
Abstract
The pathophysiology of pregnancy-induced hypertension and preeclampsia may involve abnormalities in placentation and the Fas/Fas ligand system. Hypothesizing abnormal plasma Fas and Fas ligand in pregnancy-induced hypertension, we recruited 20 hypertensive pregnant women at mean week 15 and 29 at week 30: 18 were studied at both time points. Control groups were 20 normotensive pregnant women at week 20, 29 women at week 27, and 50 nonpregnant women. sFas and sFas ligand (sFasL) were measured by enzyme-linked immunosorbent assay (ELISA). The hypertensive women had lower sFasL at both stages of their pregnancy (P < .05). There were no differences in sFas. In 18 hypertensive pregnant women, sFasL fell from week 15 to week 29 (P < .03). We conclude that sFas and sFasL is unchanged in normal pregnancy. Hypertension in pregnancy is characterized by low sFasL, and levels fall from weeks 15 to 29. This may reflect differences in placentation in the differing physiological and pathological states.
Introduction
Hypertension, a common medical complication in pregnancy, is part of a spectrum of conditions including chronic (preexisting) hypertension, preeclampsia, and eclampsia, which have significant implications on maternal and perinatal morbidity and mortality.1,2 Abnormalities in placentation may be the primary pathology responsible for the development of preeclampsia and its effects, and a possible cause for this may be irregularities in the crucial relationship between Fas (a member of the tumor necrosis factor receptor superfamily [TNFRSF]) and its ligand (ie, FasL), which in part regulate apoptosis,3–5 on key endothelial cells. Fas (CD95, but also known as Apo-1 and TNFRSF6) is a 45-kDa type I membrane receptor containing an 80-amino acid intracellular “death” domain in the intracytoplasmic tail. Engagement of membrane-bound Fas by its ligand (CD95L, also known as TNFSF6), a 36- to 40--kDa type II membrane TNFSF member) triggers apoptosis by inducing the caspase series of enzymes. Current thought suggests apoptosis has a central role in the villous trophoblast turnover, as controlled apoptosis, mediated mainly through Fas-FasL signaling, may be a defence mechanism against rejection of the fetal allograft by maternal immune system. 6
The Fas/FasL system may also be important in small-for-gestational age babies, although this is controversial.7–9 Nevertheless, there is evidence of changes in Fas and FasL that imply a role in preeclampsia.9–11 Furthermore, Fas and FasL may also be involved in the hypertension of pregnancy as Koenig and Chegini reported differential expression of Fas and FasL in fetal membranes, decidua, and placentas from gestations with hypertension than in normal controls. 12 Matrix metalloproteinases are able to cleave FasL, leading to a soluble form measurable in plasma, as reported in preeclampsia, pregnancy, and in the syndrome of hemolysis, elevated liver enzymes, and low platelets.10,13–15 However, there are no reports of plasma Fas and FasL in the hypertension of pregnancy or any of the effects of parity.
We hypothesized altered levels of Fas and FasL in the plasma of women whose pregnancy is complicated by hypertension compared with women with normotensive pregnancies and normotensive nonpregnant women, that levels would change as pregnancy proceeds. We tested our hypotheses on a cross-sectional study of women attending a specialist antenatal hypertension clinic, a standard antenatal clinic, and in healthy nonpregnant women.
Methods
The index study group were pregnant women with raised blood pressure (≥140/90 mm Hg) or normal blood pressure (<140/90 mm Hg) and on antihypertensive drugs. They were recruited from those attending an antenatal hypertension clinic, a dedicated service for the management of hypertensive disorders in pregnancy. Twenty women were recruited early in their pregnancy (around week 14), and 29 later in their pregnancy, at approximately week 28. Eighteen women were studied at both stages. A parallel group of 20 pregnant women with normal blood pressures were recruited at week 14, and another 29 women were recruited at around week 28. The study was completed by the recruitment of 50 women who were not pregnant. The normotensive pregnant women were recruited from the routine antenatal clinic, and nonpregnant controls were recruited from among staff and relatives of patients attending the clinics. Recruitment was made without referral to parity. Exclusion criteria for all women were evidence of vascular, metabolic, neoplastic, diabetic, or inflammatory disease on careful history. Women with preeclampsia and eclampsia and those with significant coexisting medical conditions, such as heart disease, renal disease, and connective tissue disease were excluded. The study was approved by the Sandwell and West Birmingham Local Research Ethics Committee, and written informed consent was obtained from each participant.
Collection of Blood Samples and Laboratory Methods
Blood samples were collected using a 21-gauge needle directly into Vacutainer tubes (Becton Dickinson, Oxford, UK) containing sodium citrate. Blood samples were centrifuged within 30 minutes from collection at 1,500g for 20 minutes at 4°C. The resultant supernatant plasma was collected and stored at –70°C until batch processing by ELISA for Fas and sFas ligand (sFasL; R&D Systems, Abingdon, UK). Lower limited of detection were 100 pg/mL for sFas and 20 pg/mL for sFasL. The intra and interassay coefficient of variation was <5% and <10%, respectively, for all assays.
Power calculations and statistical analyses
There are no reports of sFas or sFasL in the hypertension of pregnancy on which to base a power calculation. However, as other sample sizes in other sFas/sFasL cross-sectional studies range from n = 20 to n = 30 per group,12 –15 , we recruited to this target for the pregnant groups, and to approximately twice as many nonpregnant women. Following a test of statistical normality, data were expressed as mean (standard deviation, SD) or median (interquartile range, IQR), as appropriate. Noncategorical data distributed normally were analyzed by one-way analysis of variance (ANOVA), nonparametric data were analyzed by Kruskal Wallis. Intergroup differences were sought by Tukey post hoc test. Correlations were sought by Spearman’s rank method. Categorical data (parity) were analysed by the chi-square test, paired data (18 hypertensive women at week 20 and again at week 29) by paired t test or Wilcoxon test. A 2-tailed P < .05 was considered as significant.
Results
Clinical, demographic, and sFas/sFasL data of the participants are presented in Table 1 . The participant groups and controls were matched for age but not parity, which increased from the nonpregnant women (median no children), to the normotensive women (median one child), to the hypertensive women (median 2 children). At both early and late stages of pregnancy, systolic blood pressure (SBP) was significantly higher in the hypertensive pregnant group compared with the normal pregnant and nonpregnant women. Diastolic blood pressure was (DBP) was lower in the pregnant women than in the nonpregnant women and was higher in hypertensive pregnant women than both other groups.
Clinical, Demographic, and sFas/FasL Data a
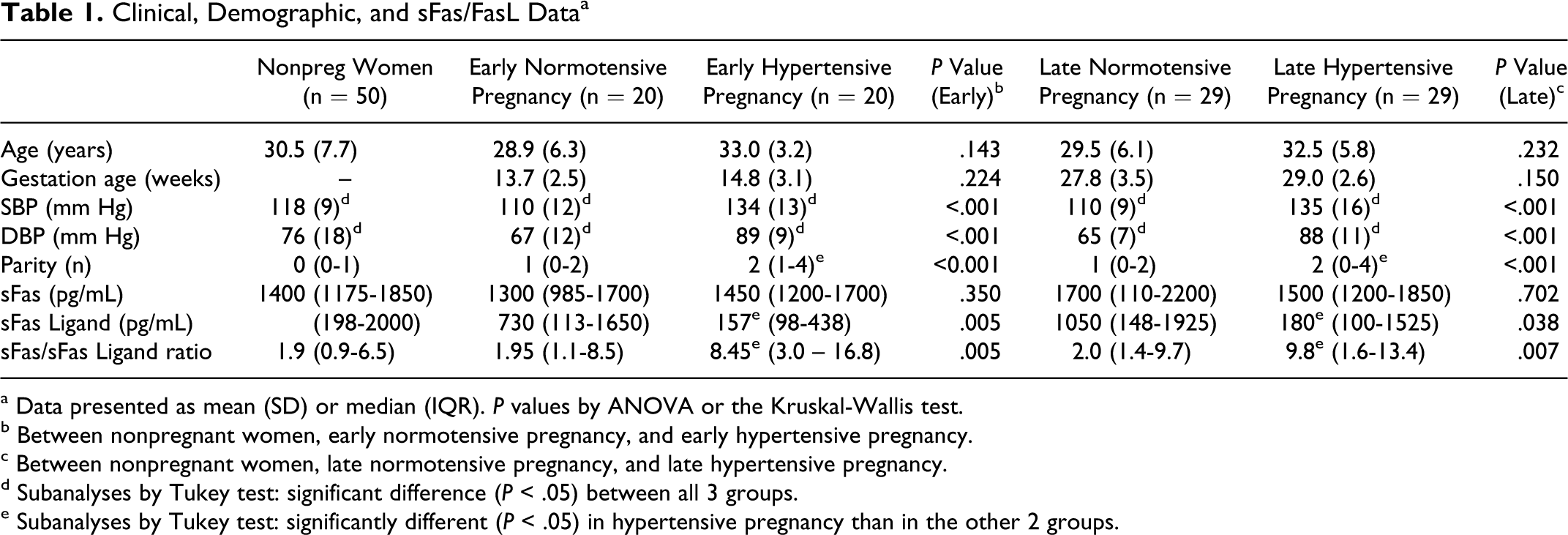
a Data presented as mean (SD) or median (IQR). P values by ANOVA or the Kruskal-Wallis test.
b Between nonpregnant women, early normotensive pregnancy, and early hypertensive pregnancy.
c Between nonpregnant women, late normotensive pregnancy, and late hypertensive pregnancy.
d Subanalyses by Tukey test: significant difference (P < .05) between all 3 groups.
e Subanalyses by Tukey test: significantly different (P < .05) in hypertensive pregnancy than in the other 2 groups.
There were no differences in sFas between the groups at either time point (early or late pregnancy). sFasL was lower, and the sFas/sFasL ratio was higher, in hypertensive pregnancy at both time points compared to both other groups. In the early stages of pregnancy (approximately week 14), sFasL was unrelated to parity (P = .058). In the late stages of pregnancy (approximately week 28), sFasL was also unrelated to parity (P = .065).
sFas and sFasL were measured in 18 women both early and late in their pregnancy. There was no difference in levels of sFas at the 2 time points: 1550 (1200-1750) pg/mL at week 20 and 1550 (1175-1825) pg/mL at week 29 (P = .955). However, sFasL fell from 130 (85-213) pg/mL at week 20 to 125 (98-735) pg/mL at week 29 (P = .028). The sFas/sFasL ratio also fell from 10.3 (6.0-18.1) to 9.9 (4.1-14.1; P = .021). sFas, sFasL, and their ratio failed to correlate significantly with gestational age, maternal age, SBP, or DBP at either time point in the pregnant women, or in the pregnant women. sFas correlated with sFasL in all groups at all time points (r = .45-0.74, P = .002-<.001) except in the hypertensive women early in their pregnancy (r = .39, P = .092).
Discussion
We examined the role of sFas and sFasL in normal pregnancy and in the hypertension of pregnancy, focusing on both early and late stages. We found no difference in sFas, sFasL, or their ratio in normal pregnancy compared with no pregnancy, and no change over the duration of the pregnancy, thus failing to confirm others who found low sFas in similar numbers of women with a normal pregnancy. 14 Harirah et al found serum levels of sFas, but not sFasL, to be significantly higher in women with the syndrome of hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome than healthy gravidas. 15 Although Koenig and Chegini observed greater expression of Fas and FasL in amnion and decidual tissue from hypertensive pregnancy gestations than in normal control pregnancies, they did not report plasma levels. 16 We complement their data by reporting low sFasL and high sFas/sFasL ratio in hypertensive pregnancy compared to nonpregnancy and normal pregnancy at both early and late stages of pregnancy. However, Kuntz et al 10 also found higher sFasL in preeclamptic pregnancy compared with control gestations but no difference in sFas. Thus, although comparison between research reports may be flawed, we and Kuntz et al both found measurement of sFas to be unhelpful. Our finding of low sFasL in hypertensive pregnancy is the reverse of their finding of high levels in preeclamptic pregnancy.
The relationship between Fas and FasL within the pregnant uterus may be important in minimizing the maternal allogeneic response,3 –6,17–19 and failure of this system may be important in preeclampsia and other conditions.11,20,21 This has lead to interest in potential roles for the measurement of these molecules in maternal blood as indicators of actual or potential complication such as intrauterine growth retardation.7 –10,14,15,22 Although a recent report failed to find a role for sFas and sFasL in intrauterine growth retardation, 23 these molecules may be important in the neonatal period. 24 Although limited by its cross-sectional design and relatively small sample size (which is comparable to, or exceeds, similar studies,10,14–16,22–24 the participant groups were matched with respect to age. An additional caveat is the marked difference in parity.
We therefore conclude that in normal pregnancy there is no change in sFas or sFasL. However, we found that sFas is low in hypertensive pregnancy, although this may be an effect of the increased parity in this group. Although sFasL and the sFas/sFasL ratio fell in 18 hypertensive women between weeks 20 and 29, this “mathematical” decrease of 4% is unlikely to have clinical value. Further studies, longitudinal in design and involving larger sample sizes, are required to clearly establish a possible etiological association between an imbalance in sFas and sFasL and the development of complications and adverse outcomes in hypertension in pregnancy.
Footnotes
Acknowledgments
We acknowledge the assistance of the Sandwell and West Birmingham Hospitals NHS Trust Research & Development programme for the Haemostasis Thrombosis and Vascular Biology Unit. We also thank Mr Balu Balakrishnan for help with laboratory work.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.