
Abstract
Background
Delayed diagnosis of hollow viscus injury (HVI) after blunt abdominal trauma is life-threatening and may be missed on initial CT imaging. Unexplained free fluid can signal HVI, yet the optimal diagnostic approach, particularly the role of repeat imaging with oral (PO) contrast, remains controversial. This study evaluates whether repeat CT with PO improves detection of missed HVI.
Methods
A single-center retrospective cohort study was performed at a level I trauma center (2017-2023) examining patients who presented with blunt abdominal trauma and free fluid on initial CT. Cohorts were grouped based on imaging modality: IV contrast only (CT IV) and IV plus PO contrast (CT IV + PO). The primary outcome was identification of new or previously missed findings prompting management changes. Secondary outcomes included postoperative complications and mortality.
Results
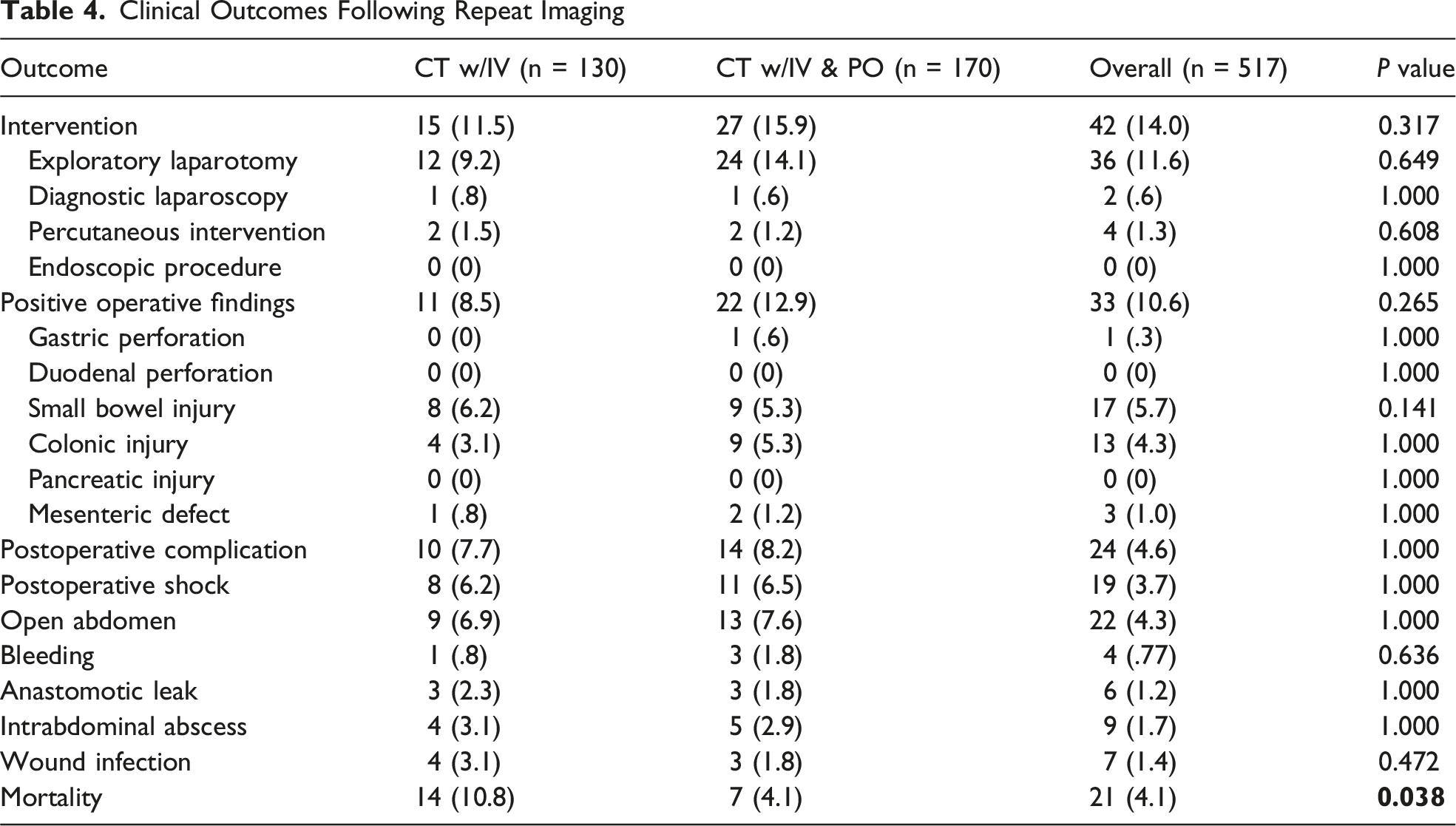
300 patients met inclusion criteria (130 CT IV; 170 CT IV + PO). New findings appeared in 34.3% overall, with no significant difference between groups (38.5% vs 31.4%, P = 0.20). Rates of operative intervention (11.5% vs 15.9%, P = 0.32), positive operative findings (8.5% vs 12.9%, P = 0.27), and postoperative complications (7.7% vs 8.2%, P = 1.00) were similar. Unadjusted mortality was higher in patients who underwent CT IV (10.8% vs 4.1%, P = 0.038); however, no difference was observed after adjusting for Injury Severity Score (P = 0.59). Delayed time to intervention strongly correlated with complications and mortality.
Discussion
Repeat CT can assist in detecting missed HVI, but adding PO contrast does not improve diagnostic yield, alter management, or affect outcomes.
Key Take Away
• Repeat CT is valuable for identifying HVI and should be considered when clinical suspicion persists. • Oral contrast does not enhance repeat CT imaging in comparison to repeat CT with IV contrast and does not offer improvement in diagnostic yield, management, or complication rates. • Timely surgical intervention is the critical determinant of outcomes underscoring the need for rapid decision-making and avoidance of unnecessary delays that are associated with PO contrast.
Background
Hollow viscus injury (HVI) is a potentially life-threatening complication of blunt abdominal trauma, involving the stomach, small intestine, colon, and mesentery. Early diagnosis is challenging since patients often present with nonspecific symptoms and subtle physical exam findings. When missed or delayed, HVI carries markedly increased morbidity and mortality, including higher rates of peritonitis, sepsis, prolonged intensive care unit (ICU) stays, multiple organ dysfunction, and death.1,2
Computed tomography (CT) with intravenous (IV) contrast is the standard imaging modality for hemodynamically stable trauma patients, offering high sensitivity for solid organ injury but only moderate sensitivity for HVI.3,4 Unexplained free intraperitoneal fluid on initial CT is often the only early radiographic indicator of HVI and typically prompts further evaluation. Strategies to improve diagnostic accuracy include serial clinical examinations, repeat CT imaging, diagnostic peritoneal lavage, and early operative exploration.5,6
Some centers have incorporated the use of oral (PO) contrast during repeat CT imaging to aid in the delineation of bowel loops in order to better visualize injuries, particularly extraluminal extravasation. However, the diagnostic yield has been found to be limited, with extravasation of contrast only occurring in 3-4% of bowel perforation. In fact, oral contrast is not routinely used in the acute trauma setting since it has been found to rarely alter management while leading to delay in diagnosis and operative management, while carrying.7,8 Furthermore, oral contrast administration may delay diagnosis, prolong time to operative management, and increased aspiration risk.7-11 Although the use of PO contrast in initial CT imaging has been well studied and found to lead to negative outcomes, the clinical value of oral contrast in repeat CT imaging for suspected HVI remains uncertain. Repeat CT imaging using IV and PO contrast has become widely utilized at our institution as well as in other trauma centers for patients who present with unexplained free fluid on initial trauma imaging.12,13 This study aims to evaluate the utility of repeating imaging using oral contrast in detecting missed HVI and guiding timely intervention.
Methods
This was a single-center retrospective cohort study conducted at a Level I trauma center between 2017 and 2023. After IRB approval was obtained, the institutional trauma registry and electronic medical record were queried to identify eligible patients. Inclusion criteria included patients greater than 18 years of age, who sustained blunt abdominal trauma, underwent CT of abdomen and pelvis with IV contrast as part of their trauma injury workup, and demonstrated unexplained free fluid. Unexplained free fluid was defined as intraperitoneal fluid in the absence of solid organ injury that had a density measurement less than 30 Hounsfield units. Only patients managed nonoperatively at presentation who underwent at least one repeat CT during hospitalization were eligible. Patients were excluded if they were younger than 18 years, sustained penetrating trauma, required operative intervention prior to repeat CT, or lacked follow-up imaging with IV or IV plus oral (PO) contrast. Patients were categorized into 2 groups based on the modality of repeat imaging: those who underwent CT with IV (CT IV) contrast alone and those who underwent CT with IV and PO (CT IV + PO) contrast (Figure 1). Study cohort selection for patients presenting with blunt abdominal trauma and free fluid. Among 1713 adults with isolated blunt abdominal trauma, 418 presented with free fluid on initial CT. Of these, 300 underwent repeat CT imaging and comprised the final cohort. Patients were grouped by repeat CT modality: IV contrast only (n = 130) and IV plus PO contrast (n = 170)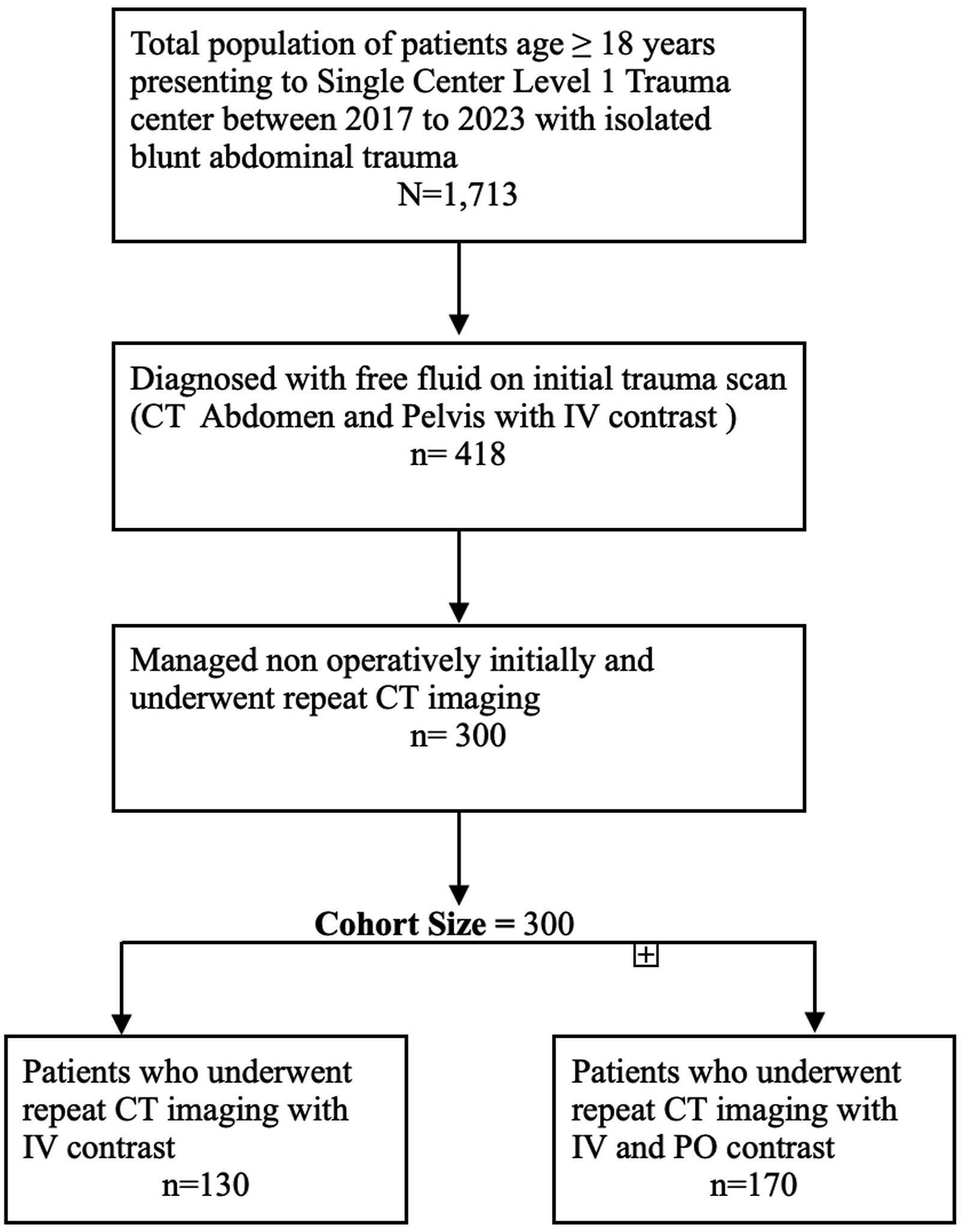
The primary outcome was the detection of new or previously missed findings on repeat imaging and subsequent management changes, including operative intervention, interventional radiology procedures, or endoscopic intervention. Secondary outcomes included postoperative complications such as shock, open abdomen, bleeding, anastomotic leak, intra-abdominal abscess, Surgical Site Infection (SSI), intensive care unit length of stay (ICU LOS), hospital length of stay (HLOS), and in-hospital mortality (IHM).
Demographic information, mechanism of injury (MOI), vital signs on presentation, Glasgow Coma Scale score (GCS), Injury Severity Score (ISS), laboratory values, transfusion requirements, and ICU admission were abstracted from the trauma registry and verified by electronic medical record review. Radiographic variables, including hemoperitoneum, bowel wall thickening, mesenteric stranding, pneumoperitoneum, and contrast extravasation, as well as operative findings, were collected from formal radiology and operative reports. Data abstraction followed a standardized codebook, and 10% of records underwent dual review for accuracy, with discrepancies resolved by consensus.
Continuous variables were tested for normality using the test of skewness. For data points that tested to have a minimal amounts of skew (−1 and 1), these data elements were compared between study groups using Student’s t-tests. For those data elements that were tested to show a significant amount of skew, the Mann-Whitney U tests were used. T-tests were expressed as means with standard deviations and Mann-Whitney U test data was reported as medians with interquartile ranges. Categorical variables were compared using chi-square or Fisher’s exact tests. Logistic regression was used to evaluate the association between imaging modality and outcomes, with adjustment for ISS. A two-sided P-value of <0.05 was considered statistically significant. All analyses were performed using SPSS Statistics version 27 (IBM Corp., Armonk, NY).
Results
Patient Demographics and Injury Severity
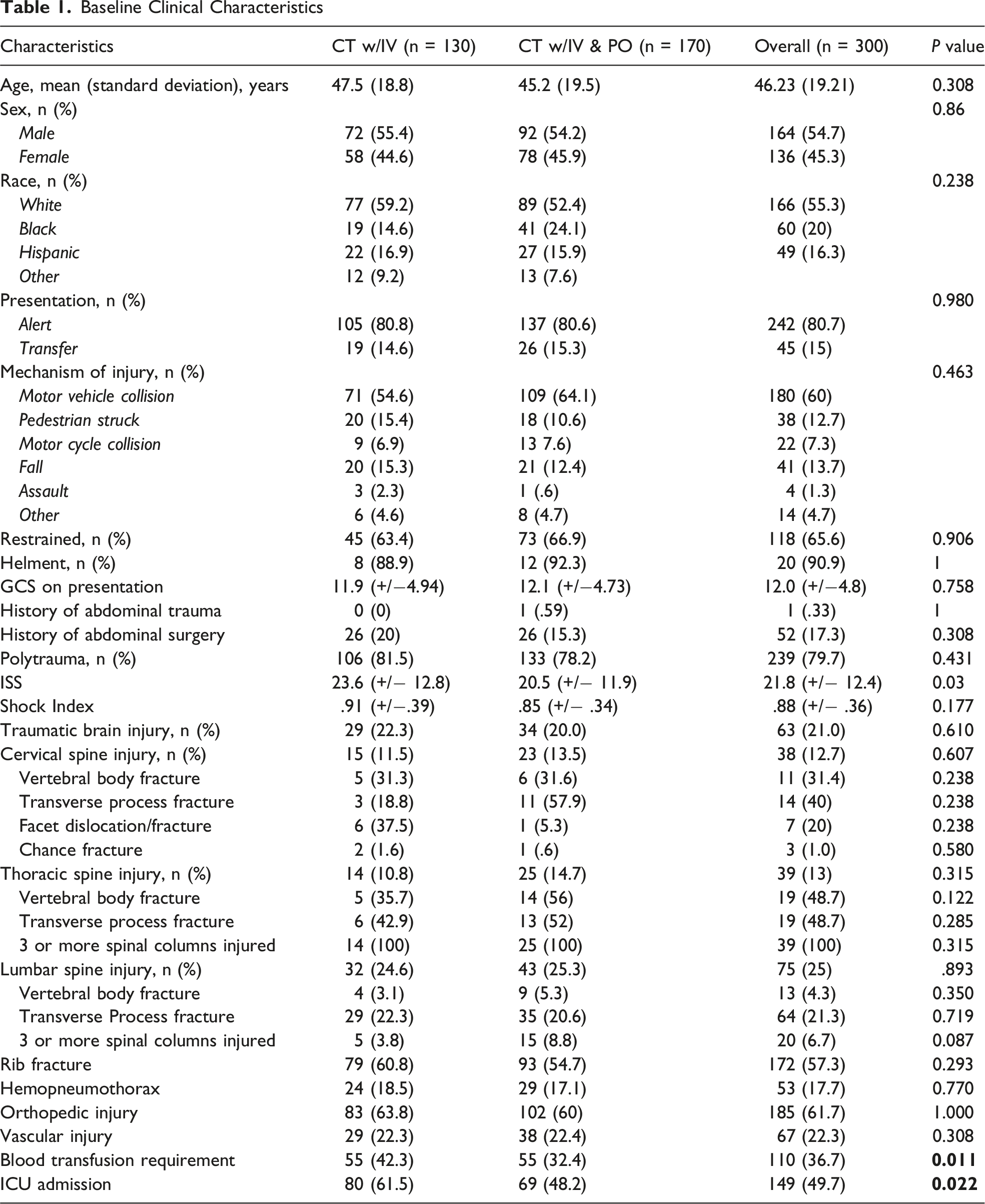
Baseline Clinical Characteristics
Findings on Repeat Imaging
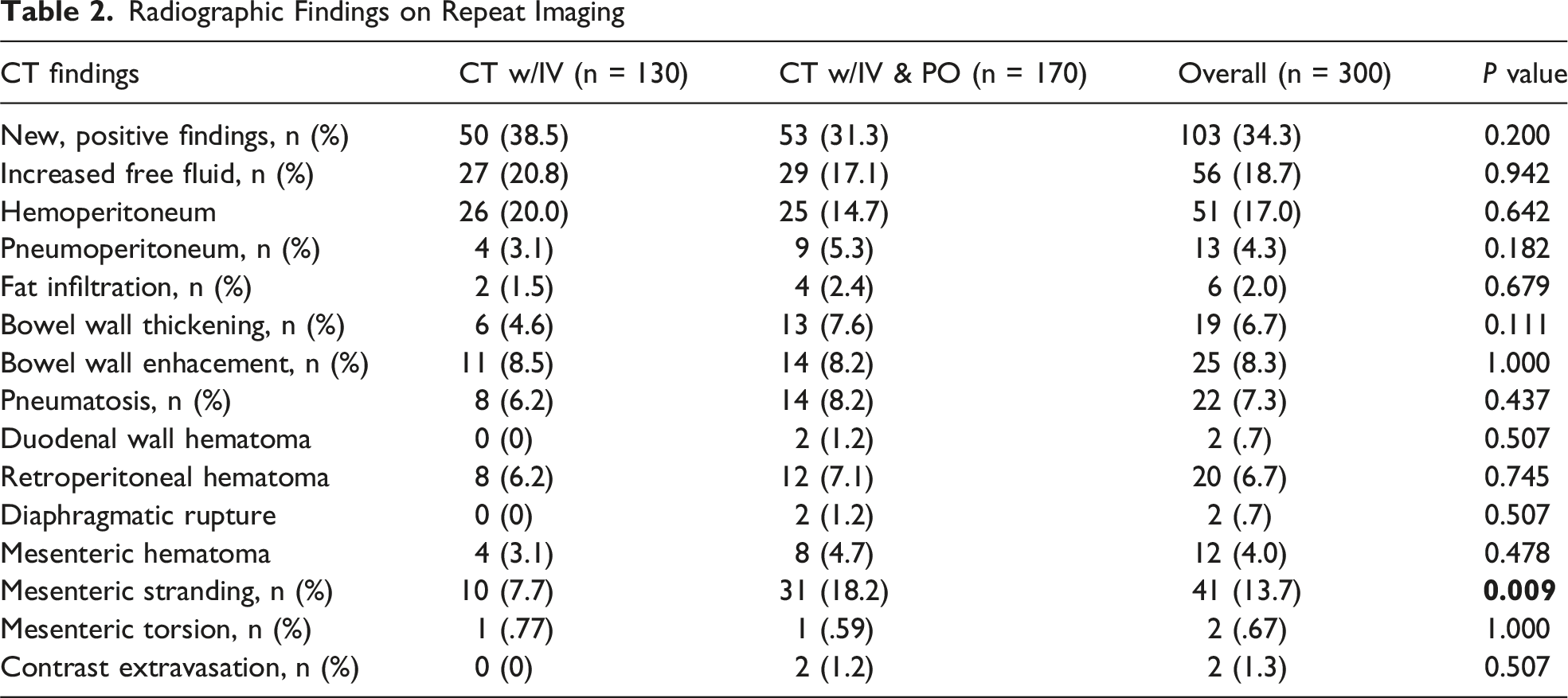
Radiographic Findings on Repeat Imaging
Adjusted Odds Ratios of Radiographic Findings on Follow-up Imaging
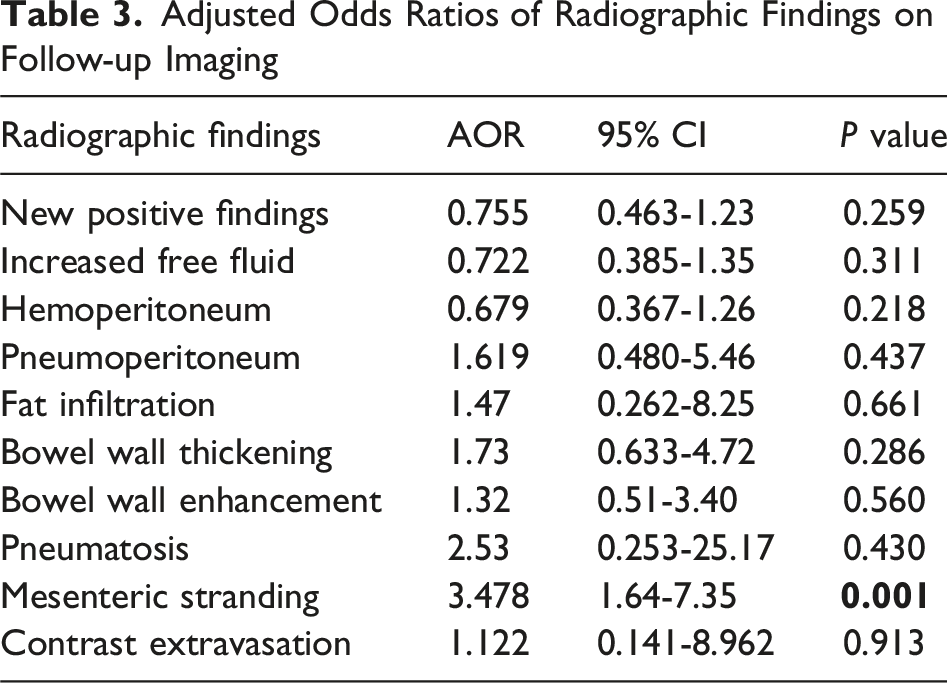
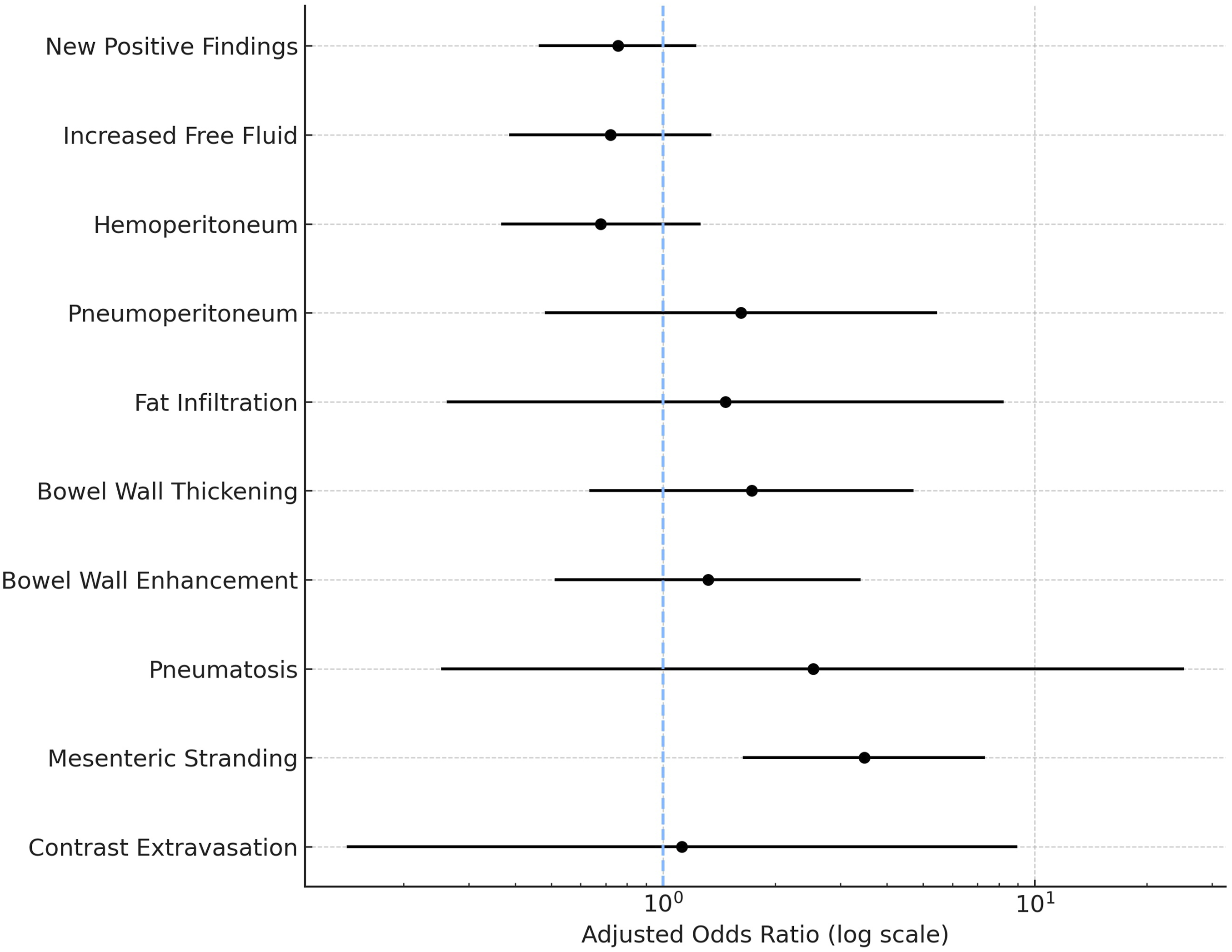
Adjusted odds ratios for radiographic findings on repeat CT imaging. Forest plot displaying adjusted odds ratios (AORs) with 95% confidence intervals for key clinical outcomes in patients undergoing repeat CT imaging with IV contrast alone vs IV plus oral (PO) contrast. Odds ratios are plotted on a logarithmic scale, with the dashed vertical line representing an AOR of 1.0 (no difference between groups). No outcome demonstrated a statistically significant difference between imaging modalities
Operative and Clinical Outcomes
Clinical Outcomes Following Repeat Imaging
Adjusted Outcomes Following Repeat Imaging
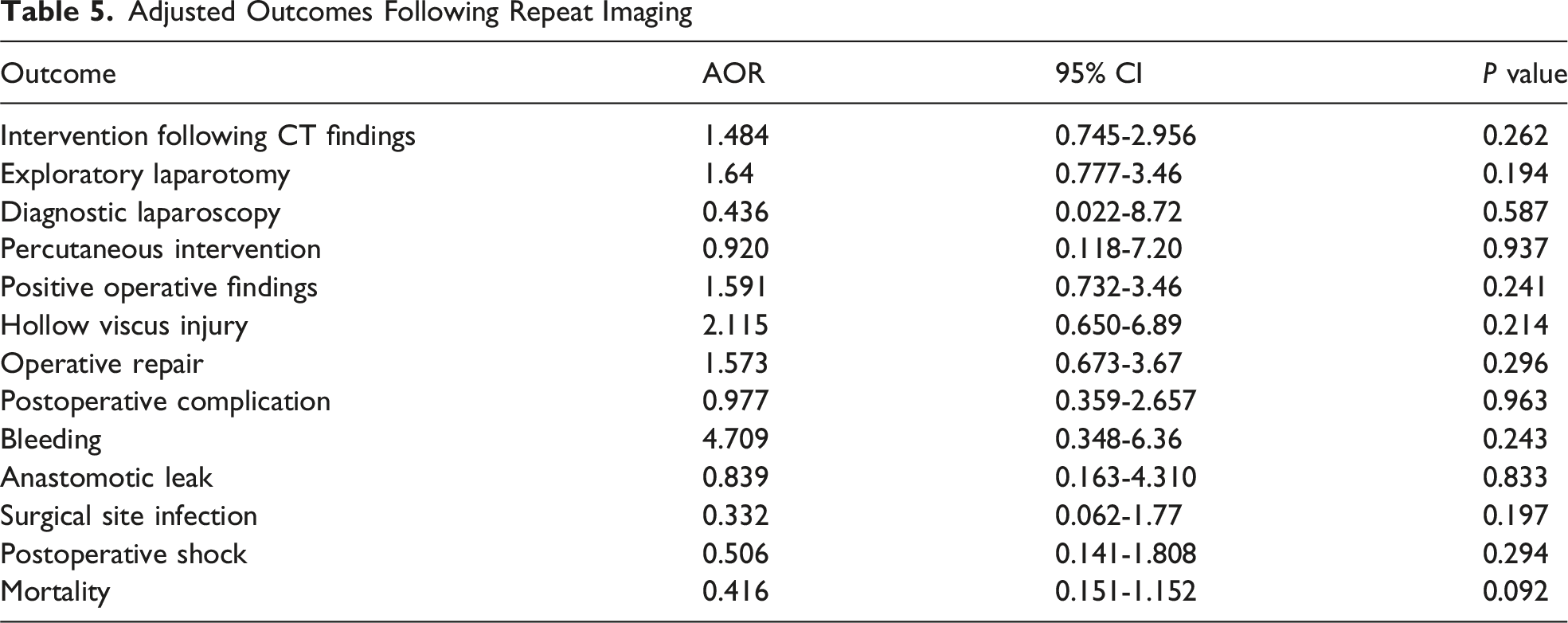
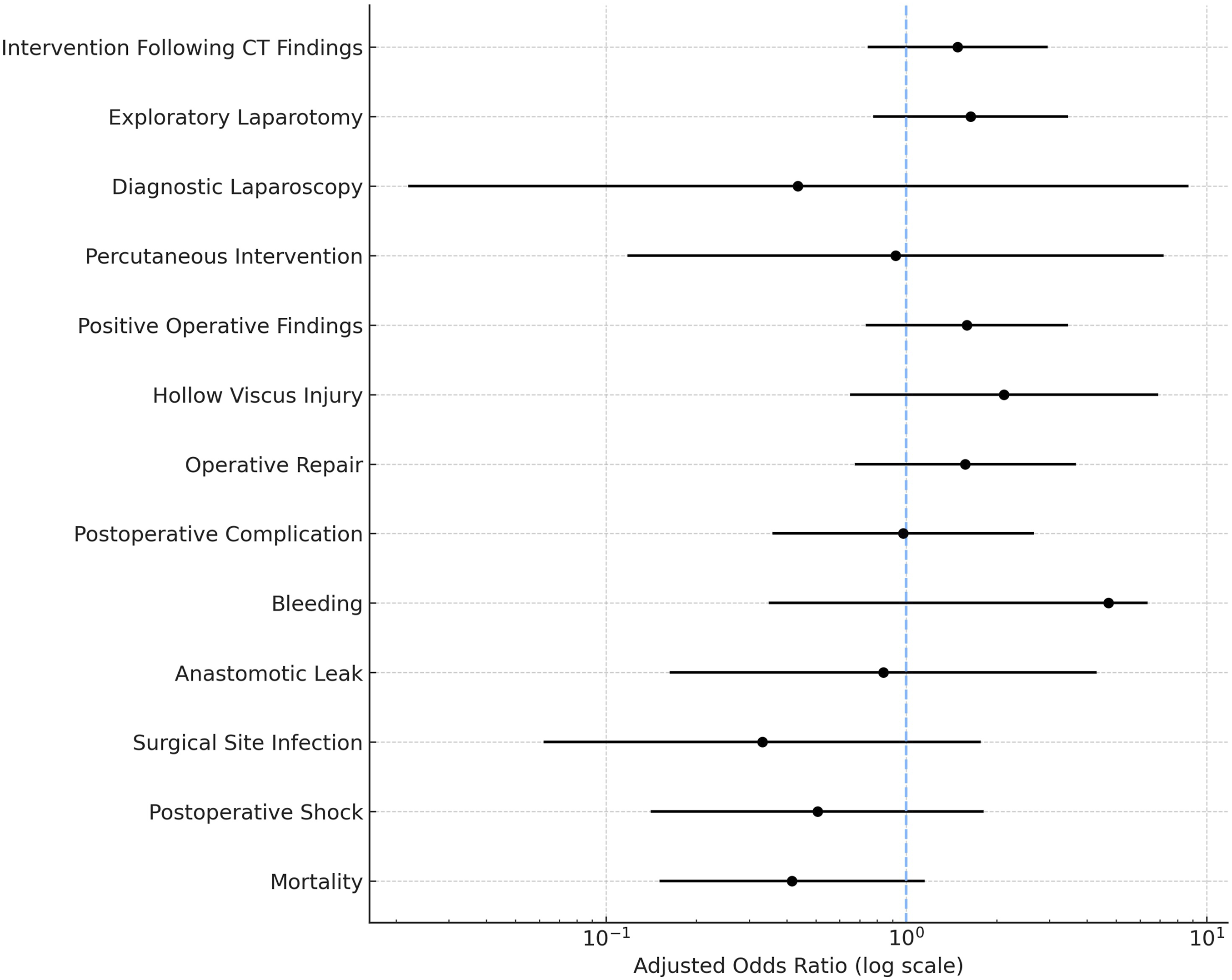
Adjusted outcomes in patients who underwent repeat imaging with CT IV vs CT IV + PO Forest plot displaying adjusted odds ratios (AORs) and 95% confidence intervals for clinical outcomes after repeat CT imaging. Odds ratios are plotted on a logarithmic scale, with the dashed vertical line representing an AOR of 1.0 (no difference between groups). None of the evaluated outcomes demonstrated statistically significant differences after adjustment
Impact of Time to Intervention on Outcomes
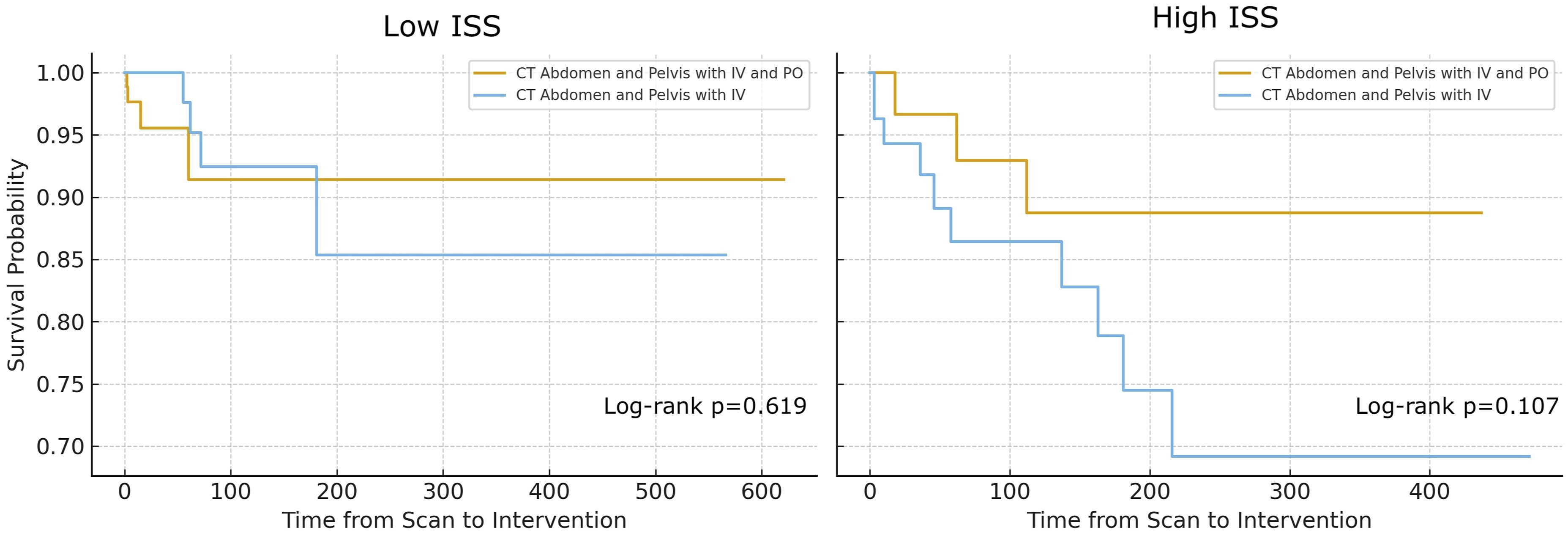
Regardless of imaging modality, time from initial trauma scan to operative intervention was found to be associated with higher rates of postoperative complications and higher mortality. Patients with postoperative complications had higher median intervention time (66 h [IQR 44-186] vs 16 h [IQR 5-45], P < 0.001. Time to intervention was almost doubled in patients with a higher mortality (66 h [IQR 38.5-167] vs 39 h [IQR 10-148)] P < 0.001) (Figure 4). Kaplan-Meier survival curves stratified by ISS further illustrate the influence of both injury severity and imaging modality. Among patients with low and high ISS, survival did not differ between CT with IV and CT with IV + PO (log-rank P = 0.619, P = 0.107) (Figure 5). Relationship between intervention timing, (A) postoperative complications and (B) mortality. (A) Time from scan to intervention in patients with postoperative complications vs without postoperative complications. Patients who developed complications had substantially longer delays to operative management. (B) Time to intervention in patients who had mortality event vs no mortality. Mortality was associated with markedly prolonged time to intervention and greater variability in intervention time Kaplan-Meier survival curves stratified by injury severity score (ISS) comparing repeat CT IV vs CT IV + PO. Kaplan-Meier survival estimates showing time from CT scan to intervention among patients stratified into low ISS (left) and high ISS (right) groups. Survival probabilities were compared between patients who underwent repeat CT IV (blue) vs CT IV + PO (gold). Log-rank testing demonstrated no statistically significant difference in survival for either cohort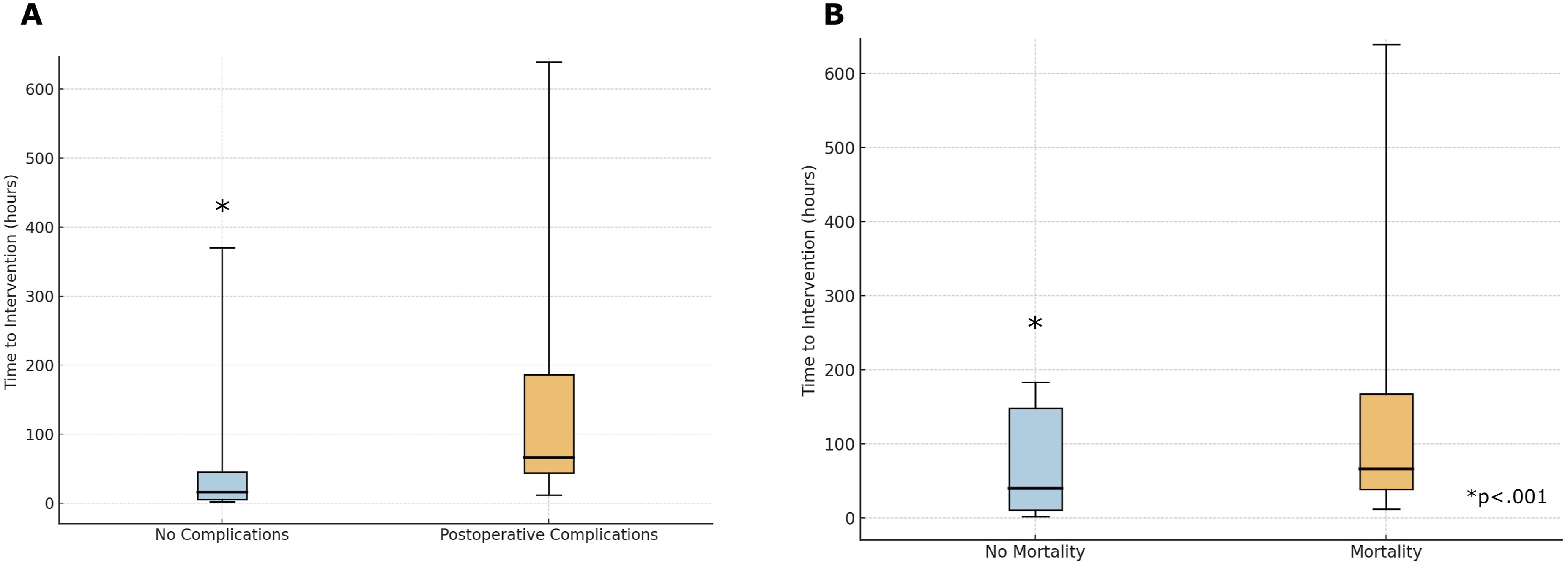
Discussion
Hollow viscus injury (HVI) is a complication of blunt abdominal trauma and while difficult to always diagnose radiographically or through physical exam, carries life-threatening risk if not diagnosed.1,2 Despite progressive advances in multidetector CT technology, including thin-slice acquisition (≤1-2 mm), multi-planar reconstruction, and higher temporal resolution, early identification of HVI is difficult. While CT is highly sensitive for solid organ injury (>95%), its sensitivity for HVI is only 50-70% sensitive and 80-95% specific for HVI detection. 14 The most frequent early indicator of possible HVI is unexplained free intraperitoneal fluid, particularly in the absence of solid organ injury. This finding occurs in roughly 20-30% of trauma CT scans and often prompts further evaluation through serial examinations, repeat imaging, or operative exploration.2,5,6 The optimal approach to these indeterminate cases remains uncertain, and imaging protocols vary widely across centers.
The role of oral contrast in improving diagnostic yield has been debated for decades. Although theoretically helpful in delineating small bowel loops or detecting extravasation, oral contrast has limited practical utility, as extravasation is reported in only 3-4% of bowel injuries.7,8 Moreover, several studies have demonstrated that oral contrast delays diagnosis without improving detection of HVI, and its use has largely fallen out of favor in initial trauma imaging.7-10 International surveys and meta-analyses have confirmed that most trauma centers omit enteric contrast from their routine protocols11,14,15,. Nonetheless, the role of oral contrast in repeat CT imaging after initial scan shows unexplained free fluid in the absence of solid organ injury has not been well studied.
Our study is the first, to our knowledge, to evaluate the diagnostic and clinical impact of oral contrast in repeat CT imaging after free fluid is identified on initial trauma scan. We found that repeat CT identified new findings in approximately 34% of patients, resulting in operative intervention in 14%. However, repeat imaging with CT IV + PO did not improve detection of missed bowel injuries compared to CT IV (AOR .755, 95% CI .463-1.23, P = 0.259).
On adjusted analysis, CT IV + PO was only associated with improved detection of mesenteric stranding (AOR 3.48, 95% CI 1.64-7.35, P = 0.001), whereas rates of bowel wall thickening, enhancement, pneumoperitoneum, and hemoperitoneum were similar between modalities. These results reinforce that enteric contrast provides minimal incremental diagnostic value.
From a radiologic standpoint, mesenteric stranding likely represents a secondary perfusion or traction injury rather than direct mucosal perforation. Enhanced detection of this subtle finding may reflect the increased conspicuity of mesenteric fat planes when opacified bowel loops are present.4,15 However, this did not translate into improved clinical decision-making, as intervention rates, complication profiles, and mortality remained unchanged. Previous radiology studies similarly show that bowel wall hypo-enhancement or mesenteric hematoma—not oral contrast extravasation—are the most specific indicators of clinically significant HVI requiring surgery.3,4,14,15
Our findings are consistent with prior studies showing limited value of enteric contrast in trauma imaging.7-10 Importantly, oral contrast introduces additional delays due to contrast transit through the bowel—often 30 to 90 min.7,9 The feasibility of oral contrast administration is further limited by clinical considerations; many trauma patients cannot safely ingest contrast due to altered mental status, airway compromise, or the need for urgent surgery.12,13
While mortality was higher in patients who underwent CT with IV contrast only, no differences in mortality were observed between imaging modalities when adjusting for patient ISS. Patients who underwent CT with IV had higher ISS, required higher rates of blood transfusion, and were more likely to require ICU hospitalization, suggesting that baseline injury severity explained the high mortality in patients who underwent repeat imaging with CT IV.
The association between delayed operative intervention and adverse outcomes underscores the importance of timely recognition and management rather than imaging technique. Prior studies demonstrate that delays beyond 24 h in diagnosing HVI can double mortality risk and increase septic complications,1,15 consistent with our finding that patients with complications or death experienced substantially longer time to surgery. Together, these data highlight that clinical vigilance and early operative decision-making remain the decisive factors in patient outcome.
This study has several limitations. It was conducted at a single tertiary trauma center, which may limit generalizability. Imaging acquisition and timing were not protocolized, introducing potential selection bias regarding which patients received repeat CT or oral contrast. Additionally, the retrospective design limits causal inference, and small numbers of certain findings (eg, contrast extravasation and duodenal or pancreatic injury) may reduce statistical power. Finally, while all scans were interpreted by fellowship-trained radiologists, inter-reader variability was not formally assessed.
Conclusion
The use of oral contrast in repeat CT imaging confers no diagnostic advantage, introduces avoidable delays, and does not alter outcomes. Nevertheless, select cases where initial imaging is equivocal may merit consideration of repeat imaging that should be performed on a prompt and timely basis without requirement for oral contrast. CT with IV contrast alone, combined with high clinical vigilance and timely surgical intervention when indicated, remains the most effective approach for managing patients at risk for missed hollow viscus injury.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.