
Abstract
Perioperative complications from carotid endarterectomy (CEA) are the main drawbacks of the procedure. The aim of this study was to assess the complication rates in patients undergoing CEA under general anesthesia (GA) or regional anesthesia (local anesthesia [LA]) at our institution. Patients undergoing CEA at our regional vascular unit between 2000 and 2004 were included. Data were collated retrospectively from a prospective database. Follow-up was up to 62 months. In all, 383 endarterectomies were performed, 260 of which were under LA. Outcome measures included 30-day death (2.1%), stroke (1.8%), and combined stroke and death (2.8%). A 30-day incidence of stroke, death, and combined stroke and death was lower in the LA group. Incidence of myocardial infarction and transient ischemic attacks, and annual mortality were higher in the LA group. No significant difference was found between the 2 groups. In a unit where CEA is preferentially performed under LA, anesthesia technique failed to significantly influence outcome.
Introduction
Benefit of carotid endarterectomy (CEA) for stroke prevention was illustrated by the symptomatic and asymptomatic CEA trials.1–4 Risks of the procedure, in particular stroke and myocardial complications, may compromise the intended benefit. Anesthesia choice may impact on the outcome of the procedure.
Local anesthesia (LA) has the benefits of observing the patient’s response, following clamping of the ipsilateral carotid artery. Postulated benefits include reduced incidence of inappropriate shunt insertion, decreased cardiorespiratory complications, and preserved cerebrovascular autoregulation. 5
The decision to insert a shunt is based on the clinical symptoms and signs in the patients undergoing CEA under LA. For patients undergoing the procedure under general anesthesia (GA), some advocate shunting all patients or measuring stump pressure, performing electroencephalogram (EEG) or transcranial Doppler to guide selective shunting. Shunting can result in complications such as damage to the arterial wall and by so doing cause emboli to the brain or dissection.
A Cochrane review suggested benefits in terms of stroke reduction and survival in those undergoing CEA under LA when compared to GA. 6 This trend was only evident in nonrandomized trials. There was no significant difference between the groups when data from randomized trials were pooled.
The GA versus LA for carotid surgery (GALA) trial enrolled 3526 patients from 95 centers in 24 countries. 7 The study was underpowered as it failed to reach its population target of 5000 but nonetheless, reported no significant differences between the 2 anesthetic techniques in terms of the primary outcome. There was, however, a marginally lower stroke rate and a higher rate of myocardial infarction (MI) in the LA group. The impact of this result and how individual institutions fair in light of this is yet to be evaluated. Recently, the influence of this study on clinical practice has been questioned. 8
With this in mind, we examined our institution data to assess which technique offered the lowest complication rate and hence allow truly informed consent for our patient population. Secondary outcome measures were the incidence of MI, minor (nondisabling) stroke, transient ischemic attacks (TIAs), local complications, and mortality at 1 year.
Methods
All patients undergoing CEA at the John Radcliffe Hospital regional vascular center, Oxford, between January 2000 and December 2004 were identified from a prospectively collected departmental database. A retrospective analysis of collected data for CEAs was undertaken. Added clinical data were obtained from the patient’s case notes. Follow-up data were obtained from neurology/vascular combined clinic letters.
In this period, both GA and LA for the procedure were performed. Patients undergoing concurrent combined procedures, for example coronary artery bypass, were excluded.
Indication for surgery and severity of carotid stenosis determined by arterial duplex was obtained. In equivocal cases, magnetic resonance angiography (MRA) was performed. All patients had a day of surgery duplex scan to exclude an occluded internal carotid artery prior to operation.
Local anesthesia technique included deep and superficial cervical plexus blockade with bupivacaine 0.375% and local infiltration of the skin and carotid sheath with 1% lidocaine. Sedation was given on an individual patient basis using either propofol or remifentanil.
Monitoring included the use of invasive arterial blood pressure measurement, oxygen saturation, continuous electrocardiogram (ECG), and clinical neurological evaluation. Following a trial clamp of the ipsilateral internal carotid artery, a Pruitt-Inahara shunt was inserted as necessary.
General anesthesia was induced by intravenous propofol and maintained with inhaled isoflurane and nitrous oxide and oxygen. Monitoring included invasive arterial blood pressure measurements, oxygen saturation, and continuous ECG. Shunt usage was based on the measurement of stump pressure and/or transcranial doppler measurement.
All procedures were performed by 1 of the 5 consultant vascular surgeons and a surgical trainee. Surgical technique was at the discretion of the individual consultant. Majority of the cases were performed using a standard procedure with selective patching and a minority using the eversion technique.
All patients were followed up with a 6-week appointment at a joint neurology and vascular clinic with a routine carotid duplex on arrival.
Primary outcome measures were 30-day death, postoperative stroke, and combined stroke and death. Secondary outcome measures assessed 30-day incidence of MI, minor (nondisabling stroke), TIA, local complications, and 1 year mortality between the 2 groups.
Analysis
A contingency table was formed for the categorical variables and Fisher exact test used for statistical analysis. Analysis was performed on an intention-to-treat basis. All analyses were carried out with Graphpad prism version 5 software.
Results
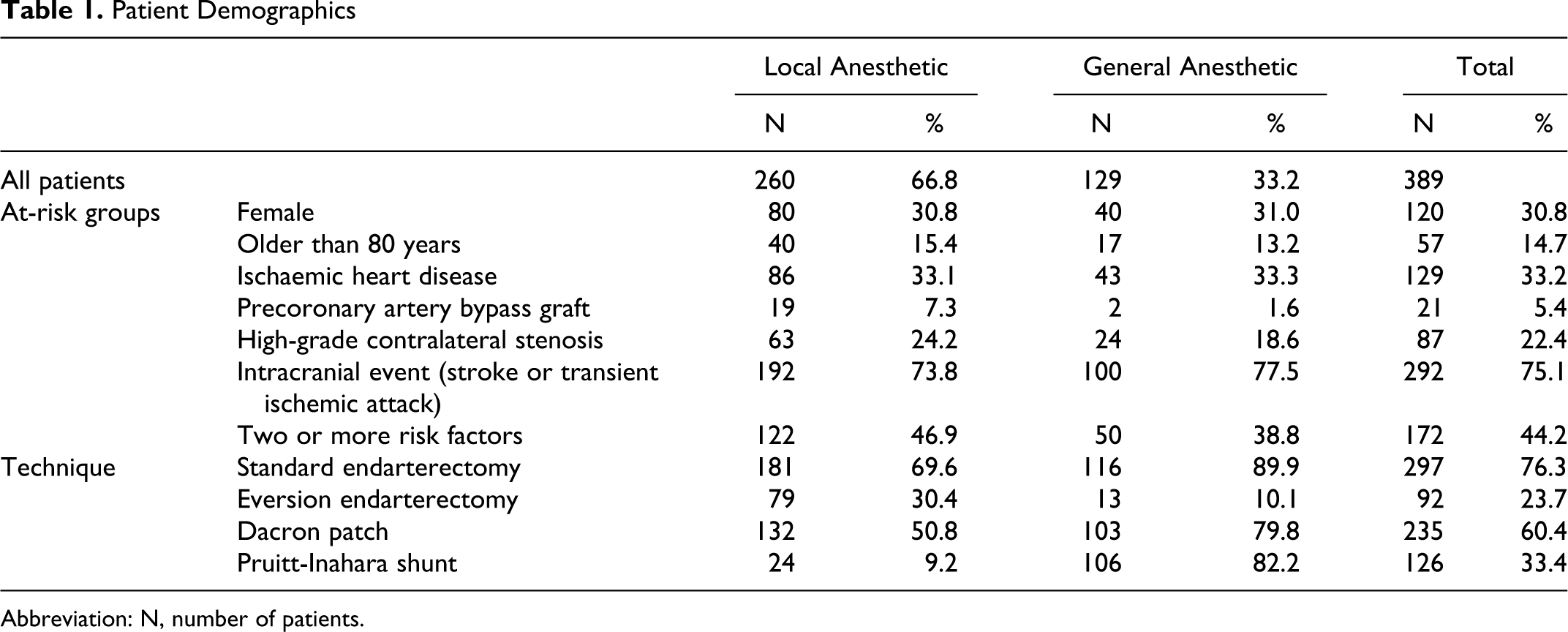
In total, 389 carotid endarterectomies were performed on 384 patients between January 2000 and December 2004. All procedures were performed by 1 of the 5 vascular consultants and a surgical trainee who was the first surgeon in 53% of cases. The majority (n = 260) were performed under LA. A third of the patients were female and approximately 15% were over 80 years old (Table 1 ). In 86% of the procedures, the indication was symptomatic significant stenosis. Cerebral hemispheric symptoms were the presenting complaint in 75% of these cases.
Patient Demographics
Abbreviation: N, number of patients.
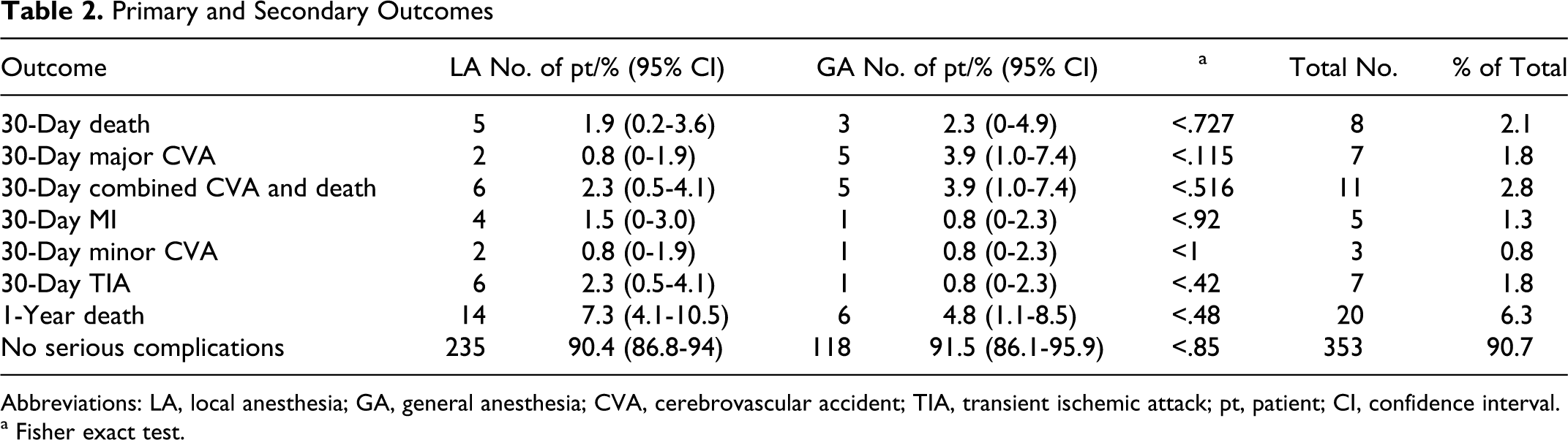
The overall 30-day all-cause mortality was 2.1%. Between the 2 groups, it was 1.9% for LA and 2.3% for GA (Table 2). This difference was not significant (P < .1). One of the deaths in the LA group occurred after intraoperative conversion to GA and later further reexploration under GA.
Primary and Secondary Outcomes
Abbreviations: LA, local anesthesia; GA, general anesthesia; CVA, cerebrovascular accident; TIA, transient ischemic attack; pt, patient; CI, confidence interval.
a Fisher exact test.
Overall 30-day incidence of disabling or fatal stroke was 1.8%; of these, 4 deaths were fatal, 3 occurred within 30 days of surgery, and 1 following a subsequent coronary artery bypass graft (CABG) operation. Those undergoing LA procedures had an incidence of major stroke of 0.8% as compared to 3.9% in the GA group.
Combined mortality and stroke at 30 days occurred in 2.8% of the procedures. Comparison of LA to GA revealed incidence of 2.3% and 3.9%, respectively. Again, this difference did not reach significance.
The incidence of MI within 30 days of surgery was 1.5% for those undergoing an LA procedure and 0.8% for those undergoing a GA procedure. Again, there was no significant difference between the groups. Of the 4 patients who had MI post-LA CEA, 1 occurred following a CABG 3 weeks after the carotid procedure.
Minor strokes occurred in 0.8% of procedures and this incidence persisted irrespective of the mode of anesthesia. Two events were in the contralateral hemisphere to the operated side. Transient ischemic attack was more common in the LA group (2.3%) as opposed to the GA group (0.8%).
Overall annual mortality was 6.3% with a higher incidence (7.3%) in the LA procedures when compared with the GA procedures (4.8%).
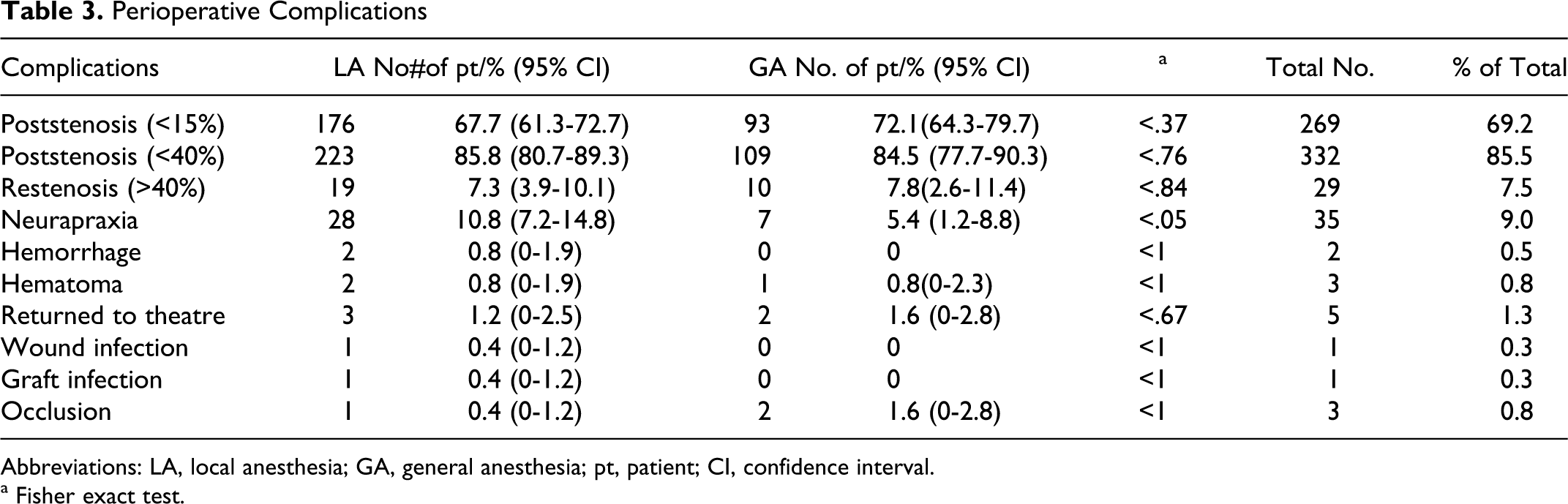
Local complications as summarized in Table 3 occurred with more frequency in LA procedures. Neurapraxia occurred in 9% of procedures and was more frequent in LA procedures (10.8% vs 5.4%), although this was not a significant difference (P < .09).
Perioperative Complications
Abbreviations: LA, local anesthesia; GA, general anesthesia; pt, patient; CI, confidence interval.
a Fisher exact test.
Discussion
The benefit of stroke prevention conveyed by CEA is balanced by the operative complications including 5% to 7% risk of perioperative stroke and 1% risk of perioperative death.1–4 Minimizing the operative risk may enable more patients to benefit from CEA. This study assessed the role of anesthetic technique on perioperative risk factors in a defined population and institution.
In keeping with the recently published data from the GALA trial, we have demonstrated no significant differences in our outcome measures between the 2 techniques. There was a trend toward a lower incidence of perioperative stroke with LA. The similarity continues, with MI being more frequent in the LA procedures.7,15,17–19,21,26–28,30
The combined analysis of the LA and GA groups reveals a 30-day incidence of major (disabling or fatal) stroke of 1.8% and 30-day combined major stroke and death incidence of 2.8%. These results compare favorably with those of the previous major case series and demonstrate that the operative outcomes of CEA at this center fall within expected targets.1–4 This study finds that LA is associated with a lower incidence of perioperative stroke and death than GA, but the difference does not reach statistical significance.
The main limitations of this study include the fact that it is nonrandomized and retrospective. Our practice is also heavily skewed in favor of LA procedures.
The direct comparison of primary outcome data without the consideration of the higher risk individuals in each anesthetic group may underplay the benefits of LA. The risk factors for postoperative stroke and death include female gender, age over 80 years, ischemic heart disease, contralateral stenosis of 70% or more, and an intracranial event as the indication for surgery.1,9–12 Indeed, there were more patients with 2 or more high-risk characteristics in the LA group (46.9% compared with 38.8% in the GA group—no statistical significant) and 7.3% of patients were operated on prior to CABG compared with 1.6% in the GA group (P > .05). However, the proportion of patients with 1 high-risk characteristic is higher in the GA group (36.5% in the LA group compared with 41.1% in the GA group—no statistical significance). One will therefore expect a lower 1-year survival in the GA group. The reverse occurs with a higher death rate at 1 year in those who had an LA operation, but this did not reach statistical significance. The possibility that patients, by virtue of having survived a GA procedure, when compared to an LA procedure, have a lower long-term mortality cannot be discounted. There is, however, no evidence to either support or refute this from the study.
The principal risk factor resulting in perioperative morbidity and mortality of CEA is stroke. Good cerebral perfusion is vital for the prevention of stroke intraoperatively. Historically, this has been facilitated by the routine shunting of the internal carotid artery. However, this has potential complications, including damage to the arterial intima layer and subsequent early thrombosis or late stenosis, embolization of atherosclerotic material from the common carotid artery, and air embolism, all of which may cause stroke.13,19 A major advantage of LA is that patients can be selectively shunted on the basis of the findings when the trial clamp is performed. Indeed, in this cohort of patients, the incidence of shunting is 9.2% in the LA group, compared with 82.2% in the GA group (P < .05), and this may contribute to the lower incidence of stroke and death in the former group.
A further potential benefit of LA is the preservation of cerebral oxygenation by a reflex rise in blood pressure on cross clamping; this may be neuroprotective.14,23–25 However, it is also known that general anesthetics, such as isoflurane and sevoflurane, reduce neuronal activity and the cerebral metabolic rate for oxygen and may thereby be attenuated; this may offset the putative disadvantage of absent cerebral protective reflexes under GA.14,29
Patients with cerebrovascular disease often have ischemic heart disease and postoperative cardiac events contribute to the perioperative morbidity and mortality of CEA. In this cohort of patients, the 30-day incidence of MI was 1.3% and was higher in the LA group (1.5% compared with 0.8% in the GA group, P < .92). This may be explained by the observation that 2 of the 4 patients who had an MI in the LA group had significant cardiac comorbidity and would not have been offered CEA under GA. Additionally, perioperative hypertension is more common in the LA group 14 ; this may improve cerebral perfusion but simultaneously increases myocardial oxygen demand, thus provoking ischemia. Conversely, general anesthetics are more likely to cause hypotensive episodes that may significantly reduce myocardial perfusion and likewise cause ischemia. 15
This study has demonstrated a trend toward early stroke-free survival in patients who undergo CEA under LA. The differences in our measured outcome variables between LA and GA do not reach statistical significance. In spite of the limitations of this study, the results mirror those of the GALA randomized controlled trial. Some of the limitations highlighted in the GALA trial, such as Statin use, also apply to this study. 8
With no firm consensus on anesthetic technique, choice should be guided by local expertise and complication rates. With reflection, best practice may dictate that a standard technique is selected as suggested above and this remains the default position for individual practice.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.