
Abstract
This study aimed at evaluating the changes in platelet-activating factor (PAF) and its metabolic enzymes over a 6-week follow-up period in patients with newly diagnosed heart failure ([HF] n = 12) compared with age-, sex-, and BMI-matched apparently healthy volunteers (n = 10). The PAF, its key biosynthetic enzymes (lyso-PAF acetyltransferase [lyso-PAF-AT] and dithiothreitol [DTT]-insensitive CDP choline: 1-alkyl-2-acetyl-sn-glycerol cholinephosphotransferase [PAF-CPT]), and its catabolic isoenzymes (PAF-acetylhydrolase [PAF-AH] and lipoprotein-associated phospholipase A2 [Lp-PLA2]) were measured in serum and leukocytes of participants. At baseline, patients with HF had lower median activities of lyso-PAF-AT (P < .001) and PAF-CPT (P = .07) in parallel with PAF levels (P = .05) and higher activities of PAF-AH (P = .02) and Lp-PLA2 (P < .001) than controls. At follow-up, PAF-CPT and PAF levels marginally increased (P = .1), lyso-PAF-AT (P < .001) remained downregulated, while PAF-AH (P = .004) and Lp-PLA2 (P < .001) remained elevated compared with the controls. Newly diagnosed patients with HF under drug treatment have an affected profile of PAF biosynthetic enzymes and especially lyso-PAF-AT.
Keywords
Introduction
The incidence of heart failure (HF) has increased at alarming rates especially since acute myocardial infarction deaths have decreased. 1 Therefore, HF is a complex public health problem with poor long-term prognosis, the pathogenesis and progression of which among others are connected to inflammation. 2 In fact, leukocytes, platelets, endothelial cells, myocardium together with other sources seem to orchestrate the inflammatory response in patients with HF. 3,4 Interestingly, circulating inflammatory markers differentiate along with the severity and progression of the disease 4,5 and may be modulated by HF-targeted therapeutic schemes, 6 which implies that monitoring their levels may facilitate the decision making in clinical practice and improve prognosis.
Platelet-activating factor (PAF, 1-O-alkyl-2-acetyl-sn-glycero-3-phosphocholine), 7 is a potent inflammatory phospholipid mediator that participates in the initiation and progression of cardiovascular disease including atherosclerosis. 8 ,9 As suggested from in vitro and animal studies, PAF is produced by human heart and it is thought to be implicated in HF since it participates in apoptosis of cardiomyocytes, induces arrhythmias, causes a negative inotropic effect and participates in the development of myocardial ischemia–reperfusion injury, stimulates secretion of atrial natriuretic peptide in rat cardiomyocytes, and is involved in leukocyte recruitment. 8,10
The activities of PAF biosynthetic enzymes correlate with inflammatory and immunologic molecules in patients with HF, 11 suggesting their possible involvement in this syndrome. With respect to PAF metabolism, 2 biosynthetic pathways are responsible for PAF biosynthesis, namely remodeling and the de novo pathway. 12 The remodeling pathway is believed to produce PAF under inflammatory conditions. In particular, cytoplasmic phospholipase A2 converts ether phosphatidylcholine into lyso-PAF which is then leading to PAF formation by the action of acetyl-CoA:lyso-PAF acetyltransferases (lyso-PAF-AT, EC 2.3.1.67). 12,13 On the other hand, the de novo pathway is considered to be responsible for the constitutive production of PAF in tissues and blood. A key step in this route is the final one, in which PAF is produced by 1-O-alkyl-2-acetyl-glycerol through the action of a specific dithiothreitol-insensitive CDP choline:1-alkyl-2-acetyl-sn-glycerol cholinephosphotransferase (PAF-CPT, EC 2.7.8.16). 14 The catabolism of PAF includes the removal of acetyl chain (or short acyl chain) from sn-2 position and its conversion into lyso-PAF through a PAF-specific acetylhydrolase (PAF-AH, EC 3.1.1.47). 15 The plasma isoform of PAF-AH is known as lipoprotein-associated phospholipase A2 (Lp-PLA2) due to its attachment to lipoproteins and mainly LDL particles. 15 Moreover, it has been characterized as a prognostic biomarker for HF development 16 and is associated with mortality in patients with HF. 17
Despite the promising role of PAF and its enzymes in the inflammation hypothesis of HF pathogenesis, the data for humans are rather scarce. Moreover, there is no study investigating the perturbations of both PAF and its enzymes along with the progression of disease. Therefore, the aim of this work was to evaluate the changes in PAF and its metabolic enzymes over a 6-week period in patients with newly diagnosed HF and to compare them with the values of normal age- and BMI-matched volunteers.
Methods
Patients
A pilot study was conducted in consecutive male patients (n = 12) with newly diagnosed HF (within the first month) that were recruited from the First Cardiology Clinic of the School of Medicine of the University of Athens for participation in the current study and were followed up for 6 weeks. The criteria for the diagnosis of HF were those published from the European Society of Cardiology. 18 All patients with HF were adequately treated. The main medical treatment included aspirin, diuretics, statins, aldosterone antagonists, and ACE inhibitors. Ten (n = 10) age- and BMI-matched apparently healthy male participants were also enrolled. These volunteers were not medically treated.
All participants were informed about the aims and procedures of the study and gave written informed consent. The study was approved by the Medical Research Ethics Committee of our institution and was carried out in accordance with the Declaration of Helsinki of 1975 (revised in 1983).
Data concerning anthropometric parameters, smoking habits, physical activity, self-assessment of health status, and quality of life were collected. More details for the protocol of the study are provided elsewhere. 19 Hypertension was defined as systolic/diastolic blood pressure >140/90 mm Hg or use of antihypertensive medication. Hypercholesterolemia was defined as total serum cholesterol >5.2 mmol/L or the use of lipid-lowering agents. Diabetes mellitus was defined as a fasting blood glucose >6.9 mmol/L or the use of antidiabetic medication. Current smokers were defined as those who smoked at ≥1 cigarette/d. Participants who did not report any physical activities were defined as sedentary. Body mass index was calculated as weight (in kilogram) divided by standing height (in meter square). A modified version of the Minnesota Living with Heart Failure questionnaire was used for the self-assessment of health status and quality of life was based on a 10-unit scale. 20 Blood samples of patients with HF were obtained on the fourth day of admission.
Materials and Instrumentation
All reagents were of analytical grade and were supplied by Sigma Co (St Louis, Missouri). Analytical grade solvents, liquid chromatography grade solvents, and silicic acid 60 (0.2-0.5 mm), used for column chromatography, were supplied from Merck (Darmstadt, Germany). 1-O-Hexadecyl-2-O-acetyl-sn-glycerol was purchased from Biomol International (Plymouth Meeting, Pennsylvania). 1-O-Hexadecyl-2-[H 3 ] acetyl-sn-glycerol-3-phosphocholine ([H 3 ] PAF) with a specific activity of 10 Ci/mmol was obtained from New England Nuclear Co (Boston, Massachusetts). The purification of PAF by high-performance liquid chromatography (HPLC) was performed at room temperature on a HP HPLC Series 1100 liquid chromatography model (Hewlett Packard, Waldbronn, Germany) equipped with a Partisil 10SCX, WCS Analytical Column (Whatman 4.6 mm × 250 mm), a 100-μL loop Rheodyne (7725i) loop valve injector, a degasser G1322A, a quat gradient pump G1311A, and a HP UV spectrophotometer G1314A as a detection system. The spectrophotometer was connected to a Hewlett-Packard model HP-3395 integrator plotter. The PAF-induced platelet aggregation was measured in a Chrono-Log (Havertown, Pennsylvania) aggregometer (model 400-VS) coupled to a Chrono-Log recorder (Havertown) at 37°C with constant stirring at 1200 rpm. Centrifugations were performed in a refrigerated superspeed Avanti 30 centrifuge (Beckman Instruments, Fullerton, California). Homogenizations were conducted with the Bandelin Sonoplus sonicator GM 2070 (Germany). Radioactivity was measured with a liquid scintillation counter (1209 Rackbeta, Pharmacia, Wallac, Finland).
The PAF Determination in Blood
The PAF was isolated from blood, purified, and determined by a previously published method. 21 Briefly, 5 mL of whole blood were poured into plastic tubes containing 20 mL of absolute ethanol. Then, blood with ethanol was centrifuged at 500g for 20 minutes and the resulting supernatant (containing free-PAF) and pellet (containing bound-PAF) were extracted according to the Bligh-Dyer method. 22 Subsequently, 2 steps of purification followed: silicic acid column chromatography and HPLC. The PAF activity was then determined by measuring the aggregatory activity toward washed rabbit platelets, comparing the PAF-induced aggregation with those induced by known concentrations of synthetic PAF. 7
Determination of Lyso-PAF-AT and PAF-CPT Activities in Leukocyte Homogenates
The isolation of leukocyte homogenates was done as previously described. 11 For the determination of lyso-PAF-AT activity, leukocyte homogenates, containing 12 μg of total protein, were incubated with 4 nmol of lyso-PAF and 40 nmol of acetyl-CoA for 10 minutes at 37°C in a final volume of 200 μL of 50 mmol/L Tris/HCl buffer (pH 7.4) containing 0.25 mg/mL of bovine serum albumin (BSA). 23 The PAF-CPT was assayed at 37°C for 5 minutes in a final volume of 200 μL of a reaction mixture containing 20 μg of leukocyte homogenate protein, 100 mmol/L Tris-HCl (pH 8.0), 15 mmol/L dithiothreitol (DTT), 0.5 mmol/L EDTA, 20 mmol/L MgCl2, 1 mg/mL of BSA, 100 μmol/L of CDP choline, and 100 μmol/L of 1-O-hexadecyl-2-O-acetyl-sn-glycerol (added in the mixture in 2 μL of dimethyl sulfoxide). Both reactions were stopped by adding 1.11 mL of cold chloroform:methanol (2% acetic acid) and 0.3 mL of cold water in order to extract PAF by the acid Bligh-Dyer method. 24 The extracted PAF was further separated by thin-layer chromatography on silica gel G-coated plates with an elution system consisting of chloroform:methanol:acetic acid:water (100:57:16:8, v/v/v/v). The band corresponding to PAF (between lyso-phosphatidylcholine and phosphatidylcholine) was identified by cochromatographing lipid standards, which were visualized by exposure of the plates to iodine vapors. 24 The PAF fractions were scrapped off, extracted by the Bligh-Dyer method, and the amount of PAF was determined by the washed rabbit platelet aggregation assay. 7 All assays were performed in duplicate. Lyso-PAF-AT and PAF-CPT activities were expressed as specific activity in nmol/min per mg and pmol/min per mg, respectively.
Determination of PAF-AH Activity in Leukocyte Homogenates and Lp-PLA2
The PAF-
Measurement of Glycemic, Lipemic, Hematologic Parameters, and Inflammatory Markers
Serum total cholesterol, HDL-, LDL-cholesterol, and triglycerides were measured using an enzymatic method in a Technicon automatic analyzer RA-1000 (Dade Behring, Marburg, Germany). Blood glucose levels were measured with a Beckman Glucose Analyzer (Beckman Instruments). Hematological parameters were measured in Cell Dyn 1700 Hematology Analyzer (Abbott Diagnostics, IL, USA). The C-reactive protein (CRP) was assayed by immunonephelometry (Date-Behring Marburg GmbH, Marburg, Germany). Interleukin (IL)-6 was measured with a high-sensitivity enzyme-linked immunoassay (R&D Systems Europe Ltd, Abingdon, United Kingdom). The intra- and interassay coefficient of variation was <5% for CRP and <10% for IL-6. Tumor necrosis factor α (TNF-α) was also measured by an enzyme-linked immunosorbent assay (ELISA) method (Quantikine HS/human TNF-α immunoassay kit, R&D Systems, Inc, Minneapolis, Minnesota). The intra- and interassay variations were up to 5.7% and 7.8%, respectively. The quantitative measurement of soluble human sCD14 in serum was done by an immunoenzymometric assay sCD14 EASIA (Biosource Europe S.A., Belgium). The determination of sCD40L was done with a commercially available ELISA kit (Bender medsystems, Austria, Vienna).
Statistical Analysis
Variables are presented as median and interquartile range (25th-75th). Binary variables are presented as percentages. Comparisons between baseline and follow-up levels of the investigated parameters were tested with the nonparametric Wilcoxon signed test, because of the not-normal distributions of the variables. For the case of PAF values, a sign test was used to assess the differences between baseline and follow-up since values were not symmetrically distributed around the mean. Differences at baseline and at follow-up between patients with HF and the apparently healthy volunteers were assessed with the nonparametric Mann-Whitney test. The level of statistical significance was set at 5%. The Statistical Package for the Social Sciences (SPSS 18.0 for Windows, Chicago, Illinois) was used for all the analyses.
Results
The basic clinical, biochemical, and anthropometric characteristics of HF volunteers and apparently healthy volunteers are listed in Table 1. The patients with HF did not differ from healthy volunteers in terms of age, sex, smoking habits, BMI, blood pressure, and platelet count but exhibited higher concentrations of glucose, CRP, and white blood cell levels. The volunteers had higher lipid levels than patients with HF. The majority of patients with HF had ischemic heart disease, followed a sedentary life, and did not have cachexia (data not shown). The patients with HF self-rated their general health status lower than healthy volunteers, which was expected, given that patients were hospitalized at the time of evaluation.
Basic Clinical and Anthropometric Characteristics of Patients With Heart Failure and Apparently Healthy Volunteers.a
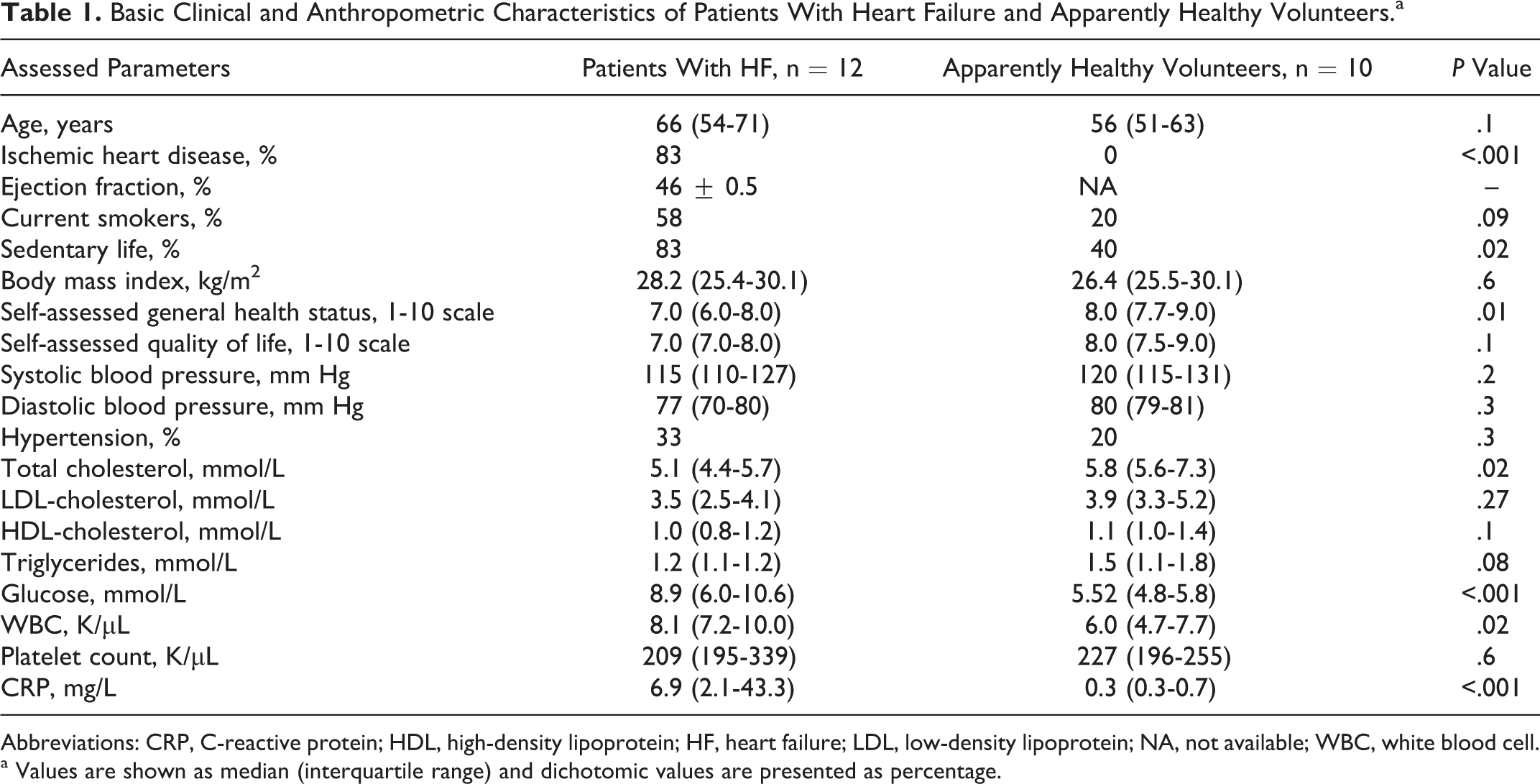
Abbreviations: CRP, C-reactive protein; HDL, high-density lipoprotein; HF, heart failure; LDL, low-density lipoprotein; NA, not available; WBC, white blood cell.
a Values are shown as median (interquartile range) and dichotomic values are presented as percentage.
In Table 2 changes in various inflammatory, immunologic, and biochemical markers are shown in patient with HF between the baseline and 6 weeks after the initial diagnosis. Glucose levels were decreased, whereas triglycerides and HDL-cholesterol were increased. A significant reduction in IL-6 and a trend for decrease in CRP levels were recorded, while no changes were observed in other established inflammatory and immunological markers.
Changes of Biomarkers Between the Baseline and Follow-Up Period of Patients With HF.a
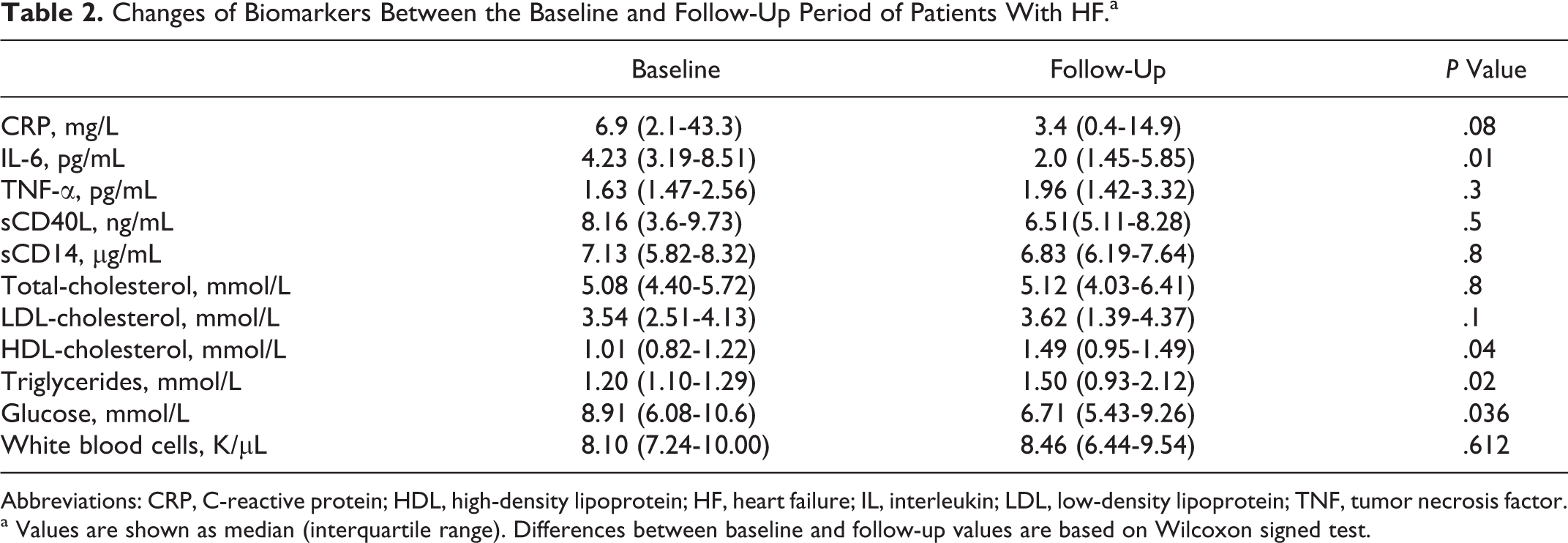
Abbreviations: CRP, C-reactive protein; HDL, high-density lipoprotein; HF, heart failure; IL, interleukin; LDL, low-density lipoprotein; TNF, tumor necrosis factor.
a Values are shown as median (interquartile range). Differences between baseline and follow-up values are based on Wilcoxon signed test.
In Table 3 the levels of PAF, lyso-PAF-AT, PAF-CPT, Lp-PLA2, and PAF-AH are presented at baseline and 6-week follow-up for patients with HF and for the apparently healthy volunteers. It is noted that PAF was not detected in 3 patients at baseline 11 and the nondetected PAF values were substituted with the method detection limit, that is, 10−5 pmol/mL, while at follow-up it was detected in all patients. The PAF showed a trend for increase between baseline and follow-up (P = .1). αt baseline free PAF was lower in patients with HF than healthy participants, while at follow-up free PAF in patients with HF was higher than that of healthy participants.
Changes of PAF and Its Metabolic Enzymes Between the Baseline and Follow-Up Period in Patients With HF and Comparison With Apparently Healthy Volunteers.a
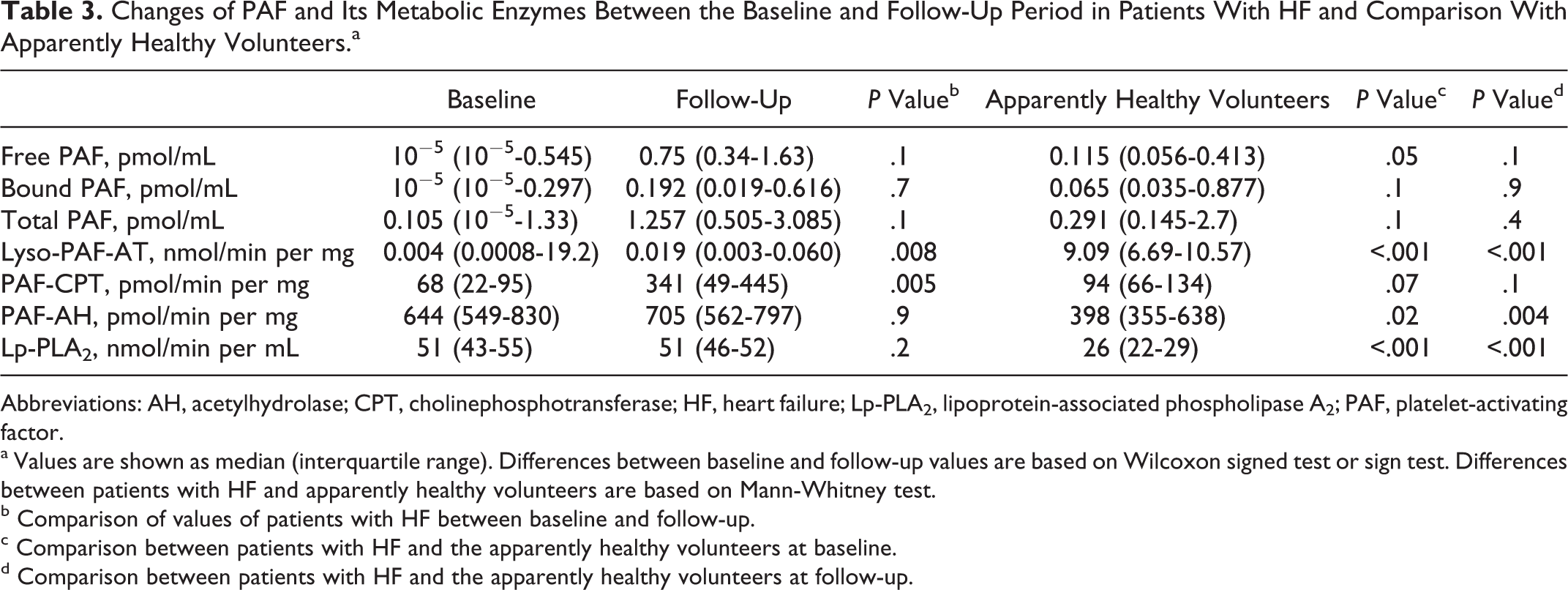
Abbreviations: AH, acetylhydrolase; CPT, cholinephosphotransferase; HF, heart failure; Lp-PLA2, lipoprotein-associated phospholipase A2; PAF, platelet-activating factor.
a Values are shown as median (interquartile range). Differences between baseline and follow-up values are based on Wilcoxon signed test or sign test. Differences between patients with HF and apparently healthy volunteers are based on Mann-Whitney test.
b Comparison of values of patients with HF between baseline and follow-up.
c Comparison between patients with HF and the apparently healthy volunteers at baseline.
d Comparison between patients with HF and the apparently healthy volunteers at follow-up.
The activities of both PAF’s investigated biosynthetic enzymes (ie, lyso-PAF-AT and CPT) increased at the follow-up period. At follow-up lyso-PAF-AT remained much lower than the values recorded for healthy volunteers, whereas PAF-CPT showed a trend for increase compared to healthy volunteers. The catabolic isoenzymes of PAF remained stable. Compared to healthy volunteers, the activities of Lp-PLA2 and PAF-AH were elevated in patients with HF at baseline and remained elevated after the 6-week follow-up.
At follow-up, lyso-PAF-AT was inversely correlated with total cholesterol (rho = −.667, P = .05) and LDL-cholesterol (rho = −.633, P = .06) and positively correlated with sCD14 (rho = .648, P = .04). The PAF-AH was also positively correlated with total cholesterol and LDL-cholesterol as well as with triglyceride levels (rho = .733, P = .02; rho = .750, P = .02; and rho = .633, P = .06, respectively). As expected Lp-PLA2 was positively correlated with total cholesterol and LDL-cholesterol (rho = .585, P < .001 and rho = .612, P < .001). No other significant correlations were observed.
Discussion
The present pilot study documents the changes in PAF and its metabolic enzymes in patients with HF over a 6-week period. The main findings of the present study include an increase in PAF’s biosynthetic enzymes in leukocytes along with a trend for increase in free and total PAF levels, whereas the activities of its catabolic isoenzymes remained stable in the 6-week follow-up. The comparison with the apparently healthy volunteers suggested that PAF’s biosynthetic enzymes are depressed in patients with HF together with free PAF at baseline. At follow-up patients with HF had a slightly elevated free-PAF accompanied with a trend for increase in PAF-CPT, while lyso-PAT-AT remained downregulated compared to healthy volunteers. The opposite trend was documented for Lp-PLA2 and PAF-AH, which were upregulated in patients with HF at all considered time points compared with apparently healthy volunteers.
The results of the present study should be critically viewed under the context of the inflammation hypothesis underlying HF pathogenesis. Several studies have suggested an implication of inflammatory molecules (such as TNF-α and IL-6) 25,26 as well as immunological markers (such as sCD40L and sCD14) 25,27 in the progression of HF and a differentiation of these biomarkers along with the severity and progression of disease. 5,27
The PAF, constituting a potent lipid mediator of inflammation, is known to be regulated from the aforementioned cytokines, 28,29 it may synergistically amplify their cellular signals 30 and further activate their expression. 31,32 In parallel, we have recently documented a strong correlation of PAF biosynthetic enzymes with inflammatory and immunological markers in patients with HF. 11 Moreover, in the present study, at follow-up lyso-PAF-AT activity was positively related to sCD14, which is in line with the fact that sCD14 may be implicated in PAF biosynthesis in different cell types. 33
A cursory glance at the increase in PAF biosynthetic enzymes and the trend to increase in PAF levels at the follow-up period may seem conflicting with the role of HF drugs, which are designed to improve the clinical condition of patients with HF with a parallel downregulation of the inflammatory response. 6 The increase in lyso-PAF-AT seem to be out of clinical significance since its range in normal volunteers is 1000-fold up compared to patients with HF. Similarly, patients with HF have depressed levels of PAF-CPT compared to healthy volunteers at baseline, although the differences are less pronounced. In contrast, PAF-CPT levels at follow-up were slightly elevated. This result may explain the slight increase in PAF levels also observed at follow-up. Indeed, in a recent study our group has shown that PAF-CPT correlates with free-PAF levels in healthy male participants. 34 It could be thus hypothesized that medical treatment keeps the “PAF network” downregulated, which may be the case for the acute drug effects at the baseline period (4th day of admission) as well as their prolonged effects after the 6-week follow-up especially for the case of lyso-PAF-AT. This hypothesis is corroborated by the fact that PAF levels seem to be low in patients with HF or in patients with myocardial infarction at admission 11,35 and the expression of its receptor is upregulated. 36 This notion is further supported by the fact that most common drugs for HF therapy (aldosterone antagonists, angiotensin-converting enzyme inhibitors, antiarrythmic agents, statins, and diuretics) have been reported to possess anti-inflammatory effects, 37,38 although there are some studies not showing such effects. 39 Statins in particular have been shown to decrease Lp-PLA2 and PAF-CPT activities and to have a neutral effect in lyso-PAF-AT activity in healthy volunteers after a 3-week medical treatment. 40 Lyso-PAF-AT is unaffected by statins in healthy volunteers, while it seems to be strongly downregulated in patients with HF in the present study. Other possible interactions between PAF and cardiovascular drugs include nitrates and calcium channel blockers, which reduce PAF production in endothelial cells, 41 and human umbilical vein endothelial cells 42 and human umbilical vein endothelial cells, angiotensin-converting enzyme inhibitors which partly inhibit PAF effects and may lead to reduced PAF synthesis 43,44 and salicylates, which inhibit the lyso-PAF-AT. 45
From a different perspective, the trend for increase in PAF observed at the follow-up period in patients with HF may favor compensatory mechanisms of the disease. Indeed, a different “cardioprotective” role has been attached to low concentrations of PAF, which do not affect heart contractility but may play a favorable role in ventricular remodeling. 46
As far as the catabolic enzymes of PAF are concerned, the research field with a special interest to Lp-PLA2 is much larger. As a matter of fact, the increased levels of Lp-PLA2 and PAF-AH in patients with HF compared to healthy volunteers is in line with the literature, since increased levels of Lp-PLA2 have been connected to incident HF 16 and patients with cardiovascular disease have increased Lp-PLA2 activity. 47 Interestingly, the catabolic isoenzymes of PAF seem not to be affected by drug treatment in the 6-week follow-up.
The small sample size is a limitation of the present study. Moreover, the ejection fraction was not measured in healthy volunteers. This means that the possibility of a healthy volunteer to have asymptomatic HF cannot be ruled out.
Conclusions
In conclusion, despite the descriptive nature of the present study, newly diagnosed patients with HF under drug treatment have an affected profile of PAF biosynthetic enzymes and especially lyso-PAF-AT. In contrast, PAF catabolic enzymes remained elevated in line with their recently suggested role as cardiovascular risk markers.
Footnotes
Authors’ Note
Paraskevi Detopoulou is a recipient of a PhD fellowship from the Greek State’s Scholarship Foundation (IKY) and the Hellenic Atherosclerosis Society.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Hellenic Atherosclerosis Society.