
Abstract
Background
Cytoreductive surgery (CRS) with or without hyperthermic intraperitoneal chemotherapy (HIPEC) is a cornerstone treatment for peritoneal metastases but carries substantial morbidity. Splenectomy is frequently performed during CRS, yet it remains uncertain whether it independently increases postoperative risk or merely reflects greater surgical complexity.
Methods
We retrospectively analyzed 124 CRS procedures performed between 2014 and 2023 at a tertiary center, including 20 splenectomy cases. Operative characteristics, morbidity, and mortality were compared between splenectomy and non-splenectomy groups. Propensity score matching (PSM; 1:2 nearest-neighbor) and inverse probability of treatment weighting (IPTW; average treatment effect on the treated) were applied to adjust for baseline imbalances across age, ASA score, PCI, blood loss, primary tumor type, sex, and number of anastomoses.
Results
Patients undergoing splenectomy exhibited higher PCI scores (median 18.5 vs 9; P < .001), greater blood loss (775 vs 450 mL; P = .037), longer operative times (9 vs 6 hours; P = .007), and more visceral resections (median 4.5 vs 2; P < .001). Severe complications occurred in 60% of splenectomy vs 27% of non-splenectomy cases (P = .007), while mortality did not differ significantly (15% vs 8.7%; P = .408). After adjustment, splenectomy was not an independent risk factor for morbidity (PSM: OR 2.69, P = .193; IPTW: OR 1.76, P = .37). Higher ASA score, perioperative fluid replacement, and blood loss remained significant predictors.
Conclusions
Splenectomy during CRS correlates with higher observed morbidity but not with independently increased risk after controlling for surgical complexity. These findings suggest splenectomy reflects procedural burden rather than a direct hazard, underscoring the importance of contextual interpretation and vigilant perioperative management.
Keywords
Introduction
Cytoreductive surgery (CRS), often combined with hyperthermic intraperitoneal chemotherapy (HIPEC), has become an established treatment option for advanced intraperitoneal malignancies with intraperitoneal metastasis. The procedure aims to achieve complete macroscopic tumor removal through extensive visceral and peritoneal resections. While CRS can improve survival in carefully selected patients, it is associated with considerable operative complexity, long procedure times, and a high risk of morbidity. Identifying factors that influence postoperative outcomes remains a priority in optimizing patient selection and surgical strategy. Splenectomy is frequently performed as part of CRS due to tumoral infiltration of the spleen or inadvertent intraoperative injury. While technically straightforward, splenectomy has historically been associated to higher rates of complications, specifically to pancreatic fistula, infectious complications and sepsis, thrombocytosis, and pulmonary effusion.1-3
In the setting of CRS, however, splenectomy may also serve as a marker of operative complexity and advanced disease burden. Patients requiring splenectomy often undergo more extensive resections, have higher peritoneal cancer indices, and experience longer operative times and blood loss—all of which are independently associated with adverse outcomes.4-6
Taken together, it remains unclear whether postoperative complications in patients undergoing CRS are attributable to the independent effect of splenectomy itself, or whether splenectomy merely reflects a surrogate of surgical complexity and tumor burden. To address this question, we evaluated the impact of splenectomy on postoperative morbidity and mortality using propensity score matching (PSM) and inverse probability of treatment weighting (IPTW), thereby aiming to disentangle its direct contribution from confounding operative and patient factors.
Material and Methods
Ethical approval for this study was obtained from the Ethics Committee of the University of Health Sciences, Ümraniye Training and Research Hospital (Approval No: B.10.1.TKH.4.34.H.GP.0.01/186), dated June 13, 2024. All study procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki.
Patient Population and Preoperative Staging
Patient records were reviewed for individuals who underwent surgery for PC in the General Surgery and Gynecologic-Oncologic Surgery units of our institution between 2014 and 2023. Data were prospectively recorded and updated one month postoperatively to include information on complications. A total of 124 operations were performed on 113 patients, comprising 31 CRS-HIPEC procedures and 93 CRS-only procedures (Figure 1). Study Flow Diagram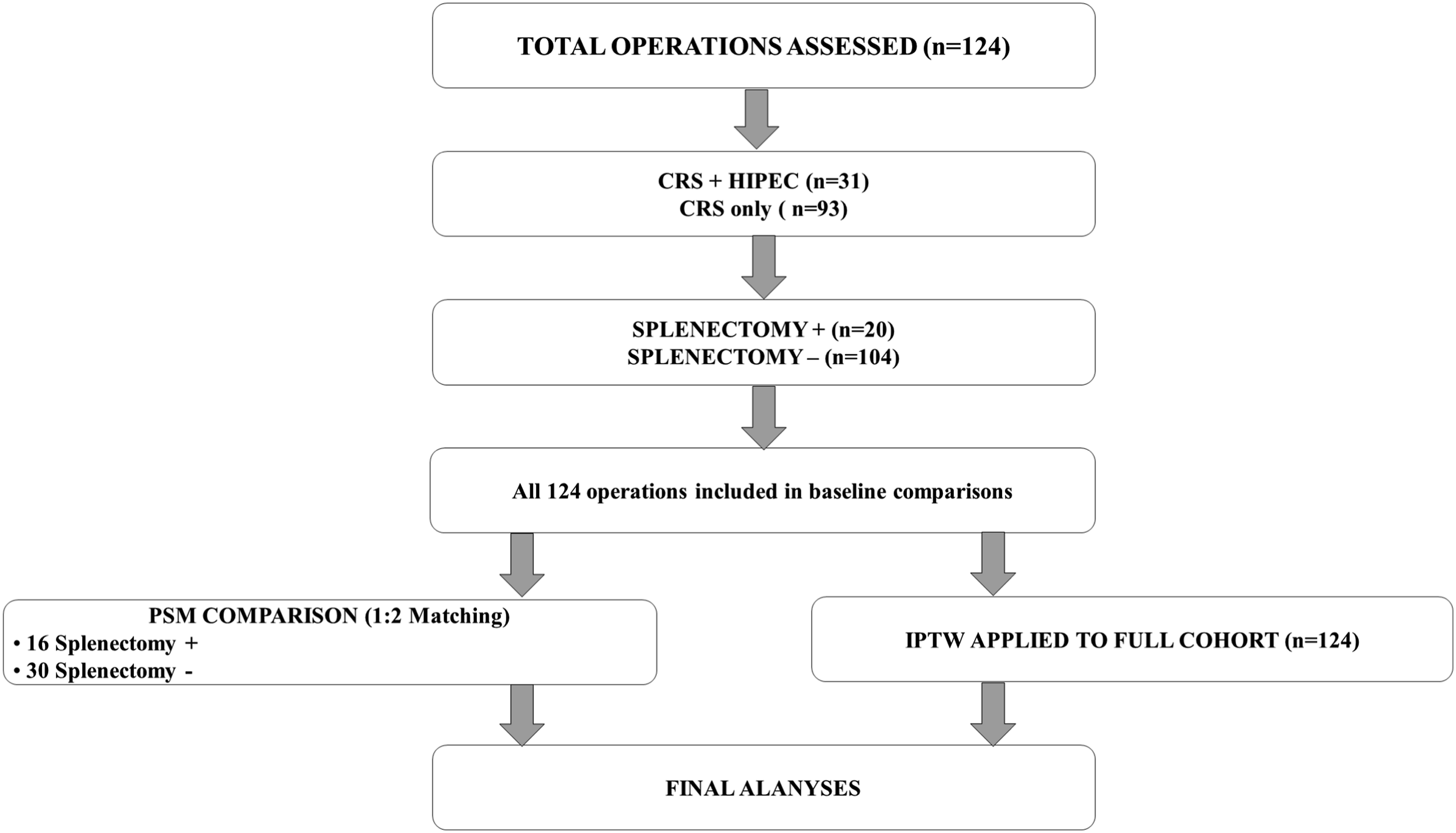
Preoperative staging was routinely performed using computed tomography (CT) scans of the chest, abdomen, and pelvis to assess the extent of peritoneal disease and rule out extra-abdominal metastases. All cases were discussed at a multidisciplinary tumor board meeting to determine suitability for CRS-HIPEC based on tumor biology, disease extent, and patient performance status. The primary tumor origins of the peritoneal metastases in our cohort included colorectal, ovarian, endometrial, mesenchymal, intestinal (GIST), and gastric cancers. The inclusion criteria were based on the patient’s suitability for complete cytoreduction, regardless of the primary tumor site, as assessed by the multidisciplinary board. Patients were selected for CRS-HIPEC based on established criteria, including resectable disease and good performance status.
Data Collection
Detailed intraoperative data were collected for each operation, including perioperative fluid replacement, estimated blood loss (EBL), blood transfusions, the Peritoneal Carcinomatosis Index (PCI), Completeness of Cytoreduction score (CC; CC-0: no macroscopic residual disease; CC-1: tumor nodules <2.5 mm; CC-2: tumor nodules 2.5 mm to 2.5 cm; CC-3: tumor nodules >2.5 cm), the number of anastomoses (NOA), organ resections performed, diaphragmatic resections, and the extent of peritonectomy. Preoperative hydration, intraoperative bleeding, and transfusion data were extracted from anesthesia records. Postoperative data included the length of hospital stay and intensive care unit (ICU) stay.
Postoperative adverse events occurring within 60 days of surgery were identified and graded using the Clavien-Dindo Classification. Additional interventions, including re-operations, unplanned interventional radiology procedures, blood transfusions, and antibiotic treatments, were identified from patient records. Postoperative mortality was assessed at 60 days as the primary endpoint to better capture early, procedure-related deaths after CRS. Ninety-day mortality was additionally evaluated as a secondary endpoint to facilitate comparisons with the existing CRS/HIPEC literature.
Surgical Treatment Definition
Cytoreductive surgery procedures involved meticulous dissection and removal of all visible peritoneal tumor implants. The specific procedures performed were tailored to the individual patient’s disease distribution and included various peritonectomy procedures (eg, parietal, diaphragmatic, omental, and pelvic) and organ resections. The decision to perform specific organ resections, such as colonic, intestinal, splenic, hepatic, or pancreatic resections, was based on the presence of tumor involvement and the feasibility of achieving complete cytoreduction with acceptable morbidity. Anastomoses were performed using standard surgical techniques, with careful attention to tension-free and well-vascularized connections. All operations were performed by the same team of four surgeons, with at least two of them participating in each procedure.
The perfusion time of HIPEC agent was 60-90 minutes, and the temperature was maintained between 41-43°C. The specific agent and duration were determined based on the primary tumor histology and patient characteristics.
Statistical Analysis
Statistical analysis was performed using SPSS 25.0 (IBM, USA) and RStudio version 2025.05.1. Categorical variables were summarized as numbers and percentages, while continuous variables were expressed as mean ± standard deviation or as median (minimum-maximum), as appropriate. The Shapiro-Wilk test was used to assess the normality of data distribution.
Baseline demographic, operative, and outcome variables were compared between patients who underwent splenectomy and those who did not. Categorical variables, including mortality and severe complications, were analyzed using the Chi-square or Fisher’s exact test, as appropriate.
Exploratory logistic regression was performed in the overall cohort. Given the small sample size and multicollinearity among operative variables, results were unstable and served primarily to motivate the use of propensity score methods (PSM and IPTW) for more reliable adjustment. Univariate analysis using logistic regression was conducted to evaluate parameters influencing complications. Variables with a P-value <.05 were included in multivariate analysis. This was mostly made to underscore the role of splenectomy as an independent risk factor for morbidity.
Propensity score methods were applied to adjust for baseline imbalances between patients who underwent splenectomy and those who did not. Propensity scores were estimated using a logistic regression model including ASA score (2-4), age, blood loss, primary tumor type (gynecologic, colorectal, other), sex, number of anastomoses, and Peritoneal Cancer Index (PCI) as covariates. For PSM, a nearest-neighbor algorithm was applied in a 1:2 ratio without caliper, yielding 16 splenectomy cases and 30 matched controls. Balance was assessed using standardized mean differences (SMD), with |SMD| < 0.1 considered acceptable. After weighting, the number of covariates exceeding this threshold was recorded.
IPTW was additionally performed on the full cohort using the same covariates. An average treatment effect on the treated (ATT) estimand was applied to approximate the effect in the splenectomy group. Extreme weights were truncated at the 1st and 99th percentiles. Post-weighting balance was confirmed by examining SMDs and visualized with Love plots (Figure 2). Weighted logistic regression models were then used to estimate odds ratios (OR) with 95% confidence intervals (CI) for severe complications and mortality. Covariate balance before and after adjustment using PSM and IPTW PSM = Propensity Score Matching; IPTW = Inverse Probability of Treatment Weighting; ATT = Average Treatment Effect on the Treated; SMD = Standardized Mean Difference; PCI = Peritoneal Cancer Index. The left panel demonstrates covariate balance achieved after 1:2 nearest-neighbor PSM, and the right panel shows balance following ATT-IPTW adjustment. Dashed vertical lines indicate the threshold for acceptable balance (|SMD| < 0.1). Both weighting methods effectively minimized baseline imbalances between splenectomy and non-splenectomy groups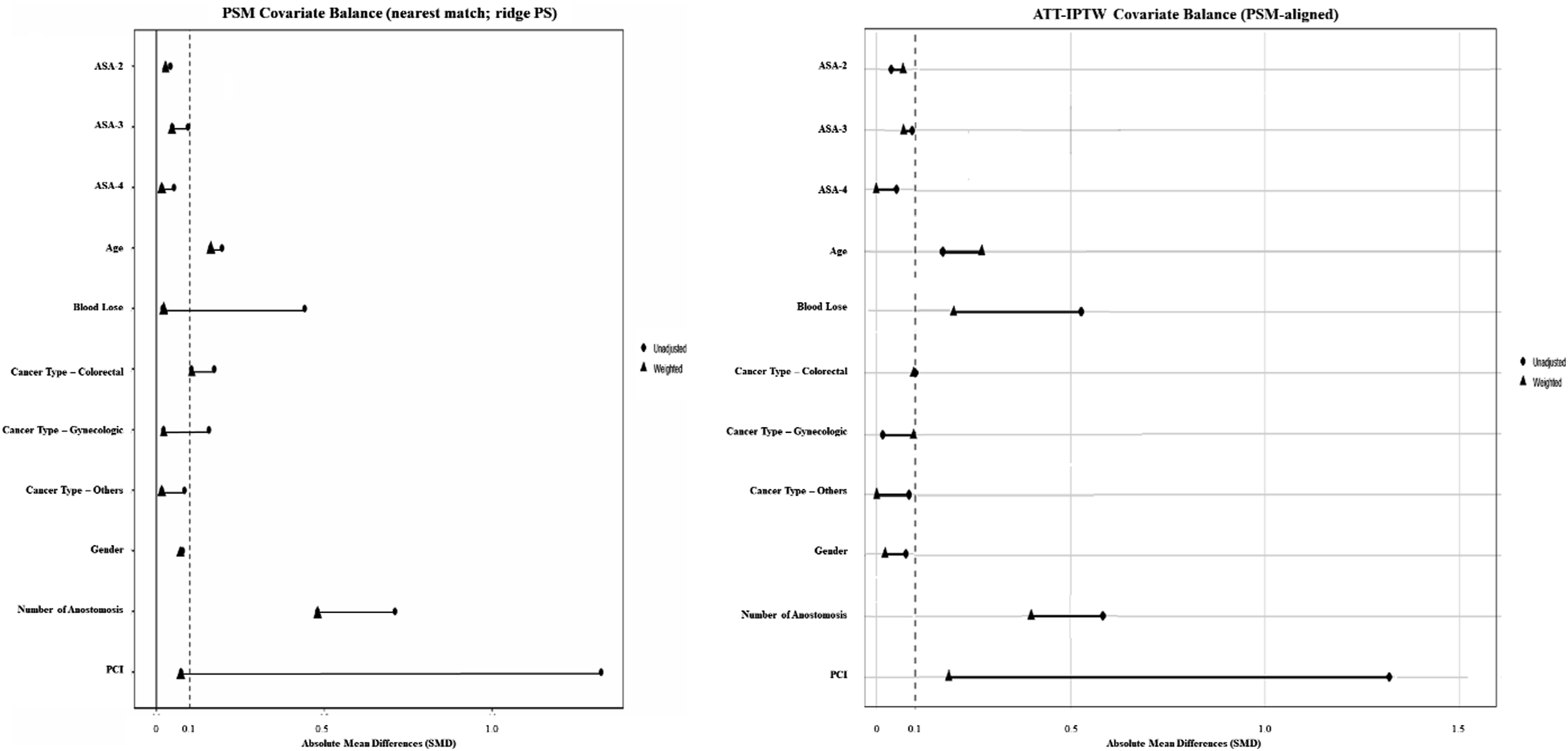
Results
Baseline Demographic and Clinical Characteristics of the Study Cohort
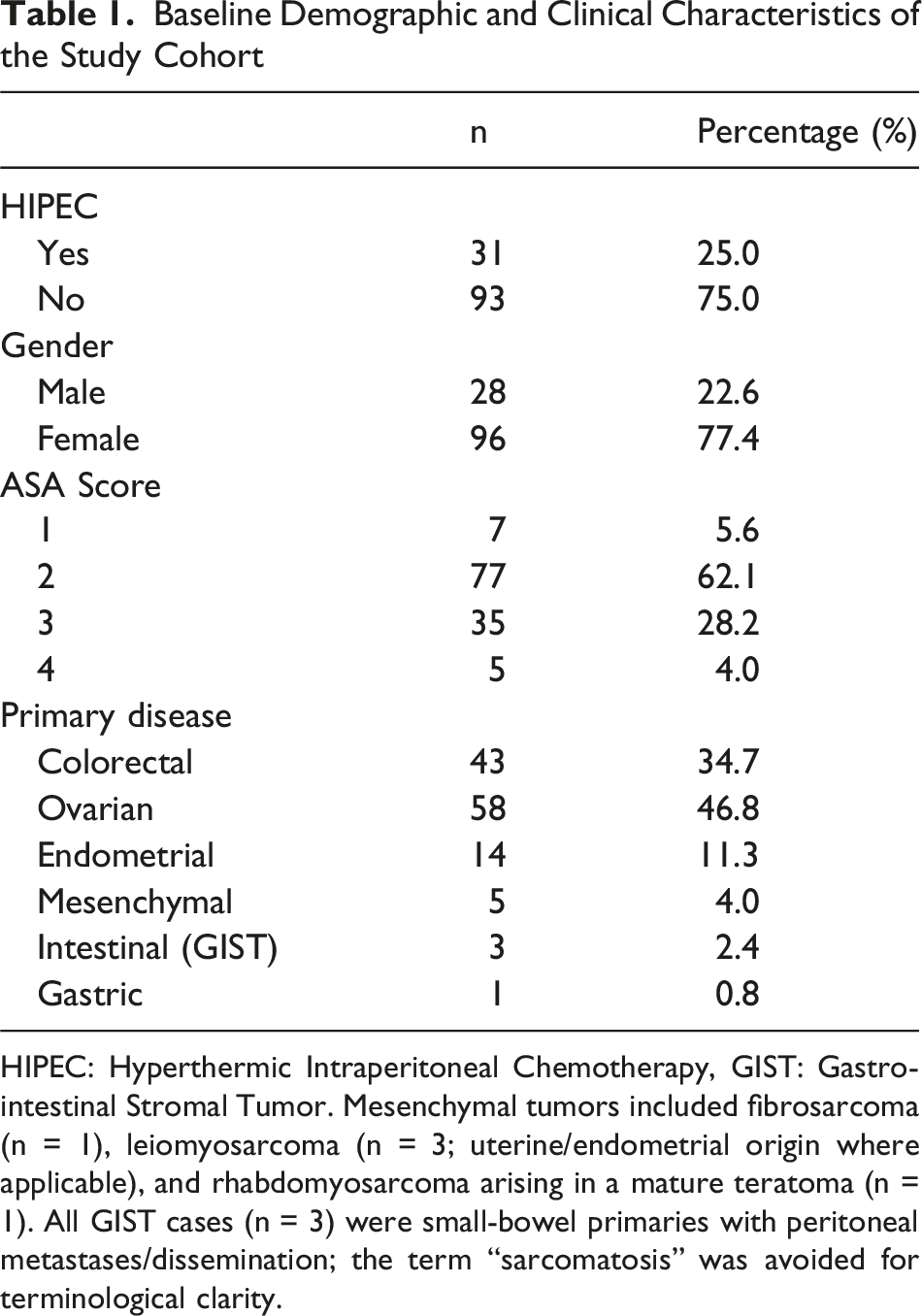
HIPEC: Hyperthermic Intraperitoneal Chemotherapy, GIST: Gastrointestinal Stromal Tumor. Mesenchymal tumors included fibrosarcoma (n = 1), leiomyosarcoma (n = 3; uterine/endometrial origin where applicable), and rhabdomyosarcoma arising in a mature teratoma (n = 1). All GIST cases (n = 3) were small-bowel primaries with peritoneal metastases/dissemination; the term “sarcomatosis” was avoided for terminological clarity.
In the overall cohort, 20 patients (16.1%) underwent splenectomy. Compared with patients without splenectomy, those requiring splenectomy exhibited greater operative complexity, as reflected by higher PCI scores (median 18.5 vs 9, P < 0.001), increased blood loss (median 775 mL vs 450 mL, P = .037), longer operative times (median 9 vs 6 hours, P = .007), and a higher number of anastomoses (median 1 vs 0, P = 0.007). As illustrated in Figure 3, the distribution of concomitant organ resections differed markedly between patients who underwent splenectomy and those who did not. Splenectomy cases were consistently associated with a broader operative scope—particularly higher rates of colonic, diaphragmatic, hepatic, and gastric resections—highlighting their greater procedural complexity within cytoreductive surgery. They also had a greater extent of visceral resections (median 4.5 vs 2, P < 0.001). Postoperatively, splenectomy patients required longer ICU stays (median 2 vs 1 days, P = .028) and prolonged hospital stays (median 15.5 vs 8 days, P < .001). Additional organ resections in the splenectomy and non-splenectomy groups The figure compares the proportion of patients undergoing additional organ resections in the splenectomy and non-splenectomy groups. Splenectomy was frequently associated with higher rates of colonic, diaphragmatic, hepatic, and gastric resections, reflecting greater operative extent and surgical complexity within the cytoreductive cohort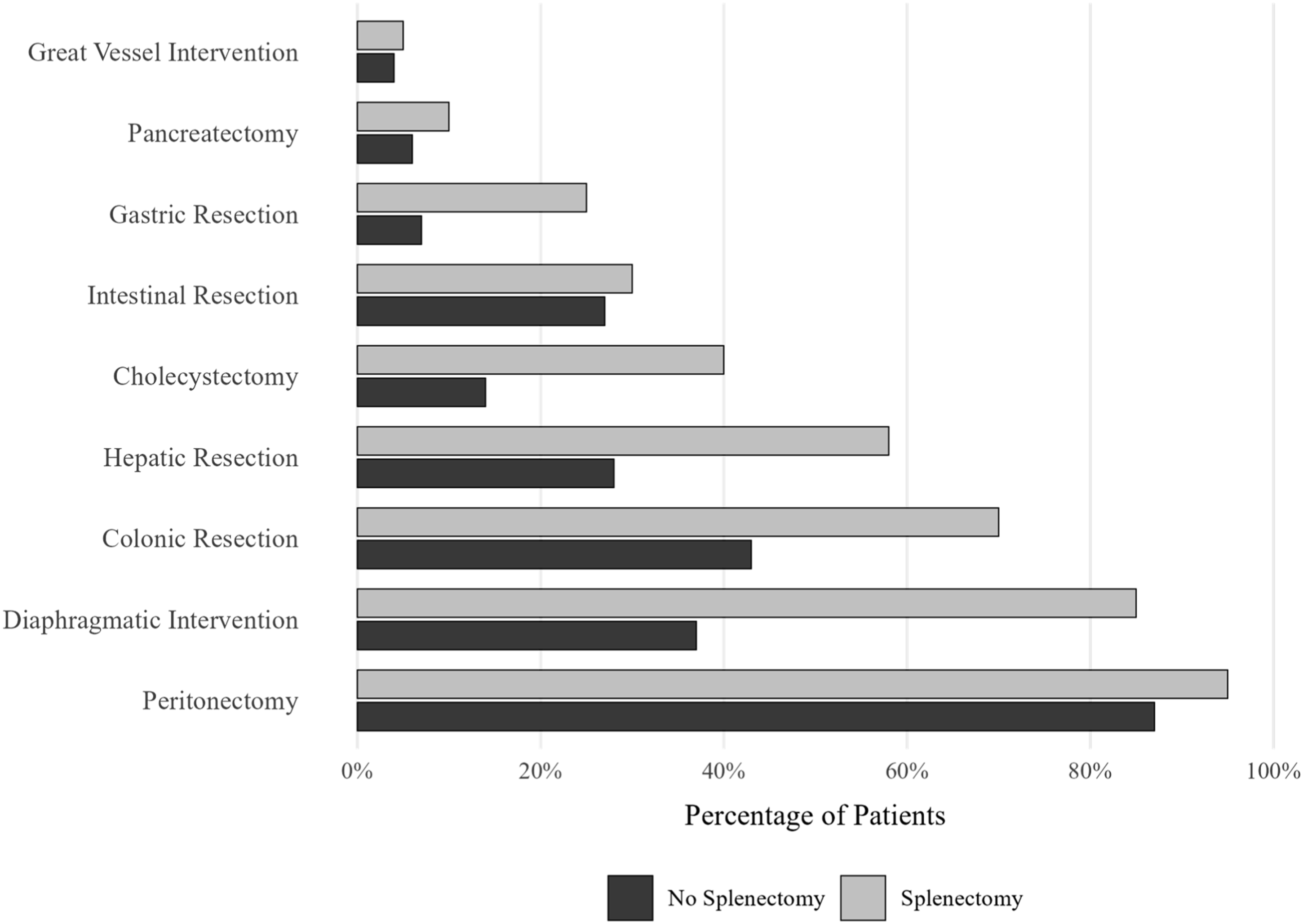
Concomitant Resections Performed in Patients Undergoing Splenectomy During Cytoreductive Surgery (n = 20)
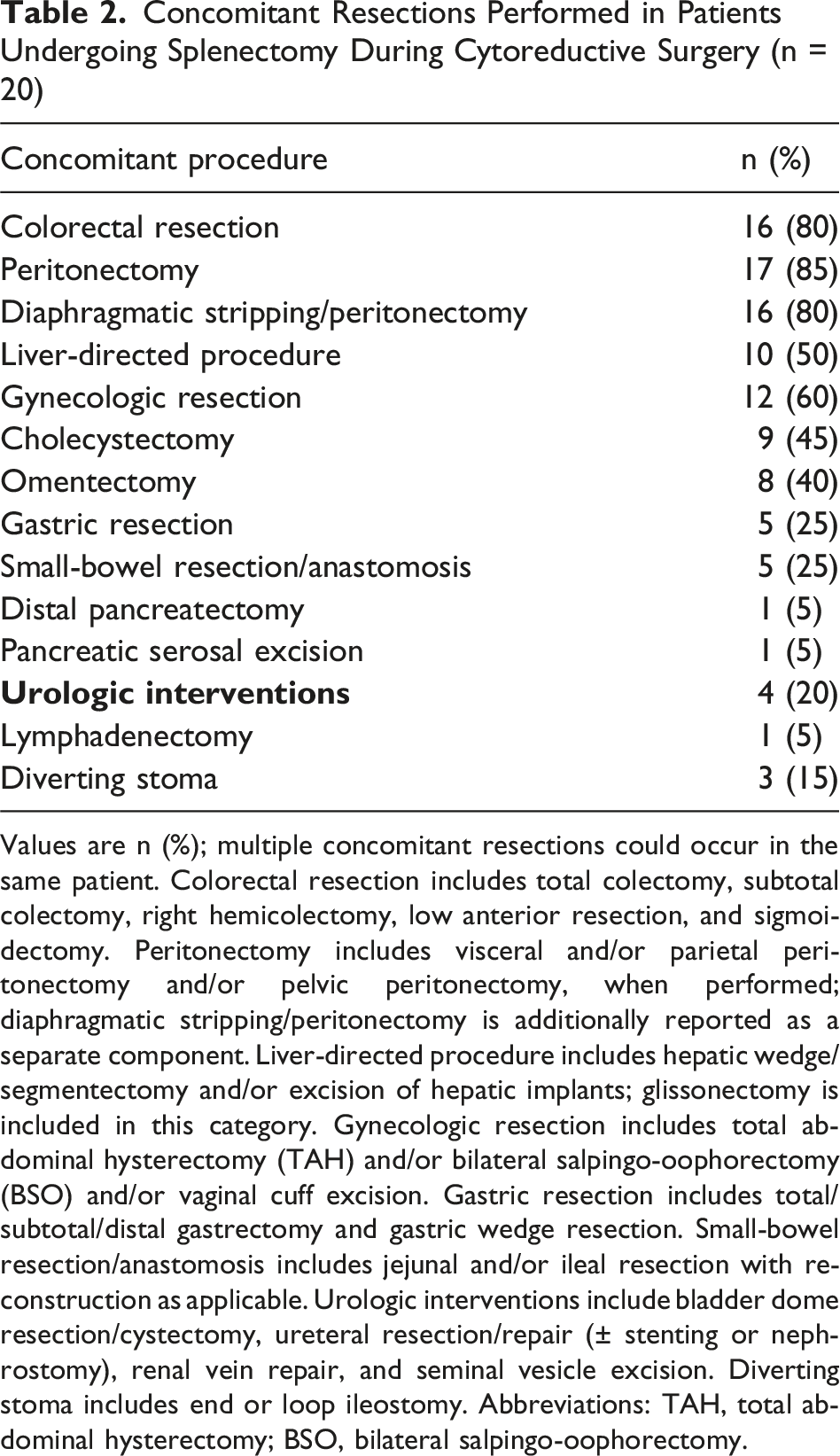
Values are n (%); multiple concomitant resections could occur in the same patient. Colorectal resection includes total colectomy, subtotal colectomy, right hemicolectomy, low anterior resection, and sigmoidectomy. Peritonectomy includes visceral and/or parietal peritonectomy and/or pelvic peritonectomy, when performed; diaphragmatic stripping/peritonectomy is additionally reported as a separate component. Liver-directed procedure includes hepatic wedge/segmentectomy and/or excision of hepatic implants; glissonectomy is included in this category. Gynecologic resection includes total abdominal hysterectomy (TAH) and/or bilateral salpingo-oophorectomy (BSO) and/or vaginal cuff excision. Gastric resection includes total/subtotal/distal gastrectomy and gastric wedge resection. Small-bowel resection/anastomosis includes jejunal and/or ileal resection with reconstruction as applicable. Urologic interventions include bladder dome resection/cystectomy, ureteral resection/repair (± stenting or nephrostomy), renal vein repair, and seminal vesicle excision. Diverting stoma includes end or loop ileostomy. Abbreviations: TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy.
Comparison of Operative and Postoperative Outcomes Between Patients With and Without Splenectomy
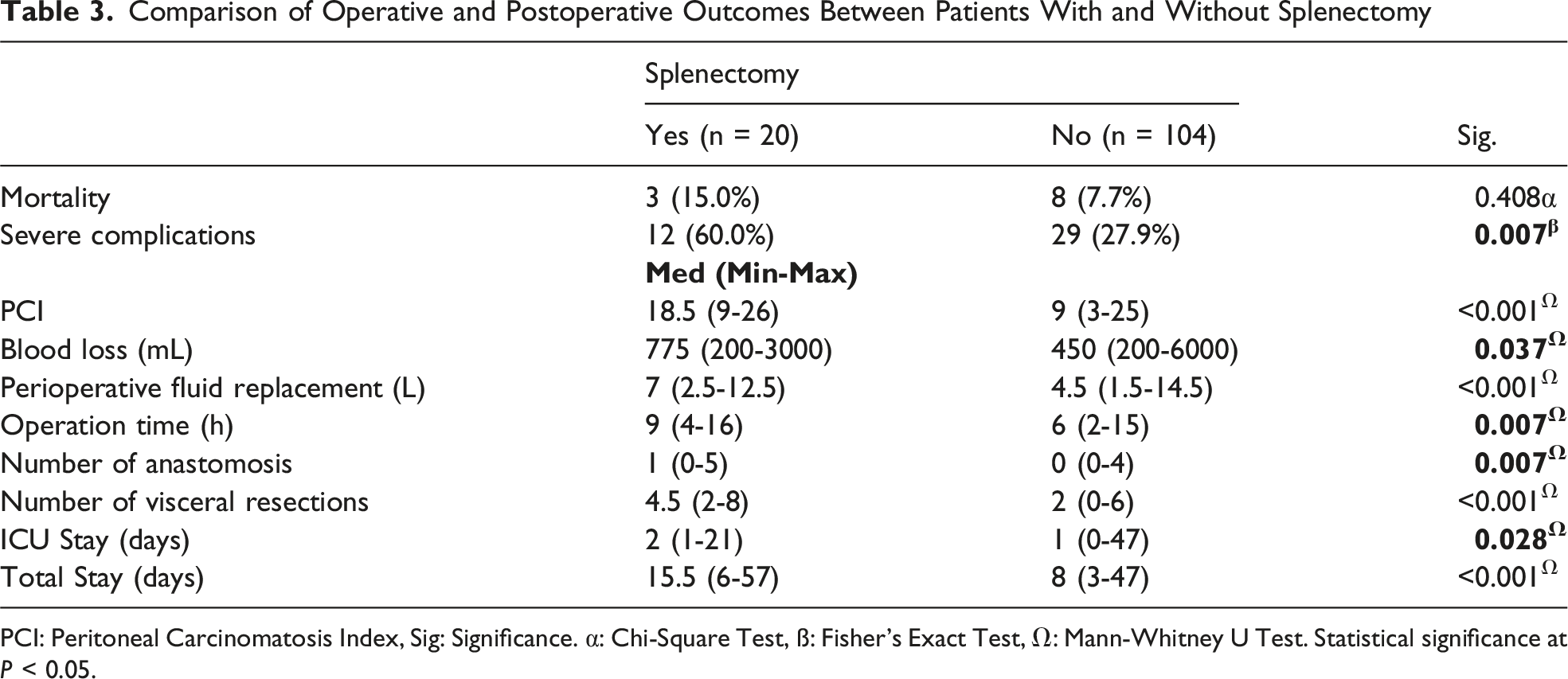
PCI: Peritoneal Carcinomatosis Index, Sig: Significance. α: Chi-Square Test, ß: Fisher’s Exact Test, Ω: Mann-Whitney U Test. Statistical significance at P < 0.05.
In exploratory univariate logistic regression, splenectomy was significantly associated with a higher risk of severe complications (OR 3.8, 95% CI 1.44-10.46, P = 0.007). However, this effect was not sustained in multivariate analysis (OR 1.3, 95% CI 0.28-3.80, P = .957). Other operative factors, including PCI, number of resections, and operative time, also demonstrated associations in univariate analysis but lost significance after adjustment, whereas ASA score (OR 3.6, 95% CI 1.57-8.57, P = 0.003), perioperative fluid replacement (OR: 1.35 95% CI: 1.00-1.85 P = .045), and blood loss (OR: 2.22 95% CI: 1.04-4.74 P = .038) showed significance(Figure 4). The instability and wide confidence intervals of these models reflected collinearity and limited sample size, supporting the use of propensity score methods to more reliably adjust for confounding. Multivariate logistic regression analysis for severe postoperative complications ASA = American Society of Anesthesiologists; PCI = Peritoneal Cancer Index; CI = Confidence Interval. The forest plot illustrates odds ratios with 95% confidence intervals for variables included in the multivariate logistic regression model. Higher ASA score and increased perioperative fluid replacement were independently associated with severe complications, whereas splenectomy itself was not an independent predictor after adjustment for operative and patient factors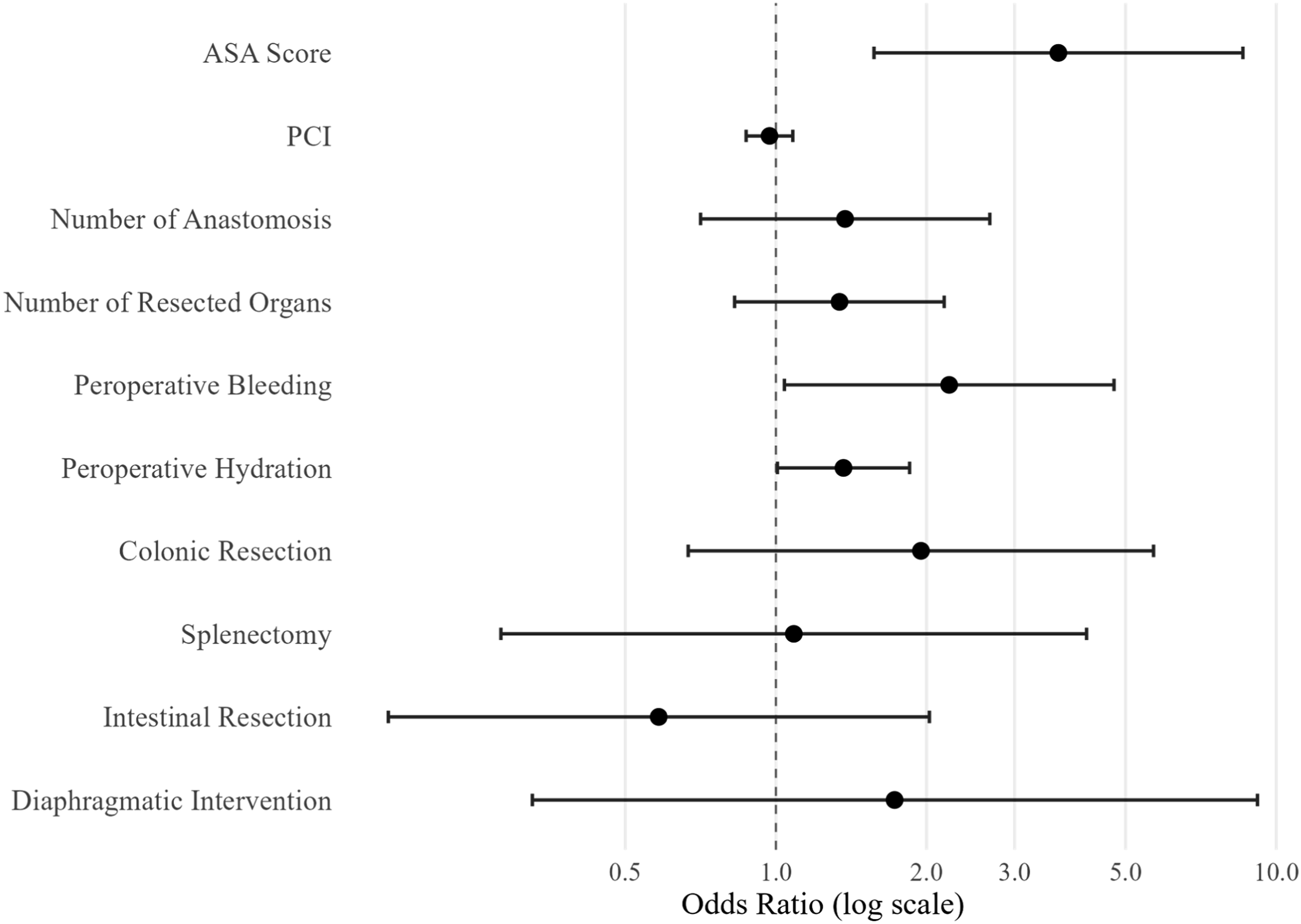
Propensity Score-based Analysis of Postoperative Outcomes According to Splenectomy Status
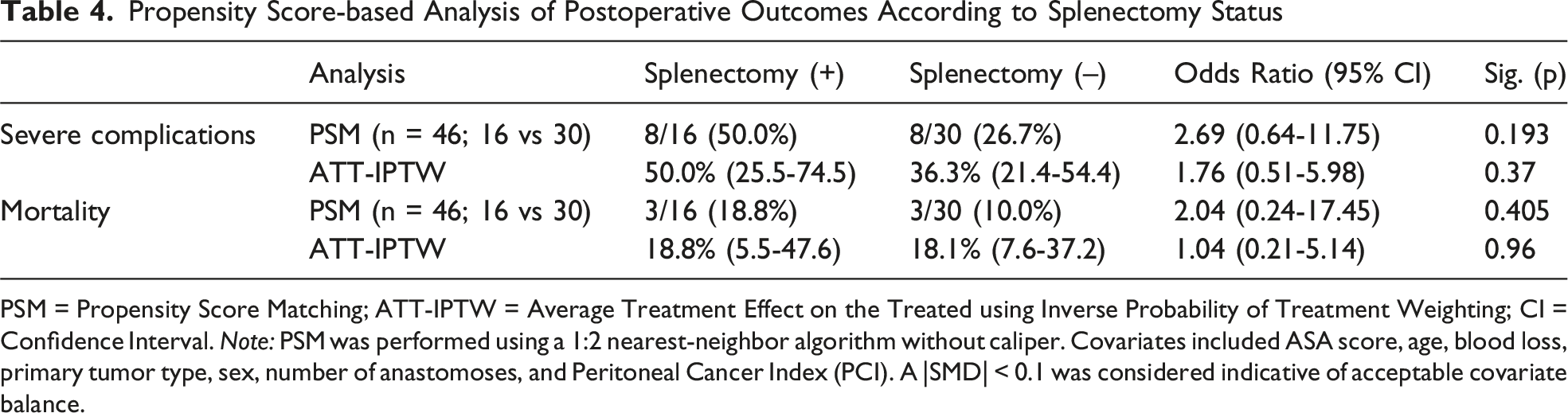
PSM = Propensity Score Matching; ATT-IPTW = Average Treatment Effect on the Treated using Inverse Probability of Treatment Weighting; CI = Confidence Interval. Note: PSM was performed using a 1:2 nearest-neighbor algorithm without caliper. Covariates included ASA score, age, blood loss, primary tumor type, sex, number of anastomoses, and Peritoneal Cancer Index (PCI). A |SMD| < 0.1 was considered indicative of acceptable covariate balance.
ATT-IPTW weighted cohort, covariate balance was achieved across almost baseline variables (|SMD|<0.1). The weighted risk of severe complications was 50.0% (95% CI, 25.5-74.5) in the splenectomy group and 36.3% (95% CI, 21.4-54.4) in controls, yielding an OR of 1.76 (95% CI, 0.51-5.98; P = .37). Weighted mortality rates were 18.8% (95% CI, 5.5-47.6) vs 18.1% (95% CI, 7.6-37.2), with an OR of 1.04 (95% CI, 0.21-5.14; P = .96) (Table 4).
Across both PSM and IPTW analyses, patients undergoing splenectomy had numerically higher complication rates compared with controls. However, these differences did not reach statistical significance, and mortality remained similar between groups.
Discussion
This study explored whether splenectomy performed during CRS, with or without HIPEC, contributes directly to postoperative complications or mainly reflects the extent of disease and surgical effort. We observed that, in the unadjusted analysis, patients who underwent splenectomy had markedly higher rates of severe complications (60% vs 27%; P = .007) and longer hospital stays (median 15.5 vs 8.0 days; P < .001). However, after adjusting for baseline differences using PSM and IPTW, splenectomy was not identified as an independent risk factor. In both adjusted models, splenectomy remained associated with numerically higher rates of severe complications, though the differences were not statistically significant (PSM: OR = 2.69, P = 0.193; IPTW: OR = 1.76, P = 0.37). Given the limited number of splenectomy cases, these estimates should be interpreted with caution, as reduced power and residual confounding may have contributed to wider uncertainty and non-significant findings despite a consistent direction of effect. Mortality rates were comparable between the groups. As far as we know, this is the first study to evaluate the impact of splenectomy on postoperative complications in patients undergoing cytoreductive surgery using a propensity score-based methodology. The only PSM-based literature on the subject compares survival outcomes in splenectomized patients. 7
Prior studies report an increase in severe complications with added splenectomy during CRS, however, also reflect an increase in operation duration, blood perfusions, and disease complexity.5,8,9 A recent meta-analysis also reports similar results confirming that splenectomy is associated with higher incidence of complications. 6 However, all these studies might have missed something rather important that splenectomy may have been an indicator for disease severity rather that indicator for postoperative morbidity. In our study, similarly to prior studies, in conventional statistical analyses there was a significant increase in postoperative complications. Also similarly, in splenectomy patients PCI (median: 18.5 vs 9, P < 0.001), blood loss (median: 775 mL vs 450 mL, P = .037), operation duration (median: 9 vs 6, P = .007), and number of different visceral resections (median: 4.5 vs 2 P < .001) were higher. Accordingly, our findings do not contradict the existing literature; rather, they refine it by demonstrating that the observed excess morbidity is strongly intertwined with overall surgical burden.
That said, the trend toward more complications among splenectomy patients remained visible across all analyses. While this pattern did not reach statistical significance after adjustment, it may still be clinically relevant, particularly in the setting of limited sample size. The spleen plays an important role in immune regulation and in maintaining hematologic and inflammatory balance. Its removal can increase vulnerability to infection and may subtly alter recovery after major surgery. Within the already intense physiological stress of CRS, even small differences in immune response could affect how patients recover. Furthermore the effect of added splenectomy associated with certain specific complications including pneumonia, pancreatic fistula, sepsis, and febrile events.10,11
The purpose of splenectomy is mostly to achieve complete cytoreduction due to splenic involvement of the disease and occasionally due to iatrogenic splenic injuries. 12 In selected cases where splenic preservation is technically feasible and oncologically safe, it may be reasonable to avoid unnecessary splenectomy. However, complete cytoreduction remains the ultimate goal, and splenic preservation should not compromise that principle. From a practical standpoint, these findings suggest that splenectomy should neither be avoided nor considered trivial. When oncologically necessary, it can be performed safely as part of comprehensive cytoreduction. However, its occurrence signals a patient likely to experience a more demanding postoperative course. Surgeons and perioperative teams should therefore anticipate potential complications and implement preventive measures accordingly.
Conclusions
In summary, splenectomy during cytoreductive surgery is associated with higher observed morbidity but not with independently increased risk after accounting for operative complexity. The consistent numerical differences reflect the reality that splenectomy accompanies more extensive and technically demanding procedures. These findings emphasize the importance of interpreting splenectomy not as an isolated hazard but as part of the broader context of surgical burden. When performed for appropriate oncologic reasons, splenectomy remains an acceptable component of CRS, provided that perioperative care is optimized and patients are carefully monitored for complications inherent to extensive cytoreduction.
Future Directions
Future research should aim to validate these observations in larger, multicenter cohorts with standardized recording of operative detail. Differentiating between therapeutic and incidental splenectomy could clarify whether outcomes differ according to indication. Integration of objective surgical complexity scores and postoperative inflammatory markers might further illuminate whether splenectomy independently modulates systemic stress or merely co-occurs with it. Such data would support evidence-based guidance on splenic preservation, perioperative prophylaxis, and postoperative monitoring strategies.
Strengths and Limitations
A notable strength of this study is the use of complementary propensity score techniques. PSM enabled a focused comparison among well-matched cases, while IPTW leveraged the full cohort to maintain statistical efficiency. The convergence of results across these methods adds robustness to the interpretation. Inclusion of both patient-related (age, ASA) and procedure-related (PCI, blood loss, number of anastomoses) variables in the adjustment model provided a realistic control for confounding inherent to complex oncologic surgery.
Still, several limitations must be recognized. The retrospective, single-center nature of the study introduces potential selection bias. The modest number of splenectomy cases limits statistical power and increases the risk of imprecise estimates, which may explain why clear numerical differences did not achieve significance. Residual confounding cannot be fully excluded despite propensity score adjustment. Furthermore, multicollinearity among operative variables—typical in CRS datasets—complicates regression modeling and inflates confidence intervals. Finally, this analysis was restricted to short-term morbidity and mortality; longer-term infectious or hematologic consequences of splenectomy were not captured.
Footnotes
Ethics Considerations
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of the University of Health Sciences, Ümraniye Education and Research Hospital (Approval No: 2024/B.10.1.THK.4.34.H.GP.0.01/186).
Consent to Participate
The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study, in accordance with national regulations and institutional guidelines. All patient data were fully anonymized to ensure confidentiality.
Consent for Publication
Not applicable. This study does not include identifying images or personal/clinical details of participants that compromise anonymity.
Authors’ Contributions
F.B., O.E., and A.A: the concept and design of the study and data acquisition; A.A., T.C., A.K., and C.Y.: statistical analysis; interpreted the results; analyzed the data and drafted the manuscript; and critically revised the manuscript; all authors approved the final version to be published and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
During the preparation of this work, the author(s) used ChatGPT, a generative AI tool by OpenAI, to improve readability and language. After using this tool, the author(s) carefully reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.