
Abstract
Background
Medicaid expansion under the Affordable Care Act has been associated with improved colorectal cancer (CRC) outcomes, predominantly attributed to earlier diagnosis and stage migration. However, it remains unclear whether survival benefits vary across disease stages.
Objective
To evaluate cancer-specific survival (CSS) after Medicaid expansion across disease stages among working-age adults with CRC, comparing the expansion state of California with the non-expansion state of Texas.
Methods
We conducted a retrospective cohort study using Surveillance, Epidemiology, and End Results (SEER) registry data (2007-2021) for patients aged 18-64 years with primary CRC. A difference-in-differences design compared pre-ACA (2007-2013) and post-ACA (2015-2021) periods between California and Texas. CSS was modeled using Cox proportional hazards regression adjusting for demographics, tumor characteristics, and treatments. Analyses were stratified by disease stage (localized, regional, distant) and race/ethnicity.
Results
Among 122,543 patients, CSS improved after Medicaid expansion in California relative to Texas. Stage-stratified difference-in-differences models showed a modest reduction in cancer-specific mortality for localized disease 0.985 (0.974-0.996), a larger reduction for regional disease 0.941 (0.900-0.983), and the greatest reduction for distant metastatic disease 0.689 (0.525-0.903). Improvements were consistent across racial/ethnic groups, with the largest relative reduction among non-Hispanic Black patients 0.855 (0.763-0.958).
Conclusion
Medicaid expansion was associated with stage-dependent improvements in CRC survival, with the most pronounced benefit for patients with metastatic disease. These findings suggest that enhanced access to systemic therapy, multidisciplinary care, and financial protection may yield survival gains beyond those mediated by stage shift alone.
Key Takeaways
• Medicaid expansion was associated with better colorectal cancer survival, with the largest benefit in metastatic disease. • Survival gains in advanced disease suggest that improved treatment access, not stage shift alone, may drive benefit. • Stage-specific evaluation of policy effects is essential for identifying where coverage expansion has the greatest clinical impact.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer and the second leading cause of cancer-related death in the United States.1,2 The Affordable Care Act (ACA) sought to improve insurance coverage and health outcomes through Medicaid expansion.3,4 California implemented expansion in 2014, whereas Texas did not.5-7 Prior studies report that expansion increased screening, shifted diagnoses toward earlier stages, and improved overall survival.8,9 However, the extent to which survival benefits vary across disease stages remains unclear.
Emerging evidence suggests that stage migration explains only part of the survival improvement associated with Medicaid expansion.10,11 A recent analysis indicated that reductions in distant-stage diagnoses mediated about 58% of the mortality reduction after expansion; additional benefits may derive from improved access to treatment, continuity of care, and financial protection. 12
In this study, we compared CRC outcomes in California vs Texas using a difference-in-differences design, focusing on stage-stratified survival. We hypothesized that while Medicaid expansion would be associated with reduced mortality overall, the magnitude of benefit would differ by disease stage, with the greatest gains among patients with metastatic disease who face intensive treatment and financial barriers.
Methods
Study Design and Data Source
This study employed a retrospective cohort design using data from the Surveillance, Epidemiology, and End Results (SEER) cancer registry to assess the impact of Medicaid expansion on colorectal cancer outcomes. The study population included individuals aged 18 to 64 years diagnosed with colorectal cancer between 2007 and 2021. The dataset was structured to compare patients from California (expansion state) and Texas (non-expansion state) to evaluate the differential effects of Medicaid expansion on cancer-specific survival (CSS).
Population and Inclusion Criteria
The cohort was restricted to residents of California (an expansion state) and Texas (a non-expansion state). Patients were categorized by period into pre-Affordable Care Act (ACA; 2007-2013) and post-ACA (2015-2021) eras. Inclusion required complete data on age, sex, race/ethnicity, stage at diagnosis, tumor grade (well differentiated, moderately differentiated, poorly/undifferentiated, or unknown), treatment variables, and follow-up. We censored individuals at the date of last known follow-up or death due to causes other than CRC.
Primary Explanatory Variable
The exposure of interest was Medicaid expansion, operationalized as a binary indicator equal to 1 for observations in California after January 1, 2014 and 0 otherwise. This variable captures the policy change attributable to Medicaid expansion, with Texas serving as the control state. To assess heterogeneity by stage, we interacted this policy indicator with stage categories and calendar period.
Outcome Measures
The primary outcome was cancer-specific survival, defined as the time from diagnosis to death attributable to CRC. Cause of death was identified using SEER’s cause-specific death classification. Patients alive at last follow-up or who died from other causes were censored.
Covariates
To control for potential confounding, we included a comprehensive set of demographic, socioeconomic, and clinical covariates in all models. Demographic variables—age, sex, and race/ethnicity—were used to adjust for baseline differences between California and Texas. Socioeconomic factors such as household income, categorized as less than US $65 000 vs at least US $65 000, and metropolitan vs non-metropolitan residence were added to capture disparities in healthcare access. Clinical characteristics included the stage of disease at diagnosis (localized, regional, or distant) and receipt of treatment modalities like surgery and chemotherapy. Adjusting for these covariates allowed for robust comparison of cancer-specific survival between expansion and non-expansion states.
Statistical Analysis
We employed a difference-in-differences (DID) framework within a Cox proportional hazards model to estimate the effect of Medicaid expansion on cancer-specific survival (CSS) while accounting for secular trends and baseline differences between California and Texas. The key analytic term was a three-way interaction between the post-ACA period indicator, the state indicator (California vs Texas), and disease stage (localized, regional, distant). The model included main effects for period, state, stage, and grade, along with two-way interactions (post × stage and state × stage) to ensure proper interpretation of the three-way term. The three-way interaction Post × California × Stage estimates whether the change in hazard after Medicaid expansion differs across stages. A similar specification was used to explore heterogeneity by race/ethnicity, replacing the stage variable with the corresponding race/ethnicity variable in the interaction.
Hazard ratios (HRs) and 95% confidence intervals (CIs) were derived from exponentiated model coefficients. Absolute and relative risk reductions were calculated as 1 − HR to provide clinically meaningful effect sizes. All analyses were conducted using Stata 16 (StataCorp).
Results
Baseline Demographic and Clinical Characteristics of Patients With Colorectal Cancer in Texas and California Pre- and Post-ACA Implementation
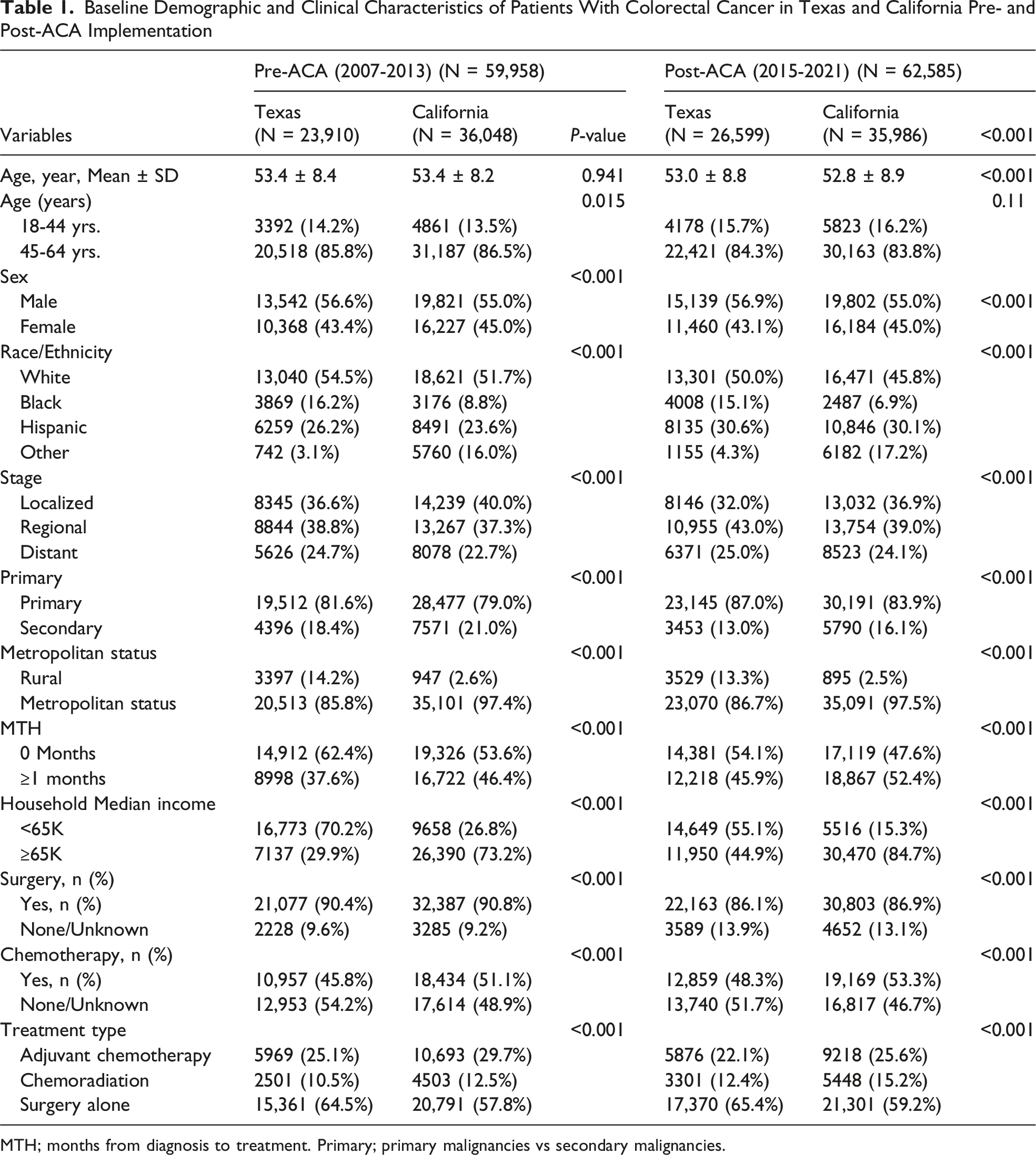
MTH; months from diagnosis to treatment. Primary; primary malignancies vs secondary malignancies.
The racial/ethnic mix differed significantly. Before expansion, Texas had higher proportions of Black (16.2% vs 8.8%) and Hispanic (26.2% vs 23.6%) patients, whereas California had more patients categorized as “Other” (16.0% vs 3.1%) these differences persisted post-expansion (P < 0.001). Stage at presentation also varied by state: localized disease was more common in California (40.0% vs 36.6% pre-ACA; 36.9% vs 32.0% post-ACA), whereas regional-stage disease predominated in Texas after expansion (43.0% vs 39.0%; P < 0.001).
Socioeconomic disparities were notable. In Texas, 70.2% of patients resided in neighborhoods with median household incomes <US $65 000 before expansion, compared with 26.8% in California (P < 0.001); even after expansion, lower-income households remained more common in Texas (55.1% vs 15.3%). Rural residence was far more prevalent in Texas (14.2% vs 2.6% pre-ACA; 13.3% vs 2.5% post-ACA; P < 0.001). Time to treatment also differed: 46.4% of California patients waited ≥1 month for therapy pre-expansion compared with 37.6% in Texas (P < 0.001); the gap widened post-expansion (52.4% vs 45.9%; P < 0.001).
Treatment patterns reflected these differences. California patients were more likely to receive chemotherapy (51.1% vs 45.8% pre-ACA; 53.3% vs 48.3% post-ACA; both P < 0.001) and chemoradiation, whereas surgery alone was more common in Texas (64.5% vs 57.8% pre-ACA; 65.4% vs 59.2% post-ACA; P < 0.001). These baseline imbalances highlight why adjustment for sociodemographic and clinical covariates—and the stage-stratified difference-in-differences approach—is essential for isolating the effect of Medicaid expansion on survival (Table 1).
Hazard Ratio and Relative Risk Reduction after Medicaid Expansion, by Stage
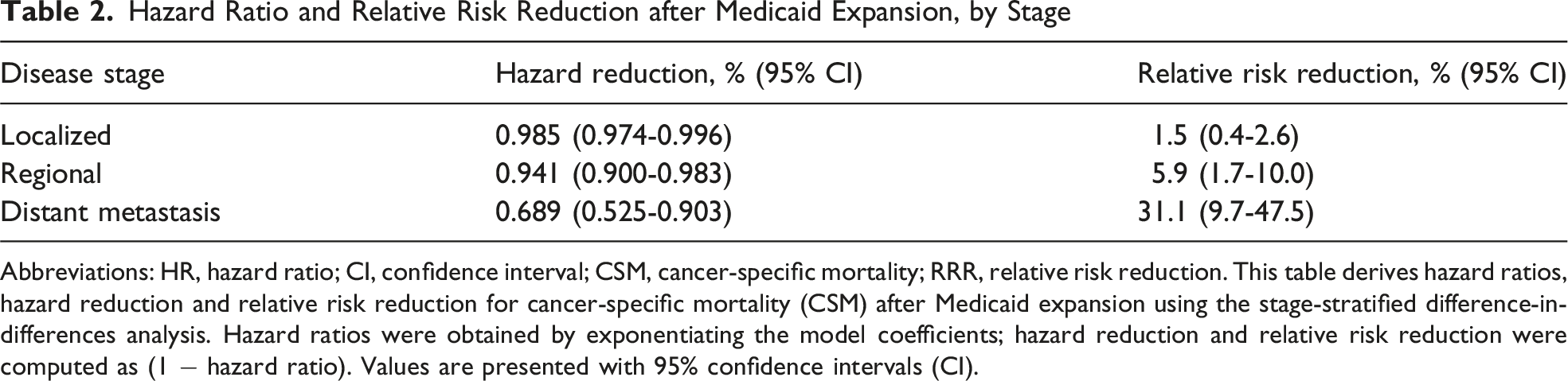
Abbreviations: HR, hazard ratio; CI, confidence interval; CSM, cancer-specific mortality; RRR, relative risk reduction. This table derives hazard ratios, hazard reduction and relative risk reduction for cancer-specific mortality (CSM) after Medicaid expansion using the stage-stratified difference-in-differences analysis. Hazard ratios were obtained by exponentiating the model coefficients; hazard reduction and relative risk reduction were computed as (1 − hazard ratio). Values are presented with 95% confidence intervals (CI).
Hazard Ratio and Relative Risk Reduction after Medicaid Expansion, by Race/Ethnicity
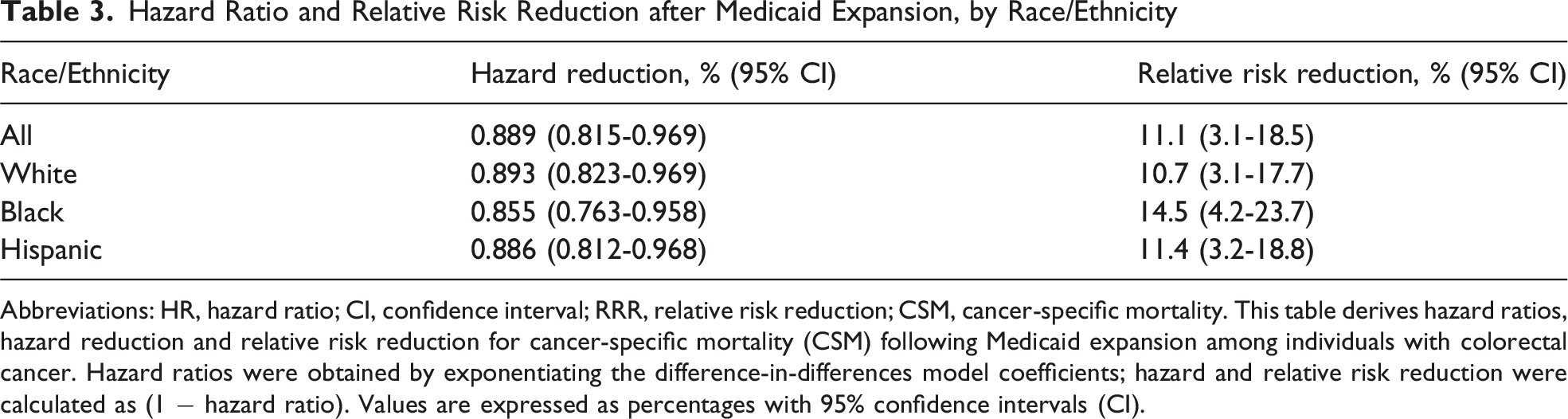
Abbreviations: HR, hazard ratio; CI, confidence interval; RRR, relative risk reduction; CSM, cancer-specific mortality. This table derives hazard ratios, hazard reduction and relative risk reduction for cancer-specific mortality (CSM) following Medicaid expansion among individuals with colorectal cancer. Hazard ratios were obtained by exponentiating the difference-in-differences model coefficients; hazard and relative risk reduction were calculated as (1 − hazard ratio). Values are expressed as percentages with 95% confidence intervals (CI).
Table 3 demonstrates that survival improvements after Medicaid expansion were evident across all racial and ethnic groups but varied in magnitude. Among all patients combined, the HR was 0.889 (95% CI, 0.815-0.969), corresponding to an 11.1% relative risk reduction (95% CI, 3.1-18.5%). When stratified, the greatest benefit was observed among Black individuals (HR = 0.855; 95% CI, 0.763-0.958), yielding a 14.5% relative risk reduction (95% CI, 4.2-23.7%). Hispanic patients also experienced significant improvement (HR = 0.886; 95% CI, 0.812-0.968; 11.4% relative risk reduction, 95% CI, 3.2-18.8%), whereas White patients saw a more modest benefit (HR = 0.893; 95% CI, 0.823-0.969; 10.7% relative risk reduction, 95% CI, 3.1-17.7%). By emphasizing effect sizes and confidence intervals rather than P-values, these results highlight that Medicaid expansion may narrow racial disparities in colorectal cancer survival by delivering proportionally larger mortality reductions among Black and Hispanic populations.
Discussion
In this population-based study, Medicaid expansion was associated with significant improvements in cancer-specific survival among working-age adults with CRC, and the magnitude of benefit differed by disease stage.
A significant finding was the pronounced reduction in mortality for patients with distant metastatic disease. 8 This pattern suggests that improved access to systemic therapy, multidisciplinary cancer care, and financial protection after Medicaid expansion may yield survival gains beyond those mediated by earlier detection.8,12,13
The modest improvement in survival observed in localized disease likely reflects both stage migration and high baseline survival, whereas the intermediate benefit in regional disease may be driven by better adherence to adjuvant therapy.8,14,15
Many previous studies demonstrate that Medicaid expansion improves survival, with some reporting shifts toward earlier-stage diagnoses.16,17 Our data do not replicate this stage-shift pattern—regional and distant disease increased in both California and Texas during the post-ACA period, reflecting a well-documented national secular trend in colorectal cancer stage distribution.16,17 Notably, survival improved differentially in California despite this parallel stage trend, indicating that mechanisms beyond stage migration—including improved treatment access, care continuity, and financial protection—are driving the observed benefit.8,15
The parallel trends in chemotherapy and chemoradiation utilization across both states do not undermine this conclusion.8,18,19 Aggregate SEER-level treatment rates reflect the full patient population; the survival benefit of Medicaid expansion operates on the margin, concentrated among patients who gained insurance and previously lacked access to guideline-concordant care.8,15 The difference-in-differences framework captures this differential effect precisely because it conditions on secular trends common to both states, isolating the policy-attributable survival gain.8,15,18 Taken together, the co-occurrence of declining early-stage diagnoses, parallel aggregate treatment trends, and yet differential survival improvement in California constitutes strong evidence that Medicaid expansion’s survival benefit operates through treatment access and financial protection on the newly insured margin—not through population-level stage migration or treatment intensification.
The hazard ratios in Tables 2 and 3 require brief clarification. They represent the exponentiated three-way interaction coefficient (Post × California × Stage or Race/Ethnicity) from the Cox model—not a simple pre-to-post comparison within California, nor a cross-sectional California vs Texas comparison. This estimand captures the additional change in cancer-specific mortality hazard in California after expansion, above and beyond secular trends shared by both states and any pre-existing between-state survival differential. A hazard ratio below 1.0 therefore reflects a differential mortality reduction in California attributable to the policy, with the pre-expansion baseline inherently conditioned upon by the difference-in-differences design.
These results support policy initiatives aimed at ensuring continuous insurance coverage and comprehensive cancer care for patients with advanced malignancies.8,10,11,15
Survival gains across racial and ethnic groups further suggest that Medicaid expansion may reduce disparities in cancer outcomes.20,21 The larger relative improvement among Black and Hispanic patients underscores the potential of coverage expansion to mitigate long-standing inequities in access to care. 22 As with the stage-stratified estimates, the race-stratified hazard ratios in Table 3 represent DID interaction coefficients that capture differential changes in California relative to Texas after expansion, above and beyond pre-existing between-state racial survival differentials—meaning that the pre-expansion racial mortality gap between states is inherently conditioned upon by the model design.
Limitations
This study has limitations inherent to observational research. We used retrospective registry data and lacked information on insurance status at the individual level, adherence to therapy, and comorbidities.
Although difference-in-differences modeling adjusts for secular trends, unmeasured confounders may persist.
The SEER registry covers only a subset of Texas counties, which could affect generalizability.
Finally, our stage-stratified analysis did not account for specific treatments received after diagnosis; future research should evaluate how access to chemotherapy, targeted therapy, and supportive care mediates survival gains.
Conclusion
Medicaid expansion was associated with improved CRC survival in California relative to Texas, and the survival benefit varied by disease stage.
The greatest reduction in cancer-specific mortality occurred among patients with distant metastatic disease. Critically, these survival gains were observed within each stage stratum and thus cannot be attributed to stage migration alone, suggesting that improved access to treatment and financial protection—rather than earlier detection—are the primary mechanisms through which Medicaid expansion improved outcomes in this cohort.
Policies aimed at expanding insurance coverage should emphasize comprehensive access to high-quality cancer care across the disease continuum to maximize survival benefits and reduce disparities.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Prior Presentation
Presented at the Southeastern Surgical Congress, Omni Island, Florida, February 2026.