
Abstract
A single dose of ceftriaxone is associated with reduced incidence of early ventilator-associated pneumonia (VAP) and decreased antibiotic exposure in patients with isolated head injury, but the impact in patients with multisystem trauma is unknown. This was a single-center, retrospective cohort study conducted in mechanically ventilated, multisystem trauma patients who were admitted to the intensive care unit (ICU) between September 2020 and September 2024. Patients who received one dose of ceftriaxone within 12 h of intubation were included in the early ceftriaxone group. Early VAP occurred in 3 (10%) patients in the early ceftriaxone group and 15 (25%) patients in the deferred or no antibiotics group (P = .10). No differences in secondary outcomes were identified. In patients who received early ceftriaxone in this cohort, there was no difference in early VAP incidence compared to those who had no or deferred antibiotics past 12 h of intubation; however, the study may have lacked sufficient power to detect a difference. Future, larger studies in multisystem trauma patients are needed to better delineate the impact of prophylactic antibiotics on VAP outcomes.
Introduction
Patients experiencing multisystem trauma and traumatic brain injury (TBI) are at a high risk for ventilator-associated pneumonia (VAP). 1 Pneumonia can occur early after admission and may be related to an aspiration event in the field or before hospital intubation. 2 Other risk factors for VAP in trauma patients include chest trauma, TBI, and alcohol and drug use disorders. 3 The development of VAP can lead to worse clinical outcomes, including longer length of stay (LOS) in the intensive care unit (ICU) and hospital. 4
Antibiotic prophylaxis to prevent VAP has been explored in patients with isolated head injuries and cardiac arrest, demonstrating a reduction in the incidence of VAP and improvements in other outcomes, such as ICU LOS and duration of mechanical ventilation.5–10 However, potential adverse effects of antibiotics, such as Clostridioides difficile infection and increased antibiotic resistance, should be considered prior to routine implementation of antibiotic prophylaxis. 3
Many multisystem trauma patients may require early antibiotic prophylaxis for injuries, particularly those presenting with open extremity fractures. The American Association for the Surgery of Trauma (AAST) clinical consensus document on antibiotic prophylaxis recommends that patients with Gustilo Type III open extremity fractures should be provided antibiotic prophylaxis within 1 h of injury and continued for 24 h after skin closure. Recommended antibiotic regimens for Gustilo Type III fractures include broad-spectrum coverage with either piperacillin-tazobactam, cefazolin plus an aminoglycoside, or ceftriaxone. 11 Therefore, our institutional protocol provides ceftriaxone to patients presenting with Gustilo Type III open extremity fractures, and it is possible that TBI patients may receive early ceftriaxone for this reason.
A recent systematic review and meta-analysis exploring the role of antimicrobial prophylaxis on VAP outcomes in patients with acute brain injury demonstrated potential benefits in preventing overall and early VAP; however, no reduction in late VAP or ICU mortality was demonstrated. 12 Currently, routine antimicrobial prophylaxis for the prevention of VAP is not broadly recommended in general trauma patients or by the Brain Trauma Foundation for patients with TBI.13,14 While early antibiotic administration has been shown to improve VAP outcomes in patients with isolated head injury, it is unclear whether the benefits of early ceftriaxone extend to those with head injury plus multisystem trauma.5–10
The purpose of this study was to compare the incidence of early VAP between mechanically ventilated, multisystem trauma patients with TBI who received early ceftriaxone vs no or deferred antibiotics within 12 h of intubation. We hypothesize that early ceftriaxone use in mechanically ventilated multisystem trauma patients with TBI may yield different VAP outcomes than those reported in isolated head injury populations, given the greater complexity of this cohort. This exploratory, hypothesis-generating observational study aims to evaluate these outcomes.
Methods
This single-center, retrospective cohort study was conducted at a level I trauma academic medical center, in mechanically ventilated patients with multisystem trauma and TBI. Eligible patients included trauma patients 16 years of age and older, admitted to an ICU with TBI and other multisystem trauma, Glasgow Coma Scale (GCS) score less than 12, and mechanical ventilation for a minimum of 48 h, who were admitted between September 30, 2020, and September 30, 2024. Patients could be intubated prior to hospital arrival or up to 48 h after injury for inclusion. Patients were excluded if their injuries were deemed non-survivable or if antibiotics other than ceftriaxone and/or cefazolin (surgical prophylaxis) were administered within 12 h of intubation. TBI was defined from the National Trauma Data Standard (NTDS) Data Dictionary for Trauma Quality Improvement Program (TQIP) measures as having an Abbreviated Injury Scale (AIS) score between 3-6 for a valid qualifying injury in the head AIS chapter with a moderate to severe GCS score (GCS 3-12). 15 Injuries were deemed non-survivable if documentation from the primary or a consult team assessed the injuries as “non-survivable” or if the withdrawal of care resulted in patient death within the first 7 days of admission.
Patients were included in the early ceftriaxone group if they received the first dose of ceftriaxone within 12 h of intubation. Patients were included in the no or deferred antibiotics group if they did not receive antibiotics within 12 h of intubation; however, the use of cefazolin only for surgical prophylaxis was allowed. The decision to prescribe and administer ceftriaxone within 12 h of intubation was based on provider discretion and the assessment of a Gustilo Type III open fracture. The duration of ceftriaxone was determined by the provider and orthopedic consult team, based on the operative course of the patient.
The study was approved by the institutional review board prior to data collection. Data was acquired through the institution’s TQIP database and chart review.
Outcomes
The primary outcome was the incidence of early VAP. Early VAP was defined as receipt of at least 5 days of antibiotics after a positive bronchoalveolar lavage (BAL) culture, which was collected within 2-7 days after intubation. A positive BAL culture was defined as the presence of any bacterial growth in culture. As BAL cultures at our institution are qualitative rather than quantitative, no colony count threshold was used to determine positivity. Additional components, including chest radiography, fever, and leukocytosis, were not included in the definition of VAP as prior studies have demonstrated their limited sensitivity and specificity for diagnosing VAP in trauma and critically ill patient populations.16,17
Secondary outcomes included the incidence of late VAP, VAP relapse, number of ventilator-free and antibiotic-free days at day 28, hospital and ICU LOS, incidence of C. difficile infection, and microbiological data from respiratory cultures in patients with early VAP. Late VAP was defined as receipt of at least 5 days of antibiotics after a positive BAL culture which was collected between 7 and 28 days after intubation. VAP relapse was defined as at least one causative organism from a previous VAP episode (early or late) that grew in a BAL culture between 2 and 14 days after completing at least 5 days of antibiotics for the previous infection. C. difficile infection was defined as both positive C. difficile PCR result and administration of treatment for C. difficile infection for a minimum of 48 h. Information about antibiotics started after 12 h of intubation through day 28 of admission was collected for each group, including the specific antibiotic, duration of use, and time to initiation from intubation.
Statistical Analysis
Comparisons between the early ceftriaxone and no or deferred antibiotics groups were made using Fisher’s exact test or Chi-square for categorical variables and Student’s t test or Mann-Whitney U for continuous variables, as appropriate. Statistical significance was determined by a P value less than or equal to .05. Statistical analyses were conducted using JMP Pro 18.0.2 (JMP Statistical Discovery LLC, Cary, NC).
Results
Baseline Characteristics and Comparison of Primary and Secondary Outcomes of Patients Who Received Early Ceftriaxone Versus no or Deferred Antibiotic Therapy
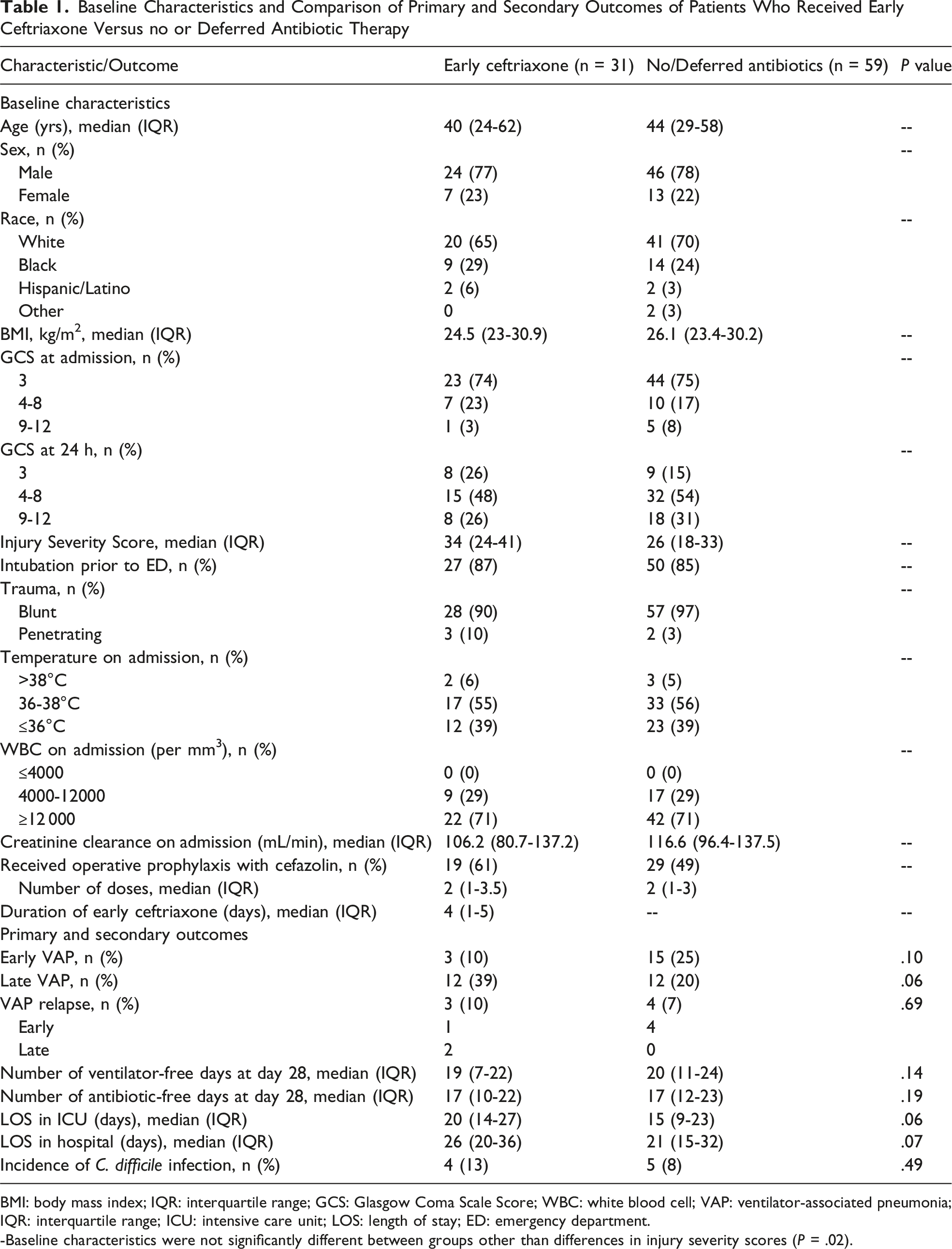
BMI: body mass index; IQR: interquartile range; GCS: Glasgow Coma Scale Score; WBC: white blood cell; VAP: ventilator-associated pneumonia; IQR: interquartile range; ICU: intensive care unit; LOS: length of stay; ED: emergency department.
-Baseline characteristics were not significantly different between groups other than differences in injury severity scores (P = .02).
Twenty-eight patients (90%) in the early ceftriaxone group and 52 patients (88%) in the no or deferred antibiotics group received other antibiotics after 12 hours of intubation. The most common antibiotics prescribed include cefepime, vancomycin, and metronidazole (Appendix 1). On average, patients received 4-7 day courses of antibiotic therapy beginning 4-7 days after presentation.
Outcomes
The primary outcome of early VAP occurred in 3 (10%) patients in the early ceftriaxone group and 15 (25%) patients in the no or deferred antibiotics group (P = .10). Late VAP was observed in 12 (39%) patients in the early ceftriaxone group and 12 (20%) patients in the no or deferred antibiotics group (P = .06). VAP relapse occurred in 3 (10%) patients in the ceftriaxone group and 4 (7%) patients in the comparator group (P = .69) with an average time to relapse of 10 and 8 days, respectively.
No statistically significant differences in the number of ventilator- and antibiotic-free days, ICU and hospital LOS, or C. difficile infection were identified (Table 1). The most common organisms isolated in early VAP cases were Klebsiella species, methicillin-susceptible Staphylococcus aureus (MSSA), Haemophilus influenzae, and Acinetobacter baumannii (Appendix 2).
Discussion
In patients with multisystem trauma and TBI in this cohort, no statistically significant difference was found in the incidence of early VAP between groups; however, the study may have been underpowered to detect a difference. These findings represent an exploratory, hypothesis-generating analysis and, to our knowledge, the first evaluation of this question in a multisystem trauma population, providing important preliminary data in an area with limited prior evidence. While these results should be interpreted with caution, the data suggest that prophylactic antibiotic strategies may need to be tailored to injury patterns rather than broadly applied, and that benefits observed in isolated head injury populations may not translate to more complex trauma cohorts.
Ceftriaxone and other antibiotic strategies have been evaluated for VAP prevention across several critically ill populations. Prior studies in patients with cardiac arrest, stroke, and mixed ICU cohorts have demonstrated reductions in early VAP with prophylactic antibiotic use.7,9,10,18,19 In the PROPHY-VAP trial, early ceftriaxone administration was associated with an 18% reduction in early VAP incidence (14% vs 32%) in patients with isolated brain injury. 9 In our cohort, although not statistically significant, a similar magnitude difference was observed, with the ceftriaxone group demonstrating a 15% lower rate of early VAP (P = .10) despite presenting with higher ISS scores. This finding suggests a potential signal of benefit that warrants further exploration. Larger studies in multisystem trauma patients are needed to better evaluate this outcome in this population.
A systematic review and meta-analysis of 10 studies evaluating antimicrobial prophylaxis for VAP prevention demonstrated reduced rates of overall and early VAP in patients with acute brain injury; however, no benefit was observed for late VAP, duration of mechanical ventilation, ICU mortality, or ICU or hospital length of stay. 12 Notably, patients with TBI represented only a subset of those included, and significant heterogeneity in antimicrobial regimens and study designs limits interpretation. Current Brain Trauma Foundation guidelines do not recommend routine antimicrobial prophylaxis in TBI, and data specific to multisystem trauma patients remain limited.9,10,13 Despite this, prophylactic antibiotics are frequently used in real-world trauma care (eg, for open fractures or penetrating injuries), yet their impact on VAP outcomes in multisystem trauma patients remains unclear. This study helps address this gap by providing preliminary data in a general trauma population and underscores the need for caution in broadly adopting antimicrobial prophylaxis in all patients with TBI, given the limited evidence in this population and concerns related to antimicrobial stewardship and potential adverse effects.
The lack of a significant difference observed in this study, compared with prior findings, may be attributable to several factors. First, the study may have been underpowered; a post-hoc power analysis suggested that a sample size of 200 patients would be needed to detect a significant difference. Additionally, patients in the early ceftriaxone group had a significantly higher ISS, indicating more severe injuries, potentially influencing infection risk. 20 Although both groups met the criteria for major trauma (ISS >15), the higher median ISS in the ceftriaxone group may reflect a greater overall burden of injury. 20 It is also unclear whether pneumonia-specific risk factors, such as rib fractures or lung contusions, were more prevalent in the ceftriaxone group and contributed to the lack of observed benefit.
This study is not without limitations. First, patient factors such as injury patterns, comorbidities, pulmonary injuries, substance use, and immunosuppression were not collected; however, given the small sample size of the study an accurate subgroup analysis based on injury pattern would not have been possible. Second, the use of cefazolin for surgical prophylaxis was allowed, which could have impacted VAP outcomes. However, this adds to the real-world applicability of the findings, since a large proportion of surgical-trauma patients receive antibiotics for surgical prophylaxis. In addition, there were no significant differences in the number of patients who received cefazolin or median number of cefazolin doses received between groups. Additionally, given the retrospective nature of the study, variability in provider practices and VAP prevention strategies over time may have occurred and could have influenced outcomes. Recognizing the challenges in diagnosing VAP in critically ill trauma patients, including limited reliability of conventional indicators such as chest radiography, we employed a VAP definition based on microbiological results and a minimum duration of antibiotic therapy; however, this approach may have led to overestimation of VAP incidence. Finally, based on a post-hoc power analysis, the study lacked power to detect a difference in the primary outcome, and therefore the study is subject to type II error. Future studies with a larger patient population may be able to determine a difference in VAP outcomes if one exists.
Conclusion
In this cohort, patients who received ceftriaxone within 12 h of intubation had no difference in the incidence of early VAP compared with those who did not receive antibiotics or whose antibiotics were deferred beyond 12 h; however, the observed numerical difference in early VAP incidence warrants further investigation, as the study may have been underpowered to detect a difference.
While no significant difference was detected, this study highlights the complexity of antibiotic prophylaxis in trauma patients and underscores the need for larger, prospective studies to better understand the interplay between injury severity, infection risk, and antibiotic timing in real-world practice. Extrapolation of findings from patients with isolated head injury to those with multisystem trauma should be approached cautiously, given concerns about antimicrobial resistance and adverse effects, and because more evidence is needed to determine whether antimicrobial prophylaxis confers benefit in the general trauma population. Further research with a larger sample size is needed to assess the impact of prophylactic antibiotics on VAP outcomes in patients who have experienced TBI and multisystem trauma.
Supplemental Material
Supplemental material - Impact of Ceftriaxone on the Incidence of Early VAP in Patients With TBI and Multisystem Trauma
Supplemental material for Impact of Ceftriaxone on the Incidence of Early VAP in Patients With TBI and Multisystem Trauma by Katelyn Helwig, Bethany R. Shoulders, Barbara A. Santevecchi, and Kaitlin Alexander in The American Surgeon™
Supplemental Material
Supplemental material - Impact of Ceftriaxone on the Incidence of Early VAP in Patients With TBI and Multisystem Trauma
Supplemental material for Impact of Ceftriaxone on the Incidence of Early VAP in Patients With TBI and Multisystem Trauma by Katelyn Helwig, Bethany R. Shoulders, Barbara A. Santevecchi, and Kaitlin Alexander in The American Surgeon™
Footnotes
Author Contributions
Conception and study design: KH, BRS, BAS, and KA; Literature Review: KH; Data acquisition: KH, BRS, BAS, and KA; Data Analysis and interpretation: KH, BRS, BAS, and KA; Drafting of the manuscript: KH, BRS, BAS, and KA; Critical revision: KH, BRS, BAS, and KA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure of Artificial Intelligence Use
During the preparation of this work the author(s) used Microsoft CoPilot in order to enhance the grammar, clarity, and flow of the writing. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.