
Abstract
Background
It is difficult to predict which patients will have longer postoperative hospital stays after rectal cancer surgery. We aimed to determine the predictors of a long hospital stay following abdominoperineal resection (APR) for rectal cancer.
Methods
Retrospective cohort analysis of patients diagnosed with rectal adenocarcinoma in the National Cancer Database between 2015 and 2019 with clinical stage I-IV cancers who underwent APR. Multiple linear regression analysis was conducted to determine the predictors of a long hospital stay. A statistical calculator was created to predict the in-hospital length of stay.
Results
7470 patients (63.2% males; mean age: 62.3 years) were included. Median hospital stay was 6 (IQR: 4-8) days. Black patients stayed nearly two days longer compared to other patients (1.9; 95% CI: 1.33-2.49, P < 0.001). Patients with a Charlson Deyo Score of 3 also had a longer length of stay (1.96, 95% CI: 1.02-2.91, P < .001). Robotic surgery was associated with shorter hospital stays (−0.7 days, 95% CI - 1.1, −0.4, P < .001), while conversion from minimally invasive to open surgery was associated with a longer hospital stay (1.1 days, 95% CI: 0.55-1.68, P < .001).
Conclusion
Older age, black race, male sex, and severe comorbidities were associated with longer hospital stays, while minimally invasive surgery was associated with decreased length of stay.
Introduction
An estimated 50,000 cases of rectal cancer will be diagnosed in 2026 in the United States. Rectal cancer makes up nearly one-third of all colorectal cancers diagnosed each year. 1 There has been a dramatic rise in the incidence of rectal cancer since 1990 in young patients (<50 years of age). 2
Despite the advent of neoadjuvant chemoradiation protocols for rectal cancer treatment, surgical resection remains the curative treatment for rectal cancer in the majority of cases.3,4 Abdominoperineal resection (APR), in which the anus, rectum and sigmoid colon are removed, is indicated for low rectal cancers, anal cancers, and inflammatory bowel diseases (IBD) that fail other therapies. 5 APR is the standard of care for ultra-low rectal cancers when a negative distal margin would not be possible, while retaining intestinal continuity, in patients with preoperative fecal incontinence or tumors that invade local structures. 6
APR can be performed as an open or minimally invasive procedure. The type of APR performed is defined by the amount of tissue removed: extrasphincteric, intersphincteric, extralevator, or ischioanal. 7 Intersphincteric APR is limited to patients with IBD or malignancy that does not involve the sphincter complex. Extrasphincteric, or the wider extralevator or ischioanal APRs, are reserved for patients with malignancy that has spread into or beyond the sphincter complex. 8 An ostomy is created in all patients undergoing an APR. The stoma presents a set of challenges for patient adjustment and education after surgery that can lead to a prolonged stay. 9 Additionally, postoperative complications after APR are common and can prolong hospital stay and lead to hospital readmission as well as prolonged healing time. The most common complications after APR are perineal wound-related, including infections, delayed wound healing, and perineal sinuses. 10 Wound complication rates are upwards of 40% overall. 11 Risk factors for complications include preoperative radiation, the creation of pelvic dead space, and the type of perineal closure. The implementation of minimally invasive surgical techniques to APR has improved postoperative outcomes and hastened recovery.
While complications can inevitably extend hospitalization, the overall status of patients, type and approach of surgery, recovery patterns, hospital resources, and discharge policy, and other logistical factors can directly influence hospital stay. Prolonged hospital stays can lead to cognitive declines and functional dependence. 12 Additional hospital days can lead to hospital-acquired infections and increased costs to both the patient and the health care system. 13 The primary aim of the study was to identify patient-, tumor-, and system-level predictors of prolonged hospitalization after APR, which has several potential implications, including improved perioperative risk stratification, optimization of discharge planning and resource allocation, identification of disparities in postoperative recovery, and development of targeted enhanced recovery pathways for high-risk patients.
Materials and Methods
Study Design
A retrospective cohort analysis of patients with rectal cancer was performed using the National Cancer Database (NCDB) (2015-2019). Given the retrospective nature of this study that used deidentified patient data from a national database, ethics/IRB approval was not necessary. The NCDB is a large national database that entails registry data from more than 1,500 hospitals accredited by the Commission on Cancer (CoC) and is a joint project of the CoC of the American College of Surgeons (ACS) and the American Cancer Society. “The ACS and the CoC have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigator”. The aim of our study was to determine the predictors of a long hospital stay after APR in patients with rectal cancer.
Study Population
Inclusion criteria were patients diagnosed with rectal adenocarcinoma (International Classification of Diseases for Oncology, Third Edition [ICD-O-3] codes 8140/3, 8480-8481/3, 8490/3) registered in the NCDB between 2015 and 2019 with clinical stage I-IV cancers who underwent an APR.
Exclusion criteria were patients with stage 0 or an unknown clinical stage. Patients who did not undergo surgery or who underwent rectal resections other than APR were also excluded from the study.
Data Collection
The following patient data were collected and used for the analysis: age, sex, race and ethnicity, Charlson Comorbidity Index score, insurance status, clinical and pathologic TNM (tumor, node, metastasis) stages, facility type, tumor histology and grade, tumor location, neoadjuvant radiation status, and surgical approach. The primary outcome was length of hospital stay.
Statistical Analysis
Statistical analyses were conducted using EZR version 1.55.14, R software version 4.1.2 (The R Foundation), and SPSS version 23 (IBM). 14 Continuous data were reported as mean ± standard deviation (SD) for normally distributed variables or as median with interquartile range (IQR) for non-normally distributed variables. Unpaired two-tailed t-test or Mann-Whitney U test was used to evaluate continuous variables. Categorical data were presented as numbers and percentages and analyzed using Fisher’s exact test or the χ2 test.
Single and multiple linear regression analyses were used to identify factors significantly associated with hospital stay after APR. The large language model ChatGPT version 3.5 was used to write an R code for a statistical calculator incorporating the independent predictors of hospital stay found in the multiple linear regression analysis.
Missing data in primary outcomes were handled using a complete case analysis. Statistical significance was defined as a two-sided P-value of less than 0.05.
Results
Description of the Cohort
Demographic Cohort Description
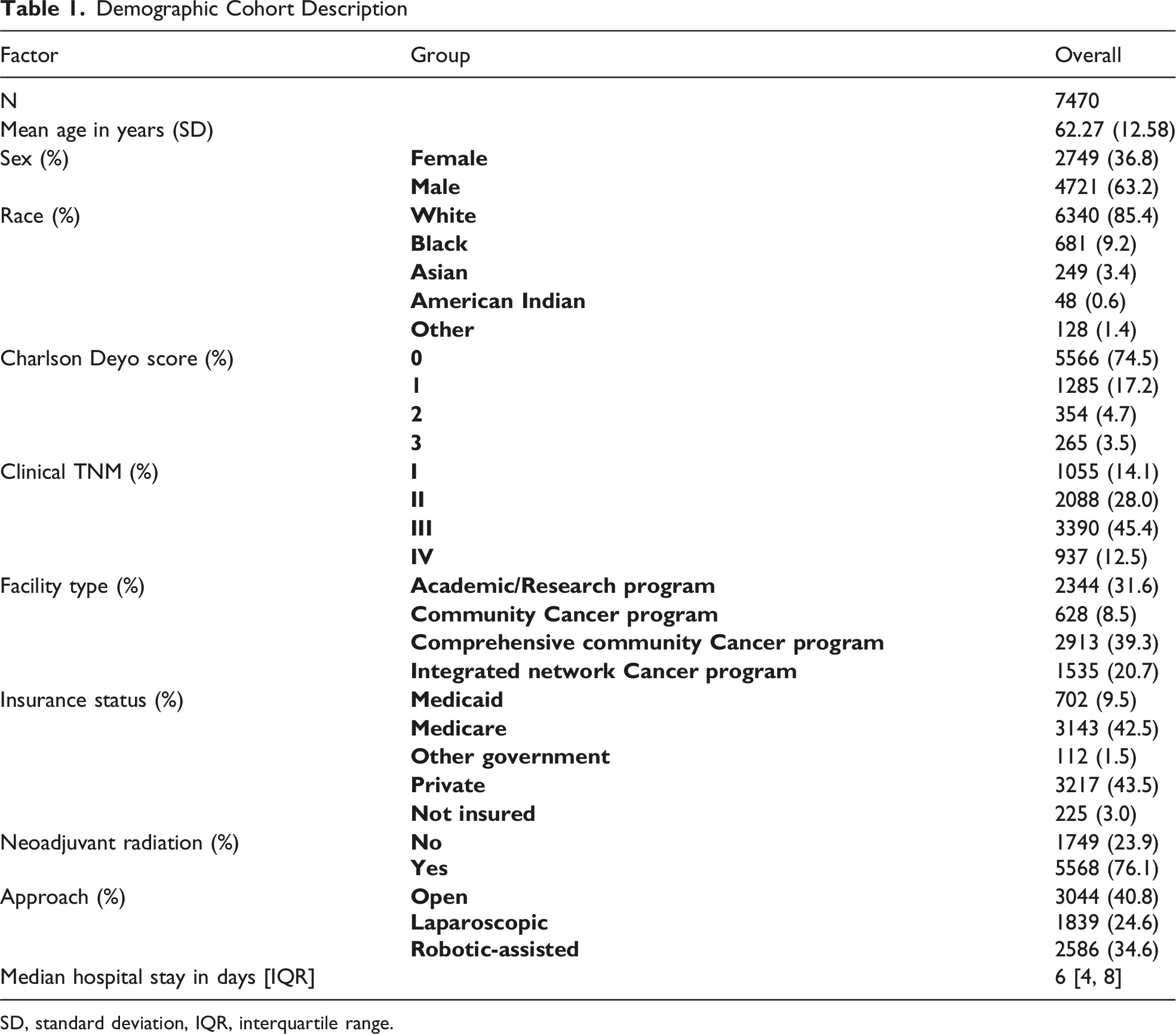
SD, standard deviation, IQR, interquartile range.
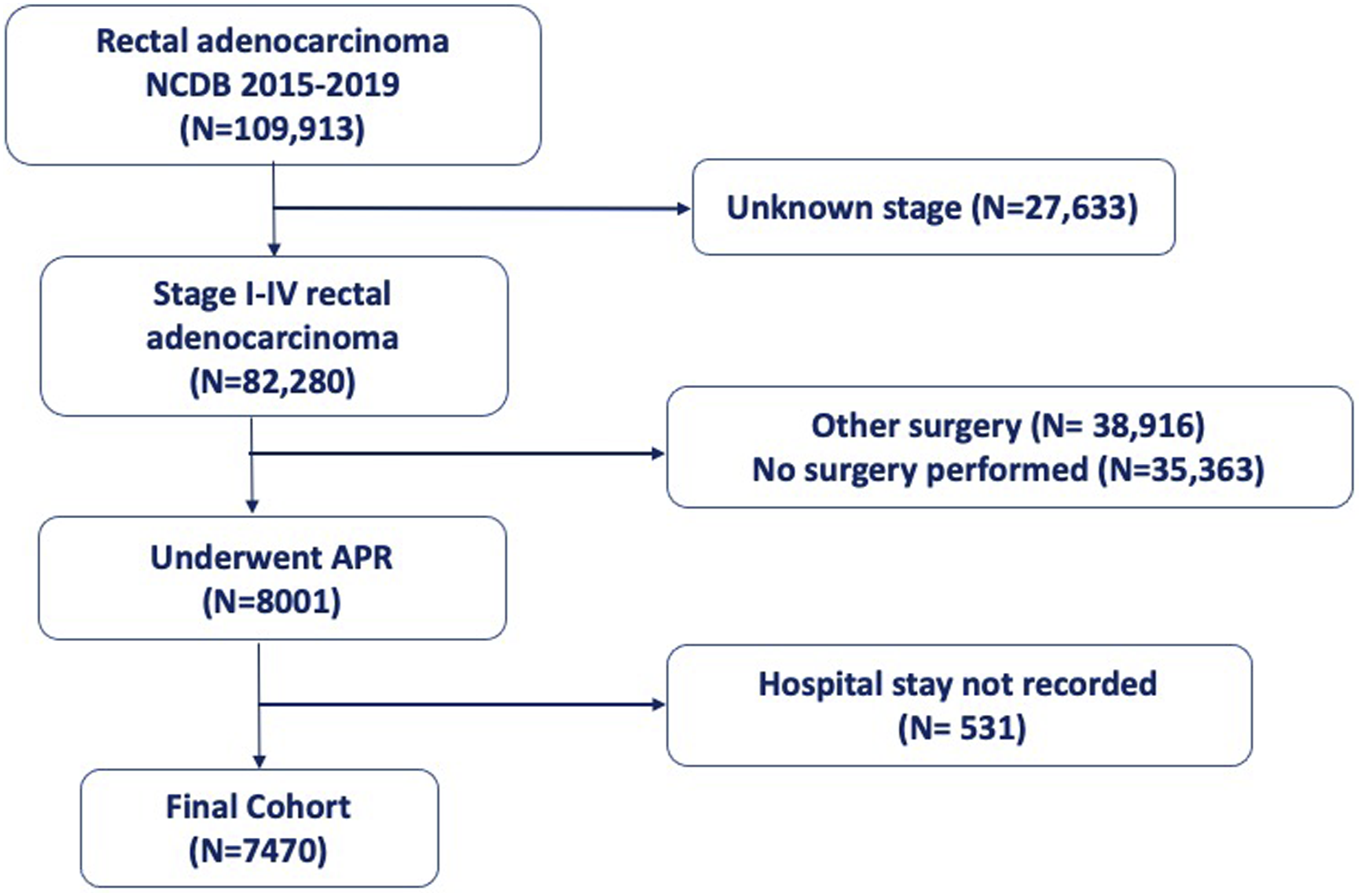
Flow chart hospital stay after APR
Single Linear Regression
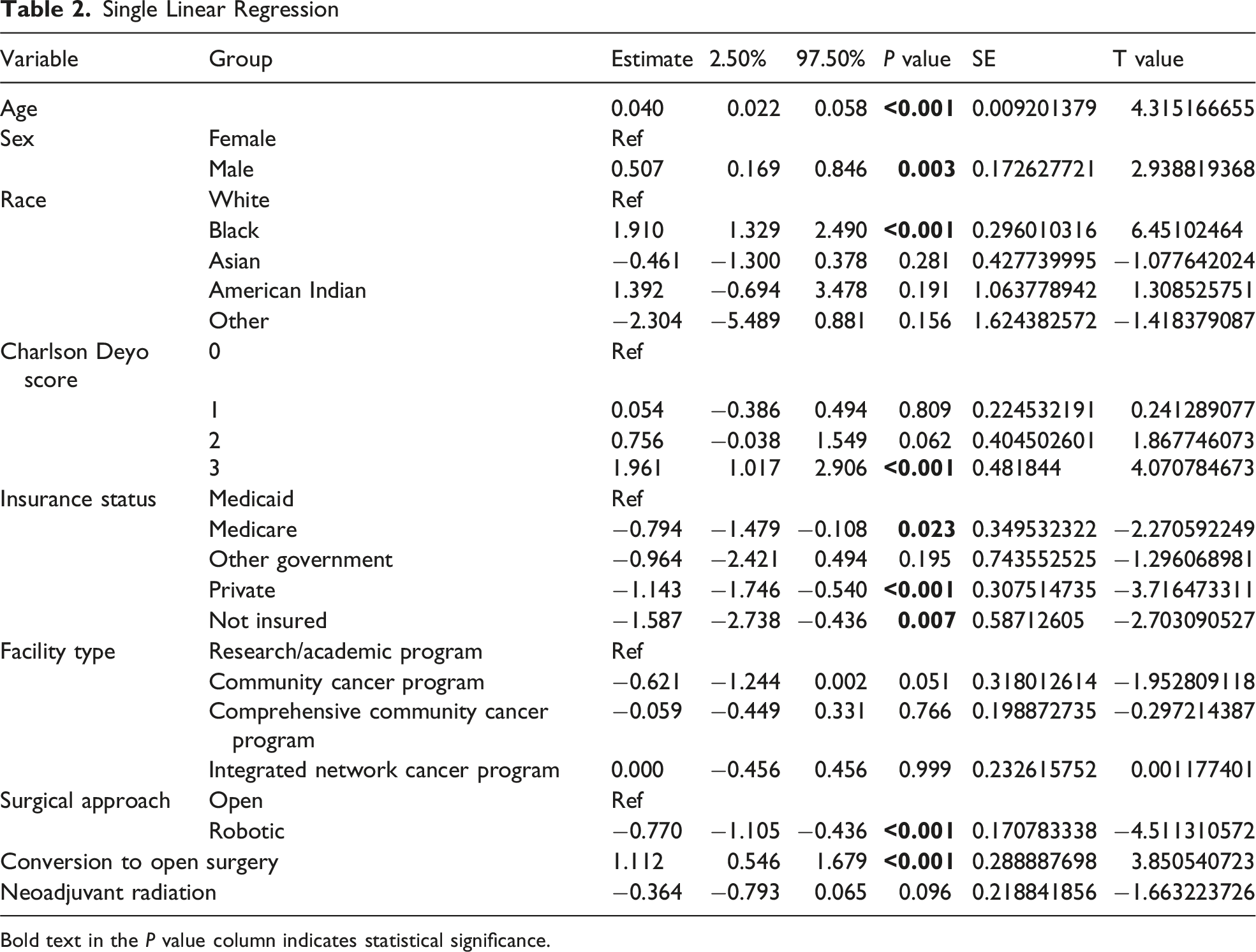
Bold text in the P value column indicates statistical significance.
Multiple Linear Regression
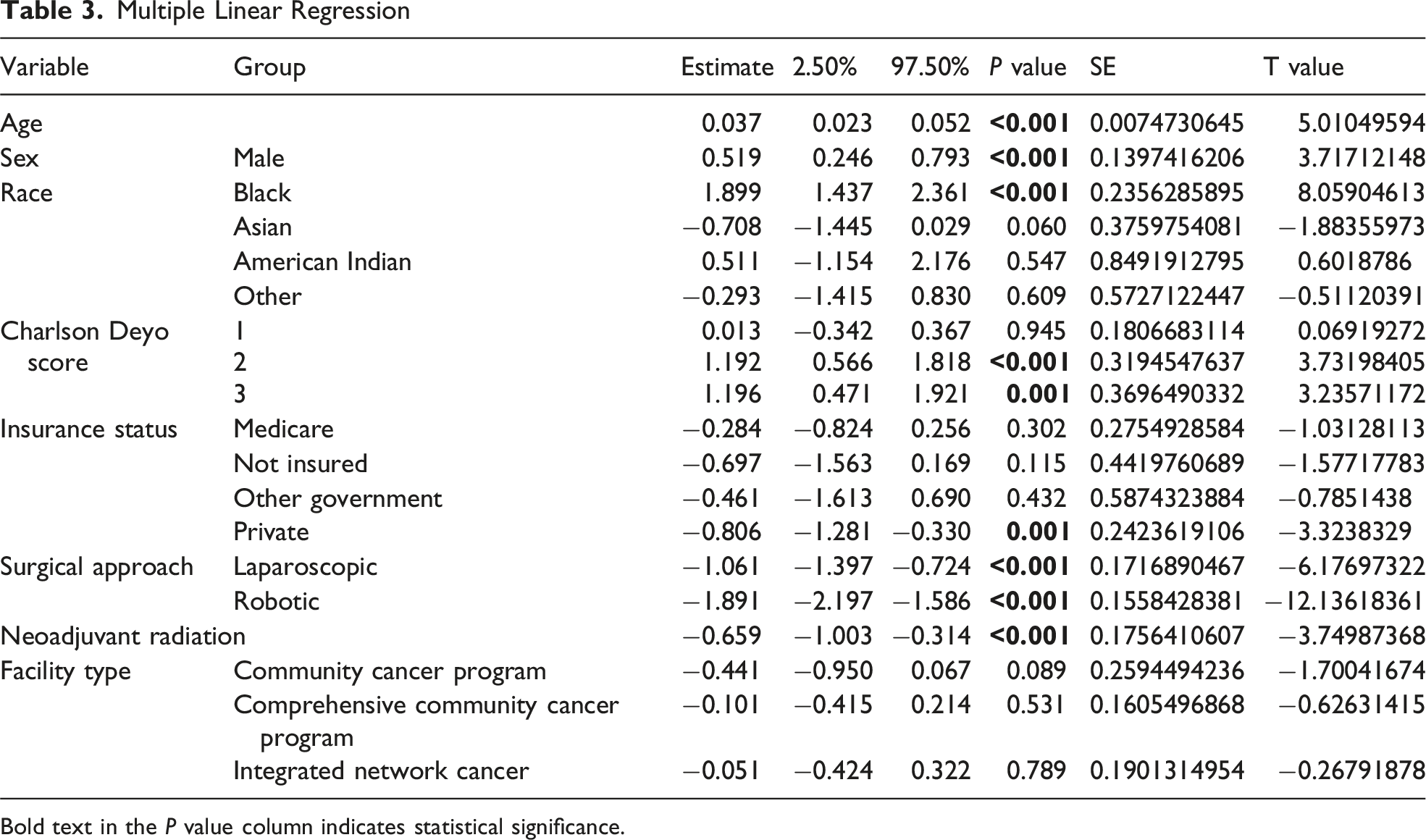
Bold text in the P value column indicates statistical significance.
Using a ROC curve analysis, 6 days was the cutoff for the number of days that signified worse overall survival. Patients with hospital stays ≥6 days had shorter overall survival (73 vs 75 months, P < .001) than patients with stays <6 days; however, any clinical significance of this difference is not clear.
Hospital Stay Calculator
The online calculator showed that a patient with several risk factors for a longer hospital stay (a 65-year-old Black male with a Charlson score of 3 and no insurance who underwent open surgery without neoadjuvant radiation therapy) had an extended hospital stay by 5.3 days, beyond the average stay of 6 days. Conversely, a 50-year-old White female with no comorbidities who had private insurance and underwent laparoscopic surgery had a shorter stay by 0.67 days. The R code of the online calculator is shown in Supplemental Figure 1.
Discussion
This study aimed to determine factors associated with hospital stay for patients undergoing APR for rectal cancer. We evaluated data from over 7000 patients during a 5-year period using the NCDB. Our data showed that older, Black, male patients with more comorbidities and Medicaid insurance had longer hospital stays. We developed a statistical calculator to estimate the length of hospital stay after APR based on patient characteristics.
Many factors that lengthen postoperative hospital stay are not modifiable. Our data showed that race and age both prolonged hospital stay. Older patients were found to stay in the hospital almost half a day longer than younger patients.
There is a void in the literature as to the length of hospital stay in elderly patients post-surgery. In the UK, patients >65 years of age undergoing emergency surgery were found to have a five-fold increase in hospital stay compared to patients treated conservatively and had higher readmission rates than their younger compatriots. 15 Elderly patients in South Africa were also found to have longer hospital stays after orthopedic surgery. 16 These findings will significantly impact those performing APRs, as the US population >65 will increase to 20% by 2030. 17 An estimated 19.5% of all persons having surgery in the US are >65 years of age. 18
Similarly, race was shown to impact hospital stay, with nearly 2 days and 1.4 days longer stay for Black and American Indian patients vs White patients, respectively. Interestingly, Black patients undergoing bariatric surgery and knee arthroplasty have a shorter length of hospital stay than other races.19,20 Alternatively, Black patients were found to have longer hospital stays than White patients undergoing surgery for malignant bowel obstructions. 21 Despite race and age being non-modifiable risk factors, targeting these patients with pre and postoperative interventions may effectively decrease their length of hospital stay.
Modifiable risk factors included neoadjuvant therapy use and operative approach. Concurrent with the literature, in our study, minimally invasive surgical approaches resulted in a short hospital length of stay. Laparoscopic surgery has been shown to shorten hospital stays and expedite the return of bowel function compared to open surgery. 22 Recent robotic surgical data have been similar. 23 These findings have been demonstrated in colorectal surgical patients with reduced pain, faster return of bowel function, and decreased complication rates.24-26
Secondly, neoadjuvant chemoradiation or total neoadjuvant therapy is common in rectal cancer treatment. At this point, there have been no significant differences in the perioperative complications of those treated in the neoadjuvant setting.4,27,28
Limitations
Our study has several limitations. First, large databases are prone to type 1 errors, showing significance despite minimal changes between the study groups. For that reason, we tried to focus on findings with significant clinical relevance. In addition, many patients were excluded from the database due to missing details, mainly clinical staging, which is key for determining survival outcome. The NCDB has no information regarding the previous surgical history of patients. Those with longer hospital stays and conversion to open surgery may have had a longer previous surgical history than those with shorter stays. Unfortunately, the NCDB does not capture data on postoperative complications, which limited our ability to evaluate complication-specific outcomes. While postoperative morbidities are known to extend hospitalization, length of stay may be seen as a broader health care utilization metric that reflects not only clinical recovery but also discharge criteria, resource availability, and socioeconomic determinants. Length of stay was previously used as a pragmatic surrogate reflecting the combined influence of surgical recovery, perioperative care, discharge logistics, and social determinants of health. Finally, registration issues are also common with database research, namely, hospital stay definitions may vary across different institutions (from admission to discharge vs from surgery to discharge).
Conclusions
Older age, Black race, male sex, and severe comorbidities were associated with longer hospital stays, while minimally invasive surgery was associated with decreased length of stay. These results may help inform perioperative planning; however, since the reason for a longer stay is likely multifaceted, further research is still needed. It is important to note that the study examined associations with prolonged hospitalization, and the findings should be interpreted as hypothesis-generating rather than practice-changing, given the retrospective nature of the data and study limitations.
Supplemental Material
Supplemental Material - Predictors of a Long Hospital Stay After Abdominoperineal Resection of Rectal Cancer: Analysis of the National Cancer Database
Supplemental Material for Predictors of a Long Hospital Stay After Abdominoperineal Resection of Rectal Cancer: Analysis of the National Cancer Database by Ashley G. Shustak, Marcus Oosenbrug, Nir Horesh, Sameh Hany Emile, Zoe Garoufalia, Rachel Gefen, Ebram Salama, and Steven D. Wexner in The American Surgeon
Footnotes
Author Contributions
Shustak: Conceptualization; Data Curation; Formal Analysis; Investigation; Methodology; Validation; Visualization; Writing – Original draft.
Oosenbrug: Data Curation; Formal Analysis; Writing – review and editing.
Horesh: Data Curation; Formal Analysis; Writing – review and editing.
Garoufalia: Data Curation; Formal Analysis; Writing – review and editing.
Gefen: Data Curation; Formal Analysis; Writing – review and editing.
Salama: Data Curation; Formal Analysis; Writing – review and editing.
Wexner: Conceptualization; Project Administration; Supervision; Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steven Wexner is a consultant for ActivSurgical, Arthrex, Baxter, Becton, Dickinson and Co., Evologics, Glaxo Smith Kline, Intuitive Surgical, New Med Tek Devices, Ostomy Secure, Polypid, Seikagaku, and Takeda, receives stock options for consulting from Polypid and Ostomy Secure, and receives royalties from Intuitive Surgical, Karl Storz Endoscopy America Inc., and Unique Surgical Solutions, LLC. Sameh Hany Emile is a consultant for Becton, Dickinson and Co. Ashley Shustak, Marcus Oosenbrug, Nir Horesh, Zoe Garoufalia, Rachel Gefen, and Ebram Salama do not report any conflicts of interest.
Data Availability Statement
Upon reasonable request from first author.
Presentations
This manuscript was presented as an E-Poster at the American Society of Colon and Rectal Surgeons annual meeting in June 1-4, 2024 in Baltimore, Maryland.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.