
Abstract
Background
Reliable and broadly applicable tools for survival risk stratification in stage II/III colorectal cancer (CRC) remain limited. The Heidelberg prognostic pancreatic cancer (HELPP) score is a multidimensional index integrating tumor burden, systemic inflammation, nutritional status, and host physiological condition, and has been well validated for prognostication in pancreatic cancer. We hypothesized that this score would also be applicable to CRC and investigated its prognostic utility.
Methods
A consecutive cohort of 481 patients with pathological stage II/III CRC undergoing curative resection was retrospectively interrogated. The prognostic impact of the HELPP score was assessed using Kaplan-Meier estimates and Cox proportional hazards modeling.
Results
With a median follow-up of 65 months, 129 patients died. Kaplan-Meier analyses demonstrated clear and consistent stratification of both overall survival (OS) and relapse-free survival (RFS) according to the HELPP score. In univariate analyses, a HELPP score >3 was significantly associated with worse OS and RFS. Importantly, this association remained robust after adjustment for clinically relevant covariates, with HELPP score >3 independently predicting OS (hazard ratio [HR] 1.99, 95% confidence interval [CI] 1.25-3.18, P = 0.004) and RFS (HR 1.78, 95% CI 1.19-2.66, P = 0.005).
Discussion
The HELPP score delivers robust, independent prognostic stratification in stage II/III CRC and represents a practical, clinically actionable tool for refined risk assessment. Its integration into clinical practice may enable more precise tailoring of adjuvant therapy and surveillance, advancing individualized management in CRC.
Key Takeaways
• Even after curative resection, advanced-stage colorectal cancer exhibits a substantial risk of recurrence and marked prognostic heterogeneity, which cannot be adequately captured by conventional tumor biology-based stratification systems alone. • We demonstrated that the HELPP score, originally established as a prognostic index in pancreatic cancer, effectively stratified long-term outcomes after curative resection in stage II/III colorectal cancer, implying its potential to inform individualized therapeutic decision-making.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer-related mortality worldwide, accounting for more than 900,000 deaths annually. 1 With ongoing lifestyle changes, including increasing obesity and dietary shifts, the incidence of CRC is projected to rise further, making it a major public health concern. 2 Despite advances in surgical techniques and adjuvant modality, the overall prognosis of CRC remains unsatisfactory. 3 In particular, substantial heterogeneity exists among patients with advanced disease that cannot be fully captured by conventional tumor biology-based classifications alone, posing challenges to the optimization of treatment strategies. 4
In this context, reliable tools for objective survival risk stratification would be of considerable clinical value. However, currently available modalities remain limited. Several inflammation-based indices, such as the Glasgow prognostic score (GPS), 5 have been proposed as simple prognostic markers, but their association with survival outcomes has not been consistently demonstrated, and the overall evidence remains inconclusive. 6 Therefore, robust and widely applicable prognostic parameters for CRC are still lacking.
In pancreatic cancer, another malignancy with persistently poor prognosis, a prognostic scoring system that has recently attracted attention is the Heidelberg prognostic pancreatic cancer (HELPP) score. 7 This score integrates routinely available clinical and laboratory parameters, including physiological condition assessed by the American Society of Anesthesiologists physical status (ASA-PS), C-reactive protein (CRP), albumin, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), and platelet count. Its ability to stratify survival risk has been demonstrated in large pancreatic cancer cohorts and subsequently validated in independent studies.8,9 Given the biological rationale underlying this score, it is conceivable that the HELPP score may also be applicable to CRC. However, to the best of our knowledge, its prognostic relevance in CRC has not yet been investigated.
Based on this hypothesis, we retrospectively evaluated the association between the HELPP score and long-term outcomes in patients with resectable advanced CRC.
Methods
Study Population
Consecutive patients who underwent curative colorectal resection for CRC at our institution between January 2009 and December 2022 were retrospectively analyzed. The exclusion criteria were as follows: pathological stage 0/I CRC, presence of distant metastasis (stage IV), non-adenocarcinoma histology, preoperative endoscopic resection, neoadjuvant chemotherapy or chemoradiotherapy, postoperative follow-up of less than 3 months, simultaneous resection for another malignancy, and insufficient preoperative data. After applying these criteria, a total of 481 patients with pStage II/III CRC were included in the final analysis. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of our institution (Approval No. 24-33). The requirement for written informed consent was waived because of the retrospective study design.
Clinicopathological Data
Indications for surgery, selection of surgical procedures, perioperative chemotherapy strategies, and postoperative surveillance protocols were generally based on the Japanese Society for Cancer of the Colon and Rectum Guidelines. 10 In principle, patients with stage III disease received adjuvant chemotherapy, primarily with CAPOX or FOLFOX regimens. For stage II disease, adjuvant therapy was considered in patients with high-risk features, such as T4 invasion or obstruction. Tumor staging was determined according to the ninth edition of the TNM classification established by the Union for International Cancer Control. 11 The study period was divided into an early era (2009-2017) and a contemporary era (2018-2022), in accordance with the timeline of the IDEA collaboration. 12
The ASA-PS score was prospectively documented preoperatively by an anesthesiologist in all cases. Right-sided colon cancer was defined as tumors located in the cecum, ascending colon, or transverse colon, whereas left-sided colon cancer included tumors involving or located distal to the splenic flexure. A bridge-to-surgery procedure was defined as decompression by insertion of a self-expandable metallic stent or an ileus tube in patients presenting with obstructive CRC. A minimally invasive approach was defined as a laparoscopic and/or robotic procedure.
The study period corresponded to a transitional phase at our institution, during which laparoscopic and robotic approaches were gradually introduced. Consequently, a substantial proportion of procedures were performed via open surgery. However, the use of minimally invasive approaches did not differ significantly by stage (stage II: 65/255 [25.5%] vs stage III: 57/226 [25.2%]). Postoperative surveillance was scheduled to include hematological tests and physical examinations at least every 3 months for 5 years after surgery. Surveillance consisted of routine physical examinations, colonoscopy, computed tomography, abdominal ultrasonography, and standard blood tests performed at intervals in accordance with the Japanese Society for Cancer of the Colon and Rectum guidelines. 10 Survival and recurrence status were confirmed through outpatient visits, medical record reviews or, when necessary, structured telephone interviews. Follow-up of the entire cohort was completed in February 2026.
GPS and HELPP Score
The GPS was evaluated as a conventional inflammation-based prognostic marker. Patients with both elevated CRP (>10 mg/L) and hypoalbuminemia (<35 g/L) were assigned a GPS of 2. Those with only one abnormal parameter were assigned a score of 1, whereas patients with neither abnormality were assigned a score of 0. 5
The HELPP score is a composite prognostic index incorporating ASA-PS, tumor marker levels (CEA and CA19-9), platelet count, CRP, and serum albumin. Risk points were assigned based on predefined thresholds for each variable, and the total score was obtained by summing these points (Supplemental Table S1): ASA-PS ≥3 (1 point); CA19-9 ≥ 37 kU/L (1 point) and ≥400 kU/L (2 points); CEA ≥2.5 μg/L (1 point); platelet count <150 ×109/L (2 points); CRP ≥5 mg/L (1 point) and ≥20 mg/L (2 points); and CRP ≥20 mg/L combined with albumin <35 g/L (3 points). 7
Statistical Analysis
All statistical analyses were performed using JMP Student Edition version 19.1.0 (SAS Institute, Cary, NC, USA). All tests were two-tailed, and P values <0.05 were considered statistically significant.
Overall survival (OS) was defined as the interval from the date of surgery to death from any cause. Relapse-free survival (RFS) was defined as the interval from surgery to the first documented recurrence or death from any cause. Survival curves were estimated using the Kaplan-Meier method and compared using the log-rank test. Representative clinically relevant variables, together with the GPS and the HELPP score, were first evaluated using univariate Cox proportional hazards models. Variables assessed in the univariate analysis were subsequently entered into multivariate Cox proportional hazards models. Separate multivariate models were constructed to evaluate the independent prognostic significance of the GPS and the HELPP score.
Results
Clinicopathological Characteristics of the Patients
Baseline Clinicopathological Characteristics of the Study Cohort
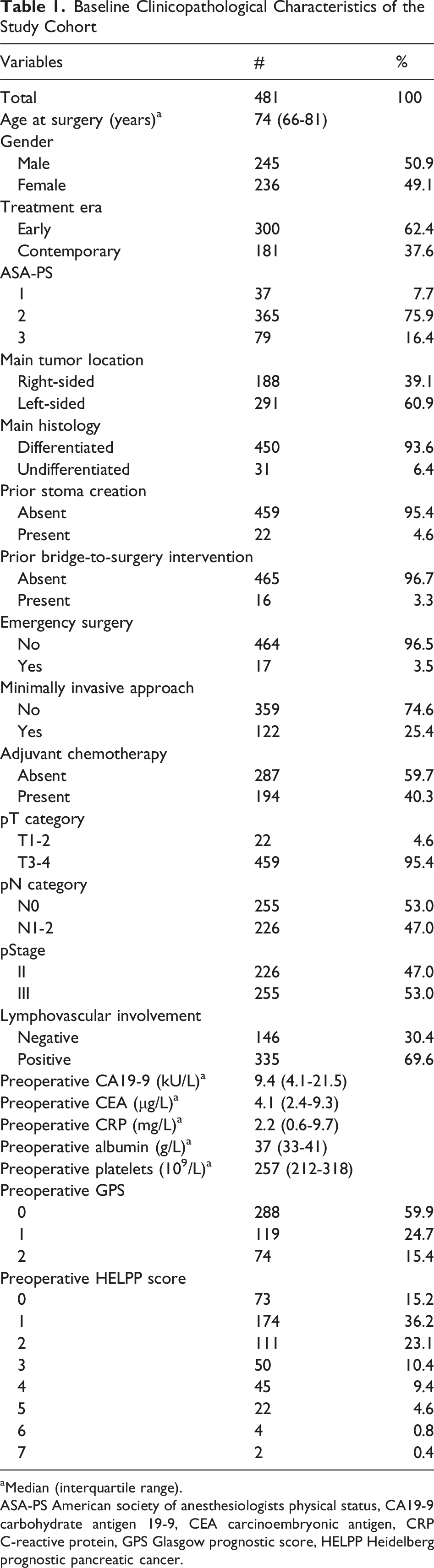
aMedian (interquartile range).
ASA-PS American society of anesthesiologists physical status, CA19-9 carbohydrate antigen 19-9, CEA carcinoembryonic antigen, CRP C-reactive protein, GPS Glasgow prognostic score, HELPP Heidelberg prognostic pancreatic cancer.
The median follow-up period among survivors was 65 months. During follow-up, 121 patients developed metachronous recurrence, of whom 71 ultimately died from the primary disease, while 58 patients died of causes unrelated to CRC.
Survival Analyses
The cutoff value for the HELPP score was defined according to a previous study, categorizing patients into two groups: HELPP score >3 (n = 73) and ≤3 (n = 408).7-9 Kaplan-Meier survival analyses based on this classification demonstrated clear separation of OS curves, with significantly poorer survival observed in patients with a HELPP score >3 (P = 0.008). Similarly, RFS was also distinctly stratified by the HELPP score (P = 0.004) (Figure 1). Kaplan-Meier curves for overall survival and relapse-free survival according to HELPP score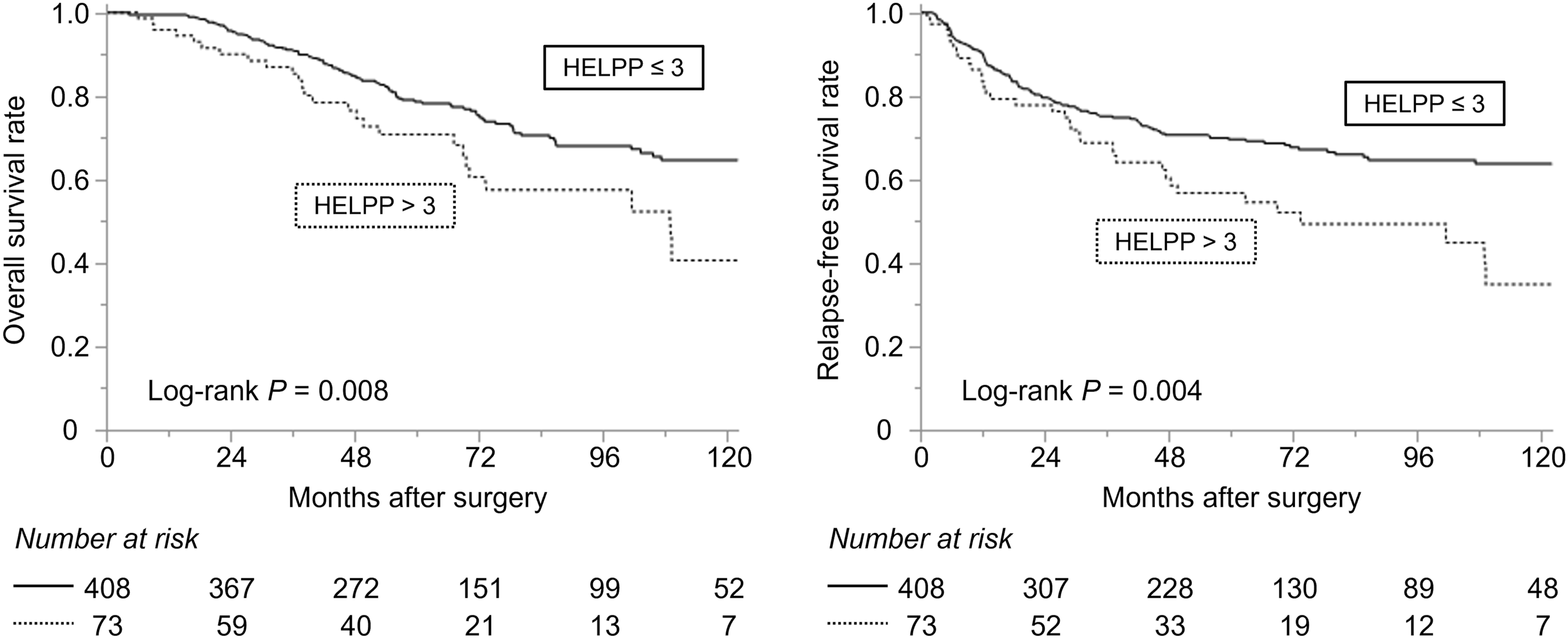
Univariate Cox Regression Analyses for Overall and Relapse-free Survival
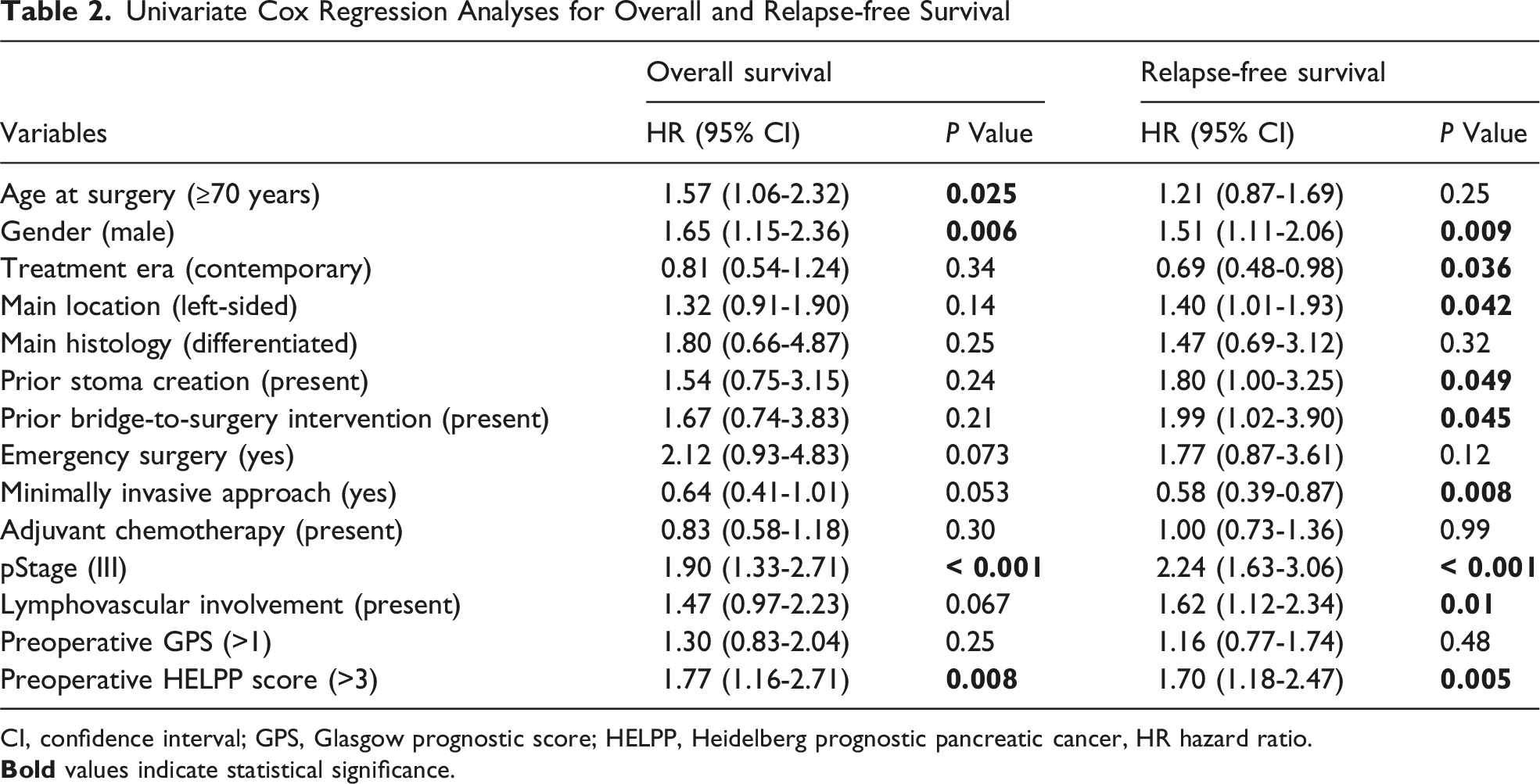
CI, confidence interval; GPS, Glasgow prognostic score; HELPP, Heidelberg prognostic pancreatic cancer, HR hazard ratio.
Multivariate Cox Regression Analyses for Overall and Relapse-free Survival
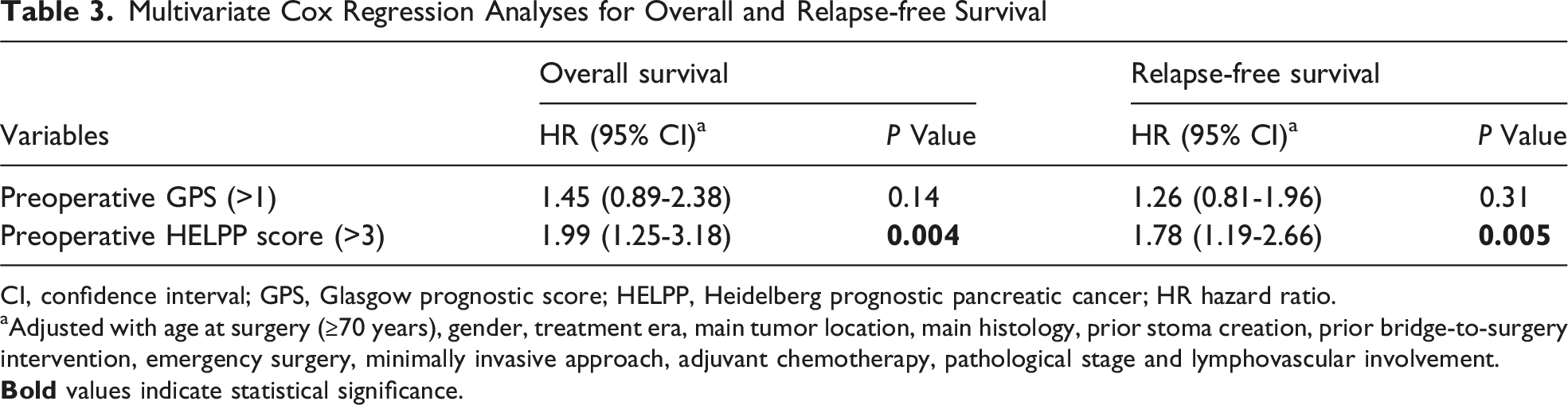
CI, confidence interval; GPS, Glasgow prognostic score; HELPP, Heidelberg prognostic pancreatic cancer; HR hazard ratio.
aAdjusted with age at surgery (≥70 years), gender, treatment era, main tumor location, main histology, prior stoma creation, prior bridge-to-surgery intervention, emergency surgery, minimally invasive approach, adjuvant chemotherapy, pathological stage and lymphovascular involvement.
Discussion
In CRC, particularly in stage II/III disease, substantial biological heterogeneity results in widely variable clinical outcomes. 4 Although conventional risk stratification has relied on tumor-centric factors such as the TNM system, these parameters alone are insufficient to capture the complexity of individual prognosis. In this context, our study demonstrates that the HELPP score provides robust stratification of both OS and RFS in patients undergoing curative resection for stage II/III CRC, outperforming the GPS. To the best of our knowledge, this represents the first evidence supporting the prognostic utility of the HELPP score beyond pancreatic cancer.
The strength of the HELPP score lies in its multidimensional design, integrating systemic inflammation (CRP), nutritional status (albumin), hematologic parameters (platelet count), tumor burden (CEA and CA19-9), and host physiological reserve (ASA-PS). This framework reflects the biological interplay between tumor aggressiveness and host resilience, which is increasingly recognized as a critical determinant of cancer outcomes. Importantly, each of these components has been independently associated with survival in CRC and has been incorporated into various prognostic models and nomograms. 13 Their integration into a single composite index therefore represents a rational and biologically grounded approach to risk stratification.
A key advantage of the HELPP score is its ability to overcome limitations inherent to individual biomarkers. Single parameters, such as CA19-9 or CRP, are subject to biological variability and external influences; for instance, approximately 5-10% of patients are Lewis antigen-negative and do not express CA19-9, while inflammatory markers may be elevated due to non-malignant conditions. 14 By combining multiple domains, the HELPP score reduces susceptibility to such artifact biases and provides a more stable and reliable assessment of prognosis.
The inclusion of ASA-PS further enhances the clinical relevance of the HELPP score. While originally designed to assess perioperative risk, ASA-PS has emerged as a meaningful indicator of host vulnerability and is increasingly linked to oncological outcomes across solid tumors. 15 Unlike more complex indices such as the Charlson comorbidity index, 16 the HELPP score relies exclusively on routinely available and easily obtainable parameters, making it highly feasible for real-world implementation.
From a clinical perspective, the HELPP score has the potential to refine treatment strategies in stage II/III CRC. Current decisions regarding adjuvant therapy are largely guided by pathological staging and selected high-risk features; however, these factors do not fully reflect individual recurrence risk. 4 The HELPP score offers an additional layer of risk stratification, identifying patients who may benefit from intensified adjuvant treatment and closer surveillance, as well as those who could be considered for treatment de-escalation. In this regard, the HELPP score represents a practical and clinically actionable tool that may facilitate more personalized management of CRC. However, at present, it may be premature to consider it a universally applicable tool. Rather, it may be more appropriately interpreted as a multidimensional host-tumor score that shows prognostic value across a heterogeneous treatment era.
Several limitations merit careful consideration. This study is inherently constrained by its retrospective, single-institution design, and thus the observed associations may, at least in part, reflect cohort-specific effects rather than universally reproducible findings. In addition, the HELPP score may be susceptible to confounding by non-malignant inflammatory conditions, which were not systematically controlled for in the present analysis. Furthermore, the extended study period spanning more than a decade introduces the possibility of temporal heterogeneity, as advances in surgical techniques, perioperative care, and systemic therapies may have influenced patient outcomes. 4 While the study attempts to mitigate bias by stratifying the study period into early and contemporary eras, this approach is not sufficient to fully eliminate it. Therefore, prospective validation in independent, contemporary cohorts is warranted to confirm its clinical utility and generalizability. Finally, although we adopted a cutoff value of 3 in accordance with prior studies,7-9 the optimal threshold for risk stratification in CRC remains to be established and may require recalibration in disease-specific contexts.
In summary, the HELPP score was an independent predictor of both OS and RFS in patients with stage II/III CRC. Risk stratification based on the HELPP score may help inform personalized therapeutic decision-making and surveillance strategies.
Supplemental Material
Supplemental Material - Application of the Heidelberg Prognostic Pancreatic Cancer Score for Survival Risk Stratification in Stage II/III Colorectal Cancer
Supplemental Material for Application of the Heidelberg Prognostic Pancreatic Cancer Score for Survival Risk Stratification in Stage II/III Colorectal Cancer by Masayuki Urabe, Masaya Hiyoshi, Mami Suzuki, Takahiro Fukai, Yui Hasegawa, Emi Terai, Yoshitaka Kiya, Goki Morizono, Toshiyuki Watanabe, and Yojiro Hashiguchi in The American Surgeon™.
Footnotes
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and the guidelines of our Institutional Ethics Committee (approval ID 24-33).
Consent to Participate
It was exempted from the requirement for written informed consent due to its retrospective nature.
Author Contributions
MU contributed to the conception and design of the study. All authors acquired data. MU performed data interpretation and drafted the manuscript. MH, YK, GM, TW and YH critically revised the manuscript. All authors read and approved the final version prior to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as there were no new data generated or analyzed during the course of this study.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.