
Abstract
Background
Gastrointestinal metastases from primary lung malignancies occur in 0.2-11.9% of autopsy series; symptomatic colonic involvement is exceedingly rare (0.1%), portending a dismal prognosis with a reported median survival of approximately 2 months.
Case Presentation
A 60-year-old woman with a 40 pack-year smoking history, chronic obstructive pulmonary disease, and prior cervical malignancy presented with a refractory acute exacerbation. In the absence of a discrete pulmonary parenchymal lesion, computed tomography pulmonary angiography incidentally identified mass-like left upper lobe bronchial wall thickening. Bronchoscopic evaluation revealed high-grade endobronchial stenosis. Mediastinal fine-needle aspiration confirmed non-small cell lung carcinoma; colonic metastases identified on staging PET-CT demonstrated TTF-1/Napsin-A positivity with a CK7+/CK20−/CDX2− immunophenotype, consistent with pulmonary adenocarcinoma. Sequential adrenal resection revealed divergent squamous differentiation (p40+/CK5/6+; TTF-1−/Napsin-A−) with KRAS/MYC and NF-1 amplification, supporting a final diagnosis of pulmonary adenosquamous carcinoma—an aggressive NSCLC variant comprising 0.4-4% of lung malignancies.
Management and Outcome
Treatment followed evidence-based, histology-guided sequencing: concurrent carboplatin-pemetrexed chemoradiation, nivolumab upon platinum resistance, and cytotoxic salvage with docetaxel followed by vinorelbine. Palliative adrenalectomy addressed refractory pain. The patient survived 42 months from diagnosis, the clinical course was shaped by adequate tissue sampling, diagnostic challenges, and multidisciplinary histology-guided treatment acquisition.
Conclusion
This case underscores the diagnostic and therapeutic complexity of lung adenocarcinoma presenting with synchronous colonic metastases without a discrete parenchymal mass, compounded by intratumoral heterogeneity and phenotypic divergence across metastases. Comprehensive tissue sampling enabling serial immunohistochemical and molecular characterization, coupled with coordinated multidisciplinary management, is essential to optimize diagnostic accuracy and therapeutic sequencing in this rare and clinically challenging disease entity.
Keywords
Key Takeaways
• Broad differential is critical: Colonic lung metastases are often asymptomatic and atypical, requiring multimodal workup to include CTA, PET-CT, bronchoscopy, and sequential biopsies for definitive diagnosis. • Adequate tissue sampling is essential: Limited biopsies risk misclassification; full IHC and molecular profiling across multiple sites are necessary to capture intratumoral heterogeneity and guide therapy. • Treatment is adaptive but resistance is inevitable: Despite guideline-concordant sequencing across 35 rounds, disease progressed through each line, driven by clonal heterogeneity, microenvironmental factors, and PD-L1 discordance. • Multidisciplinary care shapes management: Integrated surgical, pathologic, and oncologic diagnostic interpretation allowed accurate classification and adaptive treatment management in a complex disease.
Introduction
Lung cancer is the second most common malignancy in the United States, comprising 18% of new cancer diagnoses and accounting for 20.4% of cancer-related mortality.1-4 The American Cancer Society projects 226 650 new cases and 124 730 deaths attributable to lung cancer in 2025. 5 Approximately half of all cases present with metastatic disease at diagnosis, 6 with preferential spread to the lymph nodes, liver, adrenal glands, bone, and brain. 6 Gastrointestinal (GI) tract involvement is an uncommon manifestation of advanced disease, identified in 0.2-11.9% of autopsy series.6,7 Symptomatic GI metastases are rare (0.2-0.5%), 6 predominantly involve the small bowel, and carry the lowest organ-specific survival of all metastatic sites (mean 1-15 months). 8 Colonic metastases are exceedingly rare (0.1%), portending a median survival of approximately 2 months. 3 We report a diagnostic challenging case of metastatic lung adenocarcinoma presenting as colonic metastasis in absence of a discrete pulmonary parenchymal lesion, with concurrent regional lymph node involvement, highlighting the need for a broad oncologic differential, adequate tissue acquisition and an integrated clinicopathologic interpretation for appropriate management. A clinical decision-making summary as informed by the literature is provided.
Case Report
A 60-year-old woman with asthma, chronic obstructive pulmonary disease (COPD), prior cervical malignancy, and a 40 pack-year smoking history presented with progressive dyspnea and productive purulent cough refractory to outpatient bronchodilators, systemic corticosteroids, and empiric antibiotics. Physical examination demonstrated tachypnea, tachycardia, accessory muscle use, and hypoxemia requiring 5L supplemental oxygen. Laboratory evaluation revealed thrombocytosis (492 × 103/μL), mild polycythemia (hematocrit 46%), corticosteroid-induced hyperglycemia (215 mg/dL), and leukocytosis (11.5 × 106/μL). B-type natriuretic peptide was within normal limits (25 pg/mL), excluding cardiogenic etiology. Initial chest radiography was unremarkable.
Given persistent tachypnea and tachycardia refractory to standard COPD exacerbation management, computed tomography pulmonary angiography (CTPA) was performed to exclude pulmonary embolism and unexpectedly demonstrated mass-like bronchial wall thickening of the left upper lobe. Bronchoscopy revealed 80% stenosis of the left lingular segmental bronchus, complete left upper lobe segmental bronchial occlusion, and diffuse mucosal inflammation, findings atypical for obstructive airway disease and necessitating tissue diagnosis.
Fine-needle aspiration (FNA) of mediastinal station 7 confirmed non-small cell lung carcinoma (NSCLC); station 4L demonstrated high-grade pleomorphic epithelial cells consistent with adenocarcinoma. Immunohistochemistry (IHC) was negative for EGFR, PD-L1, ALK, and ROS-1; TTF-1 was not performed due to insufficient sample. Staging PET-CT (Figure 1A-C) identified hypermetabolic foci in the left hilum and aortopulmonary window with additional colonic lesions; initial colonoscopy demonstrated only benign tubular adenomas. Brain MRI was negative. FDG-18 PET-CT imaging. (A) Coronal images demonstrating hypermetabolic lesion in the left hilum (white arrow) of the lung. (B) Left hilum lesion in the axial plane (white arrow). (C) Coronal imaging with the hypermetabolic tumor in the descending colon (white arrow)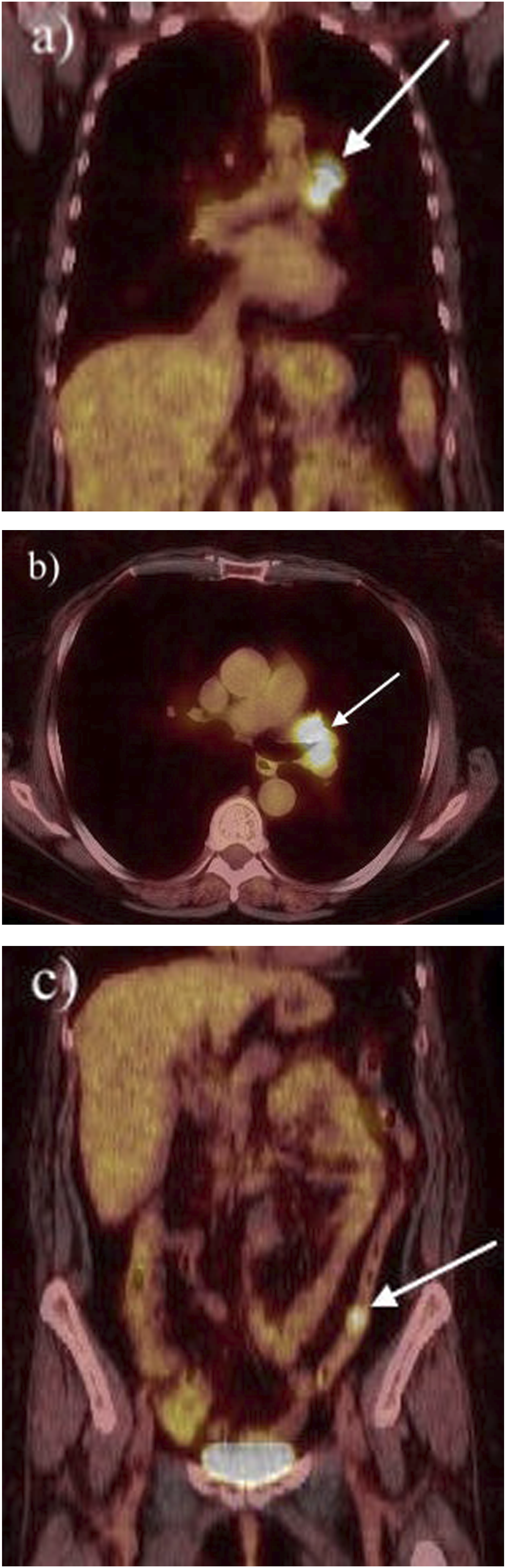
First-line therapy consisted of concurrent carboplatin-pemetrexed (four cycles) with 6000 cGy in 30 fractions, selected based on non-squamous histology and evidence of survival benefit with pemetrexed-platinum combination therapy (HR = 0.87, 95% CI: 0.77-0.98).
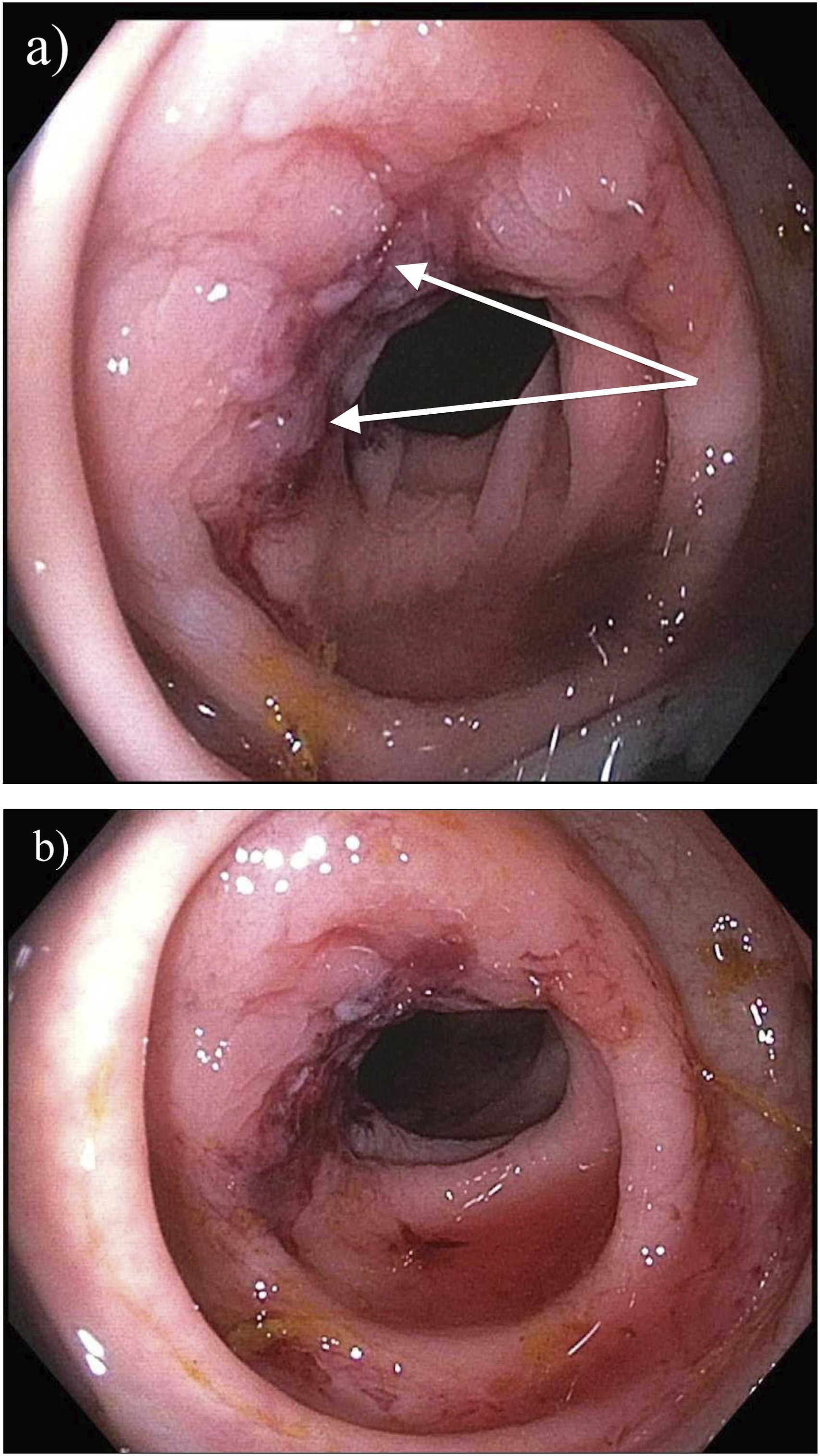
Eleven-month surveillance PET-CT (Figure 2A-D) demonstrated stable primary disease with new hypermetabolic foci in the right adrenal gland and sigmoid colon. CT-guided adrenal FNA identified malignant cells with pleomorphism, dense chromatin, and inconspicuous nucleoli; insufficient tissue precluded IHC characterization. Repeat colonoscopy identified an ulcerated sigmoid lesion (Figure 3); biopsy confirmed moderately differentiated adenocarcinoma with a TTF-1+/Napsin-A+/PD-L1+/CDX2−/CK20−/EGFR−/ALK−/ROS-1− immunophenotype, consistent with metastatic pulmonary adenocarcinoma. Notably, PD-L1 positivity at the colonic metastatic site was discordant with the PD-L1-negative mediastinal nodal profile, reflecting site-specific heterogeneity in the tumor immune microenvironment. FDG-18 PET-CT imaging 11-months post-diagnosis demonstrating hypermetabolic tumor of the right adrenal metastatic lesion (white arrows) in axial (A) and coronal planes (B) FDG-18 PET-CT imaging in the axial plane axial (C) and coronal (D) demonstrates tumor avidity at the junction of the rectosigmoid colon and descending colon (white arrow) Diagnostic colonoscopy. (A and B) An ulcerated, firm lesion of the sigmoid colon was noted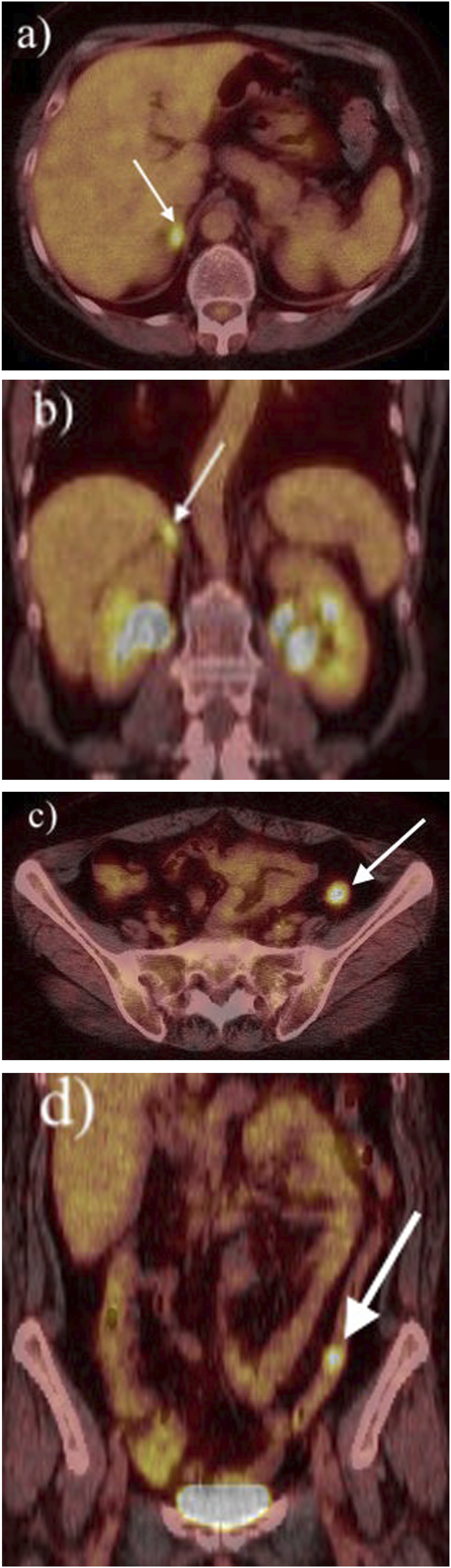
Given platinum resistance and newly identified PD-L1 positivity, second-line nivolumab 240 mg was initiated and administered for ten cycles with good tolerability, yielding stable disease on 3-month surveillance imaging. At 23 months, right adrenal progression necessitated transition to docetaxel, which was discontinued after three cycles due to intolerance. Vinorelbine was subsequently administered for 35 cycles, selected for its dual activity against adenocarcinoma and squamous cell histologies and favorable toxicity profile, and was well-tolerated.
Despite ongoing systemic therapy, new hepatic metastases and progressive adrenal enlargement (43 × 36 mm) developed. Right adrenalectomy was performed for management of intractable flank pain. IHC analysis of the resected adrenal specimen demonstrated TTF-1−/Napsin-A− malignant cells with diffuse p40 and CK5/6 positivity, indicating squamous differentiation. Adrenal cortical carcinoma was excluded by negative Melan-A, chromogranin, calretinin, and synaptophysin staining. Molecular profiling identified KRAS/MYC and NF-1 amplification without actionable driver mutations (EGFR−/PD-L1−/ALK−/ROS-1−). The composite histologic and metastatic pattern was consistent with pulmonary adenosquamous carcinoma (ASC), a rare but biologically aggressive NSCLC variant comprising 0.4-4% of lung malignancies. Palliative nab-paclitaxel was initiated; however, at 41 months post-diagnosis the patient transitioned to hospice care and died at 42 months post initial diagnosis.
Discussion
Colonic metastases from primary lung malignancies represent an exceedingly rare and diagnostically challenging entity.6,7,9 A comprehensive literature review identified 32 published case reports of GI metastases from primary lung cancer, 21 of which (65.63%) involved the colon (Supplemental Table 1). Nine review articles addressed GI metastases from lung cancer, of which seven reported colonic involvement.
High-Risk Patients Require a Broad Oncologic Differential
Published series demonstrate a predilection for middle-aged patients (approximately 60 years), male predominance in isolated colonic disease (38%), and a high prevalence of smoking history (42.86% in colon-only cohorts; Supplemental Tables 1 and 2). Consistent with the established literature, colonic metastases in the index case were entirely asymptomatic at presentation6,7,9; the diagnosis was established incidentally during workup for a presumed COPD exacerbation. When symptomatic, colonic metastases produce nonspecific manifestations, such as abdominal pain, nausea, and weight loss, which are readily attributed to alternative diagnoses or treatment-related toxicity, as occurred here.7,9,10,11 This case reinforces the imperative of maintaining a broad oncologic differential in high-risk populations, particularly those with significant smoking histories, even when the presenting syndrome appears attributable to common cardiopulmonary pathology.
Nonspecific Imaging Findings Must Prompt Tissue-Based Diagnosis
Initial chest radiography was unremarkable, underscoring its limited sensitivity in detecting endobronchial or perihilar malignancy. CTPA, performed to exclude pulmonary embolism in the setting of treatment-refractory tachypnea and tachycardia, incidentally, identified mass-like bronchial wall thickening, an atypical finding for COPD, that prompted further evaluation. Endobronchial lesions may appear nodular, ulcerated, or infiltrative on bronchoscopy 12 ; however, gross morphology does not reliably discriminate between metastatic disease, primary bronchogenic carcinoma, carcinoid tumor, or benign inflammatory processes.12,13 The identification of high-grade focal stenosis and complete segmental occlusion, incongruous with obstructive airway disease, necessitated tissue sampling. Staging PET-CT identified hypermetabolic activity in the left hilum, aortopulmonary window, and colon in the absence of a discrete parenchymal mass, an uncommonly encountered presentation that substantially increased diagnostic complexity. Colonoscopic visualization alone has limited specificity, as colonic metastases may mimic primary adenocarcinoma, inflammatory lesions, or polypoid neoplasms14,15,16; definitive characterization requires histopathologic confirmation with IHC and integrated clinico-radiographic correlation. 17
Adequate Tissue Procurement is Essential for Histopathologic and Molecular Evaluation
Adenocarcinoma is the predominant NSCLC histology identified in GI metastases (56.25% colonic; 61.90% other GI sites). 7 The TTF-1+/Napsin-A+/CK7+/CK20−/CDX2− immunophenotype established pulmonary origin of the colonic metastasis, consistent with published diagnostic criteria.7,9,17 TTF-1 nuclear positivity is observed in 60-75% of lung adenocarcinomas and is the most reliable IHC marker for distinguishing pulmonary from gastrointestinal primary.2,11 Discordant PD-L1 expression between the lymph node and colonic biopsy specimens reflects established site-specific variability in the NSCLC tumor immune microenvironment, with significantly higher PD-L1 expression reported in adrenal, hepatic, and nodal metastases compared to bone and brain (P = .004).18,19
The adrenal resection specimen revealed a divergent squamous immunophenotype (p40+/CK5/6+; TTF-1−/Napsin-A−), with KRAS/MYC and NF-1 amplification on molecular profiling. This phenotypic shift is consistent with pulmonary ASC, defined by WHO criteria as requiring at least 10% each of adenocarcinoma and squamous cell carcinoma components, with a high degree of intratumoral heterogeneity. 20 ASC accounts for 0.4-4% of lung malignancies, carries a significantly worse prognosis than pure squamous cell carcinoma (adjusted HR 5.57, P = .002), and demonstrates a propensity for adrenal metastasis.7,20 The initial diagnosis of adenocarcinoma likely reflected histologic sampling bias on limited FNA material, 21 highlighting a critical limitation of small-specimen analysis. Molecular profiling of the adrenal resection specimen, while informative, was obtained in the palliative setting and therefore could not inform earlier therapeutic decision-making. These findings underscore the essential role of adequate tissue acquisition enabling a larger panel of IHC characterization and comprehensive molecular profiling for accurate histologic classification and identification of actionable therapeutic targets.21,22
Management Requires Adaptive, Histology-Guided Treatment
Management followed evidence-based, histology-guided sequencing throughout the disease course. First-line carboplatin-pemetrexed with concurrent thoracic radiation was appropriate for non-squamous NSCLC without actionable driver mutations.7,17 Second-line nivolumab was guideline-concordant upon platinum resistance, with established survival benefit in advanced NSCLC independent of PD-L1 expression status. 17 Subsequent cytotoxic salvage with docetaxel, then vinorelbine, represented accepted later-line options in heavily pretreated patients.7,17 Palliative adrenalectomy for refractory pain is an appropriate symptom-directed intervention; surgical resection of GI metastases is reserved for complications including obstruction, hemorrhage, or perforation and does not confer survival benefit.3,17 Therapeutic resistance, observed across multiple lines of therapy, reflects the convergent effects of intratumoral heterogeneity, pre-existing resistant subclones, microenvironmental remodeling, and epigenetic reprogramming, mechanisms well-characterized in advanced NSCLC.23-26 Response rates to first-line platinum-based chemotherapy approximate 30-40%, with near-universal eventual resistance. 25
The patient survived 42 months from initial diagnosis due to an appropriate evolving strategy, repeated tissue acquisition, and multidisciplinary management directed disease classification and treatment options in the setting of marked intratumoral heterogeneity.
Conclusion
This case illustrates the diagnostic and therapeutic complexity inherent to lung adenocarcinoma presenting with synchronous colonic metastases in the absence of a discrete pulmonary parenchymal lesion, compounded by intratumoral phenotypic divergence and progressive therapeutic resistance across multiple lines of systemic therapy. Multimodal imaging, bronchoscopic evaluation, and serial tissue sampling with comprehensive IHC and molecular characterization were essential to achieving definitive diagnosis and guiding histology-concordant therapy (Figure 4). Heightened clinical vigilance, a broad oncologic differential in high-risk populations, and commitment to adequate tissue acquisition for thorough molecular profiling remain paramount to optimizing outcomes in this rare and diagnostically challenging disease entity. Flow chart outlining the disease course, histopathologic data, and treatments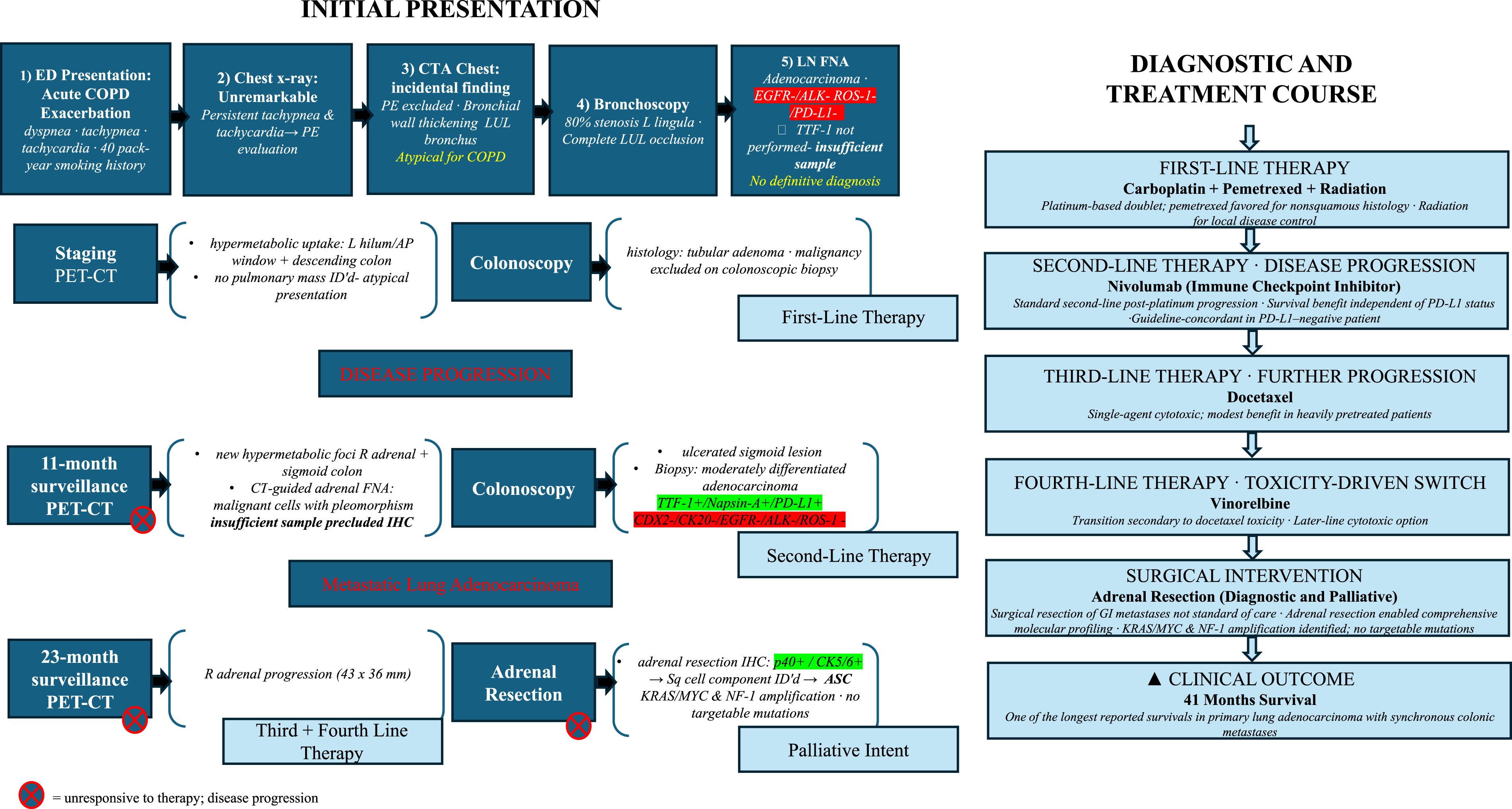
Supplemental Material
Supplemental material - Occult Pulmonary Adenosquamous Carcinoma Presenting With Synchronous Colonic Metastases
Supplemental material for Occult Pulmonary Adenosquamous Carcinoma Presenting With Synchronous Colonic Metastases by Mary Hunter Hyche, Isabella Lopez, Christine Marie-Gilligan Schammel, A. Michael Devane, David P Schammel, and Yulia Y Yurko in The American Surgeon™
Footnotes
Ethical Considerations
This work was approved by the Prisma Health IRB [Pro2404794-1] as not research; publication consent was obtained from the patient/representative.
Author Contributions
MHH—Data Curation, Validation, and Writing (Original Draft/Review); IL—Data Curation and Writing (Original Draft/Review); CMGS—Conceptualization, Writing (Original Draft/Review), Supervision, and Project Administration; AMD—Data Curation, Validation, and Writing (Original Draft/Review); DPS—Data Curation, Validation, and Writing (Original Draft/Review); YYY—Conceptualization, Data Curation, Validation, and Writing (Original Draft/Review).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not publicly available but is available from the corresponding author with a reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.