
Abstract
Academic publishing in surgery has undergone profound change during the past several decades. Expansion of medical schools, residency programs, international academic centers, and digital publishing platforms has produced unprecedented growth in manuscript submissions and intensified competition for professional attention. Journals are judged both by readership, as measured by article downloads, and by scientific influence, as reflected in scholarly citation. At The American Surgeon, these changes prompted development of editorial frameworks designed to identify contributions most likely to matter to practicing surgeons and subsequent investigators. Many manuscripts contained observations whose significance was underrecognized by their authors. This observation led to the Hidden Publishable Idea (HPI), a framework for identifying contributions most useful to readers. Once identified, the HPI often revealed methodological limitations that imposed an evidentiary ceiling, preventing definitive conclusions while suggesting new hypotheses for future investigation. Analysis of downloads and citations suggested that readership and scholarly adoption are related but distinct outcomes. This observation led to development of the CitDL matrix, a two-by-two framework based on high and low download and citation performance. The editorial objective was not simply manuscript acceptance, but identification and development of contributions that could move manuscripts toward greater readership, greater scholarly engagement, or both. These concepts represent adaptive responses to the contemporary challenge of helping useful ideas find their audience and contribute to the advancement of surgical practice and science.
Keywords
The goal of a surgical journal is not just to publish papers. It is to publish papers that surgeons will read and investigators will cite in their own research. Publication is an editorial decision. Readership and citation are judgments made by the profession itself.
For much of the twentieth century, academic publishing in surgery was dominated by departments of surgery at major academic medical centers and a relatively small number of journals. The editors in chief of those journals were often among the most prominent surgeons in the United States, and their editorial decisions helped define the boundaries of academic surgery itself. Manuscripts were prepared on typewriters, submitted in triplicate, mailed to reviewers, and eventually returned to the editor with handwritten comments filling the one-inch margins required for publication. Editorial review was slower, more personal, and centered on a comparatively small community of academic surgeons.
The science itself was changing. Surgical investigators increasingly adopted rigorous statistical methods, explored the biochemistry and cell biology of disease, and organized multicenter collaborations capable of generating data on a scale previously impossible. The sophistication of manuscripts increased, and the scholarly conversation improved accordingly. Academic departments of surgery remained full participants in this evolution and generally kept pace with rising expectations for methodological rigor and scientific depth.
The world that produced those editorial assumptions no longer exists.
As the number of medical schools, residency programs, investigators, journals, and manuscripts increased, the attention available to any individual article became increasingly diluted. Surgeons did not acquire more hours to read only because more papers were published. Publication became easier. Visibility became harder.
The number of medical schools and graduate medical education programs in surgery has increased substantially over the past few decades. New schools and residency programs expect their faculties to engage in productive scholarship, where the coin of the realm for recruitment, promotion, and academic advancement remains publication in peer-reviewed journals. Students seeking admission to medical school and applicants competing for residency positions likewise pursue publication as evidence of academic accomplishment. The demand for publication now extends from trainees entering medicine to senior faculty seeking promotion.
At the same time, academic surgery has become increasingly international. Universities throughout the world rely upon publication as a measure of scholarly achievement, and publication in established English-language journals has become an important source of academic legitimacy.
The mechanics of publishing have changed just as dramatically. Electronic submission platforms replaced typewritten manuscripts and postal mail. Manuscript assignment, peer review, editorial decision making, revision, and production are now largely computer-driven processes. Online publication is routine, and the printed journal has become largely symbolic. The effort required to submit and process a manuscript has fallen substantially, while the capacity of journals to receive and evaluate submissions has expanded.
The result has been a dramatic increase in manuscript submissions. More surgeons conduct research. More trainees seek publication. More institutions expect scholarly output. More investigators throughout the world compete for space in established journals. Editors now confront not a shortage of material suitable for review, but a continual flow of submissions seeking publication.
The consequence has not simply been more manuscripts. It has been a fundamental change in the editorial problem.
The challenge now is to identify manuscripts likely to contribute to the ongoing conversation of academic surgery. The articles most valuable to a journal were not necessarily those that were simply published. They were the articles that surgeons chose to read and that investigators subsequently cited in their own research.
Throughout this period, The American Surgeon served not only major academic medical centers but also regional surgical societies, community-based training programs, military and Veterans Affairs systems, international investigators, and medical schools seeking to establish or expand their scholarly presence. In many respects, the journal became part of the scholarly infrastructure of the broad middle of academic surgery.
Many submissions were not the randomized trials, prospective multicenter studies, large prospective registries, and translational investigations that had increasingly become the currency of higher-impact surgical journals. Instead, they arrived as retrospective institutional experiences, database analyses, systematic reviews, case reports, and surveys. The majority were honest, competently conducted, and methodologically recognizable. Yet many addressed questions that had already been answered elsewhere. They confirmed established associations, repeated familiar observations, or described experiences that mirrored those already present in the literature.
The problem was rarely validity. The problem was whether the findings were sufficiently unique and of interest to the readership beyond what had already been established.
The traditional editorial response was straightforward: the paper was not advancing the literature and therefore did not merit publication. Many such manuscripts were single-center retrospective reviews addressing questions that had already been explored in larger prospective studies, multicenter collaborations, or national databases. Others were case reports describing unusual presentations, rare complications, or novel operative experiences that were interesting but, as written, suggested little beyond the fact that the event had occurred.
Yet repeated experience suggested a more complicated reality.
Although these studies often lacked the scale and scope of larger investigations, they possessed a granularity that was frequently unavailable in multicenter trials and large databases. Within the data set there was sometimes a finding that illuminated a subset of patients, a clinical decision point, a threshold effect, or a systems issue that had been obscured by the larger numbers of more comprehensive studies.
What was striking was how often these observations were overlooked by the authors themselves. The manuscript reported the finding, but it appeared in a table, a subgroup analysis, or a secondary outcome rather than in the title, abstract, or conclusions. The data contained a contribution that was more interesting than the question the authors believed they were answering.
This occurred often enough that we adopted the shorthand term Hidden Publishable Idea (HPI). The phrase was not entirely accurate. The finding was not always hidden, and it was not necessarily publishable in its original form. More often, the observation was present but underappreciated.
Common Manuscript Contexts and Their Likely Hidden Publishable Ideas
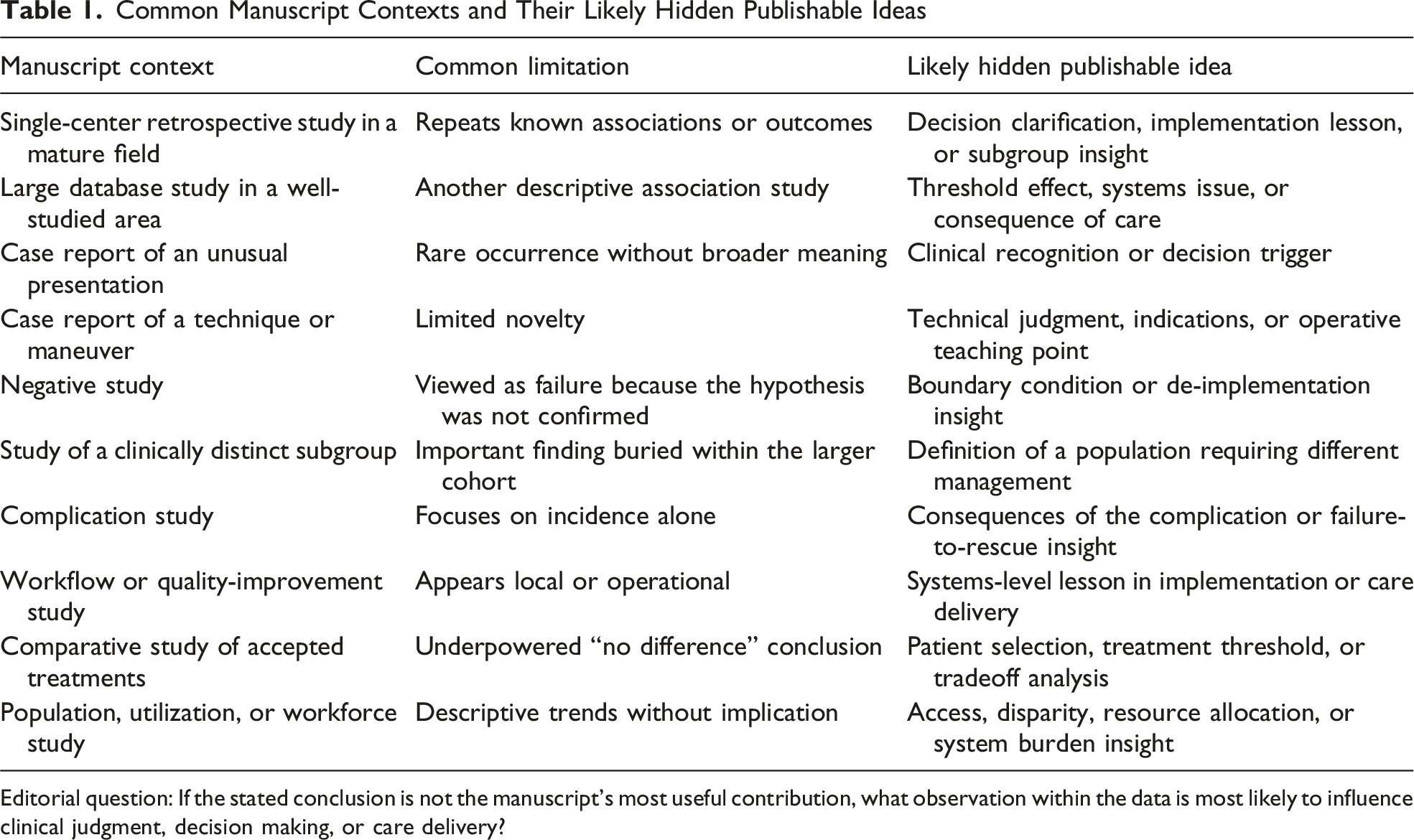
Editorial question: If the stated conclusion is not the manuscript’s most useful contribution, what observation within the data is most likely to influence clinical judgment, decision making, or care delivery?
Recognition alone, however, did not solve the editorial problem. In many cases, identification of the HPI immediately revealed a second challenge. The more interesting clinical insight suggested by the data was not always fully supported by the study design itself. We frequently found ourselves suggesting an HPI only to realize that the available data could not sustain the broader conclusions implied by that interpretation.
Then part of the editorial critique became identifying the next logical step in the investigation. The HPI often represented not what the current study had proven, but what the findings suggested should be studied next. A retrospective review might identify a subgroup requiring prospective evaluation. A case report might reveal a phenomenon deserving systematic investigation. A database analysis might identify an association whose mechanism required further study.
In this sense, the HPI frequently served as a bridge between the current manuscript and the authors’ next project.
Predominant Study Designs Encountered in Contemporary Specialty Surgical Publishing and Their Typical Evidentiary Ceilings
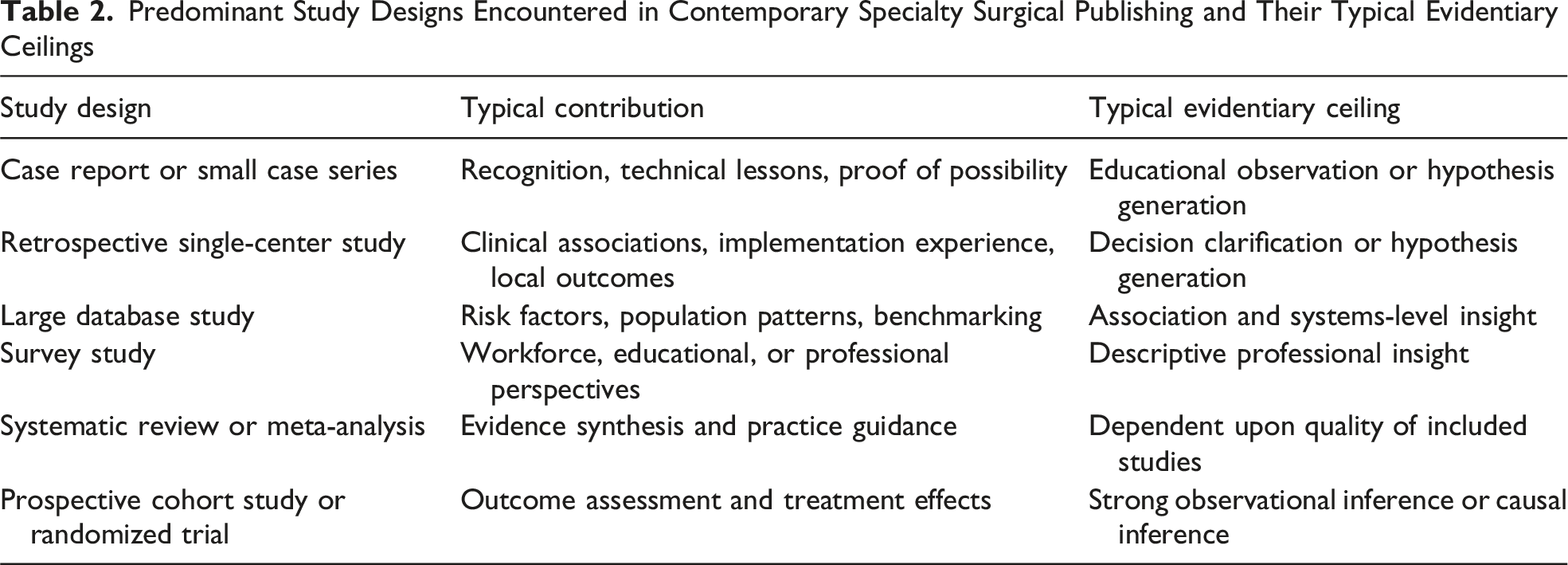
The goal of HPI and the editorial frameworks summarized in Tables 1 and 2 was to identify manuscripts most likely to contribute to the ongoing conversation of academic surgery. The most valuable articles were those that surgeons chose to read, found useful in their clinical practice, and subsequently cited in research that advanced surgical knowledge.
This perspective shifted attention from the manuscript before publication to its performance after publication. If the purpose of editorial review was to identify and develop contributions that mattered, then an obvious question followed: were readers actually finding and using those contributions?
As we examined article performance after publication, it became apparent that downloads and citations were often measuring different phenomena. Articles that attracted substantial readership were not always heavily cited, and highly cited articles did not always generate the largest number of downloads.
Downloads often reflected clinical interest. Editorials, reflective essays, historical articles, educational reviews, and practical clinical guidance frequently attracted substantial readership because surgeons found them useful, interesting, or relevant to their professional lives. Citations reflected something different. Citations represented incorporation into the scholarly literature and participation in the scientific conversation. They occurred when investigators judged a paper sufficiently relevant to inform subsequent research.
The articles most valuable to a journal were often those that achieved both. They attracted readers because they addressed questions surgeons cared about and accumulated citations because they advanced understanding of those questions. Such articles combined topical interest with scholarly contribution.
Every journal seeks highly cited articles. Those articles frequently generate substantial readership as well. The reality for specialty journals, however, is that many of the most highly cited papers gravitate toward journals with substantially higher impact factors and broader readership. Our objective was therefore different. Rather than pursuing occasional home runs, we sought to improve the manuscripts we received by helping authors identify contributions that would be more interesting to clinical surgeons and more useful to subsequent investigators.
This objective reinforced the importance of the Hidden Publishable Idea. The HPI represented the part of a manuscript most likely to attract attention from both audiences. For that reason, we increasingly encouraged authors to place the HPI where readers were most likely to encounter it: in the title, in the first portion of the abstract, and in the opening sentences of the discussion. These were often the only portions of a manuscript many readers would review before deciding whether to continue reading.
CitDL Matrix: Visibility and Scholarly Impact
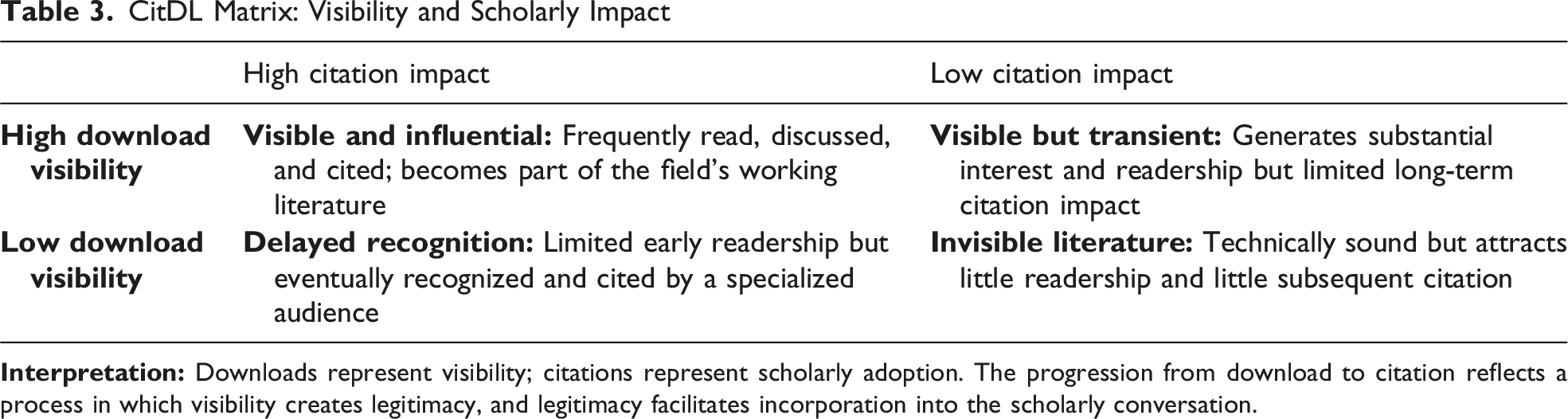
The CitDL framework also suggested that visibility operates at both the article and journal level. Articles that attracted readership increased the visibility of the journal itself. Increased journal visibility strengthened legitimacy, broadened readership, and improved the likelihood that future articles would enter the scholarly conversation. In this sense, downloads were not merely article metrics. They were indicators of the journal’s participation in the professional life of surgery.
The pathway increasingly appeared to be:
Publication → Visibility → Legitimacy → Citation.
Readers must first encounter an article. They must recognize its relevance. The article must enter the collective awareness of the field before it can become part of the scholarly conversation. Citation is therefore more than acknowledgment of prior knowledge. It is also an act of trust. When investigators cite a paper, they signal that it deserves inclusion in the scholarly conversation they are constructing.
The impact factor of The American Surgeon has remained modest, hovering near 1.0, a value we sometimes jokingly referred to as the Mendoza line of scholarly publishing. We could aspire to attract occasional highly cited articles, but those manuscripts often found homes elsewhere. Our approach was different. We sought to identify useful contributions, improve their presentation, and increase their visibility. In baseball terms, the goal was not to wait for home runs. It was to hit singles, draw walks, advance runners, and steadily move manuscripts toward greater relevance and impact.
The editorial frameworks developed during this period were not independent innovations. The HPI sought to identify contribution. Evidentiary ceiling assessment sought to align contribution with evidence. Executional review sought to determine whether the manuscript successfully delivered that contribution. CitDL sought to understand whether readers ultimately recognized its value.
These frameworks emerged from a common challenge. For most of modern scholarly publishing, editors managed scarcity. The defining challenge of contemporary surgical publishing is managing abundance. In an environment where information is plentiful and attention is limited, editorial stewardship becomes the discipline of identifying signal within noise, aligning contribution with evidence, and helping useful ideas find their audience.