
Abstract
The Coronary Artery Disease in gENeral practiCE (CADENCE) study examined chronic stable angina (CSA). This further analysis examined atherosclerotic risk factors, symptomatic status, clinical management, and quality of life in patients with CSA with and without peripheral arterial disease (PAD). The CADENCE study involved 207 Australian general practitioners (GPs) recruiting 10 to 15 consecutively presenting patients with CSA (n = 2031). General practitioners completed a 2-page case report form, detailing demographic data, cardiovascular status, risk factors, and GP perception of control. Patients completed the Seattle Angina Questionnaire. Patients with coexisting CSA and PAD (17%) were more likely to be older and had more comorbidities than patients with CSA without coexisting PAD. Patients with peripheral arterial disease had a longer history of heart disease and were more likely to experience angina on a weekly basis. Patients with peripheral arterial disease had poorer quality-of-life indices.
Introduction
Cardiovascular disease has a major impact on most developed countries, not only by its impact on mortality but also by its associated morbidity. Atherosclerosis is a fundamental pathological process that underlies many cardiovascular disorders including coronary heart disease (CHD), peripheral artery disease (PAD), and cerebrovascular disease. Accordingly, it is not uncommon for patients to have more than 1 of these vascular disorders. Although a number of studies have investigated this relationship in hospitalized patients with CHD and PAD, 1 few studies report the relationship in stable patients with CHD attending primary care practices.2,3 Moreover, few studies have focused on the clinical implications of having both CHD and PAD.
The recently published Coronary Artery Disease in gENeral practiCE (CADENCE) study examined a large cohort of patients with chronic stable angina (CSA) 4 in relation to their symptomatic status and quality of life. This study demonstrated that approximately one third of patients with CSA attending general practice clinics experienced angina at least once a week and these patients were significantly disabled compared with those who experienced angina less frequently. Importantly, the presence of PAD in the patients with CSA was an independent predictor of disabling weekly angina.
This investigation further examines the relationship between these cardiovascular disorders by comparing patients with CSA recruited into the CADENCE study either with or without coexisting PAD. Specifically, we aimed to identify differences in (a) atherosclerotic risk factors, (b) symptomatic status, (c) clinical management strategies, and (d) impact on quality of life between those with and without PAD, all of whom had underlying CSA.
Methods
The CADENCE study was a cluster-stratified cross-sectional survey of 2031 consecutive patients attending general practitioners (GPs) throughout Australia, with a clinical diagnosis of CSA. The study was registered with the ANZ Clinical Trials Registry (CCTRN 1260 8000 347369) and approved by the Royal Australian College of General Practitioners National Research and Evaluation Ethics Committee. Detailed methods have been previously published 4 and are briefly summarized below.
Recruitment Strategy
Expressions of interest for study participation were sought from all registered GPs in Australia. Of those interested, participation was restricted on the basis of practice location to ensure a representative sample. Practices were selected based upon urban/rural location with proportional representation from each state/territory.
From October 2006 until March 2007, 207 actively participating GPs, prospectively recruited 10 to 15 patients with a “clinical diagnosis of angina.” Angina was defined from clinical history and chart review as substernal chest discomfort (typically “squeezing,” “tightness,” or “heaviness”) usually persisting for a few minutes. Patients were recruited irrespective of the purpose of their visit to the GPs, and all provided written informed consent. For the purpose of this study, PAD was defined from clinical history and chart review by 1 or more of the following: (1) clinical diagnosis by a medical practitioner of leg claudication, (2) imaging studies with a stenosis >50% in the peripheral vasculature, or, (3) a history of peripheral vascular intervention either surgical or radiological. Thus, the study was limited to symptomatic patients with PAD, and the ankle-brachial index was not recorded. Exclusion criteria included being unable to give consent or complete the Seattle Angina Questionnaire (SAQ).
Data Collection and Analysis
General practitioners completed a 2-page case report detailing demographic data, PAD, other cardiovascular history, cardiovascular risk factors, and current medications. General practitioners were asked to assess angina symptoms using the Canadian Cardiovascular Society Classification (CCSC). 5 They were also asked whether in their opinion, their patients’ angina was “optimally controlled.”
Independently, patients completed the SAQ, a validated disease-specific quality-of-life instrument for CHD. 6 The SAQ independently quantifies clinically important domains: angina frequency—a lower score indicates more frequent angina symptoms; physical limitation—a lower score indicates greater physical limitation due to angina symptoms; angina stability—scores above 50 indicate progressive levels of improvement and scores below 50 indicate decline in angina symptoms over the preceding 4 weeks; quality of life—a lower score indicates a reduced quality of life; and treatment satisfaction—a lower score indicates reduced satisfaction with angina management.
Statistical analysis used SAS statistics software (version 9.1; SAS Institute, Cary, North Carolina). Pairwise comparisons of patients with CSA between those with/without PAD were undertaken using a general linear model with PAD as a categorical predictor variable and the outcome variable being either continuous or binary. The difference between means for patients with/without PAD could be estimated and a 2-tailed P value determined (using a t test) using the appropriate variance estimate accounting for the survey design. Patients with PAD were older than those without (74 ± 10 vs 70 ± 11 years; P < .0001) and thus age-adjusted analyses were undertaken for other variables.
Results
Study Population
Of the 2031 recruited patients with stable angina, data concerning their PAD status were available in 1533 patients. Of these, 265 (17%) had evidence of PAD compared with the remaining 1268 (83%) who did not. Those with PAD were significantly older (74 ± 10 vs 70 ± 11years; P < .001), but there was no gender difference (males 66% vs 65%; P > .05) between the groups. Considering the difference in age between the groups, all subsequent data analysis was undertaken using age-adjusted comparisons.
Clinical Features
In this CSA population, those with coexisting PAD were more likely to have several risk factors and related disorders (Table 1). These included a history of smoking (70% vs 56%; P < .001), hypertension (81% vs 70%; P < .001), diabetes (48% vs 31%; P < .001), heart failure (36% vs 20%; P < .001), and obstructive airways disease (34% vs 19%; P < .001). However, there was no difference between those with or without PAD in the frequency of hypercholesterolemia, obesity, and alcohol consumption. The incidence of hypercholesterolemia was 83% in patients with CSA only and 86% in patients with CSA and PAD, and a similar proportion in each cohort were treated with a statin (83% in both groups).
Age-Adjusted Comparisons for Clinical Features of CSA Patients With and Without PAD
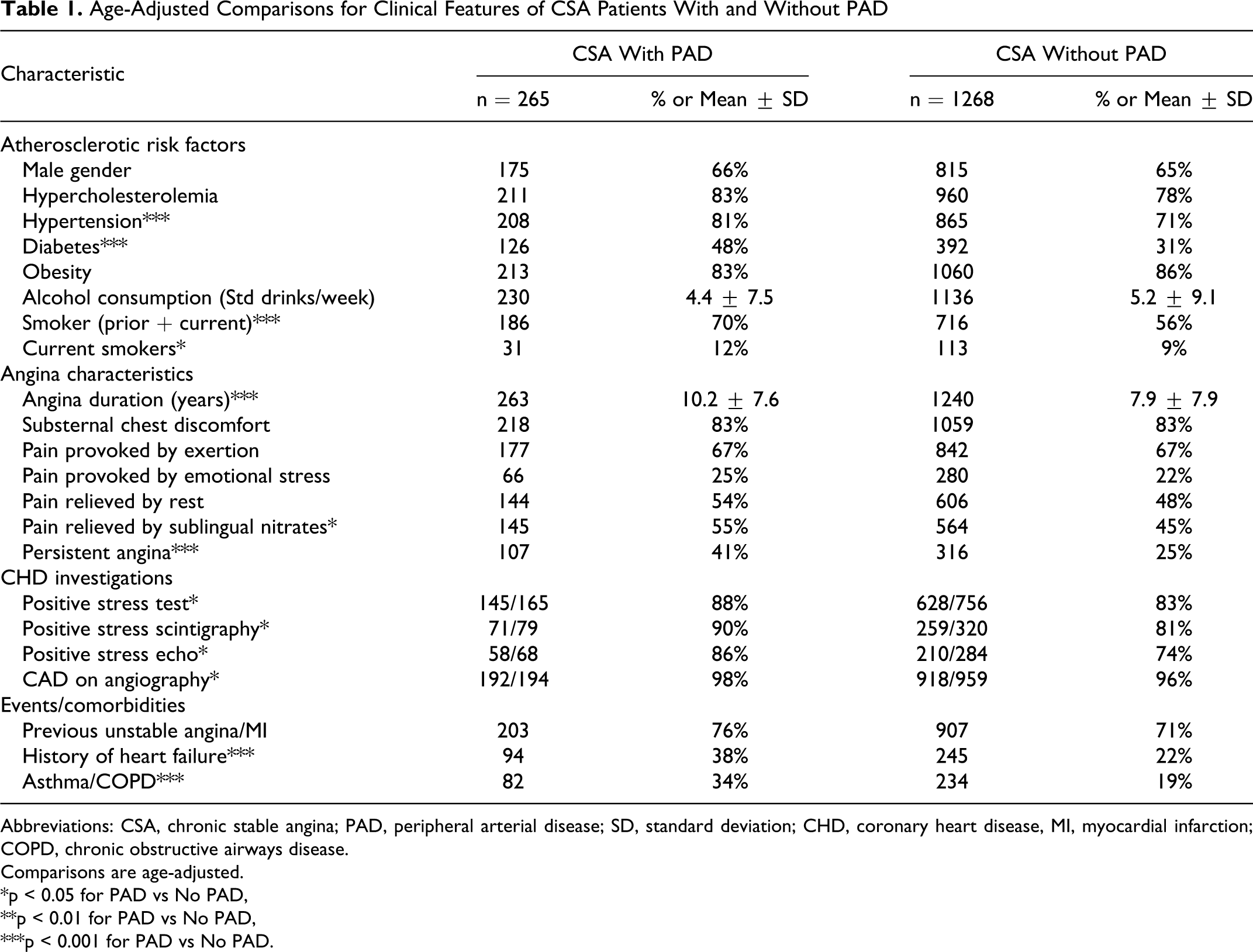
Abbreviations: CSA, chronic stable angina; PAD, peripheral arterial disease; SD, standard deviation; CHD, coronary heart disease, MI, myocardial infarction; COPD, chronic obstructive airways disease.
Comparisons are age-adjusted.
*p < 0.05 for PAD vs No PAD,
**p < 0.01 for PAD vs No PAD,
***p < 0.001 for PAD vs No PAD.
Patients with coexisting CSA and PAD had a longer history of CHD and were more likely to experience angina on at least a weekly basis compared with those without coexisting PAD (Table 1). Interestingly, those with both CSA and PAD reported their angina to be responsive to sublingual nitrates compared with those who only had CSA (Table 1). Furthermore, patients with both CSA and PAD were more likely to have objective evidence of either myocardial ischemia (stress testing, scintigraphy, or echocardiography) or CHD on angiography (Table 1).
Clinical Management
Patients with both CSA and PAD were more likely to have been reviewed by a cardiologist than those with only CSA (94% vs 89%, respectively; P < .05). Despite having at least 2 documented atherosclerotic conditions, of those with both CSA and PAD, only 80% were prescribed antiplatelet agents and 83% statin therapy. This was similar to those who had CSA alone (Table 2 ).
Age-Adjusted Comparisons for the Clinical Management of CSA Patients With and Without PAD
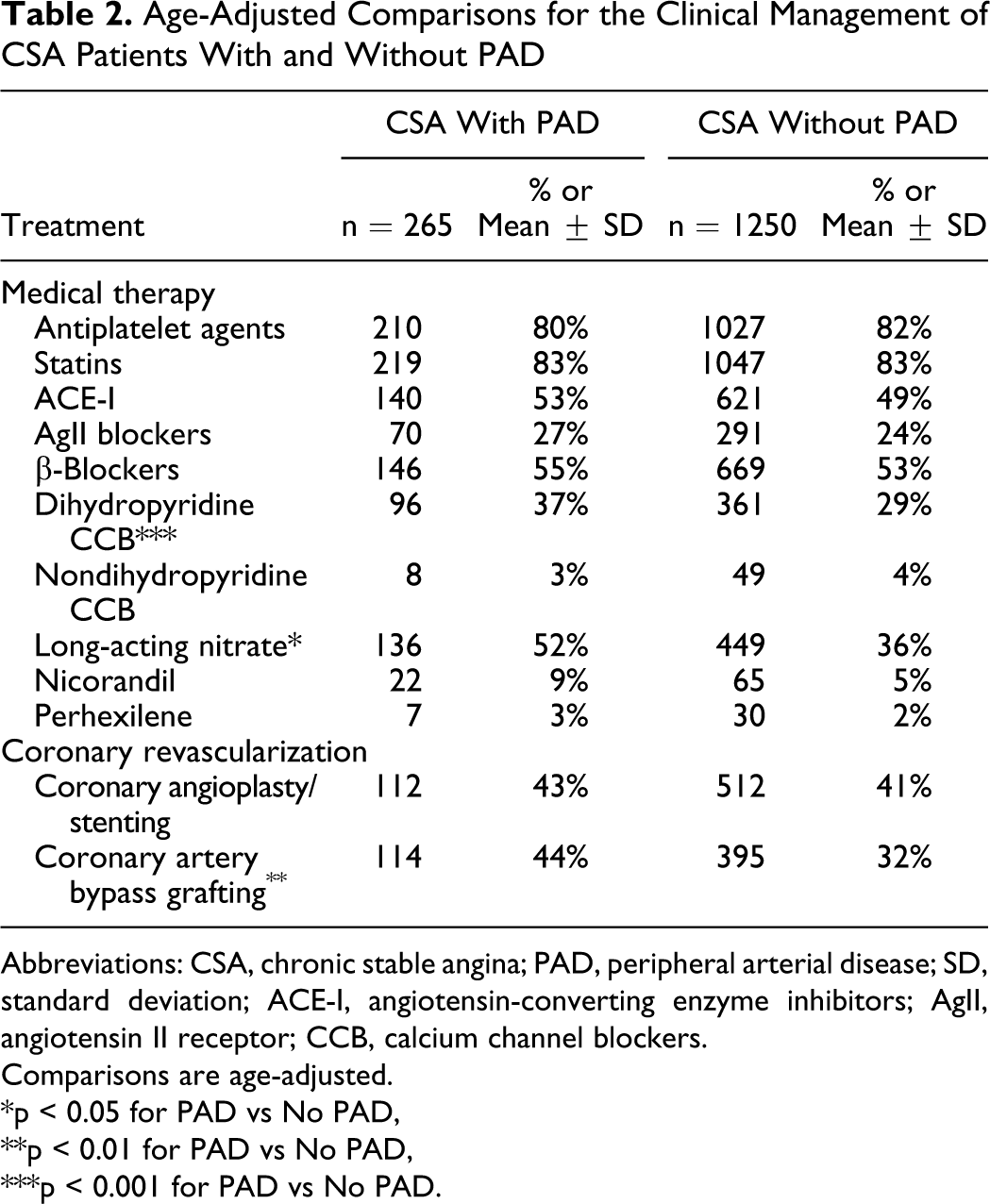
Abbreviations: CSA, chronic stable angina; PAD, peripheral arterial disease; SD, standard deviation; ACE-I, angiotensin-converting enzyme inhibitors; AgII, angiotensin II receptor; CCB, calcium channel blockers.
Comparisons are age-adjusted.
*p < 0.05 for PAD vs No PAD,
**p < 0.01 for PAD vs No PAD,
***p < 0.001 for PAD vs No PAD.
Those patients with combined CSA and PAD were more likely to have undergone coronary artery bypass grafting and be prescribed long-acting nitrates compared with those with CSA alone (Table 2). Although there were no differences in the use of angiotensin-converting enzyme inhibitors (ACE inhibitors), angiotensin II receptor blockers (Ag II blockers), β-blockers, or verapamil/diltiazem, patients with CSA and PAD were more likely to be prescribed dihydropryridine calcium channel blockers (Table 2). The increased use of the latter agent may reflect the increased angina symptoms in this group or their increased prevalence to hypertension.
Patient Health Status
Patient assessed health status was determined by the SAQ and the findings are shown in Figure 1. Patients with CSA and PAD (compared with those without PAD, respectively) had lower SAQ scores in physical limitation (57 ± 27 vs 73 ± 26; P < .001), angina frequency (77 ± 26 vs 86 ± 21; P < .001), angina stability (59 ± 27 vs 63 ± 25; P < .05), and quality of life (64 ± 26 vs 72 ± 23; P < .001). Also the GPs perceived the control of angina were less optimal in those with both CSA and PAD (71% vs 82%; P < .001). Consistent with lower SAQ scores, there was a significantly lower proportion of patients with coexisting CSA and PAD in the CCSC class 1 group (43% vs 64%; P < .001; Figure 2).
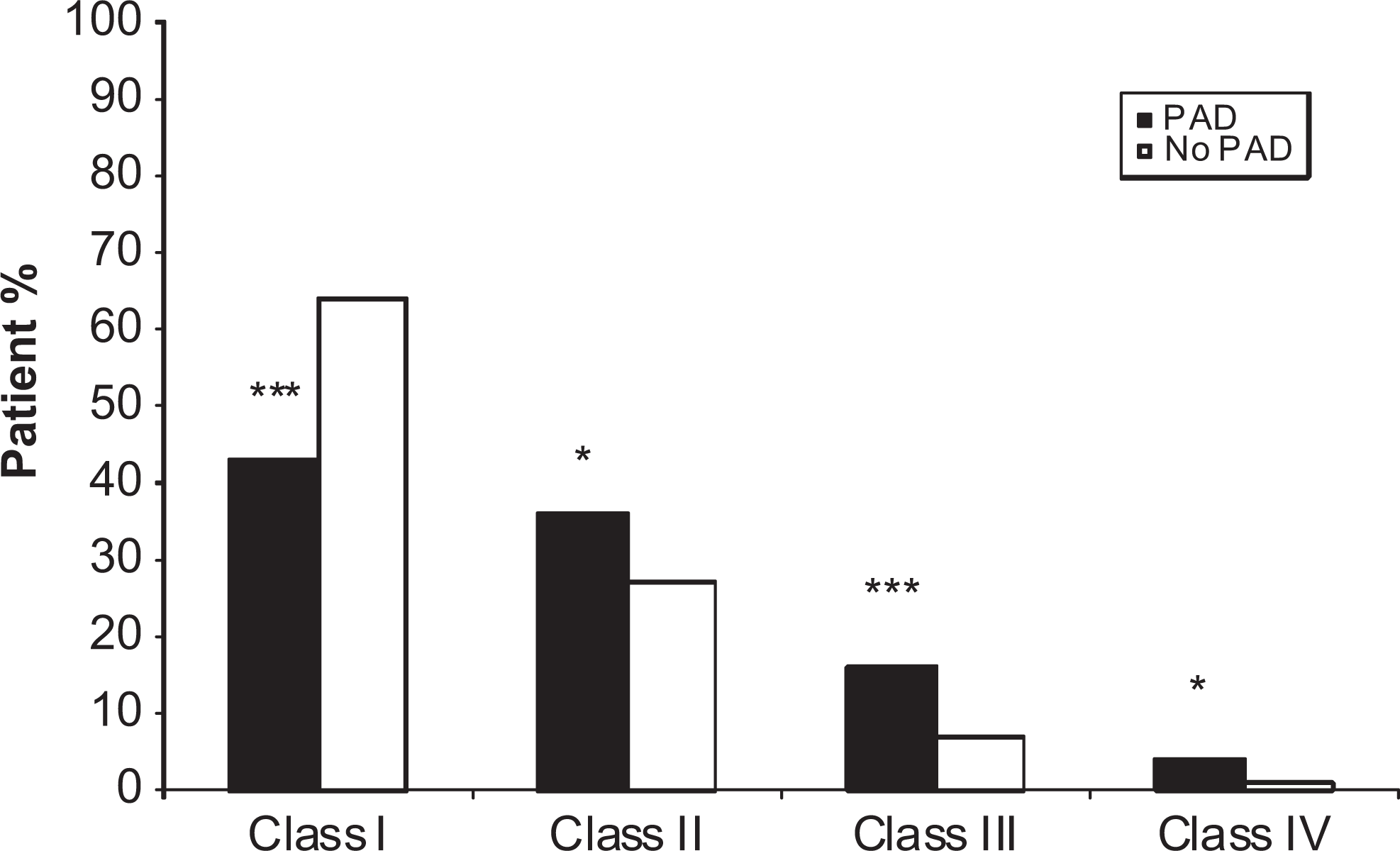
General practitioner-assessed Canadian Cardiovascular Society Class for Chronic Stable Angina Patients with and without coexisting peripheral artery disease (PAD). **p < 0.01 for PAD vs No PAD, ***p < 0.001 for PAD vs No PAD. Comparisons are age-adjusted.
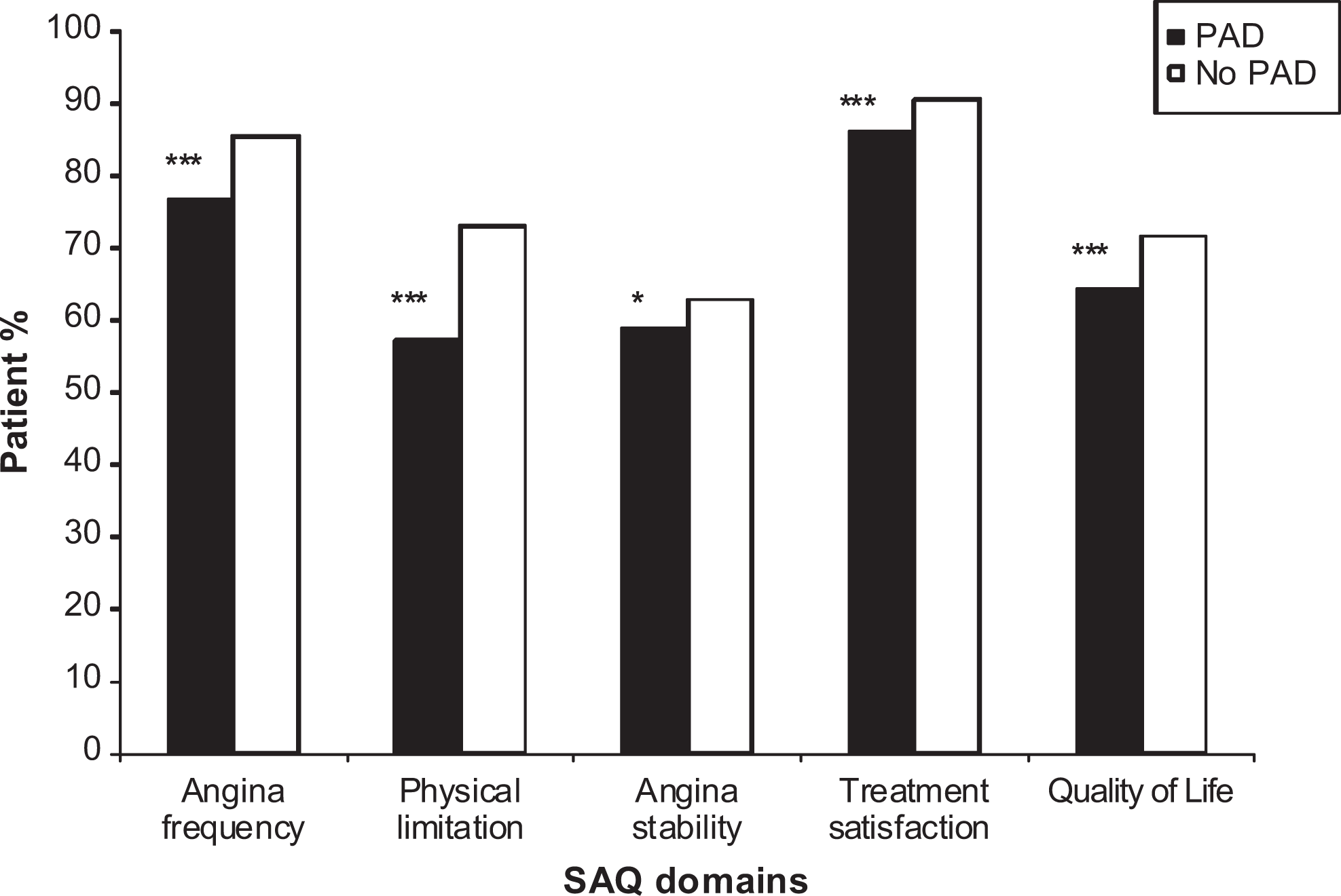
Patient-derived Seattle Angina Questionnaire Scores (SAQ) for chronic stable angina patients with and without co-existing peripheral artery disease (PAD).
Discussion
This study recruited a large representative cohort of Australian patients with CSA attending primary care clinics. The study compared the clinical characteristics and health outcomes of those with and without coexisting PAD. We observed differences in age, risk factors, CHD manifestations/management, and the health outcomes in patients with coexisting PAD. Patients with CSA and coexisting PAD were older but even after adjustment for age, they were more likely to have a history of smoking, hypertension, diabetes, chronic obstructive pulmonary disease, and heart failure. Furthermore, they more often experienced angina at least once a week and thus not surprisingly, were more likely to have been seen by a cardiologist, undergo cardiac investigations for CHD, and have surgical coronary revascularization. However, there were no differences between groups in the medications prescribed except for long-acting nitrates and dihydropyridine calcium channel blockers, which may reflect the incremental therapy required for the more persistent angina among these patients. Considering the more symptomatic CHD and coexisting conditions (PAD, COPD, and heart failure), it is not surprising that the patients with CSA with PAD have greater physical limitations and a poorer quality of life as a result of their disease. These findings are consistent with those observed in other studies1–3 and have important implications in the management of these patients.
Prevalence of Coexisting Coronary Heart Disease and Peripheral Artery Disease
Coronary heart disease and PAD share a common underlying pathophysiology, namely atherosclerosis. Thus, not unexpectedly they may coexist, with patients having common risk factors and a high risk of cardiac events. The reported prevalence of combined CHD and PAD varies with the recruitment strategy and diagnosis of these disease entities. Similar to the present study, Jeger et al surveyed patients with CHD and found that 7% had coexisting PAD by patient self-report. 1 Dieter et al also sampled patients with CHD but reported a 40% prevalence of coexisting PAD when the diagnosis was made by assessment of ankle-brachial index (ABI); however, only half of these patients had previously diagnosed PAD. 7
Another approach in assessing the occurrence of coexisting CHD and PAD is to evaluate the prevalence of CHD among a PAD population. Dormandy et al examined inpatients with critical leg ischemia and found <50% had CHD when identified by clinical history and electrocardiograph (ECG), whereas over 90% were identified when coronary angiography was used. 8 The PARTNERS study screened for the presence of PAD in a primary care setting on the basis of history and ABI. 3 This multicenter study identified 1865 patients with PAD of whom 56% had other cardiovascular diseases (half of whom had angina). The international REACH registry recruited almost 68 000 patients with atherothrombotic disease of whom 8273 had evidence of symptomatic PAD; among these patients with PAD, 52% had coexisting CHD. 9 Hence, in a patient population with PAD approximately a half can be expected to have CHD, whereas <10% of a CHD population will have symptomatic PAD.
Clinical Features in Patients With CHD and PAD
Although CHD and PAD share common atherosclerotic risk factors, in this study hypertension, diabetes, and a history of cigarette smoking were more prevalent among those with both conditions, whereas there was no difference between those with/without PAD in the incidence of hypercholesterolemia (Table 1). The increased prevalence of hypertension, diabetes, and smoking could reflect the older age of patients with CSA and coexisting PAD; however, age-adjusted analyses demonstrate a persistence of this observation. Diabetes and smoking are considered the most prominent risk factors for PAD. 10 Our findings are similar to a smaller study of cardiac inpatients that reported an increased prevalence of diabetes and hypertension in patients with coexisting PAD. 11 Furthermore, in the REACH study, patients with PAD were more likely to be current smokers and diabetic but less likely to have hypercholesterolemia compared with patients who had CHD.
Health Outcomes in Patients With CHD and PAD
Patients with PAD have a higher risk of cardiovascular events than those with CHD. For example, in the 3-year follow-up of the REACH study, 14.8% of patients with PAD had experienced a vascular event (myocardial infarct/stroke or vascular death) as compared with 11.6% of patients with CHD. 12 Furthermore, in the 4-year follow-up study of this registry, the presence of symptomatic polyvascular atherothrombotic disease was an independent predictor of a vascular event. 9
In contrast to the many cardiovascular end point studies, few have addressed the impact of polyvascular disease involvement on patient’s quality of life. In this study, patients with CSA and PAD have greater limitations in their physical activities and a poorer quality of life than those without PAD. Similarly, the Edinburgh Artery Study demonstrated that patients with both claudication and angina had lower physical function than healthy controls. 2 In the PARTNERS Study, 3 patients with polyvascular involvement had poorer physical summary scores in the Short Form-36 questionnaire compared with those who had PAD alone.
Cardioprotective Therapies
Over 80% of the CSA patient cohort in this study were receiving antiplatelet agents or statin therapy, irrespective of whether they had coexisting PAD (Table 2). Considering the important prognostic benefits of these agents in patients with atherosclerotic disease, the use of these agents requires closer scrutiny. By comparison, in the REACH registry study (which enrolled patients with CHD and/or PAD) 12 antiplatelet agents were administered to 92% of patients and statins in 76%. The findings of both CADENCE and REACH suggest that these cardioprotective therapies require closer scrutiny.
Limitations
The population study group included patients with CSA with PAD rather than primarily PAD. Ankle-brachial index is more sensitive at detecting asymptomatic PAD. This is important since asymptomatic disease predicts future vascular events and indicates the need for risk factor modification. However, in this study, PAD was not defined by an objective test such as ABI. Rather PAD and CSA were defined in terms of history and chart review. Patients with subclinical PAD could have been present in the CSA only group. However, neither of these factors should confound the results since the Edinburgh Artery Study found no difference in health-related quality-of-life scores between those with asymptomatic PAD and those with no PAD after adjustments for confounding variables. 2
Conclusions
Patients with PAD and coexisting CSA have greater comorbidity, more angina symptoms, and poorer quality of life than patients with single territory CSA without PAD. Secondary prevention strategies are suboptimal in a significant minority of all patients. The findings of CADENCE support recent statements from Trans-Atlantic Inter-Society Consensus (TASC) 13 and American College of Cardiology/American Heart Association (ACC/AHA) 14 and identify patients with PAD as an increased cardiovascular risk population.
Footnotes
Acknowledgments
Dr John Beltrame is supported by a National Heart Foundation of Australia Clinical Post doctoral Research Fellowship. Rosanna Tavella is a Queen Elizabeth Hospital Research Foundation Scholarship recipient. The authors acknowledge the support of the Royal Australian College of General Practitioners and the contribution of the 207 participating general practitioners in undertaking this study. Without their time and enthusiasm, this research would not have been possible. The study was conducted with the generous assistance of Servier Australia and could not have been completed without the meticulous work of Annie Solterbeck (Statistical Revelations, Melbourne).
Study design, data analysis, and the writing of this manuscript were primarily the responsibility of the University of Adelaide investigators, who had full access to all of the data and take responsibility for the integrity of the data and the accuracy of the data analysis. The University received a consultation fee for the expert opinion of their researchers. Dr Andrew Weekes and Claire Morgan are employed by Servier Australia as Head of Medical Department and Scientific Project Associate, respectively, and collaborated with the University of Adelaide Investigators in the study design and review of the submitted article.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CADENCE study was conducted as a collaborative investigation between the University of Adelaide and Servier Laboratories (Australia) Pty Ltd. It was unconditionally funded by Servier Laboratories (Australia) Pty Ltd.