is a nationally validated database that includes de-identified, prospectively collected clinical data from participating hospitals across the United States. Hospitals contributing to NSQIP include academic, community, and private institutions, allowing for a nationally representative sample of surgical patients.
Participants
Eligible participants were adults (age ≥18 years) who underwent colectomy for diverticulitis. Patients were identified in the ACS NSQIP database using relevant Current Procedural Terminology (CPT) codes (Appendix A). Patients were included if their primary indication for surgery was diverticulitis, as defined in NSQIP’s Targeted Colectomy Participant Use Data File user guide.
Exposure Variable
The primary exposure was the year of surgery, categorized as pre-COVID (quarters 2-4, 2018, control year), during COVID (quarters 2-4, 2020), or post-COVID (quarters 2-4, 2022, control year). Control years, 2018 and 2022, were chosen based on a prior publication to account for any COVID impact on health institutions in late 2019 or early 2021. 6
Outcomes
The primary outcome was emergency case status rates across the 3 time periods, as defined by NSQIP’s emergency case designation. Secondary outcomes included patient comorbidities, severity of presenting illness, reason for emergency surgery, surgical approach, end colostomy creation rates, 30-day postoperative complications, and disposition status across the 3 time periods. Additional patient- and procedure-level variables included the patient’s age, sex, race, body mass index (BMI), and American Society of Anesthesiologists (ASA) class. Thirty-day complications included superficial and organ space surgical site infections (SSIs), wound disruption or dehiscence, postoperative pneumonia, unplanned intubation, pulmonary embolism, failure to wean from ventilator >48 hours, urinary tract infections, stroke, myocardial infarction, sepsis, septic shock, reoperation, readmission, or mortality.
Statistical Analysis
Continuous variables are shown as mean with standard deviation and were compared using one-way analysis of variance (ANOVA). Categorical variables are shown as proportions and were compared using Chi-square tests. A multivariable adjusted logistic regression analysis examining between-period differences in emergency case status was carried out using backward selection, beginning with all variables with P < 0.20 in the univariate association, and retaining all variables with P < 0.05 in the final model. No patients were excluded due to missing data. Variables with >10% missingness (race and ethnicity) were retained by coding missing values as separate categories. Since all other variables had <10% missingness, no formal imputation was performed. All statistics were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
IRB Exemption
Since this study analyzed only de-identified, publicly available data, it was deemed exempt from Institutional Review Board approval.
Results
Study Population Characteristics
Study Population Characteristics by Time Period
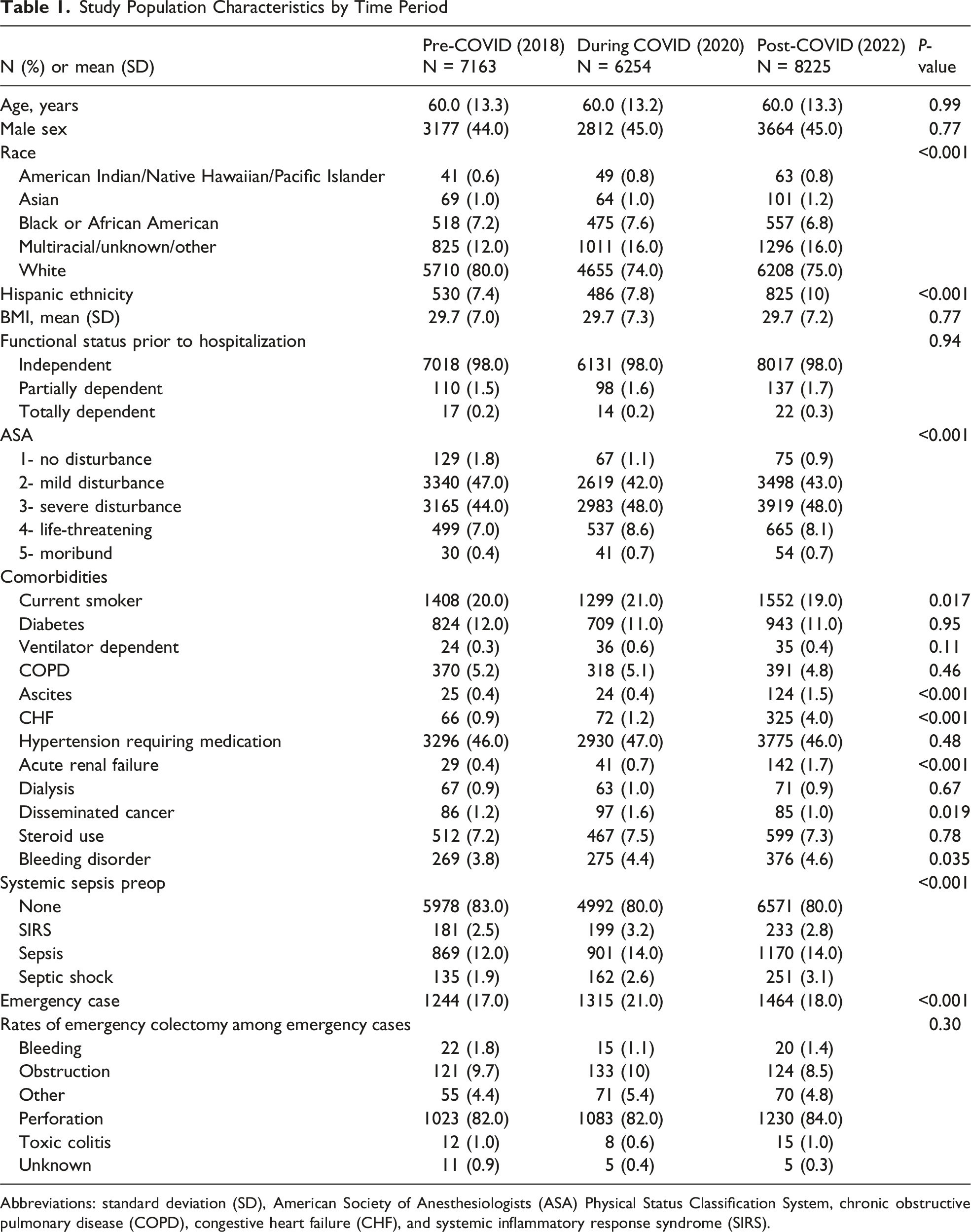
Abbreviations: standard deviation (SD), American Society of Anesthesiologists (ASA) Physical Status Classification System, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), and systemic inflammatory response syndrome (SIRS).
Patient Demographics
Across the 3 time periods, there were no significant differences in the rates of colon resection for diverticulitis by age (60 years) or sex (44-45% male). There was a significant difference among the various races that underwent a colonic resection across the 3 time periods (P < 0.001) (Table 1). Colon resections for black individuals slightly increased (7.2% to 7.6%) from pre-COVID to COVID, which then receded below pre-pandemic levels (6.8%). The proportion of colonic resections among white individuals decreased from 80% pre-COVID to 74% during COVID, before slightly increasing to 75% in the post-COVID period. Across the 3 time periods, the proportion of colonic resections for Hispanic individuals persistently increased (from 7.4% to 10%).
Patient Comorbidities
During the COVID era, there was a greater proportion of patients with significant comorbidities who underwent a colonic resection for diverticulitis (Table 1). A greater proportion of ASA class 4 patients underwent colonic resection for diverticulitis during the COVID era. Current smokers and patients with disseminated cancer were also more likely to undergo resection during the pandemic, whereas acute renal failure, ascites, bleeding disorders, and CHF were more common in the post-COVID period.
Emergency Case Status
Likelihood of Undergoing an Emergency Case by Time Period
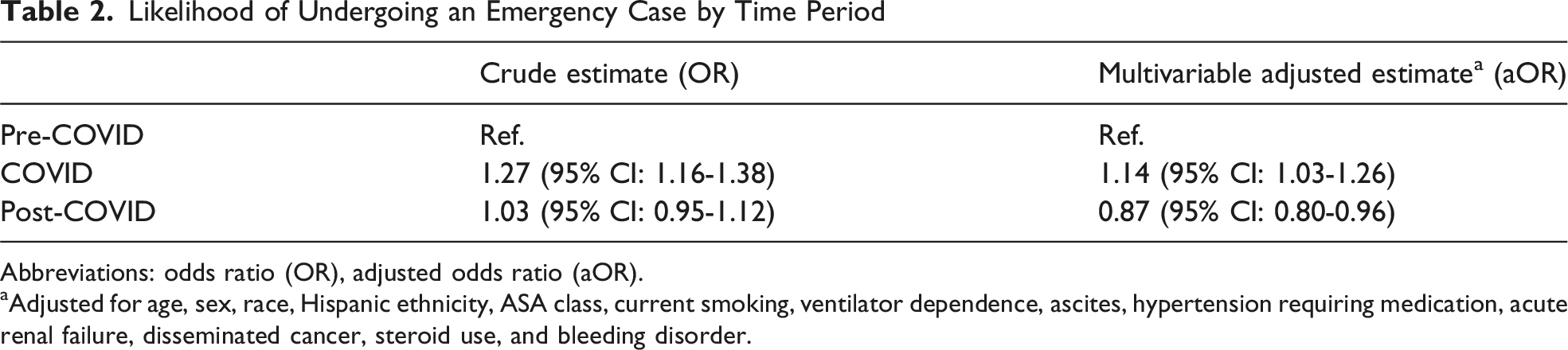
Abbreviations: odds ratio (OR), adjusted odds ratio (aOR).
aAdjusted for age, sex, race, Hispanic ethnicity, ASA class, current smoking, ventilator dependence, ascites, hypertension requiring medication, acute renal failure, disseminated cancer, steroid use, and bleeding disorder.
Perioperative Factors
Preoperatively, a greater proportion of patients presented with sepsis during and after the COVID pandemic compared to before. The proportion of patients diagnosed with septic shock preoperatively increased during the COVID period and continued to rise in the post-COVID period.
Intraoperative Factors
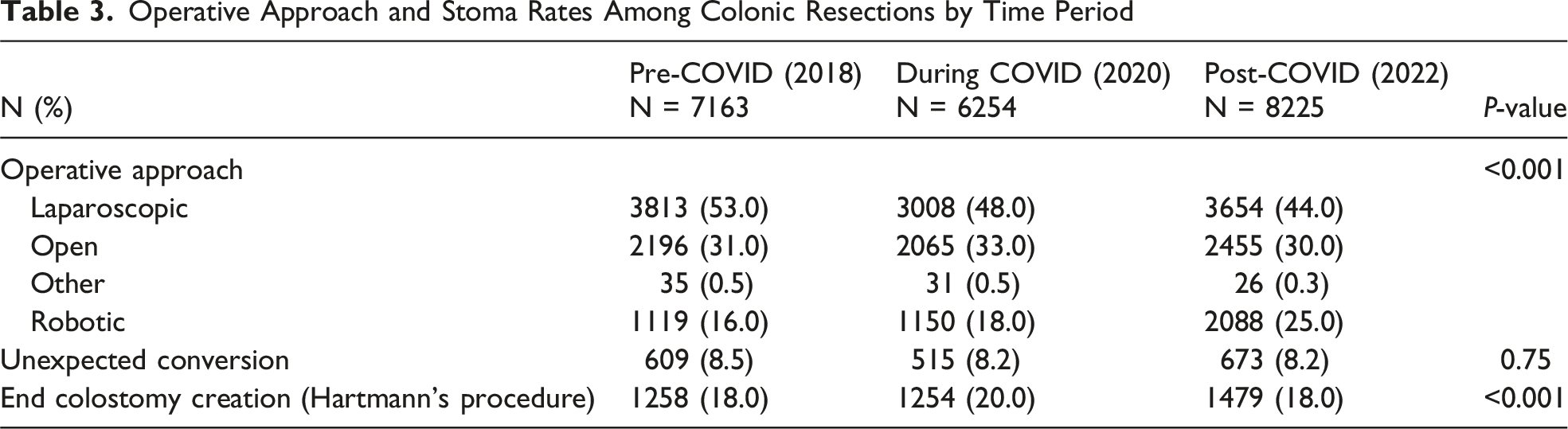
Operative Approach and Stoma Rates Among Colonic Resections by Time Period
Postoperative Complications
30-Day Postoperative Complications and Disposition Status by Time Period
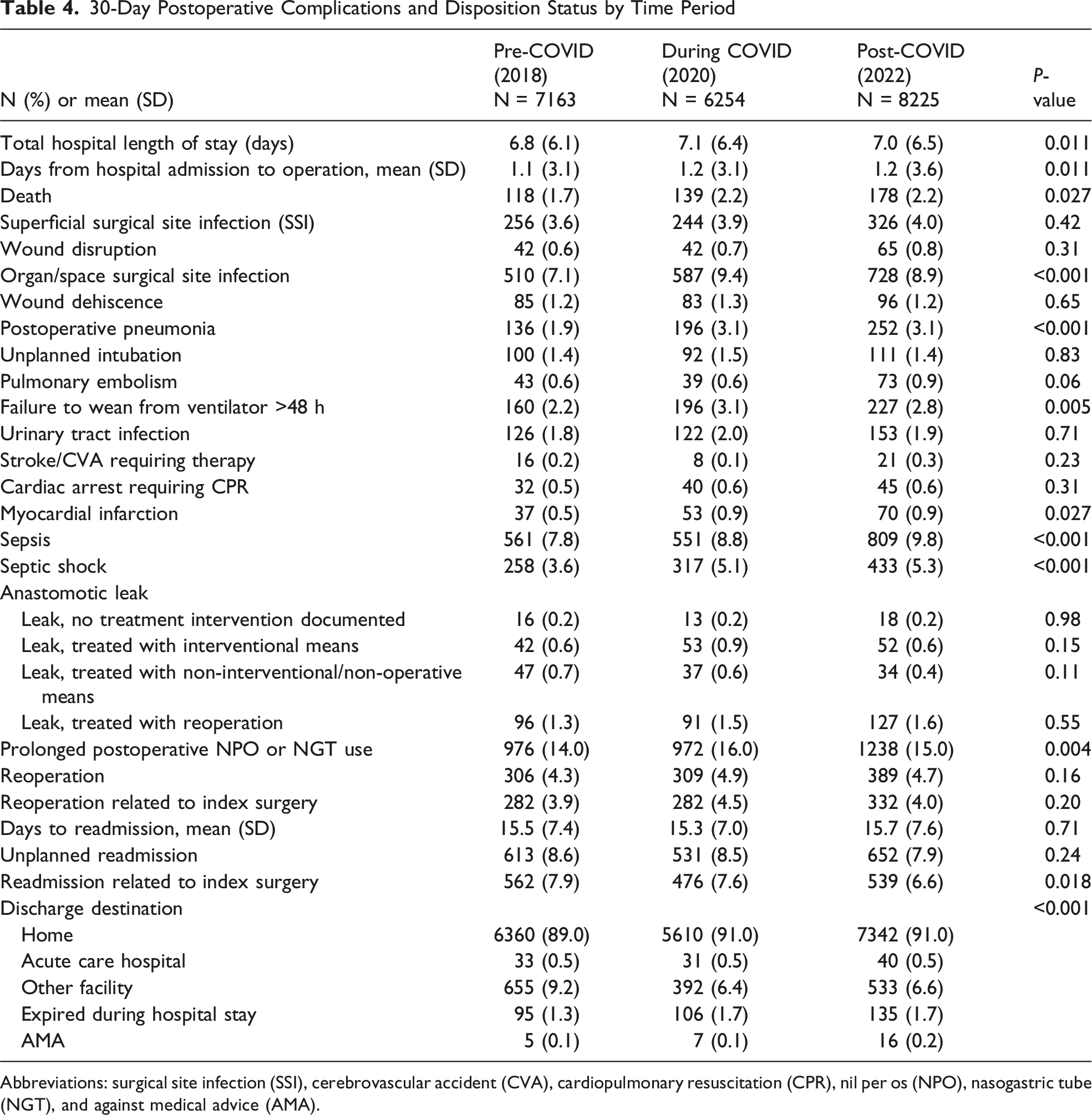
Abbreviations: surgical site infection (SSI), cerebrovascular accident (CVA), cardiopulmonary resuscitation (CPR), nil per os (NPO), nasogastric tube (NGT), and against medical advice (AMA).
Discussion
This study demonstrates that following the COVID-19 pandemic, although there was an overall increase in the total number of colectomies performed for diverticulitis, the proportion of emergency cases has returned to pre-pandemic levels. In many other pathologies, the literature has shown that the COVID pandemic caused interruptions in clinical care, leading to delays in treatment and altered health care-seeking behavior, resulting in increased severity at presentation and worse outcomes for both acute and chronic conditions.10,11 However, the long-term implications of these delays remain an active area of investigation.
Previous studies have reported similar patterns in emergency colonic resection rates for diverticulitis when comparing pre-COVID pandemic and COVID pandemic periods5,6,7,8,9,12; however, these trends do not appear to be consistent across other disease pathologies. One study demonstrated that patients with inflammatory bowel disease were less likely to undergo an emergency operation in 2020 than in 2019. 13 These differences likely reflect underlying pathophysiological differences in disease course and the thresholds at which operative intervention is pursued. The increased rates of emergency colectomies and end colostomy creations during the COVID pandemic may be attributed to several factors. Studies have suggested that the rise in emergency cases during the pandemic may reflect increased use of conservative management and delays in care, as patients avoided seeking medical attention or were unable to undergo elective resections, potentially allowing disease progression.6,8,9,14,15,16 Our multivariable logistic regression model supports these findings and suggests that, after adjusting for demographic and perioperative factors, the increase in emergency vs elective colonic resections during the COVID period was temporary, with case mix returning toward pre-pandemic levels post-COVID.
Another plausible explanation for the higher rates of emergency colonic resection and end colostomy creation during the pandemic may be the direct effects of coronavirus infection on disease severity. Unfortunately, the diagnosis of COVID-19 at the time of colonic resection was not available for all 3 time periods in the NSQIP database. Recent studies have demonstrated a possible link between acute diverticulitis and COVID-19 infection.6,17,18 These studies suggest that the COVID-induced chronic inflammatory state may cause inflammation-mediated tissue damage, leading to increased intestinal edema and promoting bacterial overgrowth, which could result in acute diverticulitis and intestinal perforation. However, we did not detect a significant difference in indications, including perforation, for emergency colectomy cases in patients with diverticulitis before, during, and after the COVID pandemic.
Similar to other studies, our findings demonstrated that more patients underwent an open operative approach, including procedures involving end colostomy creation, during the COVID-19 pandemic, likely reflecting a transient rise in emergency cases. 14 This increase in the proportion of open operative approaches and end colostomy creations was observed only during the pandemic. Laparoscopic cases steadily decreased, while robotic approaches significantly increased throughout the study period. These findings highlight a broader evolution in the management of diverticulitis, including the adoption of minimally invasive techniques and more individualized surgical decision-making. 19 Another plausible explanation for the transient increase in open procedures and end colostomy rates during the COVID period was reduced access to colorectal surgeons. While this cannot be discerned through NSQIP, subspecialty-trained colorectal surgeons may be more likely to employ minimally invasive techniques and perform primary anastomosis, in keeping with the American Society of Colon and Rectal Surgeons clinical practice guidelines on diverticulitis. 20 Finally, another plausible explanation for the transient rise in open procedures is that early in the pandemic, there was concern regarding potential SARS-CoV-2 transmission via aerosolization during laparoscopic insufflation, leading many surgeons to favor open approaches during this period.21,22
Postoperative outcomes varied modestly across the study periods. During the COVID period, higher rates of organ space infections and prolonged ventilator dependence were observed, whereas the post-COVID era showed slight increases in pneumonia, sepsis, and septic shock. Despite a transient rise in emergency cases, reoperation rates did not differ significantly across the study periods. We also observed a modest increase in 30-day mortality between the pre-COVID and COVID periods, which aligns with findings from prior studies.8,14 Our analysis extends these observations by including data from the post-COVID era. Although emergency colectomy rates returned toward pre-pandemic levels, 30-day mortality and hospital length of stay remained modestly elevated following the pandemic. These patterns may reflect the persistent increase in illness severity among patients undergoing colectomy during and after the pandemic. While this study cannot assess outpatient access to care or delays in presentation, we only observed slight increases in the time from hospital admission to surgery across the time periods. These findings provide additional context for the patterns of postoperative outcomes among patients undergoing colectomy for diverticulitis before, during, and after the COVID-19 pandemic.
In our study, we observed a continued trend of patients being discharged home rather than to post-acute care facilities, a pattern that emerged during the COVID period and persisted thereafter. This finding aligns with a prior NSQIP analysis demonstrating decreased discharges to post-hospitalization facilities despite increased emergency colonic resections during the pandemic. 23 Our findings expand on this work by providing additional context for discharge practices during and after the COVID period.
Study Strengths and Limitations
Strengths of this study include the use of the NSQIP database, which enabled us to evaluate trends in colonic resections for diverticulitis across the pre-COVID, COVID, and post-COVID periods. Additionally, the month-matched analysis, including only quarters 2-4, aligns the study periods with the onset of the pandemic and accounts for the known seasonality of diverticulitis, strengthening the validity of the analysis. To our knowledge, this is the first study to characterize post-pandemic trends in the surgical management of diverticulitis at a national level. Specifically, we document that emergency colonic resections for diverticulitis returned to pre-pandemic levels following temporary disruptions caused by the pandemic, with only modest differences observed in select postoperative outcomes.
This study has several limitations that should be considered when interpreting our findings. First, it is retrospective and relies on data from the NSQIP database, which may not capture all relevant clinical variables, including COVID-19 infection status, disease recurrence, or details of outpatient management. Next, unmeasured confounding factors may have influenced the designation of emergency status, such as hospital triage policies, surgeon preferences, or regional case surges during the pandemic. Finally, NSQIP does not capture outpatient access, non-operative management, or the direct effects of lockdown policies, so we were unable to assess whether system-level improvements or timely clinical evaluation influenced the management of diverticulitis across the 3 time periods.
To our knowledge, this is the first nationwide study to report post-pandemic trends in colon resections for diverticulitis and to demonstrate a return to pre-pandemic levels of emergency cases. Our findings show that although the proportion of emergency cases and the rates of end colostomy creation increased during the COVID period, operative urgency returned to pre-pandemic levels in the post-COVID era, while several short-term postoperative outcomes differed modestly across the study periods. These results provide national-level context for patterns in the surgical management of diverticulitis before, during, and after the pandemic and may help guide surgical practice during future health care disruptions.
Footnotes
Acknowledgments
American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Author Contributions
Dr. Gallant and Dr. Aulet were responsible for conceptualization, investigation, methodology, resources, writing—original draft, writing—review and editing, and validation. Ms. Crawford conducted the formal analysis and assisted with writing—review and editing. Dr. Peponis, Dr. Sturrock, Dr. Alavi, and Dr. Maykel contributed to investigation, methodology, and writing—review and editing. Dr. Hu, Dr. Oldewurtel, and Mr. Hwang contributed to methodology and writing—review and editing. All authors provided substantial contributions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1-TR001453. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Meeting Presentation
E-poster presentation at the American Society of Colon and Rectal Surgeons meeting (ASCRS), May 10-13, 2025, San Diego, CA.
IRB Approval
Since this study analyzed only de-identified, publicly available data, it was deemed exempt from approval by the University of Massachusetts Chan Medical School Institutional Review Board.
Appendix
The following CPT procedure codes were included: 44140, 44141, 44143, 44144, 44145, 44146, 44147, 44150, 44151, 44160, 44204, 44205, 44206, 44207, 44208, and 44210.