
Abstract
Background
Contemporary rectal cancer management increasingly relies on MRI-based risk stratification to identify low-risk cT3 tumors that may avoid neoadjuvant therapy. This meta-analysis compared upfront total mesorectal excision with neoadjuvant therapy in MRI-defined low-risk cT3 rectal cancer.
Methods
PubMed, Scopus, and Cochrane Central were systematically searched through June 2025. Pooled odds ratios (ORs), mean differences (MDs), and hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated using random-effects models. Heterogeneity was assessed with the I2 statistic. Analyses were performed using R (version 4.4.2). A complementary Bayesian random-effects meta-analysis was performed to explore posterior uncertainty and potential equivalence between strategies.
Results
Five studies, including 1447 patients, were analyzed. Upfront surgery was associated with shorter operative time (MD −25.7 min; 95% CI −38.6 to −12.7) and more lymph nodes retrieved (MD 6.6; 95% CI 6.0-7.3). No significant differences were observed in perioperative complications, including anastomotic leaks, intra-abdominal abscesses, or reoperations. Oncologic outcomes were comparable, including circumferential resection margin positivity (CRM+) (OR 1.05; 95% CI 0.49-2.26), local recurrence (OR 0.99; 95% CI 0.58-1.70), and distant recurrence (OR 1.03; 95% CI 0.64-1.65). Survival outcomes were also similar, with no differences in disease-free (DFS) or overall survival (OS). Bayesian analyses supported these findings, with effect estimates centered around the null and probabilities of superiority close to equipoise, indicating inconclusive evidence.
Conclusion
In MRI-defined low-risk cT3 rectal cancer, upfront TME may provide oncologic outcomes comparable to neoadjuvant therapy. However, the available evidence remains exploratory and insufficient to support definitive treatment recommendations.
Keywords
Introduction
Colorectal cancer represents a major global health burden, consistently ranking among the most frequently diagnosed malignancies and remaining 1 of the leading causes of cancer-related mortality worldwide.1,2,3 Rectal cancer accounts for approximately 28% of large bowel neoplasms, and in symptomatic presentations, locally advanced tumors are more commonly encountered.2,3,4 Although neoadjuvant chemoradiotherapy remains a standard strategy for locally advanced rectal cancer, contemporary management increasingly relies on MRI-based risk stratification to individualize treatment selection according to mesorectal fascia status, extramural venous invasion, nodal disease, depth of extramural spread, and tumor location.3,4,5,6,7,8,9,10,11,12,13,14,15,16 Nevertheless, its role in patients without threatened mesorectal fascia, particularly those staged as cT3N0, remains incompletely elucidated.4,6,9,12,13,14
Despite neoadjuvant treatment improving local control and disease-free survival, its impact on overall survival remains uncertain.6,16,17 Moreover, chemoradiotherapy carries significant toxicity, including fecal incontinence, bowel dysfunction, and sexual impairment, all of which adversely affect quality of life.6,9,11,13,16 For selected patients with cT3 rectal cancer, upfront TME may be sufficient, as the risk of local recurrence is reported to be below 3%, thereby sparing patients from the adverse effects of radiotherapy.6,14,16,17 Advances in high-resolution pelvic magnetic resonance imaging now allow objective assessment of circumferential resection margin (CRM) involvement before surgery.6,8,9,14,16,17 Threatened mesorectal fascia (≤1 mm) and extramural venous invasion are considered major high-risk MRI features associated with adverse oncologic outcomes, whereas in cT3 tumors with a clear mesorectal margin (≥2 mm from the fascia), TME alone may be a reasonable alternative to neoadjuvant therapy.6,14,16,17,18,19
To our knowledge, no previous meta-analysis has directly compared upfront surgery and neoadjuvant therapy in patients with cT3 rectal cancer. The present study was designed to specifically evaluate cT3 tumors and clear mesorectal fascia (MRF), without involvement of the anorectal ring. Our aim was to evaluate whether upfront TME may represent a feasible treatment strategy for carefully selected MRI-defined low-risk cT3 rectal cancer compared with neoadjuvant therapy followed by surgery.
Methods
This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 20 as outlined in Supplemental Table S1. The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the identification number CRD420251161495. 21
Systematic Search Process
We conducted a broad literature search using PubMed, the Cochrane Central Register of Clinical Trials, and Scopus to identify studies published until June 2025. The PubMed search strategy was as follows: (“rectal cancer” [tiab] OR “rectal neoplasms” [MeSH]) AND (“surgery alone” [tiab] OR “total mesorectal excision” OR “abdominoperineal resection” OR “lower anterior resection”) AND (“neoadjuvant chemoradiotherapy” OR “preoperative chemoradiotherapy” OR “neoadjuvant treatment” [tiab] OR “neoadjuvant therapy”). The Scopus and Cochrane strategies used simplified terms, as follows: (“rectal cancer”) AND (“surgery alone” OR “total mesorectal excision” OR “abdominoperineal resection”) AND (“neoadjuvant chemoradiotherapy” OR “preoperative chemoradiotherapy”).
Study Selection Criteria
We included comparative observational studies evaluating upfront surgery vs neoadjuvant therapy followed by total mesorectal excision (NEO + TME) in adults with mid or low rectal adenocarcinoma, with no language restrictions. The analysis was restricted to studies reporting outcomes in patients with cT3 rectal cancer and clear mesorectal fascia (MRF). However, definitions of sphincter involvement were not uniformly reported across studies, and eligibility was therefore based primarily on MRF status and tumor location. Exclusion criteria were as follows: (1) watch-and-wait strategies after neoadjuvant treatment; (2) local excision or transanal procedures; (3) studies evaluating radiotherapy alone in the neoadjuvant setting; (4) non-comparative reports (single-arm studies, case reports, or case series); and (5) non-original publications (conference abstracts, reviews, editorials, letters, or animal studies).
Data Extraction and Endpoints
Two reviewers (B.F.P. and G.L.B.) independently screened the studies and extracted data from those that met the inclusion criteria. Discrepancies were resolved by consensus or, if necessary, a third reviewer (F.B.F.) provided adjudication. The following intraoperative and postoperative outcomes were evaluated: (1) operative time (OT), (2) lymph node harvested, (3) intraoperative blood loss, (4) anastomotic leak, (5) intrapelvic abscess, (6) reoperation (7) positive circumferential margin (CRM+), (8) local recurrence, (9) distant recurrence, (10) 3-year disease-free survival (DFS), (11) 5-year disease-free survival (DFS), and (12) 3-year overall survival (OS).
Quality Assessment
Two reviewers (B.F.P. and G.B.L.) independently assessed the quality of the included studies using the Revised Cochrane Risk-of-Bias Tool (ROBINS-I) for non-randomized control trials. 22 In this assessment, each study was categorized as critical, serious, moderate, or low risk in the 7 domains: confounding, selection, classification, deviations from intended interventions, missing data, measurement of outcome, and selection of reported results. Disagreements were resolved by consensus, with arbitration by a third reviewer (F.B.F.) when required. The certainty of evidence for each outcome was rated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework, with levels of confidence classified as very low, low, moderate, or high. 23
Statistical Analysis
Binary outcomes were expressed as odds ratios (ORs) with 95% confidence intervals (CIs), and continuous variables as mean differences (MDs), also presented with 95% CIs. When continuous data were reported as median and range or interquartile range (IQR), the corresponding mean and standard deviation (SD) were estimated using the methods proposed by Luo et al (2018) and Wan et al (2014), respectively.24,25 For time-to-event outcomes, hazard ratios (HRs) and their corresponding standard errors were extracted directly when reported. When HRs were not available, they were estimated from published Kaplan–Meier curves using digital extraction (WebPlotDigitizer) and reconstructed according to the methods described by Tierney et al (2007). 26 Random-effects models were applied using the restricted maximum likelihood (REML) method. A P-value less than 0.05 indicates rejection of the null hypothesis. Heterogeneity was assessed using the Cochran Q test and the I2 statistic; I2 values greater than 25%, and P-values less than 0.10 were interpreted as indicative of substantial heterogeneity. Statistical analyses were performed using R software version 4.4.2.
Sensitivity Analysis
For outcomes with substantial heterogeneity (I2 ≥ 25%), we performed additional sensitivity analyses using 2 distinct strategies. First, Baujat plots were generated to identify which individual studies had the most significant influence on both the pooled estimate and overall heterogeneity. 27 Second, leave-one-out analyses were conducted to assess the robustness of the results by iteratively excluding each study and recalculating the pooled effect.
Bayesian Analysis
In addition to conventional frequentist methods, Bayesian random-effects meta-analyses were conducted for key oncological outcomes, including CRM+, local recurrence, and distant recurrence. A Bayesian framework was adopted to better characterize uncertainty and provide probabilistic interpretation of treatment effects, particularly given the limited number of included studies and relatively low event rates across these outcomes, conditions under which frequentist estimates may be unstable and difficult to interpret.28,29 For each outcome, pooled effect estimates were obtained using Bayesian random-effects models. An empirical heterogeneity prior based on Turner et al was used as the primary τ prior, reflecting non-pharmacological vs non-pharmacological comparisons and corresponding to a typical between-study variance of τ2 ≈ 0.12. 29 Sensitivity analyses were conducted using half-normal priors with scales of 0.5 and 1.5. For the overall treatment effect, a weakly informative prior centered at the null was used in the primary analysis, specified as μ ∼ Normal(0, 2.72). Sensitivity analyses were performed using a more informative prior, μ ∼ Normal(0, 0.822), to evaluate the robustness of the findings.28,29,30 Posterior summaries included pooled effect estimates with 95% credible intervals, the between-study heterogeneity parameter (τ), posterior probabilities of treatment superiority, and 95% prediction intervals.28,29,30,31 Posterior probabilities were interpreted using pragmatic thresholds, with values close to 50% indicating equipoise and more extreme values suggesting increasing evidence for or against treatment effects.28,29
Results
Study Inclusion and Baseline Characteristics
In Figure 1, we present the flow of the literature search. A total of 3876 records were initially identified. After removing 1026 duplicates and excluding 2817 articles during title and abstract screening, 30 studies were selected for full-text review. Of these, 5 observational studies met the eligibility criteria and were included in the final analysis.6,9,12,13,14 The reasons for study exclusion are presented in Supplemental Table S2. Across the included studies, a total of 1447 patients were analyzed, of whom 700 (48.3%) underwent upfront surgery (TME), and 747 (51.7%) received neoadjuvant therapy followed by TME. The mean follow-up duration was approximately 41.7 months. Male patients accounted for 951 individuals (65.7% of the total population). The average age across studies was approximately 57.1 years in the TME group and 56.8 years in the NEO + TME group.6,9,12,13,14 Prisma flow diagram of study screening and selection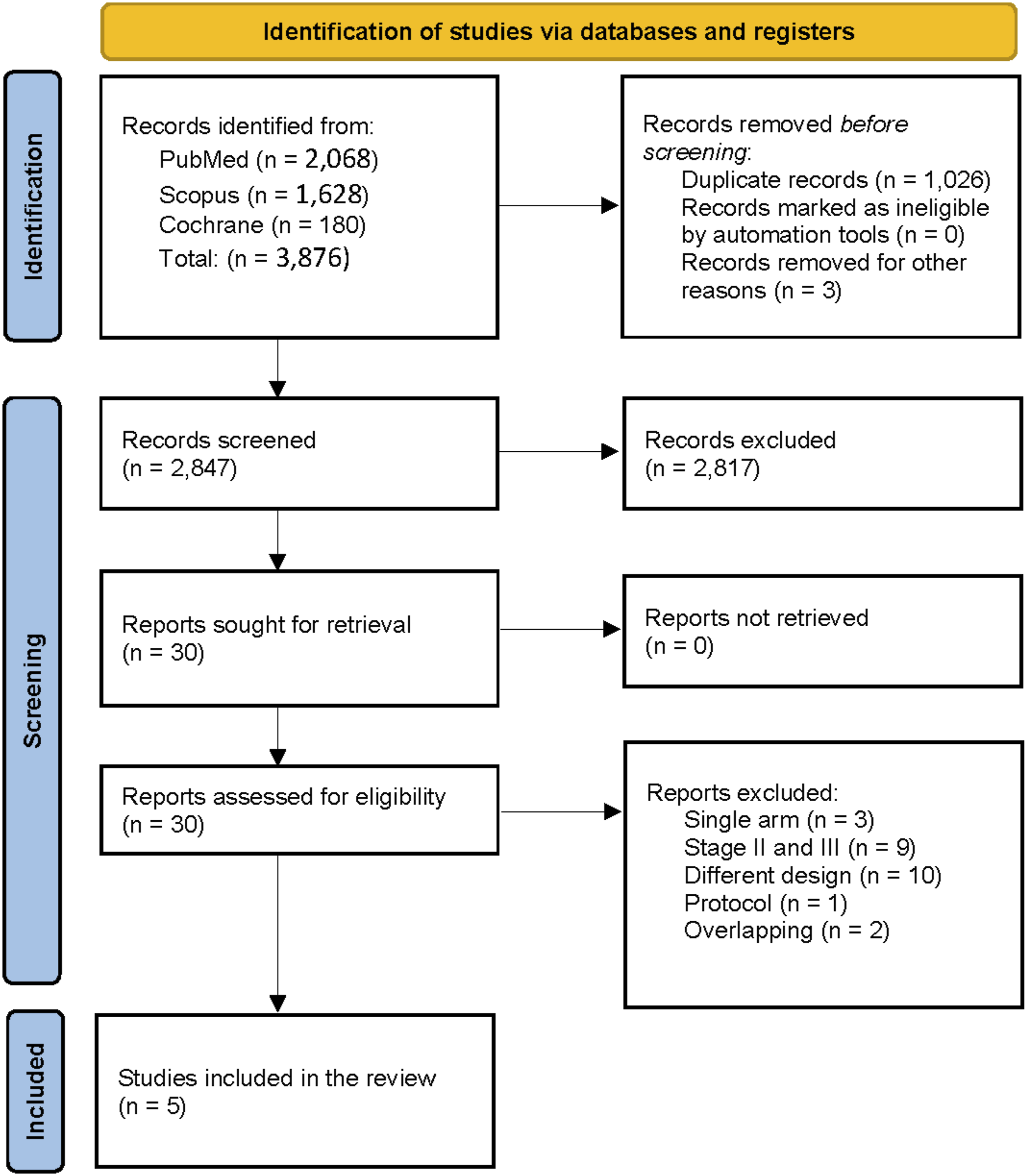
Tumor location was predominantly in the mid to low rectum, with the mean distance from the anal verge ranging from 5.6 to 5.9 cm in the upfront surgery and neoadjuvant groups, respectively. Surgical management was largely comparable across studies, with sphincter-preserving procedures being the most frequently performed approach. Low anterior resection represented the predominant technique (81.6% vs 84.6%), while intersphincteric resection was performed in selected cases (7.6% vs 8.5%).6,9,12,13,14
Baseline Characteristics of the Included Studies
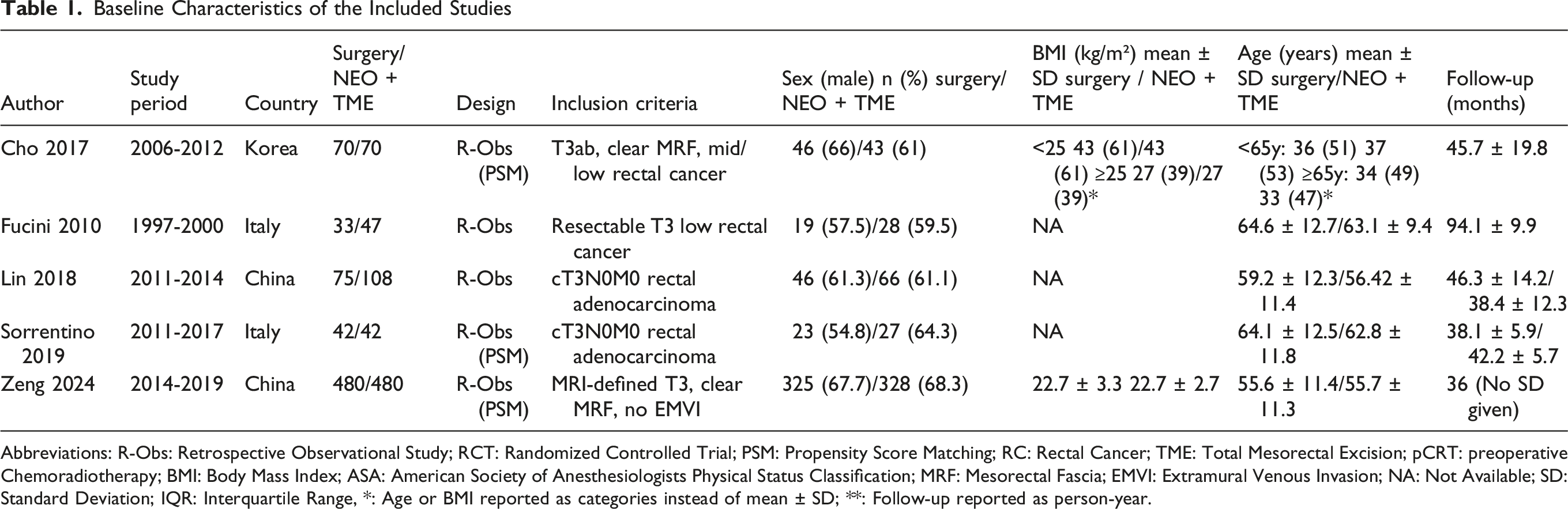
Abbreviations: R-Obs: Retrospective Observational Study; RCT: Randomized Controlled Trial; PSM: Propensity Score Matching; RC: Rectal Cancer; TME: Total Mesorectal Excision; pCRT: preoperative Chemoradiotherapy; BMI: Body Mass Index; ASA: American Society of Anesthesiologists Physical Status Classification; MRF: Mesorectal Fascia; EMVI: Extramural Venous Invasion; NA: Not Available; SD: Standard Deviation; IQR: Interquartile Range, *: Age or BMI reported as categories instead of mean ± SD; **: Follow-up reported as person-year.
Treatment Characteristics and Response Assessment of Included Studies
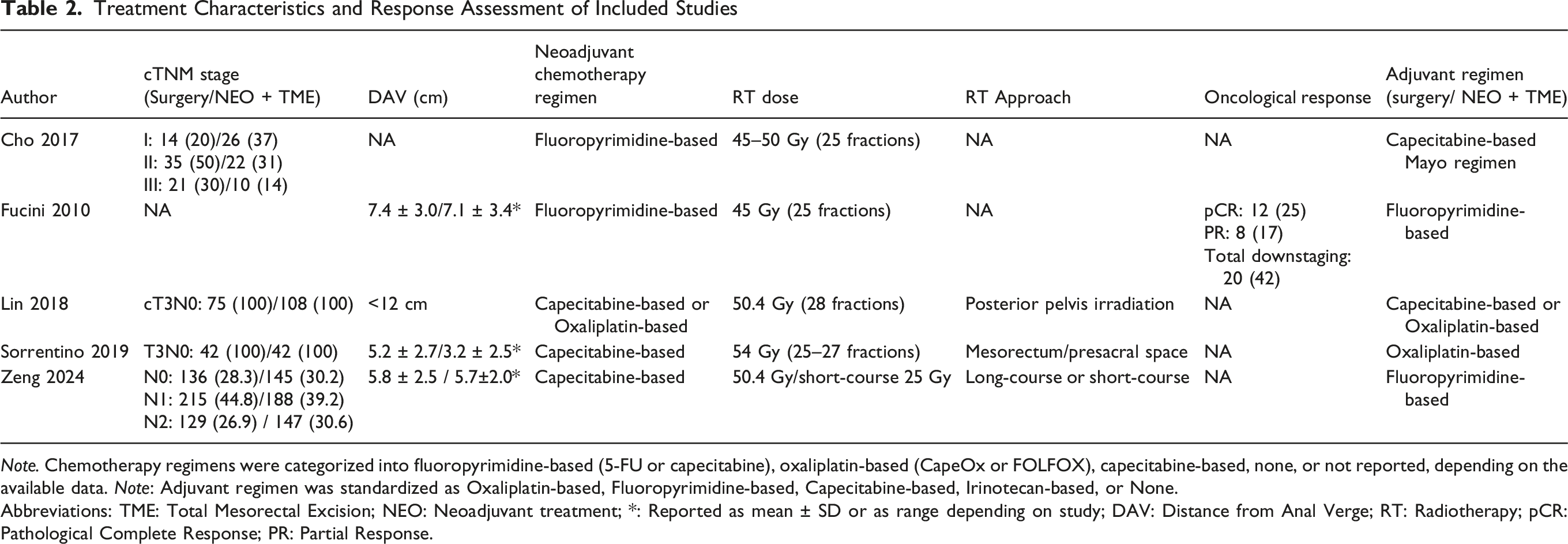
Note. Chemotherapy regimens were categorized into fluoropyrimidine-based (5-FU or capecitabine), oxaliplatin-based (CapeOx or FOLFOX), capecitabine-based, none, or not reported, depending on the available data. Note: Adjuvant regimen was standardized as Oxaliplatin-based, Fluoropyrimidine-based, Capecitabine-based, Irinotecan-based, or None.
Abbreviations: TME: Total Mesorectal Excision; NEO: Neoadjuvant treatment; *: Reported as mean ± SD or as range depending on study; DAV: Distance from Anal Verge; RT: Radiotherapy; pCR: Pathological Complete Response; PR: Partial Response.
Surgical and Pathological Characteristics of the Included Studies
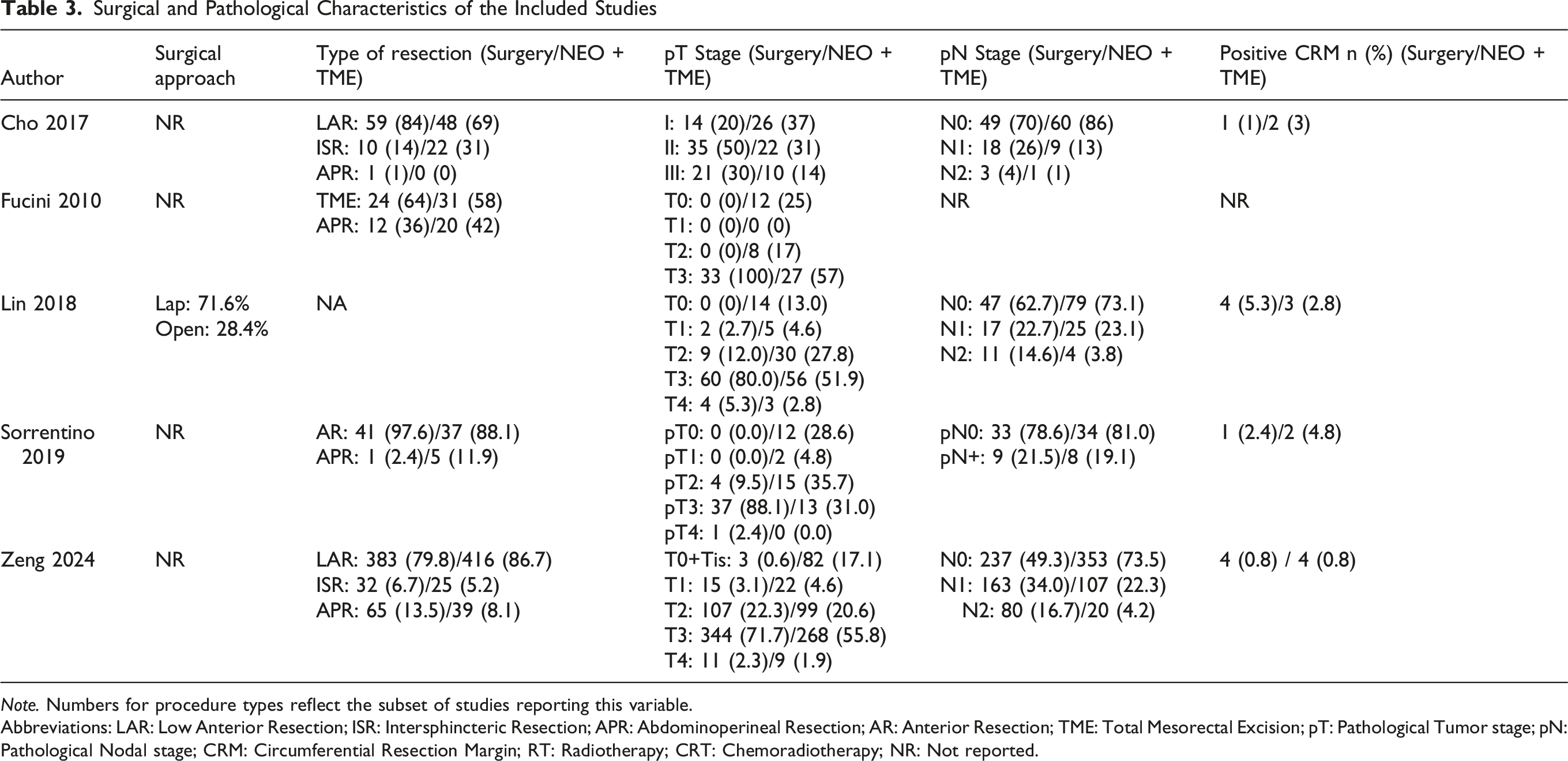
Note. Numbers for procedure types reflect the subset of studies reporting this variable.
Abbreviations: LAR: Low Anterior Resection; ISR: Intersphincteric Resection; APR: Abdominoperineal Resection; AR: Anterior Resection; TME: Total Mesorectal Excision; pT: Pathological Tumor stage; pN: Pathological Nodal stage; CRM: Circumferential Resection Margin; RT: Radiotherapy; CRT: Chemoradiotherapy; NR: Not reported.
Pooled Analyses of the Included Studies
Perioperative Outcomes
Operative time was shorter in the TME group than in the NEO + TME group (MD −25.7 minutes; 95% CI −38.6 to −12.7; P < 0.01; I2 = 48%; Figure 2A),6,12,14 with moderate heterogeneity across studies. The number of lymph nodes retrieved tended to be higher in the TME group (MD 6.6; 95% CI 6.0 to 7.3; P < 0.01; I2 = 0%; Figure 2B),6,12,13,14 demonstrating low heterogeneity. No statistically significant difference was observed between groups in terms of intraoperative blood loss (MD 4.9 mL; 95% CI −12.1 to 21.9; P = 0.57; I2 = 0%; Figure 2C),6,12,14 with low heterogeneity. Forest plots comparing upfront surgery (TME) and neoadjuvant chemoradiotherapy followed by surgery (NEO + TME)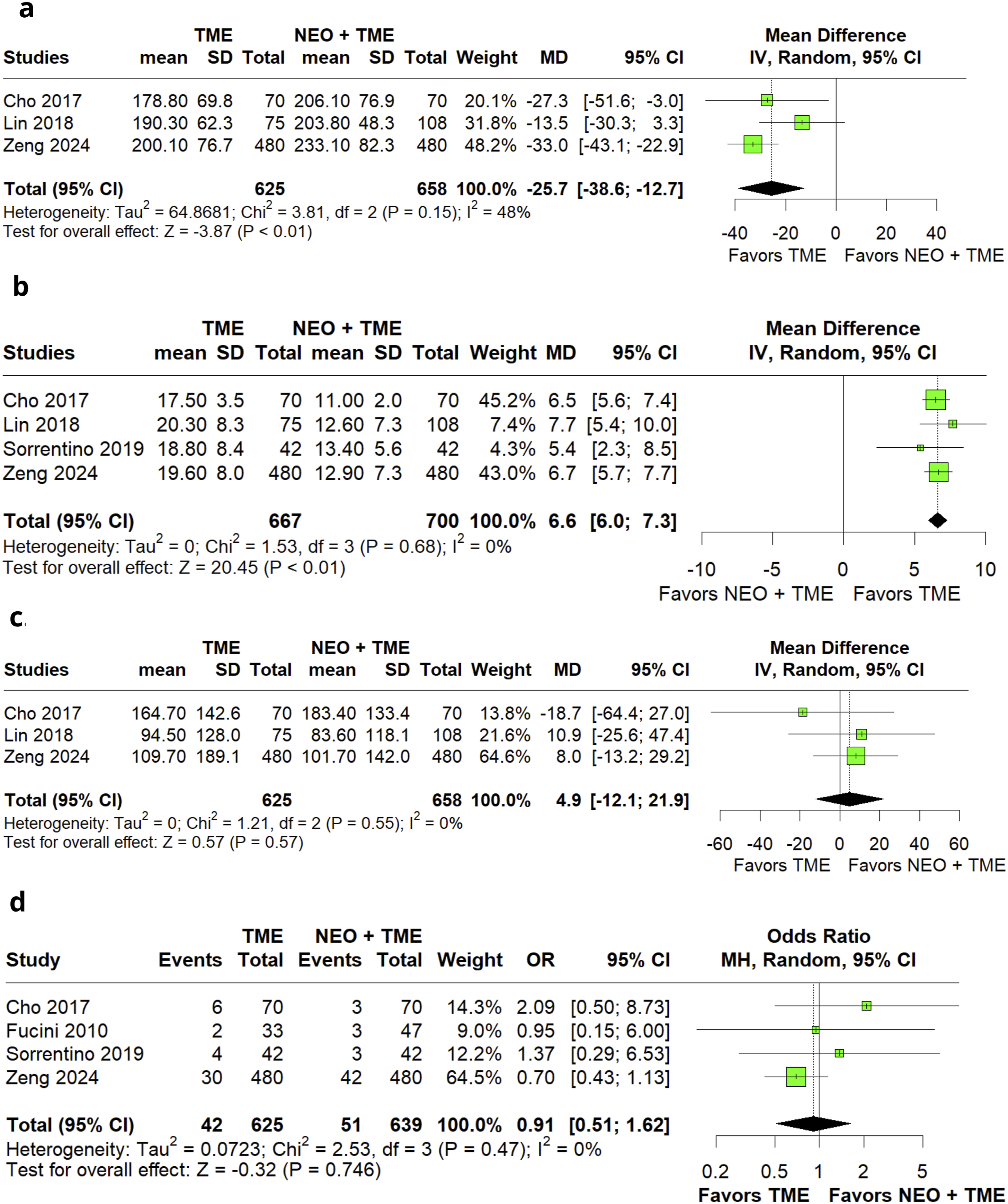
Similarly, no differences were found for anastomotic leak (OR 0.91; 95% CI 0.51 to 1.62; P = 0.75; I2 = 0%; Figure 2D) or intra-abdominal abscess (OR 0.47; 95% CI 0.15 to 1.47; P = 0.20; I2 = 0%; Figure 3A),6,9,13,14 both demonstrating low heterogeneity. Reoperation rates were also comparable between groups (OR 0.46; 95% CI 0.13 to 1.57; P = 0.21; I2 = 28%; Figure 3B),9,13,14 with moderate heterogeneity. Forest plots comparing upfront surgery (TME) and neoadjuvant chemoradiotherapy followed by surgery (NEO + TME)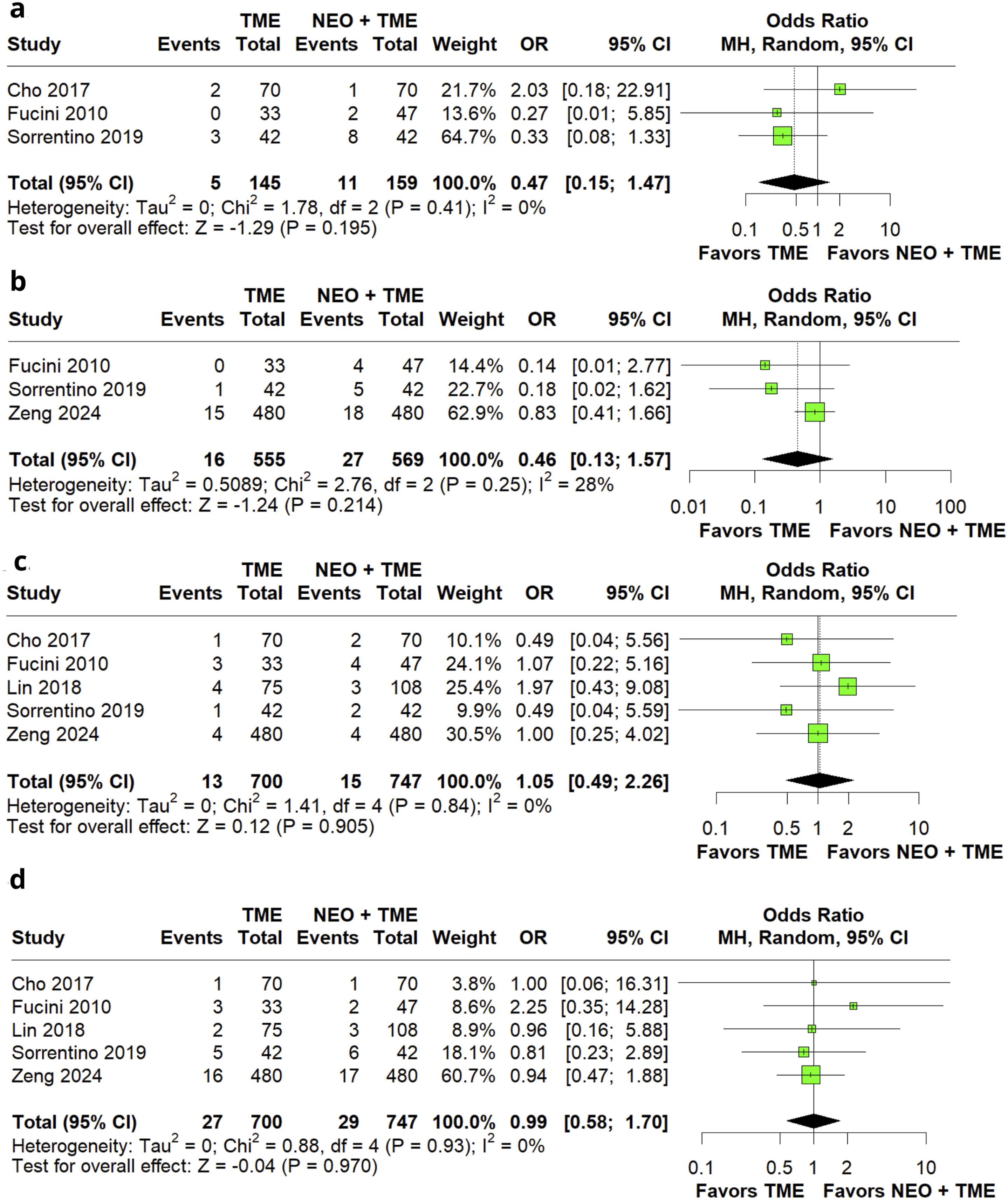
Oncological Outcomes
No statistically significant differences were observed between upfront surgery and neoadjuvant groups in terms of CRM + (OR 1.05; 95% CI 0.49 to 2.26; P = 0.91; I2 = 0%; Figure 3C),6,9,12,13,14 local recurrence (OR 0.99; 95% CI 0.58 to 1.70; P = 0.97; I2 = 0%; Figure 3D),6,9,12,13,14 or distant recurrence (OR 1.03; 95% CI 0.64 to 1.65; P = 0.92; I2 = 0%; Figure 4A),6,9,12,13 all with low heterogeneity. Forest plots comparing upfront surgery (TME) and neoadjuvant chemoradiotherapy followed by surgery (NEO + TME)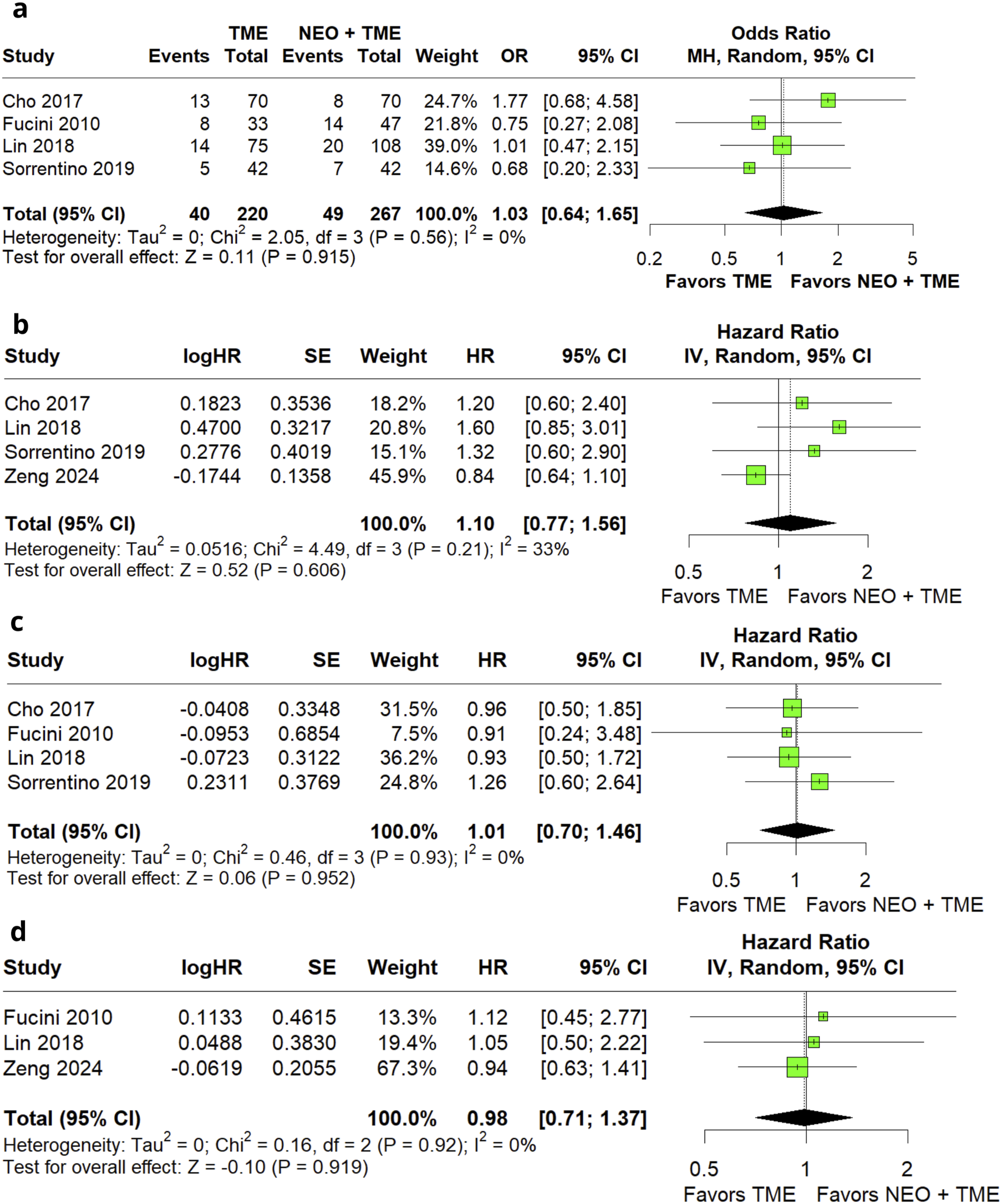
Survival Outcomes
No statistically significant differences were observed between groups for disease-free survival at 3 years (HR 1.10; 95% CI 0.77 to 1.56; P = 0.61; I2 = 33%; Figure 4B),6,12,13,14 with moderate heterogeneity. Similarly, no differences were found for 5-year disease-free survival (HR 1.01; 95% CI 0.70 to 1.46; P = 0.95; I2 = 0%; Figure 4C) or overall survival at 3 years (HR 0.98; 95% CI 0.71 to 1.37; P = 0.92; I2 = 0%; Figure 4D),6,9,12,13,14 both demonstrating low heterogeneity.
Sensitivity Analyses
Sensitivity analyses were performed using leave-one-out approaches and Baujat plots to evaluate the influence of individual studies and sources of heterogeneity. For operative time, the overall effect remained consistent across leave-one-out iterations, although moderate heterogeneity was observed, with the study by Lin et al contributing most to between-study variability (Supplemental Figures S1 and S2). 12 For 3-year disease-free survival, results were stable across sensitivity analyses, with no single study substantially altering the pooled estimate. Moderate heterogeneity was primarily driven by the study by Zeng et al (Supplemental Figures S3 and S4). 14 For reoperation, sensitivity analysis showed variability in the pooled estimate, indicating a notable influence of individual studies, particularly Zeng et al, although the overall effect remained non-significant (Supplemental Figure S5). 14 For intraoperative blood loss, leave-one-out analysis demonstrated consistent findings with no significant impact of individual studies and no evidence of heterogeneity (Supplemental Figure S6).
Bayesian Analysis
CRM Positivity
A Bayesian random-effects meta-analysis including 5 studies demonstrated no meaningful difference between TME and NEO + TME regarding CRM positivity. The pooled posterior odds ratio was 1.03 (95% CrI: 0.44-2.39). Between-study heterogeneity was moderate, with a posterior median τ of 0.309 (95% CrI: 0.076-0.706). The posterior probability that TME was superior to NEO + TME was 47.2%, indicating no directional evidence favoring either strategy. The 95% prediction interval ranged from 0.32 to 3.25, indicating substantial uncertainty about the expected effect size in future studies. Sensitivity analyses using alternative priors yielded consistent results, confirming the robustness of the primary model (Supplemental Table S3; Supplemental Figures S7–S11).
Local Recurrence
A Bayesian meta-analysis including 5 studies showed no significant difference between treatment strategies. The pooled posterior odds ratio was 1.01 (95% CrI: 0.51-2.00). Between-study heterogeneity was moderate, with a posterior median τ of 0.294 (95% CrI: 0.075-0.664). The posterior probability that TME was superior to NEO + TME was 48.8%, indicating inconclusive evidence with no clear advantage for either approach. The 95% prediction interval ranged from 0.37 to 2.80, suggesting variability in the potential effect across future settings. Sensitivity analyses demonstrated stable effect estimates across all prior specifications (Supplemental Table S4; Supplemental Figures S12–S16).
Distant Recurrence
A Bayesian meta-analysis including 4 studies demonstrated no meaningful difference between TME and NEO + TME. The pooled posterior odds ratio was 1.01 (95% CrI: 0.55-1.85). Between-study heterogeneity was moderate, with a posterior median τ of 0.297 (95% CrI: 0.075-0.668). The posterior probability that TME was superior to NEO + TME was 47.9%, indicating no evidence favoring either strategy. The 95% prediction interval ranged from 0.38 to 2.67, reflecting uncertainty in the expected magnitude and direction of effect in future studies. Sensitivity analyses confirmed the robustness of these findings (Supplemental Table S5; Supplemental Figures S17–S21).
Quality Assessment and Certainty
The risk of bias of the included studies was assessed using the ROBINS-I tool (Figure 5), with detailed domain-level justifications provided in Supplemental Table S6. Overall, all studies were judged to have a moderate risk of bias, mainly due to residual confounding inherent to observational designs and variability in treatment allocation. Bias related to intervention classification and outcome measurement was consistently low across studies, whereas deviations from intended interventions and incomplete reporting contributed to moderate concerns. Critical appraisal of non-randomized according to the Cochrane Collaboration’s tool for assessing risk of bias. ROBINS-I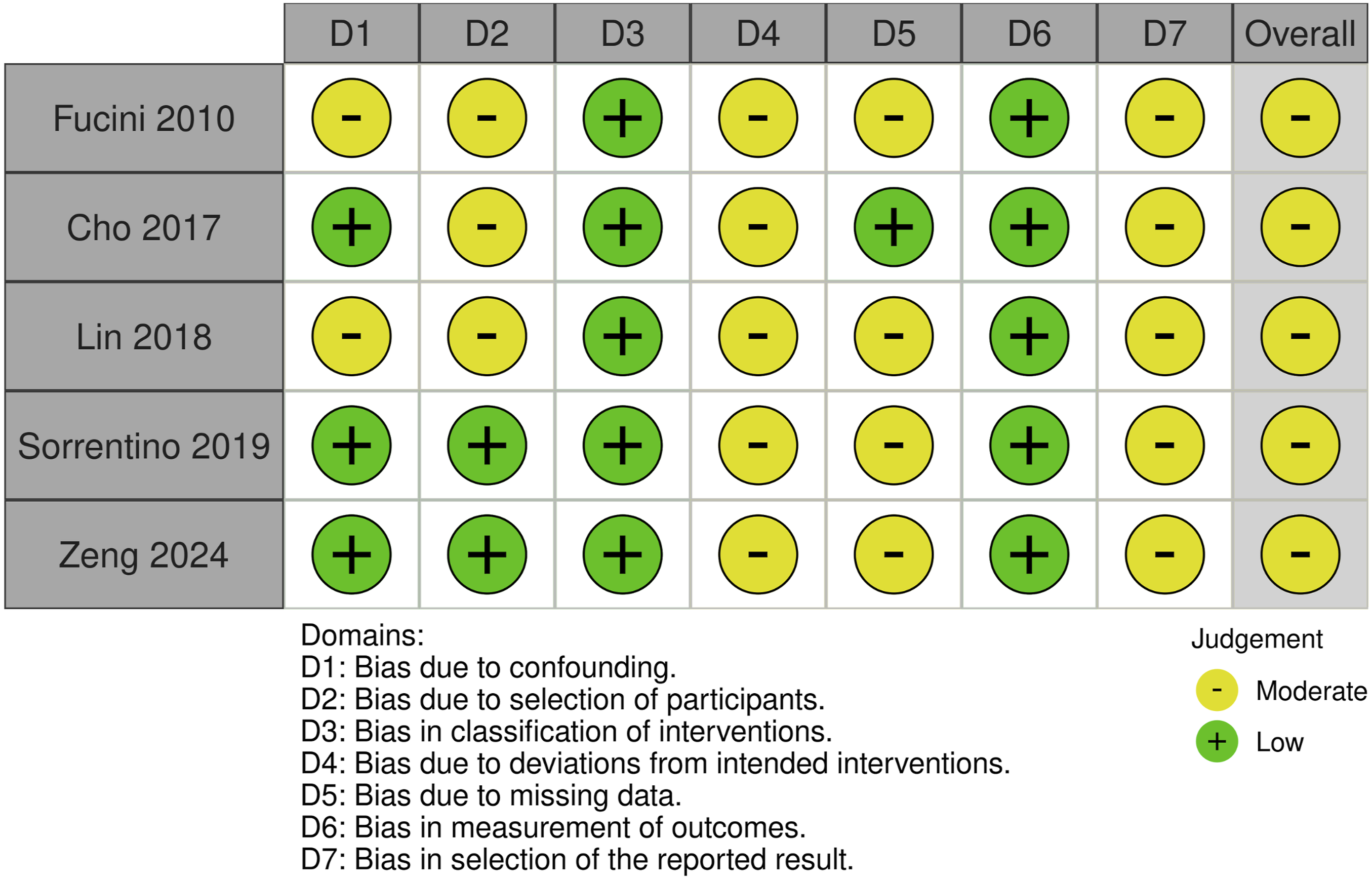
The certainty of evidence was evaluated using the GRADE approach, as summarized in Supplemental Table S7. Overall, the certainty ranged from low to very low across most outcomes. This was primarily driven by the observational nature of the included studies (downgraded for risk of bias) and imprecision of effect estimates, particularly for oncological and survival outcomes, where confidence intervals were wide and frequently crossed the null value. Moderate inconsistency was observed for selected outcomes, including operative time, reoperation, and 3-year disease-free survival, while most other outcomes demonstrated low heterogeneity. No serious concerns regarding indirectness were identified, as all studies focused on patients with cT3 rectal cancer.
Publication bias could not be assessed because no outcome included the minimum of 10 studies required to perform a funnel plot inspection or Egger’s regression test.
Discussion
In this systematic review and meta-analysis, including 5 observational studies encompassing 1447 patients with cT3 rectal cancer, upfront TME was associated with shorter operative time and a higher number of lymph nodes retrieved compared to NEO + TME. No statistically significant differences were observed between groups in terms of blood loss, anastomotic leak, intra-abdominal abscess, reoperation, CRM positivity, local recurrence, distant recurrence, 3- and 5-year DFS, and 3-year OS. For CRM positivity, local recurrence, and distant recurrence, Bayesian analysis also demonstrated no meaningful difference between strategies, with posterior probabilities remaining close to equipoise. These findings should be interpreted within the contemporary framework of MRI-directed treatment selection and selective de-escalation strategies for low-risk rectal cancer.
The rationale for questioning the routine use of preoperative chemoradiotherapy in all cT3 rectal tumors arises from evidence that, in the absence of threatened mesorectal fascia, upfront TME alone can provide adequate oncological outcomes.6,9,11,14,16,17,32 In an institutional series, Frasson et al evaluated 152 patients with cT2N + or cT3N0/N+ rectal cancer treated exclusively with TME and reported 5-year DFS and cancer-specific survival rates of 65.4% and 77.8%, respectively, identifying threatened mesorectal fascia as the only independent predictor of poor prognosis. 32 Similar findings have been reported in broader stage II–III populations. A large multicenter cohort by Kulu et al demonstrated comparable rates of CRM+, recurrence, and survival between patients treated with and without neoadjuvant therapy, while long-term results from a randomized trial by Wang et al also showed no differences in DFS, OS, or recurrence outcomes between treatment strategies.7,10 Together, these data suggest that the benefit of routine neoadjuvant therapy may not be universal, particularly in patients without high-risk features.6,14,16,17
In this context, our findings regarding a more selected cT3 population are consistent with the available literature. We observed no differences in key oncological outcomes, including CRM +, local and distant recurrence, and survival endpoints. These results support the concept that, when appropriate selection criteria are applied, upfront TME may achieve adequate disease control without preoperative treatment. However, the accuracy of preoperative staging remains a critical limitation. As highlighted by Guillen et al, up to 22% of clinically staged cT3N0 patients may harbor occult nodal disease, potentially leading to undertreatment in selected cases. 33 Nevertheless, the methodological limitations of this study, including its single-arm design and lack of survival outcomes, reduce its applicability to contemporary decision-making. 33
Beyond oncological outcomes, operative and pathological parameters provide additional insights. In the present analysis, a higher number of lymph nodes was retrieved in the TME group, a finding consistent with the known effects of neoadjuvant therapy, which can induce fibrosis and reduce nodal yield. 34 Regarding postoperative morbidity, no significant differences were observed between groups. However, large external data sets, such as the multicenter cohort by Akagi et al, have reported lower rates of postoperative complications and anastomotic leakage in patients undergoing neoadjuvant chemoradiotherapy. 5 These findings suggest that, although not demonstrated in our pooled analysis, neoadjuvant treatment may influence postoperative outcomes in selected populations. 5 In addition, avoidance of pelvic radiotherapy may have important implications for long-term bowel, urinary, and sexual function, which are increasingly recognized as critical survivorship outcomes in rectal cancer management.
Rectal cancer management has shifted toward a goal-directed approach based on high-resolution MRI and individualized risk stratification. 16 Contemporary treatment paradigms and modern trials, including MERCURY, RAPIDO, PRODIGE 23, and PROSPECT, increasingly emphasize biologic risk stratification and selective treatment escalation or de-escalation according to MRI-defined risk features. In addition to tumor-related factors such as mesorectal fascia status and tumor location relative to the anorectal ring, patient-related characteristics may also influence treatment decisions.2,4,8,18,19 Factors such as male sex with a narrow pelvis, advanced age, long anal canal, obesity, comorbidities, and potential involvement of the anorectal ring may directly impact surgical complexity, sphincter preservation, and postoperative outcomes.2,4,8,18,19 Within this framework, selected patients with cT3 tumors, clear mesorectal fascia, and favorable anatomical characteristics may achieve adequate oncologic outcomes with upfront TME, whereas others may benefit from neoadjuvant strategies tailored to specific therapeutic objectives.6,9,12,13,14 However, these considerations remain hypothesis-generating and should be interpreted with caution given the limited sample size, observational design, and low certainty of evidence.
This study acknowledges several limitations. First, the analysis was based on a small number of observational studies, inherently subject to residual confounding, selection bias, and variability in treatment allocation. Second, although inclusion was restricted to cT3 tumors with clear mesorectal fascia, definitions of sphincter involvement and tumor location relative to the anorectal ring were not uniformly reported, introducing clinical heterogeneity. Third, the limited sample size and relatively low event rates resulted in imprecise effect estimates, with wide confidence and credible intervals, reducing the ability to detect clinically meaningful differences. In addition, inaccuracies in preoperative staging remain a concern, as a proportion of clinically staged cT3N0 patients may harbor occult nodal disease, potentially influencing treatment selection and outcomes. Variability in surgical technique, institutional expertise, and neoadjuvant protocols may have further contributed to heterogeneity. Publication bias could not be formally assessed due to the small number of included studies. Finally, although Bayesian analyses were performed to better characterize uncertainty and provide complementary probabilistic interpretation, they do not overcome the inherent limitations of observational evidence and clinical heterogeneity. Accordingly, the results remained centered around equipoise and should be interpreted as exploratory rather than definitive evidence of treatment equivalence or superiority.
Conclusion
In this systematic review and meta-analysis, which included 5 observational studies encompassing 1447 patients with cT3 rectal cancer, the TME group had shorter operative time and a higher number of lymph nodes retrieved compared to the NEO + TME group. No statistically significant differences were observed between groups for blood loss, anastomotic leak, intra-abdominal abscess, reoperation, CRM+, local recurrence, distant recurrence, 3- and 5-year DFS, and 3-year OS. For CRM+, local recurrence, and distant recurrence, Bayesian analysis also suggested no clear evidence of difference between TME and NEO + TME, with posterior probabilities remaining close to equipoise. These findings support the hypothesis that carefully selected MRI-defined low-risk cT3 tumors may represent candidates for selective omission of neoadjuvant therapy within contemporary risk-stratified treatment frameworks.
Supplemental Material
Supplemental Material - Upfront Total Mesorectal Excision for MRI-Defined Low-Risk cT3 Rectal Cancer: A Systematic Review and Meta-Analysis
Supplemental Material for Upfront Total Mesorectal Excision for MRI-Defined Low-Risk cT3 Rectal Cancer: A Systematic Review and Meta-Analysis by Bernardo Fontel Pompeu, Camila Haddad Baptista, Thais Henriques Abud, Mateus Lima Ulisses Trindade, Maria Eduarda Caetano Batista de Paiva, Gabriel Leal Barone, Lucas Monteiro Delgado, Claudia Theis, Sergio Mazzola Poli de Figueiredo, and Fernanda Bellotti Formiga in The American Surgeon
Footnotes
Author Contributions
Conception and design: BFP, FBF, SMPF, CT
Data acquisition: BFP, CHB, CT, GLB, LMD, THA, MLUT, MECBP.
Data analysis: BFP, CHB, FBF, CT, GLB, LMD, THA, MLUT, MECBP.
Data interpretation: BFP, CHB , CT, GLB, LMD, THA, MLUT, MECBP.
Drafting and editing the manuscript: BFP, SMPF, FBF, GLB, LMD, THA, MLUT, MECBP.
Critical revision for important intellectual content: BFP, FBF, SMPF, CT.
All authors approved the final version of the article, including the authorship list.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Formiga reports speaker honoraria from Janssen Brazil outside the submitted work. Dr. Figueiredo reports honoraria from Intuitive and Distal Motion outside the submitted work. All other authors declare no related financial interests or potential conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.