
Abstract
We measured brachial artery flow-mediated dilatation (FMD) and common carotid intima-media thickness (cIMT) in overweight (n = 67) and normal weight children (n = 115, controls). Age at examination ranged from 72 to 182 months (mean 123 ± 27). Compared to controls, the overweight children had increased weight, waist and hip circumference, systolic and diastolic blood pressures (all P < .001), right and left mean cIMT (mm; 0.58 [0.42-0.68] vs 0.44 [0.3-0.64], P < .001 and 0.56 [0.32-0.70] vs 0.44 [0.3-0.60], P < .001), respectively, and decreased FMD (%; 6.25 [3.33-19.05] vs 7.69 [3.45-16], P < .001). The cIMT and FMD were closely related to the serum insulin concentrations. Age, waist circumferences, and serum triglycerides were independent predictive risk factors for increased cIMT, and fasting glucose and BMI were independent predictive variables for decreased FMD. Overweight children are also potentially at risk of early atherosclerosis as much as obese children.
Keywords
Introduction
The rate of childhood obesity in the United States is about 16.9% and those children are at risk of later heart disease. 1 However, it has not been established whether this risk also applies to overweight children.
The measurement of the brachial artery flow-mediated dilatation (FMD) and carotid artery intima-media thickness (cIMT) by ultrasound imaging are validated and reproducible methods that have been used for the assessment of endothelial and arterial function, as well. 2 –6 A decreased brachial artery FMD represents endothelial dysfunction, and an increased cIMT is considered an indicator of early structural vascular damage. 7,8
Brachial artery FMD, cIMT, and serum insulin levels are markers for future cardiovascular events and there is a correlation between the degree of obesity and the serum levels of insulin. 9
There are studies that reported an association between brachial artery FMD and carotid IMT and obesity in children, 10 –12 whereas these 2 measures of subclinical atherosclerosis have not been adequately evaluated in overweight children. The aim of this study was to assess whether there is a relationship between the brachial artery FMD and cIMT and serum insulin levels in overweight children.
Methods
Study Design
This study is a cross-sectional, observational study.
Study Population and Protocol
Between June 2011 and May 2012, 182 consecutive children were enrolled from our pediatric clinics, examined in our cardiology and pediatric clinics, and classified into 2 groups. The first group comprised 67 overweight children (29 female and 38 male, between 72 and 182 months old, body mass index [BMI] between 25.0 and 29.9 kg/m2, mean BMI 27.2 ± 1.1 kg/m2) as the overweight group. Normal-weight peers (n = 115; 47 female and 68 male, between 74 and 177 months old, BMI between 18.7 and 24.8 kg/m2, and mean BMI 21.2 ± 1.3 kg/m2) acted as the control group. The baseline characteristics such as anthropometric, clinical features, biochemical, and hormonal parameters of the study and control groups are shown in Table 1.
Anthropometric, Clinical Features, and Biochemical Parameters of the Overweight and Control Groups.a
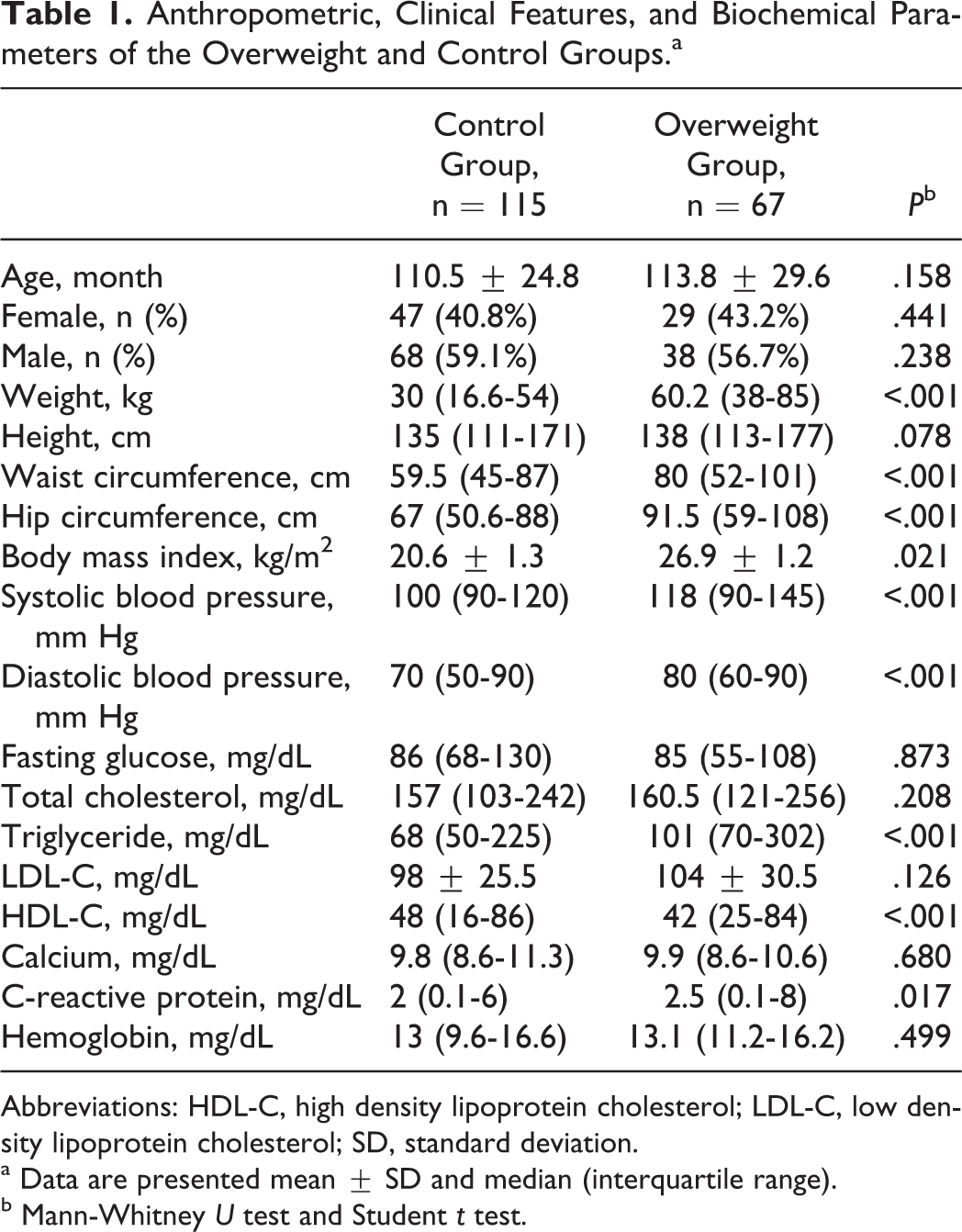
Abbreviations: HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; SD, standard deviation.
a Data are presented mean ± SD and median (interquartile range).
b Mann-Whitney U test and Student t test.
The inclusion criteria were BMI ≥25 and ≤29.9 kg/m2 for the overweight group, and the children with BMI ≥18.5 and ≤24.9 kg/m2 for the control group.
Exclusion criteria were defined for the 2 groups as the following: children with BMI ≤18.5 kg/m2, moderate to severe valvular disease, left ventricle ejection fraction <45%, electrolyte disorders, history of heart disease, hypertension, diabetes mellitus, or any systemic disease as well as those with known hormonal disorders.
All participants underwent routine clinical and laboratory examinations, including anthropometric measurements and routine blood tests. We examined all the participants in the morning in the outpatient ultrasonography room after obtaining their blood sample. The brachial artery FMD and cIMT were measured in all study participants. Our primary goal was to evaluate the relationship between brachial artery FMD and cIMT and serum insulin levels in overweight children.
The procedure and the study protocol were approved by the bioethics committee of our institution. Informed consent was obtained from the children and their parents before the investigation.
Clinical Characteristics and Biochemical Analysis
Blood samples and anthropometric measurements were obtained after the ≤10-hour fasting period from all the study participants, and then their BMIs were calculated. The glucose oxidase method was used to measure serum glucose concentration. The resting systolic and diastolic blood pressure was measured using the sphygmomanometric method and a standard 10-cm cuff with a length of 40-cm (small adult cuff, Johnson and Johnson, USA). Total cholesterol (TC) and triglycerides (TGs) were measured by the enzymatic method; a chromogenic substrate kit for the determination of high-density lipoprotein cholesterol (HDL-C) was used, and then low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald equation (LDL = TC − [HDL-C − [TG/5]). 13 The quantitative analysis of insulin was measured using the Cobase 601 Kit (detection range: 0.2-1000 mIU/mL), Roche Diagnostics, Mannheim, Germany.
Ultrasonographic Assessment
All ultrasonographic data were obtained by 1 experienced cardiologists who was unaware of the study participants’ group with an Esaote, My Lab 50 (Florence, Italy) ultrasound scanner that has a functional electrocardiogram (ECG) mode and an 11 MHz linear array transducer. Both brachial artery FMD and cIMT were obtained with an optimal resolution of the vessel layers as previously described. 2
All the participants were examined in a comfortable supine position after resting for about 10 minutes. At least 3 consecutive B-mode ultrasonographic images of both the right and the left common carotid arteries with a synchronized ECG were measured during diastole at the examination time, and the zoom function of the ultrasound was used to focus the lumen–intima interface and media–intima interface on the posterior common carotid artery wall, 10 to 20 mm below the bulb. Immediately afterward, the ultrasonographic carotid diameter and inner layer measurements were obtained, and the brachial artery FMD measurements were performed according a standardized and validated protocol. 14,15
To obtain optimal longitudinal brachial artery B-mode images, a linear transducer was placed immediately above the antecubital fossa with simultaneous ECG recordings. First, after the measurement, the 3 consecutive diastolic arterial diameters on the frozen m-line image were calculated using the average value as baseline diameter. Second, a pneumatic cuff was placed above the antecubital fossa and then rapidly inflated to at least 50 mm Hg above suprasystolic pressure for a 5-minute occlusion of the brachial artery flow. Images to visualize reactive hyperemia were continuously obtained following the rapid deflation of the pneumatic cuff, then the average of 3 frozen m-line images as postdilatation diameter were calculated. Finally, dividing the baseline diameter by the difference of the baseline and postdilatation diameter, the FMD (%) was calculated.
A total of 20 overweight children were reexamined after 10 days to determine the visiting coefficients of variation. These were 3.9% and 3.3%, respectively, for cIMT and Δ diastolic diameter of the brachial artery for the FMD.
Statistical Analysis
We obtained all statistics data by using PASW Statistics 18 for Windows (SPSS Inc, Chicago, Illinois). A Kolmogorov-Smirnov test was used to check continuous variables distributions. The Student t test was used when the data fit to the normal distribution, and Mann-Whitney U test was performed for abnormal distribution data. A P ≤.05 was considered significant. The continuous variables are presented as a mean ± standard deviation (SD) for the parametric data or median (interquartile range) for the nonparametric data. A stepwise multiple linear regression analysis was performed for detecting the independent variables affecting cIMT and FMD. Pearson correlation test was performed to test the relationships between cIMT and brachial artery FMD and serum insulin levels.
Results
Study Population, Baseline Characteristics, and Biochemical Measurements
The baseline demographic, anthropometric, clinical, biochemical, cIMT, and FMD measurements are shown in Table 1. There were predominantly males in the 2 study groups. There was no significant difference in terms of age, gender, height, fasting glucose, TC, LDL-C, Ca2+, C-reactive protein, or hemoglobin value. Weight (60.2 [38-85] vs 30 [16.6-54] kg, P < .001), waist (80 [52-101] vs 59.5 [45-87] cm, P < .001) and hip circumference (91.5 [59-108] vs 67 [50.6-88] cm, P < .001), BMI (26.9 ± 1.2 vs 20.6 ± 1.3 kg/m2, P = .021), systolic (118 [90-145] vs 100 [90-120] mm Hg, P < .001) and diastolic blood pressure (80 [60-90] vs 70 [60-90] mm Hg, P < .001], and TG value (101 [70-302] vs 68 [50-225] mg/dL, P < .001) were significantly higher in the overweight group than in the control group (Table 1).
The cIMT, FMD, and Serum Insulin Levels
Right and left cIMT values were higher in the overweight group compared to the control group (0.58 [0.42-0.68] vs 0.44 [0.3-0.64] mm, P < .001 and 0.56 [0.32-0.70] vs 0.44 [0.3-0.60] mm, P< .001, respectively). The brachial artery baseline diameter was similar between the 2 groups. There was a significant difference between the overweight and the control groups in terms of FMD (6.25 [3.33-19.05] vs 7.69 [3.45-16]%, P < .001; Table 2; Figure 1).
Serum Insulin Levels and Ultrasonographic Parameters of the Overweight and Control Groups.a
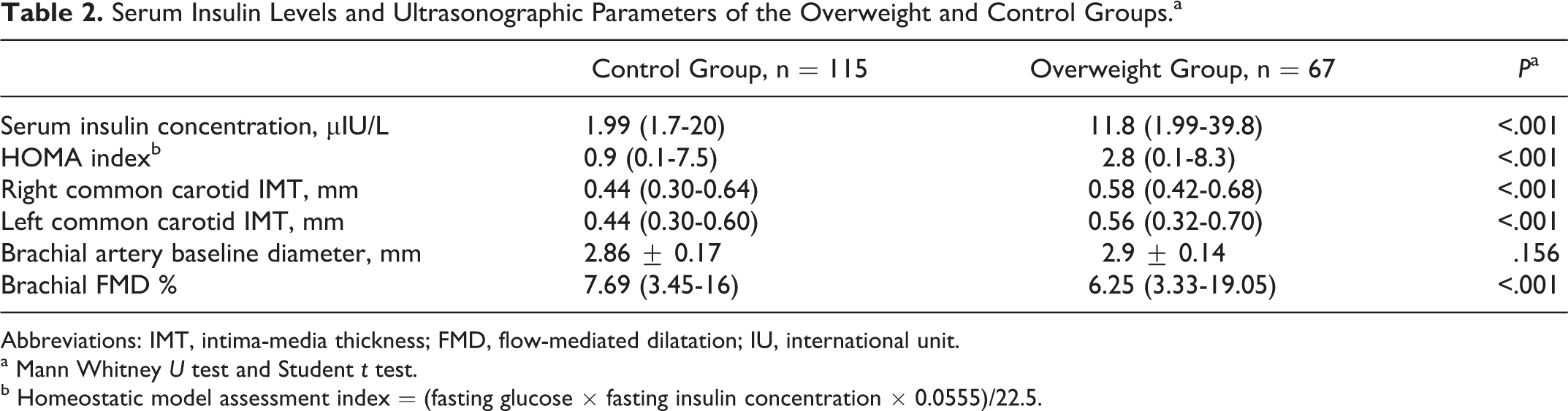
Abbreviations: IMT, intima-media thickness; FMD, flow-mediated dilatation; IU, international unit.
a Mann Whitney U test and Student t test.
b Homeostatic model assessment index = (fasting glucose × fasting insulin concentration × 0.0555)/22.5.
Comparison of flow-mediated dilatation between overweight children and control group.
Serum insulin concentration and homeostatic model assessment index were higher in the overweight group than that of the control group (11.8 [1.99-39.8] vs 1.99 [1.7-20] µIU/L, P < .001 and 2.8 [0.1-8.3] vs 0.9 [0.1-7.5] µIU/L, P < .001; Table 2). In the overweight children, brachial artery FMD was negatively correlated with serum insulin levels (r = −.314, P < .0001; Figure 2). Both the right and the left cIMT correlated with serum insulin levels (r = .502, P < .0001 and r = .521, P < .0001; Figures 3 and 4). In a stepwise multiple linear regression analysis, age, waist circumference, and high TG levels were significantly related with cIMT, while FMD seemed to be influenced by the fasting glucose and BMI (Table 3).
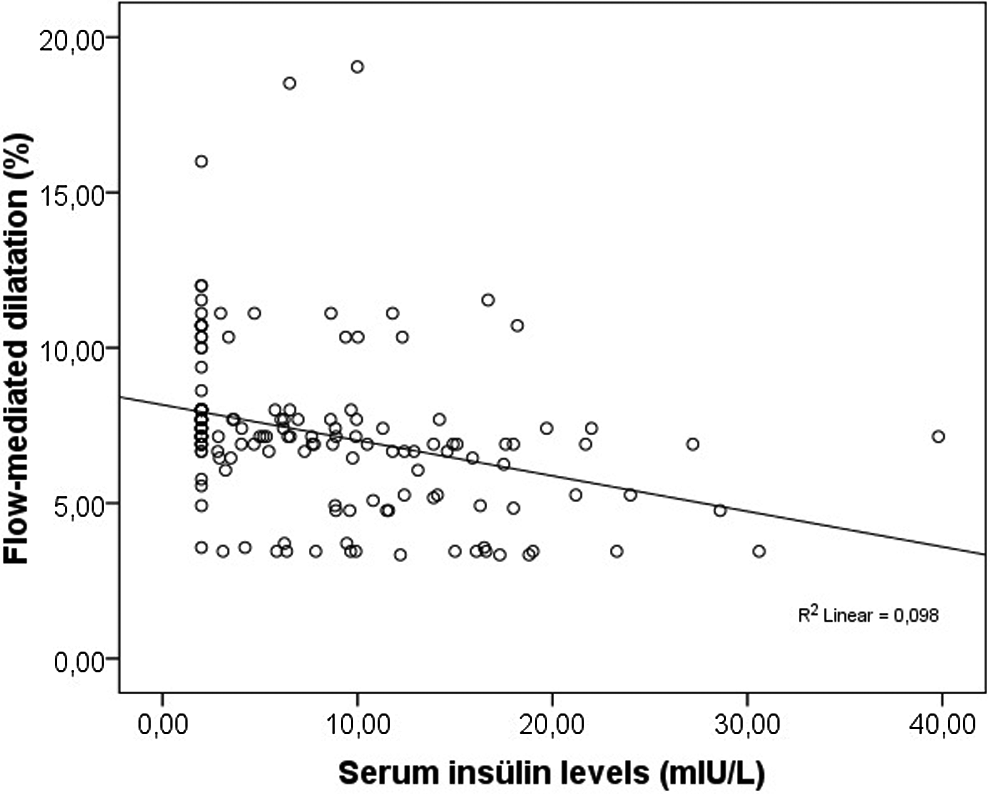
A negative linear relation between serum insulin levels and increasing flow-mediated dilatation is shown on scatter diagram (r = −.314, P < .0001).
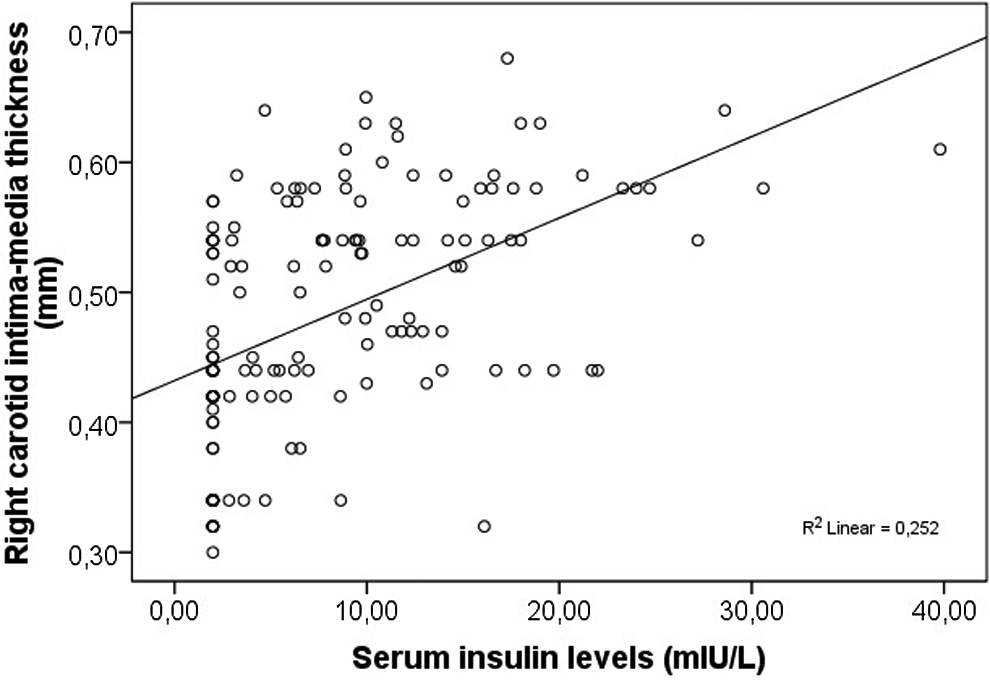
Correlation between right carotid intima-media thickness and serum insulin levels (Pearson coefficient r = .502, P < .0001).
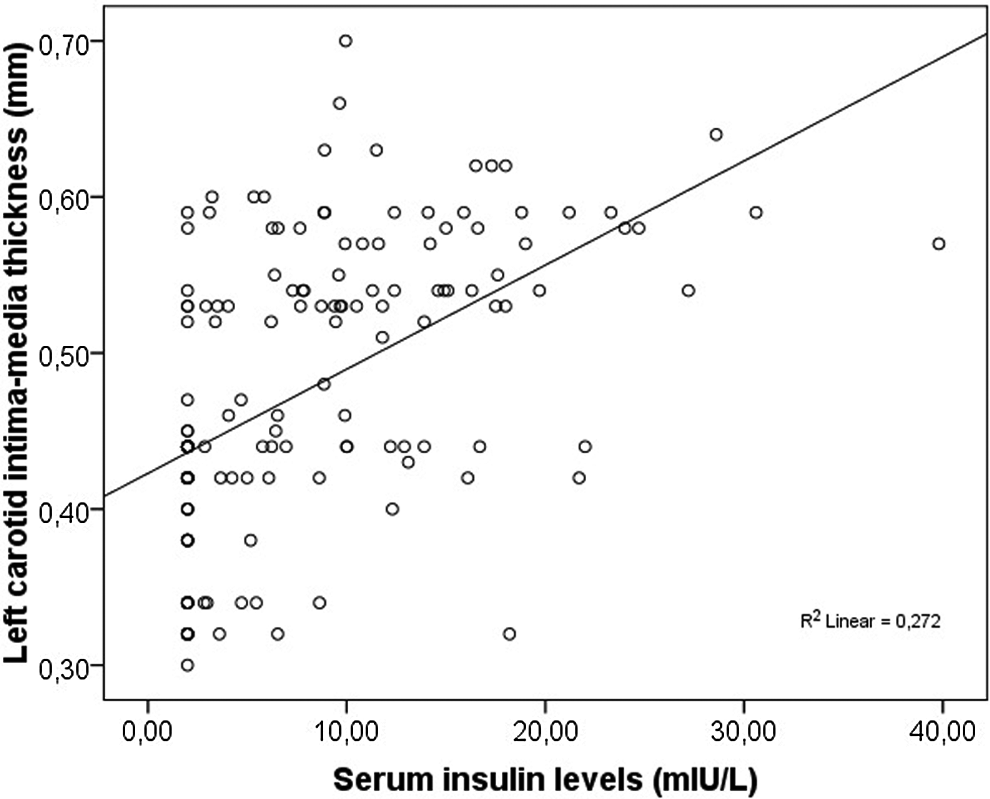
Correlation between right carotid intima-media thickness and serum insulin levels (Pearson coefficient r = .521, P < .0001).
Stepwise Multiple Linear Regression Analysis.

Abbreviations: BMI, body mass index; TG, triglyceride; cIMT, carotid intima-media thickness; FMD, flow-mediated dilatation.
Discussion
Obesity is associated with hypertension, dyslipidemia, and abnormal glucose metabolism in children, which are the risk factors for early atherosclerosis. 16 The detection of the early atherosclerosis by the FMD and cIMT measurements is highly reproducible and easy, especially in the clinics with experienced ultrasound technicians. 14,17 –19 There are enough findings regarding FMD, cIMT, and insulin levels in obese children, but these variables have not been well documented in overweight children.
Morrison et al 20 found that there was no vascular structural change in terms of cIMT in overweight children with multiple cardiovascular risk factors. In contrast, we found that the cIMT and serum insulin levels in overweight children were higher than that of normal weight children, and the FMD in overweight children was lower than that in normal weight children. The level of serum insulin was positively correlated with the cIMT and negatively correlated with the brachial artery FMD in overweight children. These results are not different from the previous studies in obese children, 10 –12 and our study suggested that overweight children are at risk of early atherosclerosis as much as obese children.
Both brachial artery FMD and cIMT are validated methods for the diagnosis of early atherosclerosis in children with hyperlipidemia and hypertension. 18,19,21 Brachial artery FMD is less well validated than cIMT in the detection of early subclinical atherosclerosis.
In the present study, overweight children had lower FMD values when compared to normal weight children and had higher systolic and diastolic blood pressures than normal weight children, even though in the normotensive range. It is known that waist circumference is often associated with higher blood pressure values, 22 and cIMT is strongly associated with age, systolic blood pressure, BMI, fasting glucose, TC, and LDL-C as well as high TG levels. 4,20,22,23 Age, waist circumference, and high TG levels were the factors associated with the cIMT, and there was a positive correlation between the cIMT and insulin levels in our study. Higher blood pressure values in overweight children than in normal weight children may be a reason for an increased cIMT. Therefore, overweight children should be considered at risk of early atherosclerosis. Brachial artery FMD impairment occurs prior to cIMT 24 and correlates negatively with cIMT. It is known that the serum glucose level is a cause of endothelial dysfunction. 25 In the present study, according to regression analysis, we found that fasting glucose and BMI are significantly related to the FMD, although fasting glucose values were similar between overweight and normal weight children. Additionally, serum insulin concentration did not directly associate with FMD, but there was a negative correlation between FMD and insulin levels.
The main limitation of the present study was that the study population was small. According to our findings, overweight children are potentially at risk of early atherosclerosis. However, further studies are necessary to confirm that our study is applicable to the general population of overweight children. The FMD and cIMT assessment, serum insulin concentrations as well as high TG levels and increased waist circumference may help in the detection of early subclinical atherosclerosis in overweight children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.