
Abstract
Most patients with peripheral arterial disease (PAD) are asymptomatic and have similar vascular morbidity and mortality with patients with symptomatic PAD. Despite being a very highly prevalent disease, physicians underdiagnose and undertreat PAD. A total of 100 participants with aortic valve sclerosis (AVS) and 100 participants without AVS and age-, gender-, and cardiovascular risk factor–matched participants were enrolled. Ankle–brachial index (ABI) and AVS were evaluated by handheld Doppler device and echocardiography, respectively. There was significantly lower ABI in participants with AVS compared with those without AVS (1.04 ± 0.14 v 1.11 ± 0.07, P = .001). There was a negative correlation between ABI and AVS (r = −.29, P < .001). Linear regression analysis demonstrated an independent association between ABI and AVS (95% confidence interval [CI]: −0.91 to −0.27, P < .001) and β-blocker use (95% CI: −0.96 to −0.02, P: .04). Our findings confirm an association between AVS and PAD that may be attributed to shared vascular risk factors.
Peripheral arterial disease (PAD) of lower extremities, a manifestation of atherosclerosis, is associated with a significant increase in cardiovascular morbidity and mortality.1–3 Not only symptomatic PAD but also asymptomatic PAD carries a high mortality and vascular event risk. 4 The prevalence of PAD in the general population aged ≥40 years is approximately 4%, but it strongly increases with age up to 15%. 5 However, PAD has long been underestimated, underdiagnosed, and undertreated.6,7
Aortic valve sclerosis (AVS) is defined by echocardiography as thickening and calcification of the normal trileaflet aortic valve without obstruction to left ventricular outflow. Several reports have demonstrated a significant association between AVS and atherosclerosis risk factors or clinical atherosclerosis.8–10
Our aim in this study was to assess the link between AVS and PAD and to see which risk factors are shared and to what extent.
Methods
Participants
Participants with AVS (n = 100) and age-, gender-, and established cardiovascular risk factors–matched 100 participants without AVS were prospectively selected from patients referred to the echocardiography laboratory at the Ahi Evren Thoracic and Cardiovascular Surgery Training and Research Hospital. Patients with aortic stenosis (transaortic flow velocity >2.5 m/s), rheumatic valvular disease prosthetic valves, bicuspid aortic valves, congenital heart disease, bacterial endocarditis, atrial fibrillation, or hypertrophic obstructive cardiomyopathy as well as those who had symptomatic vascular disease such as stroke, transient ischemia, coronary heart disease (CHD), congestive heart failure, and intermittent claudication or any peripheral artery revascularization were excluded from the study. The CHD was defined by (1) self-reported myocardial infarction, angina, or use of nitroglycerin and (2) self-reported history of coronary angioplasty or coronary artery bypass surgery. Cerebrovascular disease was defined by self-reported stroke, transient ischemic attack, or carotid endarterectomy. The AVS is defined by echocardiography as thickening and calcification of the normal trileaflet aortic valve without obstruction to the left ventricular outflow. Ankle–brachial index (ABI) measurement and echocardiography examination were performed by 2 different investigators who were blinded to the patient’s clinical data (M.O.V. and H.B., respectively). Informed consent was obtained from all participants.
Assessment of Cardiovascular Risk Factors
In addition to questions about the symptoms of CHD, PAD, and stroke, data on cardiovascular risk factors, diabetes mellitus, arterial hypertension, and smoking habits were obtained. Patients were considered to be hypertensive if they had a systolic blood pressure (BP) >140 mm Hg and/or diastolic BP >90 mm Hg or were using antihypertensive drugs. Participants with fasting glucose ≥126 mg/dL and/or on treatment were considered as having diabetes. Smoking was defined as “current smokers” or “nonsmokers.” Hypercholesterolemia was defined as total cholesterol >200 mg/dL or taking medications.
Measurement of ABI
Lower limb BP was determined with the patient in the supine position from the right and left posterior tibial arteries. When the posterior tibial artery BP was not measurable, the dorsalis pedis artery was used. All measurements were performed using an appropriately sized cuff. The systolic BP was detected with a handheld Doppler probe. The ABI was calculated for each lower limb by dividing the ankle systolic BP by the average of the 2 systolic BP measurements performed on the arm. For each patient, the lowest ABI recorded in the 2 ankles was used for analysis. Participants with ABI ≥1.4 were excluded because these participants were considered to have noncompressible arteries.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation and categorical variables were expressed as percentage. An analysis of normality of the continuous variables was performed with the Kolmogorov-Smirnov test. A comparison of the categorical variables between the groups was performed using a chi-square test. Continuous variables were compared using unpaired t test and Mann-Whitney U test. Pearson and Spearman correlation tests were used for continuous variables. Chi-square analysis was used for categorical variables. Linear regression analysis was performed in order to identify independent determinants for ABI. A P < .05 (2-sided) was considered significant. Statistical analysis was carried out using SPSS 14.0 statistical software.
Results
Demographics and clinical characteristics of participants are listed in Table 1. Participants with AVS had higher rate use of angiotensin-converting enzyme inhibitors or angiotensin receptor blocker, β-blockers, and aspirin (ASA). There was significantly lower ABI in participants with AVS compared with those without AVS (1.04 ± 0.14 vs 1.11 ± 0.07, P = .001; Figure 1). There was statistically negative correlation between ABI and AVS (r = −.29, P < .001), age (r = −.19, P = .05), β-blocker (r = −.21, P = .03), and ASA (r = −.17) use (Table 2). Linear regression analysis demonstrated independent association between ABI and AVS (95% confidence interval [CI]: −0.91 to −0.27, P < .001) and β-blocker use (95% CI: −0.96 to −0.02, P = .04). Table 3 lists the clinical and demographic characteristics of patients with AVS with and without PAD.
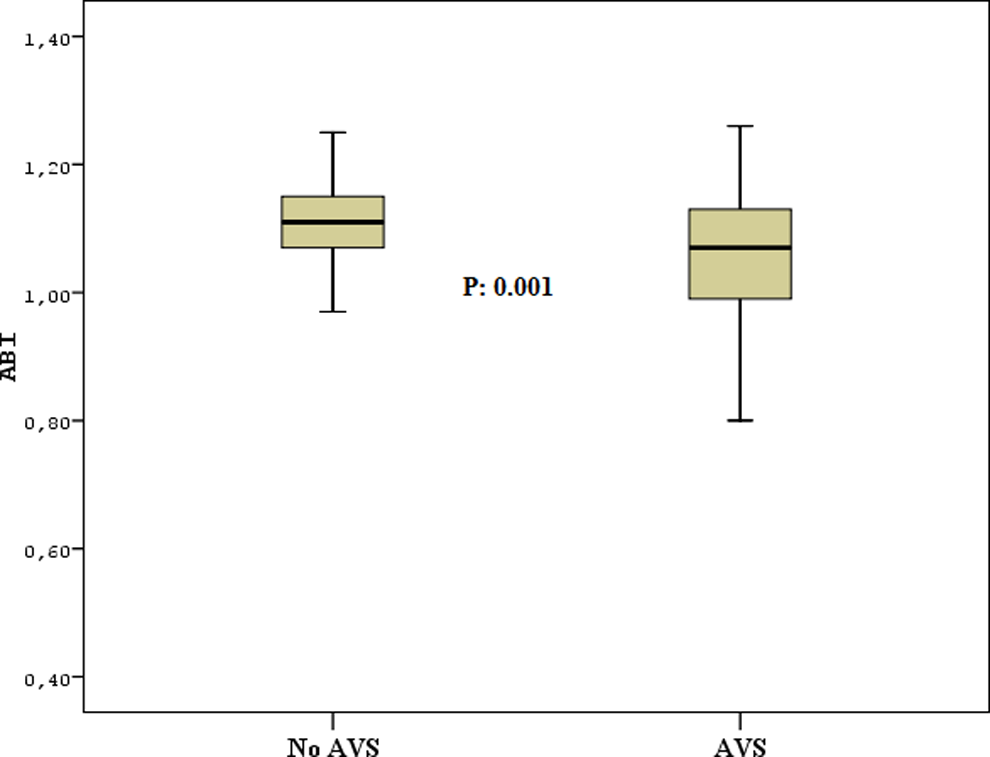
The ABI values in participants with and without AVS. ABI indicates ankle–brachial index; AVS, aortic valve sclerosis.
Clinical, Demographic, and Laboratory Characteristics of Patients and Control Participants.
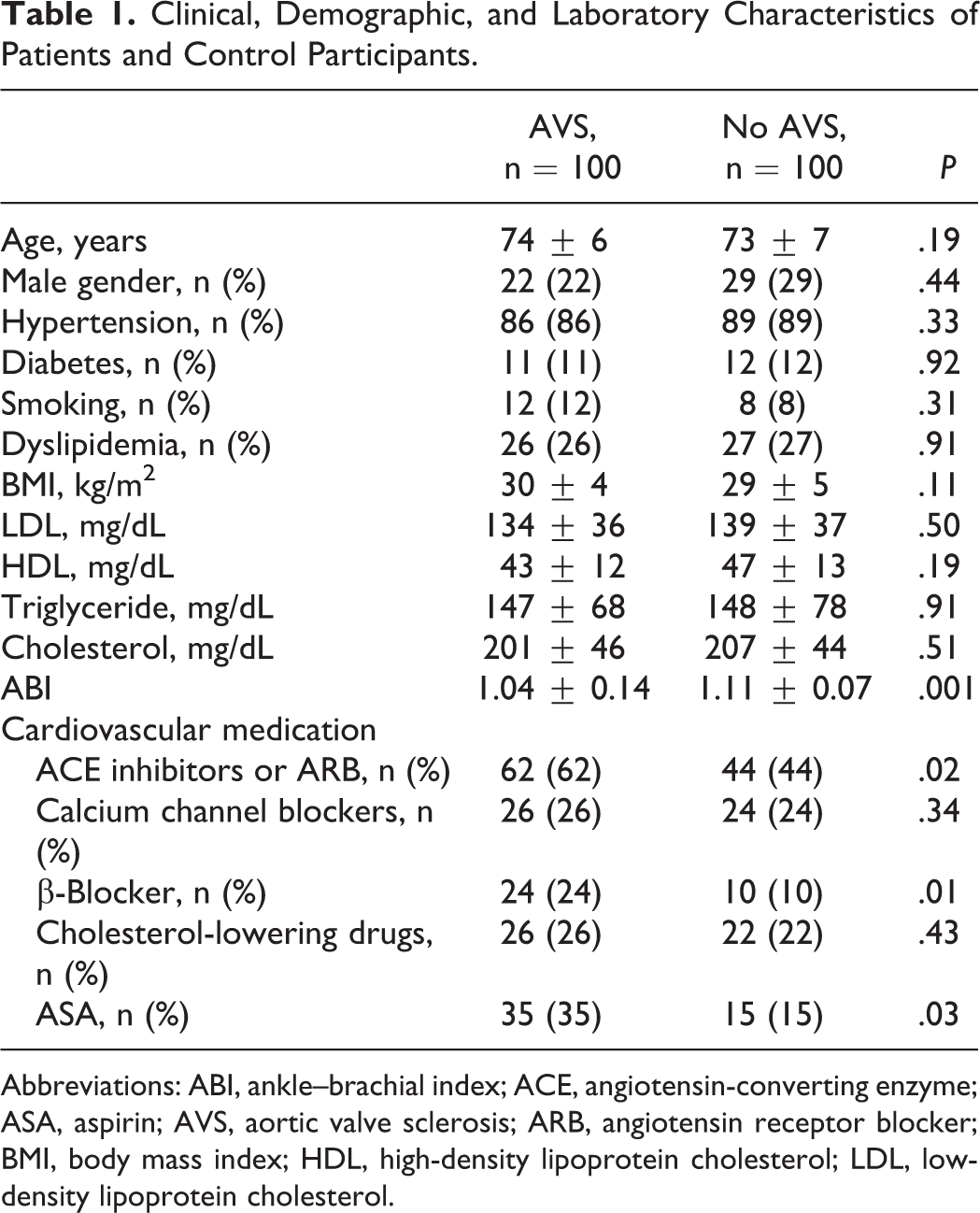
Abbreviations: ABI, ankle–brachial index; ACE, angiotensin-converting enzyme; ASA, aspirin; AVS, aortic valve sclerosis; ARB, angiotensin receptor blocker; BMI, body mass index; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol.
Univariate Analyses of ABI and Other Variables.
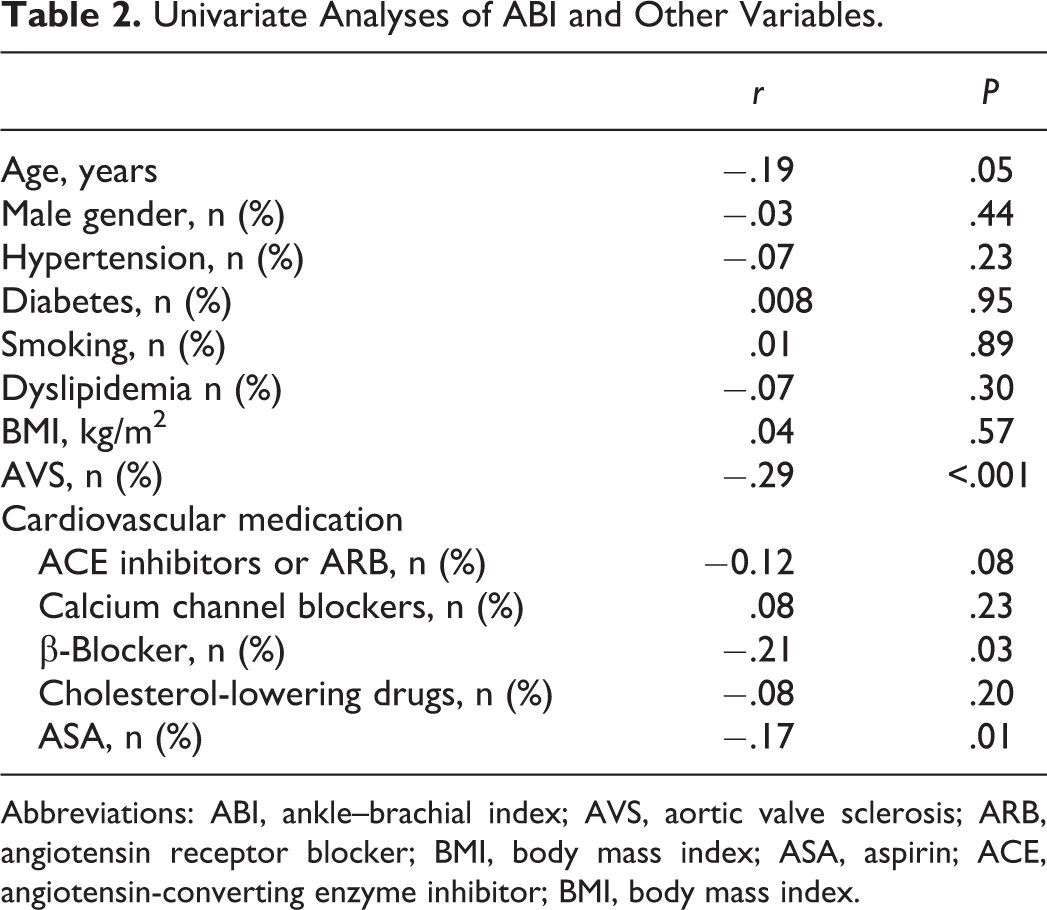
Abbreviations: ABI, ankle–brachial index; AVS, aortic valve sclerosis; ARB, angiotensin receptor blocker; BMI, body mass index; ASA, aspirin; ACE, angiotensin-converting enzyme inhibitor; BMI, body mass index.
Clinical, Demographic, and Laboratory Characteristics of Patients With AVS According to the ABI Categories.
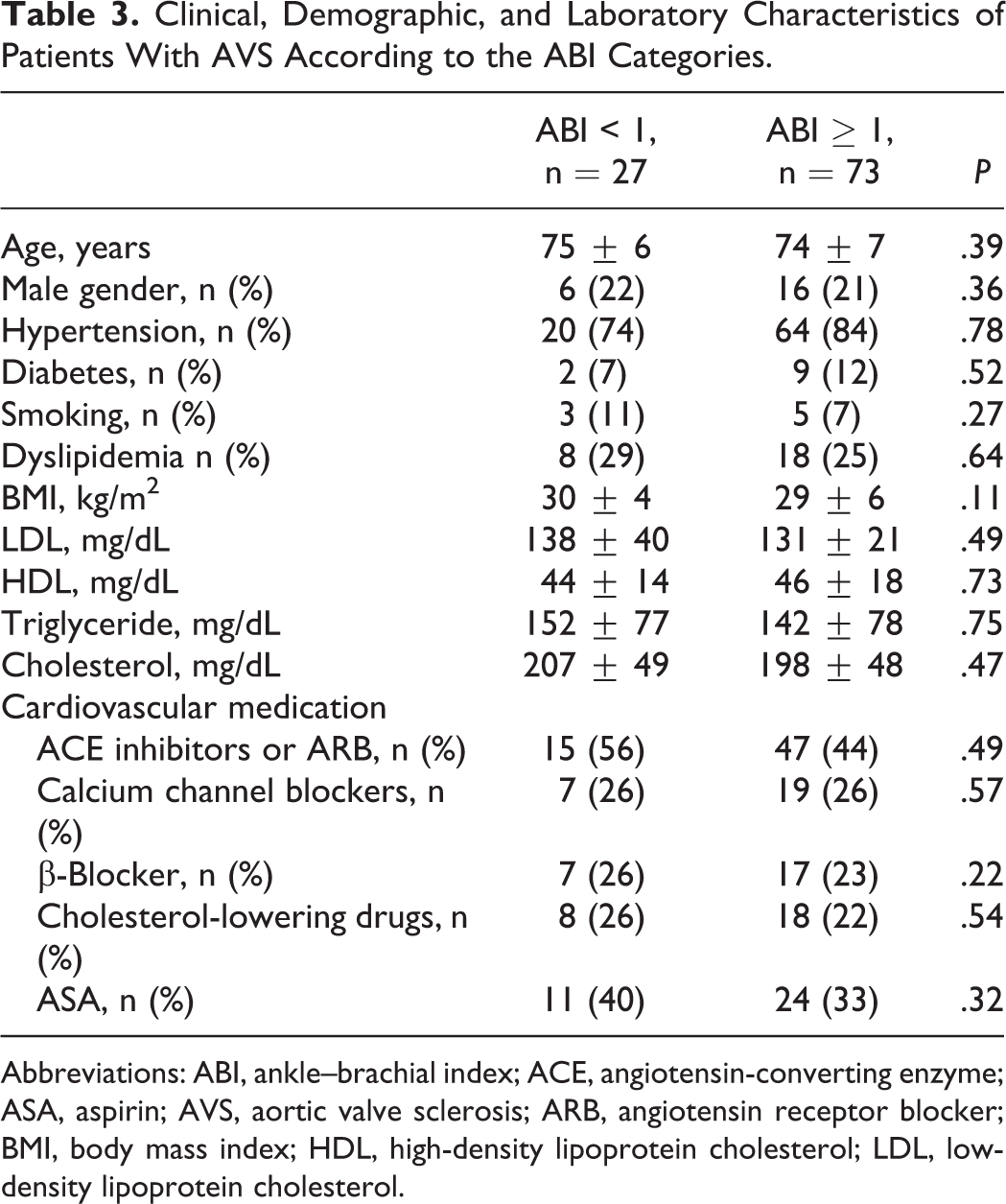
Abbreviations: ABI, ankle–brachial index; ACE, angiotensin-converting enzyme; ASA, aspirin; AVS, aortic valve sclerosis; ARB, angiotensin receptor blocker; BMI, body mass index; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol.
In all, 34 participants (17%) had low ABI reflecting overt and borderline PAD (ABI <1) and 166 participants had normal ABI (ABI ≥ 1) meaning normal peripheral arteries. In low ABI group, 27 (80%) out of 34 participants had AVS, whereas in normal ABI group 70 (42%) out of 166 participants had AVS (P < .001; Figure 2).
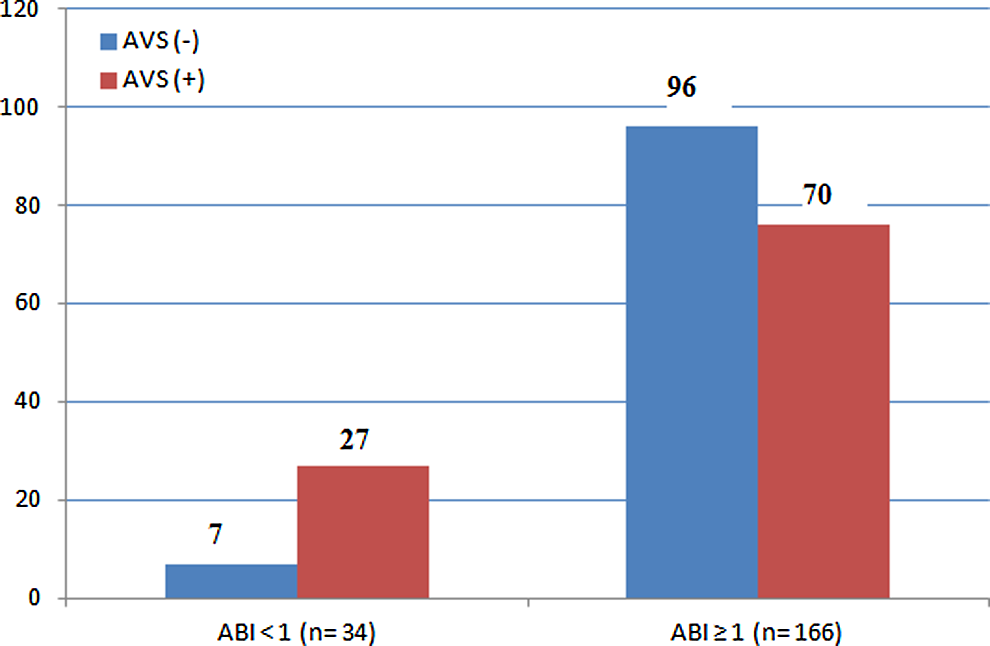
Distribution of participants with and without AVS according to the ABI values. ABI indicates ankle–brachial index; AVS, aortic valve sclerosis.
Discussion
We found decreased ABI values in asymptomatic participants with AVS. Also, we have detected higher prevalence of AVS in patients with asymptomatic PAD. Noteworthy, most of these patients are not on guideline-recommended medical treatments.
The majority of individuals with PAD do not experience recognizable limb ischemic symptoms, and asymptomatic PAD is 2 to 5 times more prevalent than symptomatic PAD. The PAD, even without classic claudication, is often associated with leg dysfunction, diminished functional status, and increased cardiovascular ischemic risk.2,11–13 The risk of cardiovascular mortality is increased and independent of established cardiovascular risk factors (eg, age, sex, BP, smoking, cholesterol, and diabetes in asymptomatic PAD).14,15
Although PAD is well described and the overall public health implications are well understood, this condition is still underdiagnosed and undertreated. 16 This is mostly attributable to the fact that nearly half of the patients with PAD can be asymptomatic and the main symptom, intermittent claudication, is only present in some patients. 17 Evaluation of claudication is especially difficult in elderly participants who are physically inactive although they may have significant stenoses and not have symptoms until the demand for blood flow to leg muscles is increased. Recently, it has been demonstrated that the clinical examination, the presence of cardiovascular risk factors, and the presence of cardiovascular morbidity do not identify patients with a low ABI in general practice. 18 On the other hand, screening in asymptomatic unselected older adults with ABI may yield lower rate of PAD. 19 In addition, there is a great disagreement regarding routine screening of patients for asymptomatic PAD. 7
The most efficient, objective, and practical means of documenting the presence and severity of PAD is measuring the ABI. It is a simple, inexpensive, and noninvasive measurement, 5 even at the presymptomatic phase when intervention can improve prognosis and prevent or delay severe complications.6,7 Measurement of ABI is necessary to identify patients with PAD, since clinical examination alone cannot exclude the presence of PAD. 20 The importance of measuring ABI is also stressed by the fact that patients with asymptomatic PAD have similar vascular morbidity and mortality in patients with symptomatic PAD.4,13
The relation between AVS and ABI may be explained by the fact that PAD is a common manifestation of the atherosclerotic process. In addition, risk factors for PAD are similar to those important in the etiology of CHD and are the typical risk factors for atherosclerotic disease. Recent studies have suggested that AVS is a manifestation of the atherosclerotic process and documented overlap in the clinical factors traditionally associated with AVS and atherosclerosis. 21
Our study has limitations. First, the number of study participants was low and selected from those who underwent echocardiography. The reasons for echocardiography examination are generally for evaluating dyspnea and cardiac murmurs. Also, our study design does not allow us in detail for pathophysiological mechanisms responsible for this relation.
In conclusion, since the majority of patients with PAD are asymptomatic, an echocardiographic assessment of the aortic valve planned for non-PAD-related symptoms may identify a group of patients at high risk of PAD. Our findings also confirm an association between AVS and PAD that may be attributed to shared vascular risk factors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.