
Abstract
We assessed the impact of preprocedural high-sensitivity C-reactive protein (hsCRP) on the incidence of contrast-induced nephropathy (CIN) in patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (p-PCI). We retrospectively studied 1452 patients with STEMI undergoing p-PCI. Baseline clinical characteristics, CIN incidence, and other inhospital clinical outcomes were compared among hsCRP quartiles; 212 (14.6%) patients developed CIN. The overall inhospital mortality rate was 4.5% (65 patients). Univariate analysis revealed CIN incidence was significantly associated with hsCRP, with 7.44% for quartile Q1 (<3.00 mg/L), 12.6% for Q2 (3.00-5.90 mg/L), 16.9% for Q3 (5.91-11.4 mg/L), and 21.49% for Q4 (>11.4 mg/L; P < .001). Patients with a higher hsCRP experienced a higher rate of inhospital complications. After adjusting for potential confounders, hsCRP >6.50 mg/L was significantly associated with the occurrence of CIN. Preprocedural hsCRP levels are significantly related to the incidence of CIN in patients with STEMI undergoing p-PCI.
Keywords
Current treatment guidelines for acute myocardial infarction (AMI) recommend that the early opening of the infarct-related artery is the key to successful treatment. In recent years, large-scale clinical trials reported higher patency rate and event-free survival rate of emergency percutaneous coronary intervention (PCI) compared with thrombolysis. However, contrast-induced nephropathy (CIN) continues to be a common major adverse side effect of cardiac catheterization and is associated with short- and long-term morbidity and mortality. 1,2 Many studies have shown that patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary PCI (p-PCI) had higher incidence of CIN than patients undergoing nonemergency catheterization. The pathogenesis of CIN is not completely understood. High-sensitivity C-reactive protein (hsCRP) is a marker of systemic inflammation that has the potential to become a diagnostic and therapeutic target for CIN prediction and management. Few studies have assessed the relationship between CRP and progression of CIN. 3,4 However, no studies have established the prognostic value of preprocedural hsCRP for CIN in patients with STEMI undergoing p-PCI. Therefore, we studied the impact of preprocedural hsCRP on the incidence of CIN in patients with STEMI undergoing p-PCI.
Patients and Methods
Study Design and Patient Population
We retrospectively studied patients with STEMI consecutively referred to the catheterization laboratory for p-PCI in 2 large hospitals (Beijing Anzhen Hospital and Beijing Daxing Hospital, Capital Medical University). The inclusion period was January 2007 to October 2012 for the Daxing Hospital and January 2009 to October 2012 for the Anzhen Hospital. During these time frames, hsCRP was routinely measured at admission in all patients with STEMI.
Patients with STEMI were required to have (1) continuous chest pain upon presentation refractory to nitrates and lasting for ≥30 min; (2) ST-segment elevation of ≥0.2 mV in ≥2 contiguous precordial leads or ≥0.1 mV in ≥2 contiguous limb leads, or new (or presumably new) left bundle branch block on admission electrocardiogram; and (3) presentation within the first 12 hours from index pain.
Primary PCI and Laboratory Determinations
All patients were taken to the catheterization laboratory on arrival, and p-PCI was performed by a 24-hour on-call interventional team. All patients were pretreated with aspirin 300 mg + clopidogrel 300 to 600 mg loading dose during transportation to the hospital, or these drugs were administered in the emergency ward. The contrast dose was left to the discretion of the interventional cardiologist. All patients received nonionic, low osmolar contrast media (Iohexol). After p-PCI, the patients received isotonic (0.9%) saline intravenously, 1 mL/kg/h for 6 to 12 hours. In patients with left-ventricular ejection fraction (LVEF) of <40% or overt heart failure, the hydration rate was reduced to 0.5 mL/kg/h. The use of adrenergic blocking agents, angiotensin-converting enzyme inhibitors, platelet glycoprotein IIb/IIIa receptor inhibitors (tirofiban hydrochloride), diuretics, intraaortic balloon pump support, or inotropic drugs was left to the discretion of the interventional and coronary care unit cardiologists. During hospitalization, medications were changed as needed at the discretion of the cardiologist responsible for the patient.
Duration of chest pain was estimated by the time interval between chest pain onset and the time of arrival to the emergency room. Multivessel disease was defined as the presence of >2 major epicardial coronary arteries or their major branches with stenosis of ≥70%, assessed during initial coronary angiography.
The serum creatinine (sCr) concentration and hsCRP were measured in all patients in the emergency ward (prior to p-PCI). The hsCRP was tested with a Beckman Coulter Image immunobiochemistry system, USA using nephelometry. Creatinine clearance was estimated by the Cockcroft-Gault formula, 5 and the glomerular filtration rate (eGFR) was estimated by the simplified modification of diet in renal disease equation. 6,7
Exclusion Criteria
Patients were excluded if they had history of severe heart failure, severe renal failure requiring renal replacement therapy, or definite myocardial infarction (MI).
Study End Points and Definitions
The primary end point was the development of CIN, defined as an increase in sCr of ≥25% or 0.5 mg/dL over the baseline value within 3 days after administration of contrast medium. 8,9
Inhospital major adverse cardiac events (MACEs) included death, life-threatening cardiac arrhythmias with a need for resuscitation or pacemaker implantation, angina with electrocardiogram changes, recurrent MI, and repeated urgent revascularization. Recurrent MI was defined as a new increase in creatine kinase-MB fraction of more than 3 times the upper limit of normal, associated with chest pain and/or electrocardiographic changes. Urgent revascularization was defined as a repeated coronary revascularization performed within 48 hours of the index revascularization procedure.
Composite MACEs were cardiac death, angina, life-threatening cardiac arrhythmias, recurrent MI, and repeated urgent revascularization.
Statistical Analysis
Categorical data are presented as frequencies (percentages); continuous data are presented as mean value ± standard deviation. Differences between the means were compared by unpaired t test when the variables showed normal distribution or by the Mann-Whitney U test when they did not. We used the chi-square test to compare the categorical variables or the Fisher exact test, as appropriate. Receiver–operating characteristic (ROC) analysis was conducted to determine the cutoff value of hsCRP for predicting CIN. The significant variables in the univariate analysis were introduced in a multivariate logistical regression model to obtain the predictive variables of adverse outcomes. A P value < .05 (2 sided) was considered significant. Data were analyzed with SPSS 13.0 (Chicago, Illinois).
Results
As defined by the inclusion and exclusion criteria, we enrolled 1670 patients with STEMI who were treated with p-PCI. Patients with missing hsCRP (n = 218) data were excluded from the study. Final analysis was therefore performed on 1452 patients. In all, 212 (14.6%) patients developed CIN. The overall inhospital mortality rate was 4.5% (65 patients).
Quartiles of hsCRP for the study population were Q1 (<3.0 mg/L), Q2 (3.0-5.9 mg/L), Q3 (5.91-11.4 mg/L), and Q4 (>11.4 mg/L). Baseline clinical characteristics are shown in Table 1. Age, LVEF, Killip >1 on admission, and eGFR were significantly different between the lowest hsCRP quartile and the other quartiles; other variables were not significantly different. The mean hsCRP value was significantly higher in patients with CIN than in those without CIN (12.5 ± 8.4 vs 6.8 ± 4.2; P < .001). Univariate analysis revealed CIN incidence was significantly associated with hsCRP, with 7.4% for quartile Q1 (<3.0 mg/L), 12.6% for Q2 (3.0-5.9 mg/L), 16.9% for Q3 (5.91-11.4 mg/L), and 21.5% for Q4 (>11.4 mg/L; P < .001; Figure 1). Patients with a higher hsCRP experienced a higher rate of inhospital complications, including inhospital death (1.7%, 4.1%, 5.8%, and 7.2% for Q1-Q4, respectively; P = .003; Table 2 and Figure 2), composite MACEs (10.7%, 18.6%, 23.3%, and 29.5% for Q1-Q4, respectively; P trend < .001), and hospital days (6.8 ± 3.8, 7.2 ± 4.1, 7.8 ± 4.2, 8.4 ± 4.3 for Q1-Q4, respectively; P < .001; Table 2).
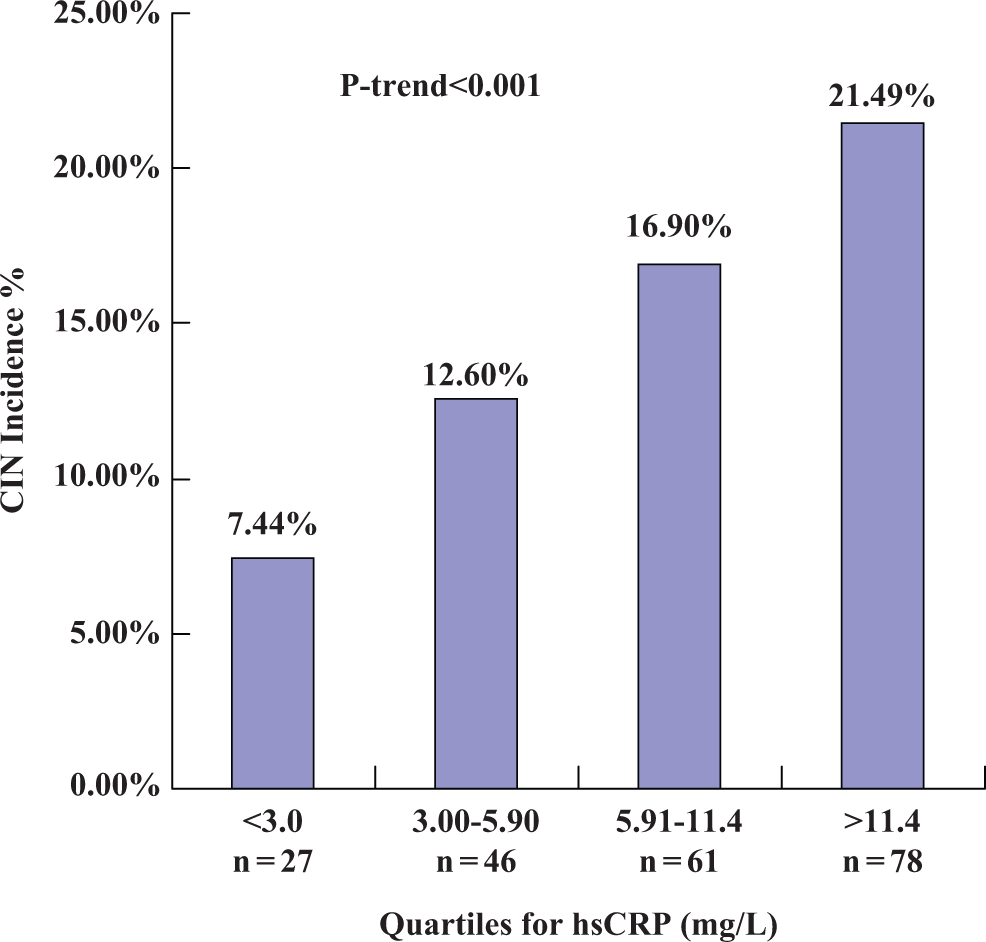
Relationship between hsCRP and incidence of CIN. The association between preprocedural hsCRP and incidence of CIN was significant (P < .001, overall and for trend). hsCRP indicates high-sensitivity C-reactive protein; CIN, contrast-induced nephropathy.
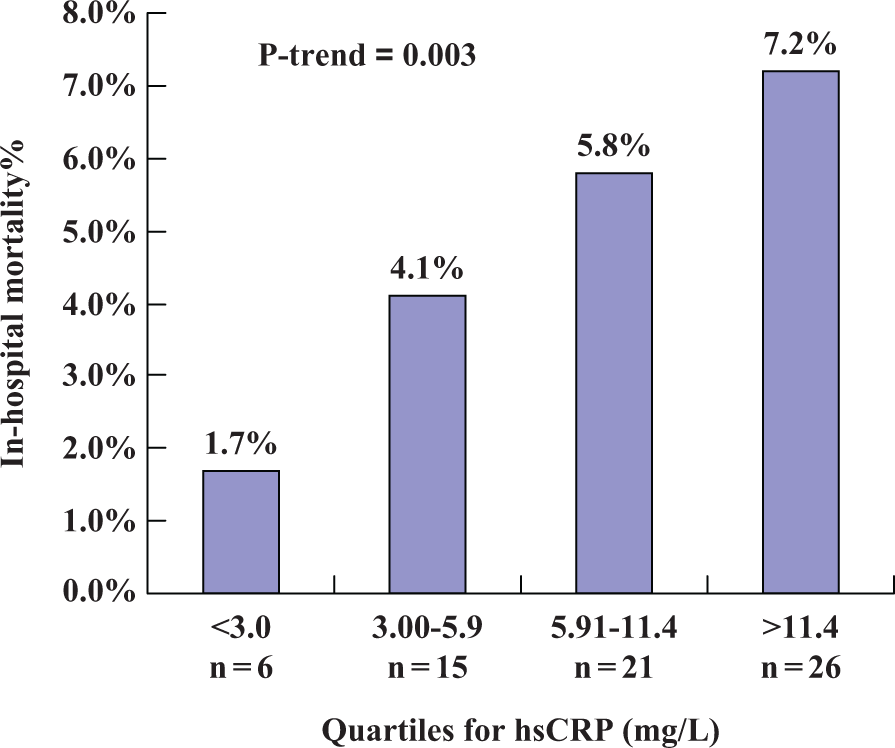
Relationship between high-sensitivity C-reactive protein (hsCRP) and inhospital mortality. The association between preprocedural hsCRP and inhospital mortality was significant (P = .003, overall and for trend).
Baseline Clinical Characteristics.a,b
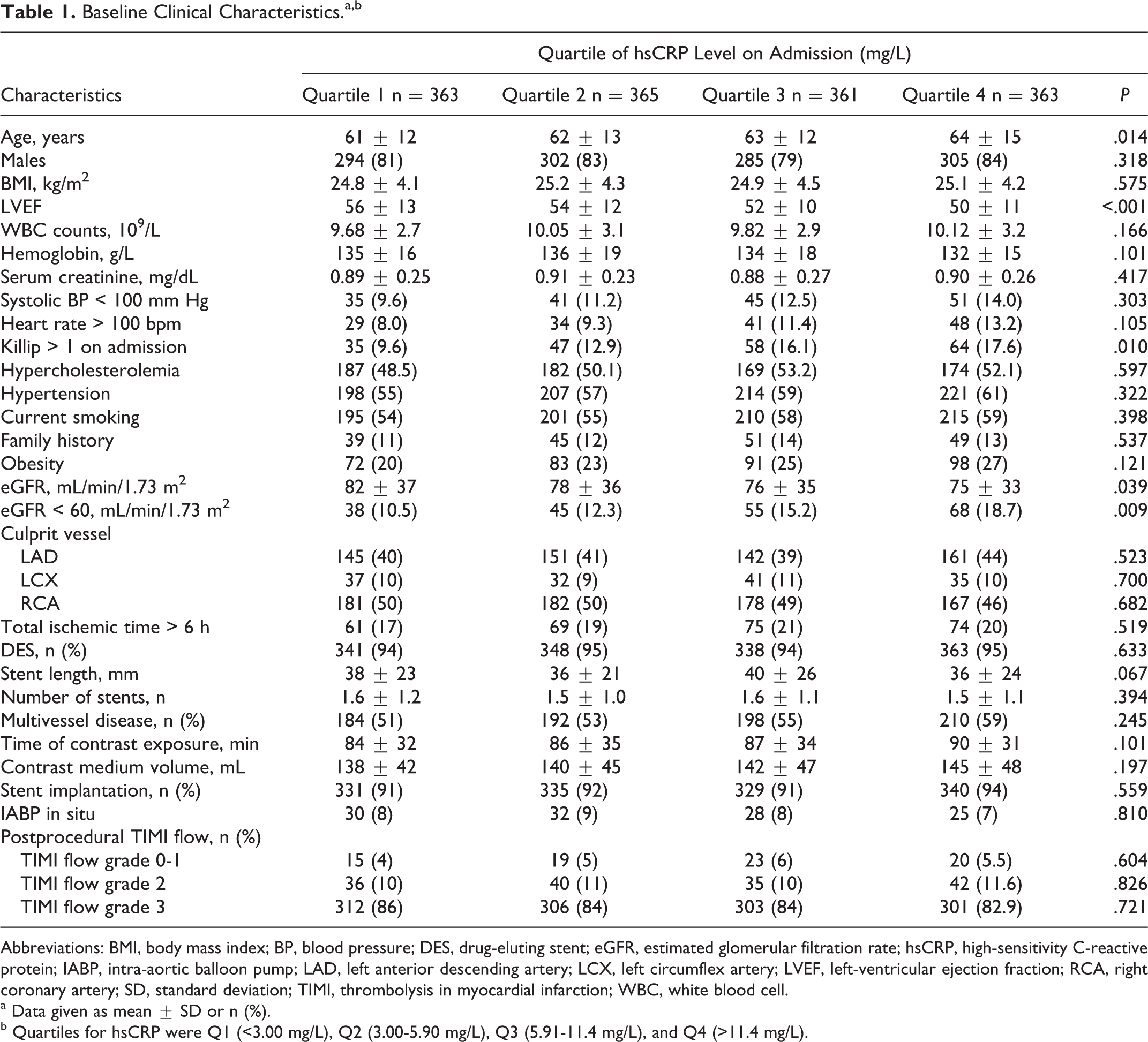
Abbreviations: BMI, body mass index; BP, blood pressure; DES, drug-eluting stent; eGFR, estimated glomerular filtration rate; hsCRP, high-sensitivity C-reactive protein; IABP, intra-aortic balloon pump; LAD, left anterior descending artery; LCX, left circumflex artery; LVEF, left-ventricular ejection fraction; RCA, right coronary artery; SD, standard deviation; TIMI, thrombolysis in myocardial infarction; WBC, white blood cell.
a Data given as mean ± SD or n (%).
b Quartiles for hsCRP were Q1 (<3.00 mg/L), Q2 (3.00-5.90 mg/L), Q3 (5.91-11.4 mg/L), and Q4 (>11.4 mg/L).
Inhospital Clinical Complications and Hospital Days Based on hsCRP.a
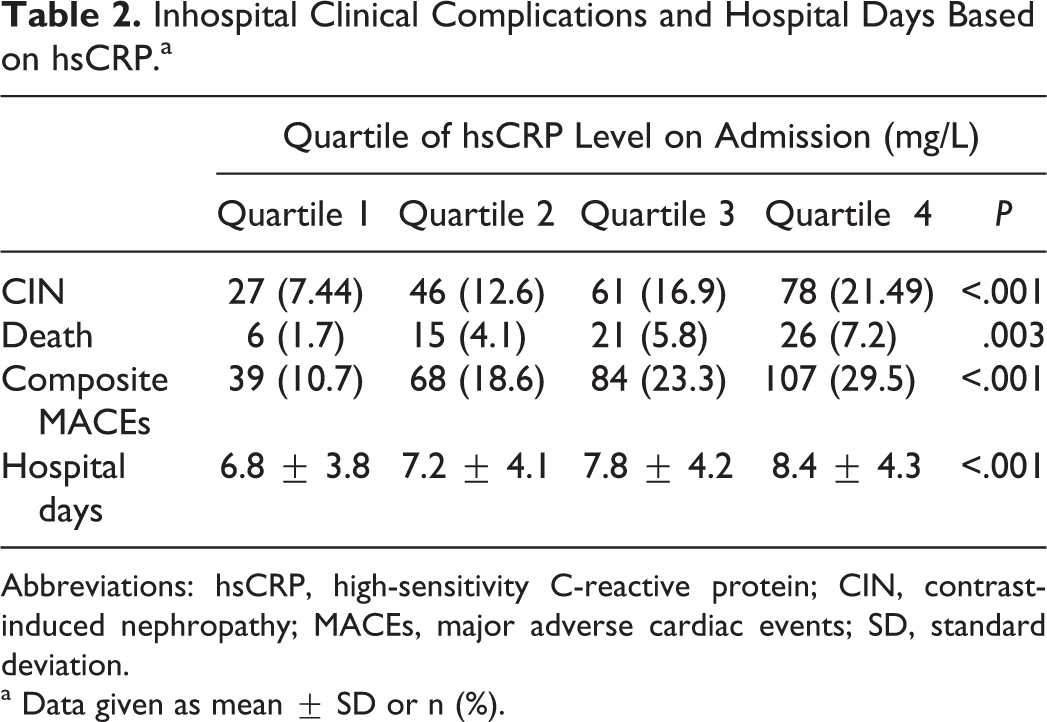
Abbreviations: hsCRP, high-sensitivity C-reactive protein; CIN, contrast-induced nephropathy; MACEs, major adverse cardiac events; SD, standard deviation.
a Data given as mean ± SD or n (%).
As shown in Table 3, inhospital mortality was significantly higher in patients with CIN than in those without (10.8% vs 3.4%, P < .001); CIN was associated with higher occurrence of repeated revascularization (P = .031) and angina (P = .004). Composite MACEs occurred in 29.7% of the patients with CIN and in 19.0% of the patients without CIN (P < .001). Patients with CIN had a longer hospital stay compared to patients without CIN (P < .001). The ROC curve analysis showed that at a cutoff of 6.50, the value of hsCRP exhibited 75.6% sensitivity and 61.4% specificity for detecting CIN (C statistic of 0.62). Univariate logistic regression indicated that hsCRP > 6.50 was a highly significant predictor of CIN (odds ratio [OR] = 5.82; 95% confidence interval [95% CI], 2.04-14.48). Multivariate logistic regression was performed including the variables hsCRP > 6.50, age > 65 years, LVEF < 40%, Killip > 1 on admission, and baseline eGFR < 60 mL/min, and it showed that hsCRP >6.50 was significantly associated with the occurrence of CIN (OR = 5.24; 95% CI, 1.42-12.66).
Inhospital Clinical Complications and Hospital Days.a
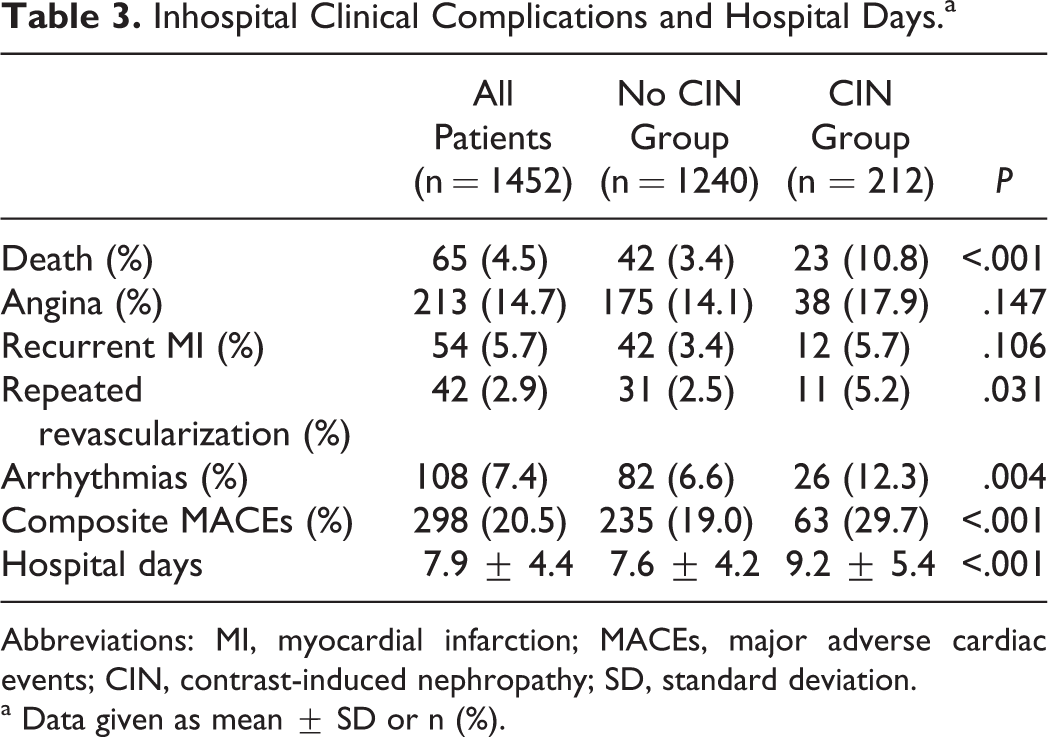
Abbreviations: MI, myocardial infarction; MACEs, major adverse cardiac events; CIN, contrast-induced nephropathy; SD, standard deviation.
a Data given as mean ± SD or n (%).
Discussion
The principal finding of our study was the demonstration that preprocedural hsCRP levels are related to the incidence of CIN in patients with STEMI undergoing p-PCI. We also found that preprocedural hsCRP >6.50 mg/L was an independent and significant predictor of CIN after p-PCI. Moreover, we also showed a high level of hsCRP was strongly associated with inhospital mortality and composite MACEs.
The risk of CIN after percutaneous coronary revascularization in the general population is low (0.6-3.0%). 9 However, in the setting of STEMI, the incidence of CIN can be considerably higher. Rihal et al 2 identified AMI as an independent predictor of CIN after cardiac catheterization. Marenzi et al 1 reported an incidence of CIN of 19% in 208 patients who had undergone primary angioplasty. Bouzas-Mosquera et al 10 reported an incidence of CIN of 12.0%. The CIN incidence in our study (14.6%) was similar to the results from other studies. 1,10 Contrast-induced nephropathy is associated with an increased inhospital morbidity and mortality 11 In our study, poor prognosis for clinical outcome in patients with CIN undergoing p-PCI was also observed. Compared to patients without CIN, those with CIN had significantly higher inhospital mortality (10.8 vs 3.4%, P < .001) and incidence of composite MACE (29.7 vs 19.0%, P < .001). Although the exact mechanisms of CIN are yet to be fully elucidated, several causes have been described. Increased adenosine, endothelin, and free radical-induced vasoconstriction and reduced nitric oxide and prostaglandin-induced vasodilatation have been observed. 12 These mechanisms cause ischemia in the deeper portion of the outer medulla, an area with high oxygen requirements and remote from the vasa recta supplying the renal medulla with blood. 12 Contrast agents also have direct toxic effects on renal tubular cells, causing vacuolization, altered mitochondrial function, and apoptosis. 13
The CRP along with interleukin 6 (IL-6) and other cytokines/adipokines have been found to directly promote endothelial cell inflammation and atherosclerotic processes. 14 Oberg et al 15 thought that elevations in biomarkers of inflammation such as CRP and IL-6 were present earlier in the course of kidney disease than previously recognized but suggested that they are not necessarily well correlated with GFR. In baseline data from the Cardiovascular Health Study, levels of CRP and IL-6 were found to be significantly higher in patients with renal insufficiency compared to patients with normal kidney function. 16 The mechanism underlying the association between hsCRP and the risk of CIN has not yet been elucidated. Many factors may be involved. First, close interrelation between glucose metabolism and inflammation has been shown in several studies. 17
Elevated blood glucose levels occur commonly in patients with AMI; glucose at admission are independently associated with elevated levels of CRP in men during the early stage of STEMI. 18 High levels of blood glucose, even in levels within the normal range, promote inflammation in the vascular cells. 19,20 Elevated preprocedural glucose was associated with greater risk of CIN in patients who undergo coronary angiography in the setting of AMI. 21 So, we think that elevated hsCRP and hyperglycemia may jointly contribute to the development of CIN. Second, hsCRP is an inflammatory biomarker and a growing body of evidence supports the active role of hsCRP in the devolvement of vascular damage. The CRP caused downregulation of endothelial nitric oxide synthase 22,23 and was involved in oxidative stress and generation of reactive oxygen species. Third, Xinwei et al 24 found that pretreatment with simvastatin 80 mg before PCI decreased the occurrence of CIN compared with simvastatin 20 mg, and the benefit was associated with the lowering of hsCRP. Quintavalle et al 25 observed that a single high loading dose of atorvastatin administered within 24 hours before contrast media exposure was effective in reducing the rate of CIN. Based on these evidences, we think that hsCRP may play an important role in the development of CIN. We did not use statin loading.
An increased plasma concentration of the acute-phase reactant hsCRP reflects activation of systemic inflammation. The associates of the elevated CRP level with AMI might have an impact on the instability of the culprit coronary lesion. The CRP was predictive of adverse cardiovascular outcome. 26 Schoos et al indicated that preprocedure hsCRP predicts outcome after p-PCI in patients with STEMI. 27 Delhaye et al showed that preprocedural high hsCRP levels before coronary stent implantation were associated with the risk of death or MI but are not related to stent-related complications. 28 Marsik et al reported that patients with CRP concentrations >5 mg/L at the time of hospital admission had a 50% to 330% increase in risk of death from any cause. 29 Our findings also showed a high level of hsCRP was strongly associated with inhospital mortality and composite MACEs.
Patients with STEMI undergoing p-PCI are at higher risk of CIN than those undergoing elective interventions. Our goal should be to recognize risk factors for CIN. Patients with chronic renal failure, diabetes mellitus, congestive heart failure, older age, hypotension, and anemia are at particular risk. 13 Current evidence supports preprocedural hydration preferably with intravenous administration of 0.9% isotonic saline or an isotonic sodium bicarbonate solution. But in patients with STEMI undergoing preprocedural p-PCI, a high-loading dose of a statin may decrease the risk of CIN, inhospital mortality, and composite MACEs, especially in patients with high hsCRP levels, which provide new insights into the prevention of CIN in clinical emergency conditions.
Study Limitations
First, this is not a randomized trial but a retrospective evaluation. Second, blood samples for hsCRP were obtained at the time of admission; we did not observe the serial changes in hsCRP concentration after p-PCI. Third, many laboratory data are missing and a longer period of follow-up is necessary to determine the long-term prognostic value of preprocedural hsCRP.
Conclusions
Preprocedural hsCRP levels are markedly related to the incidence of CIN in patients with STEMI undergoing p-PCI. Higher baseline hsCRP level (>6.50 mg/L) was an independent and significant predictor of CIN after p-PCI. A high level of hsCRP was strongly associated with inhospital mortality and composite MACE.
Footnotes
Authors’ Note
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive license (or nonexclusive for government employees) on a worldwide basis to the publishing group and its licensees to permit this article (if accepted) to be published to exploit all subsidiary rights, as set out in our license.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.