
Abstract
We determined the role of anxiety level on radial artery spasm during transradial coronary angiography. Eighty-one patients who had an indication for coronary angiography were enrolled. Radial artery vasospasm was determined by addressing 5 signs: persistent forearm pain, pain response to catheter manipulation, pain response to sheath withdrawal, difficult catheter manipulation after being “trapped” by the radial artery, and considerable resistance on withdrawal of sheath. Radial spasm defined as at least 2 of the 5 signs. The Hamilton Anxiety scale questionnaire was used to determine the level of anxiety. Vasospasm was observed in 19.1% of the patients. Anxiety score was significantly higher in women (11.1 ± 7.2 vs 17.6 ± 7.3; P < .001). Vasospasm was significantly correlated with female sex (P < .001, r = .43) and anxiety score (P = .007, r = .29). Female sex was associated with higher anxiety scores (P < .001, r = .43). In conclusion, higher anxiety scores and female sex are important risk factors for radial artery vasospasm.
Introduction
The radial artery approach is increasingly used for coronary procedures due to its advantages like early mobilization and patient comfort, but radial artery vasospasm remains a problem. 1 –3 Similar efficacy and safety profile compared with the femoral approach resulted in increased use of this technique. This is especially relevant for patients with high bleeding risk such as those receiving intensive antiplatelet, anticoagulant therapies, and fibrinolytics and have a need for emergency coronary intervention. Furthermore, the presence of ulnar artery collaterals decreases the risk of distal embolic and ischemic complications. Many types of coronary, cerebral, vertebral, and renal interventions can be carried out using the radial approach. 4 –7
The radial artery is more vulnerable to vasospasm than other arterial entry sites, since it is rich in smooth muscle and has a comparatively small diameter. The most frequent complication encountered in clinical practice is arm pain due to vasospasm. The incidence of vasospasm is reported as 7.8% to 25%. 4,8 –12 These rates are high for a diagnostic procedure and imply the need for risk factor determination before the procedure. Currently, the following variables are identified as risk factors for radial vasospasm: female sex, age, radial artery diameter, and the number of interventions performed. 4,8 –12
Various psychiatric disorders are associated with cardiovascular (CV) diseases. Depressive mood and anxiety are associated with increased rates of CV events. Subclinical CV pathologies are seen more frequently in patients with anxiety. 13
Cardiovascular events are capable of triggering psychiatric diseases. In addition, another theory is that a common pathology may trigger both CV events and psychiatric disorders. 14
We investigated the relationship between vasospasm during radial artery approach and. To our knowledge, no published study investigated this relationship.
Methods
The study was performed in the Department of Cardiology, Gaziantep University School of Medicine, Gaziantep, Turkey. A total of 81 patients were consecutively enrolled between January and June 2012. All patients had an indication for coronary angiography (eg, unstable angina and angina resistant to medical therapy). We did not include patients with acute myocardial infarction. The Allen test was satisfactory for each patient. Our clinic is a tertiary center where an average of 3500 coronary angiographies or interventions are performed each year, and we have an increasing experience with the radial approach for nearly 8 years. The percentage of radial approach in our center is about 20% of all coronary interventions. All procedures were performed by operators experienced with radial interventions (radial approach used in >40% of their cases). Approval of local ethics committee was obtained before starting the study.
Method Used for Radial Angiography
The access site was anaesthetized with lidocaine and then arterial puncture was performed using a 5F puncture set (PreludeTM sheath, Utah, USA). In order to prevent vasospasm and thromboembolic events, 200 μg verapamil and 3000 U heparin were injected into the radial artery along the sheath. Immediately after the procedure, the sheath was removed and the puncture site was compressed. The compression was reduced after l to 2 hours and completely released 4 to 6 hours after the procedure. Sedative agents are not routinely used for coronary angiography, and this usually depends on physician preference. We do not use sedative agents routinely and also did not use these agents throughout the entire study. The radial artery approach was unsuccessful in 3 patients due to severe radial vasospasm; the procedure was completed by the femoral route in these patients.
Clinical Definition of Radial Artery Spasm
Operator-assessed radial artery spasm was determined based on a questionnaire addressing 5 signs: persistent forearm pain, pain response to catheter manipulation, pain response to sheath withdrawal, difficult catheter manipulation after being “trapped” by radial artery, and considerable resistance on withdrawal of the sheath. Patients who had at least 2 of these 5 signs were diagnosed as having clinical radial artery spasm. 9
Determining the Anxiety Score
All patients were evaluated by a psychiatrist using the Hamilton Anxiety scale (HAM-A) 1 hour before the angiography. This questionnaire is used to evaluate the level of anxiety, distribution of signs and to determine the severity of anxiety. The HAM-A consists of 14 questions examining both mental and physical signs. Every item has a score between 0 and 4, with a total between 0 and 56. Turkish validity and reliability studies of the scale were performed. 15
Statistical Analysis
Data were analyzed using SPSS (Statistical Package for Social Sciences) version 15.0. Continuous variables were reported as mean ± standard deviation (SD). For bivariate analysis, when the variables were parametric, the Student t test was used. The analysis of correlation between radial artery spasm and other risk factors was performed using Pearson or Spearman correlation methods. A 2-sided P < .05 was considered significant.
Results
The male to female ratio was 45:36. Mean age for men and women were 55.9 ± 12 (range 30-78) and 55.9 ± 10 (35-79) years, respectively. Mean anxiety score of the whole study population was 14.0 ± 7.9 (2-31). The score was 17.6 ± 7.3 (2-31) for women and 11.1 ± 7.2 (2-30) for men. Anxiety score was significantly higher in women (P < .001; Table 1).
Comparison of Male and Female Patients Who Underwent Radial Coronary Angiography.
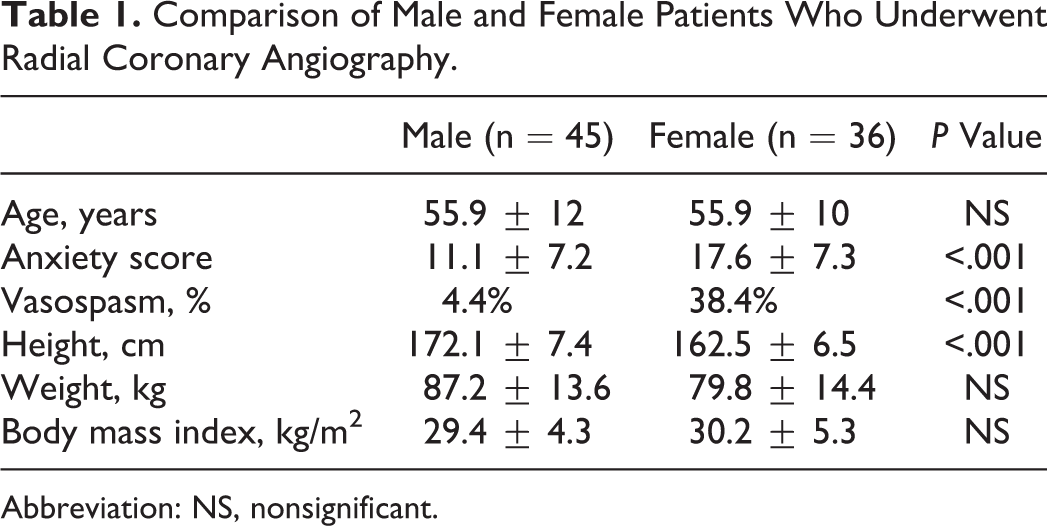
Abbreviation: NS, nonsignificant.
Vasospasm was observed in 19.1% of the population. The rate of vasospasm was 4.4% for men and 38.4% for women (P < .001). Vasospasm was strongly correlated with female sex (P < .001, r = .43). There was also a strong correlation between vasospasm and higher anxiety score (P = .007, r = .29). Female sex was associated with higher anxiety scores (P < .001, r = .43). However, age was associated neither with anxiety score nor with vasospasm (P > .05). Multivariate regression analysis revealed that female sex and high anxiety score independently predict radial artery spasm (P = .001 and P = .017, respectively).
Discussion
We evaluated the association between the degree of anxiety and vasospasm during transradial procedures. The rate of vasospasm among patients undergoing coronary angiography via radial artery route was 19.1%. Vasospasm was more frequent in female patients and significantly correlated with the anxiety score.
Recently a comprehensive consensus document on the increasing role of radial approach in percutaneous CV interventions was published. 16 However, arm pain due to vasospasm is an important consideration. Intensive sympathetic alpha-receptor density found in the radial artery is accepted as the primary determinant for vasospasm. 17 In addition, dysregulation of serotonin and nitric oxide levels triggered by endothelial dysfunction contribute to vasospasm. 10 Symptoms seen in patients with anxiety are triggered by increased sympathetic tone, which leads to increased circulating levels of catecholamines. 18 –20 Our study suggests that higher anxiety score is an important risk factor for radial artery vasospasm possibly triggered by increased sympathetic tone in patients with high anxiety scores.
Studies revealed that patients with psychiatric disorders demonstrate anomalous blood flow properties related to endothelial dysfunction. 10,13,14 Spasmolytic cocktails are recommended to prevent vasospasm. The SPASM trial (Prevention of arterial spasm during percutaneous coronary interventions through radial artery: The SPASM Study) showed that verapamil and molsidomin significantly reduced the rates of vasospasm in patients undergoing coronary angiography via the radial route. 21 Vefali et al concluded that the procedural success rate of radial approach is similar to that of the femoral approach. 22 Despite not using any vasodilator agents, they reported that only 1 patient experienced vasospasm among 487 patients. However, the operators in this study routinely used premedication sedation with midazolam.
A recent study demonstrated that preprocedural administration of opioid analgesia combined with sedation (fentanyl and midazolam) significantly reduced the incidence of radial artery spasm during transradial procedures. 23 Although these investigators did not assess the anxiety score, their study implicates a possible role of sedation in preventing radial artery spasm during the procedure. This study supports our findings that underscore the relationship between high anxiety score and radial artery spasm.
In addition, minimally invasive procedures like endoscopic procedures, dental interventions, coronary angiography, and pediatric echocardiography are performed with greater success rates with the help of midazolam as an anxiolytic agent. 24,25 Along with the sedative effect, midazolam also suppresses sympathetic reflex response in animal models. 26,27 We used calcium channel blockers before the procedure in our study. Persistently high basal levels of catecholamines seen in anxiety facilitate radial artery vasospasm, which is rich in alpha-receptors, and also reduce the effectiveness of calcium channel blockers in preventing vasospasm.
Population-based studies revealed that anxiety is seen 2 times more frequently in females. 28,29 In our study, anxiety score was consistently higher in female participants and accordingly, vasospasm was more frequent in women. The SPASM trial also documented that female sex and younger age were independent predictors of vasospasm in transradial procedures. 21 Higher frequency of vasospasm seen in women was attributed to increased anxiety scores in the present study. In contrast to previous studies, age was not associated with vasospasm in our study. This may be related to the finding that age was not associated with anxiety score.
Findings from previous studies suggest that small radial artery diameter was also associated with vasospasm. Small radial artery diameter observed in women also has a role in higher rates of vasospasm in this gender. 30,31 Vasospasm risk is reduced with smaller diameter cannulations 32 ; however, percutaneous coronary interventions performed with greater diameter catheters provide greater success rates. 33
Anxiety score across different populations varies considerably. Sartorius et al studied 25 000 patients from 15 different countries and found that the prevalence of anxiety was 10.5%. 34 Different rates of vasospasm reported in the literature during radial procedures can also be explained in part by different populations and ethnicity. 35 Despite the fact that vasospasm was more common among subgroups with high anxiety score, it remains to be established whether anxiety was the causative factor for vasospasm
Study Limitations
Our study was conducted in a single center with relatively small number of patients. However, the present study is a pilot study and larger scale controlled trials using anxiolytics need to be preformed to define the relation between anxiety and vasospasm. According to our findings, premedication with anxiolytic agents may improve vasospasm. We are currently conducting a trial testing this hypothesis. We did not evaluate the plasma levels of catecholamines. Another limitation is that we did not take into consideration the radial artery diameter as a potential risk factor for vasospasm. Radial artery diameter is smaller in female patients, which might explain why this gender is at a higher risk of vasospasm.
In conclusion, higher anxiety scores and female sex are risk factors for radial artery vasospasm during percutaneous radial interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.