
Abstract
We investigated the association between coronary artery ectasia (CAE) and Neutrophil-to-lymphocyte ratio (NLR), an indicator of the inflammatory state. The study population included 434 patients (247 males, mean age 62 ± 10 years) including 230 patients with isolated CAE and 104 patients with coronary artery disease and 100 patientss with normal coronary arteries. The NLR was measured at admission and 30 days after coronary angiography in all the patients. The NLR was significantly higher in patients with CAE than those with normal coronary arteries (2.2 ± 0.6-1.3 ± 0.6, P < .001). Linear regression analyses revealed that NLR (coefficient β = −.61, P < .001) was significantly associated with severity of CAE. The NLR is significantly higher in patients with CAE compared to controls with normal coronary arteries, and NLR is associated with severity of CAE.
Introduction
Coronary artery ectasia (CAE) is defined as abnormal dilatation of a coronary artery luminal diameter to ≥1.5 times wider than the adjacent normal segment. 1 The reported prevalence of CAE varies from 0.3% to 5% among patients undergoing coronary angiography and 1.4% to 4.9% in postmortem studies. 2 –4 One-third of CAEs have been considered to be congenital in origin, whereas as 20% to 30% of CAEs have been described in association with inflammatory diseases. 5 Infectious diseases, toxic, and traumatic causes also play role in etiology of CAE. 6 It has been shown that histology of arterial wall is similar in both CAE and atherosclerosis except loss of musculoelastic arterial wall that is seen in CAE. 7 The mixed etiopathogenesis of CAE suggests that CEA is a syndrome with various components beyond a single-arterial disease. Ectatic coronary arteries may be associated with potential significant complications due to distal embolization as a result of stasis in the dilated segments and impaired coronary flow. 7
Although, atherosclerosis is the suggested etiologic factor in one-half of the patients with CAE, the underlying pathogenic mechanisms of CAE still remain unclear. 6 Inflammation is one of the suspected mechanisms playing role in pathogenesis of CAE. Although there are many data reporting the relation between inflammation and atherosclerosis, evidence indicating the role of inflammation in ethiopathogenesis of CAE is weaker. 8 –11 Therefore, we aimed to investigate whether there is an association between neutrophil-to-lymphocyte ratio (NLR) and CAE.
Materials and Methods
Patient Selection
A total of 434 patients were consecutively selected among patients who underwent coronary angiography for suspected coronary artery disease (CAD) in the catheterization laboratory of the Kayseri Education and Research Hospital between August 2011 and December 2012. The CAE was defined as localized coronary dilatation exceeding the diameter of normal adjoining segments by 1.5 times. The study population consisted of 3 groups including 230 patients with isolated CAE, 104 patients with CAD, and 100 patients with normal coronary arteries (NCA). Patients with a history of acute coronary syndrome, heart failure, previous percutaneous coronary intervention, coronary artery bypass grafting surgery history, active infectious disease, inflammatory or immunologic disease, cirrhosis, peripheral arterial disease, chronic obstructive pulmonary disease, chronic kidney disease and malignancy were excluded from this study. Also, patients using angiotensin converting enzyme inhibitors and angiotensin receptor blockers, statins or fibric acid-derivative drugs, and hepatotoxic drugs were excluded.
Biochemical Analysis
Fasting blood samples (12 hours) were collected on the day of admission to the hospital. All measurements were performed within 30 minutes after blood collection. Complete blood count (Cell-Dyn 3700 System; Abbot, Abbott Park, Illinois), fasting blood glucose, creatinine levels, and lipid profile were analyzed for all patients using Beckman-Coulter AU 2700 (Australia Pty Ltd, Sydney, Australia). High-sensitivity C-reactive protein (hsCRP) level was analyzed using BN-II nephelometer (Siemens, Marburg, Germany). For NLR measurement, complete blood count was repeated 30 days after coronary angiography, and the average of 2 measurements was used for statistical analysis.
Coronary Angiography
Quantitative coronary angiography was performed using the Judkins technique by 2 experienced interventional cardiologists unaware of the clinic and laboratory results of the patients. Angiographic images were then interpreted by these interven-tionalists. The CAE was defined as localized coronary dilatation exceeding the diameter of normal adjoining segments by 1.5 times. Significant CAD was defined as >50% stenosis in at least 1 coronary artery. The complexity of CAE was graded as follows: type 1, diffuse ectasia of ≥2 coronary arteries; type 2, diffuse ectasia in 1 coronary artery and localized ectasia in another coronary artery; type 3, diffuse ectasia of 1 coronary artery; and type 4, localizsed or segmental ectasia of only 1 coronary artery. 12
Statistical Analysis
Statistical analysis was performed using the SPSS software version 15 (SPSS Inc., Chicago, Illinois, USA). Continuous variables were presented as mean ± standard deviation; categorical variables were defined as percentage. The variables were investigated using Kolmogorov-Smirnov test to determine whether or not they are normally distributed. Continuous variables were compared using the 1-way analysis of variance and the post hoc Tukey test. The chi-square test was used for univariate analysis of the categorical variables. Linear regression analysis was performed to identify the significance of relation between CAE and several variables. A 2-tailed P < .05 was considered significant.
Results
The clinical characteristics and laboratory parameters of the study population are listed in Table 1. There were no significant differences between patients with CAE, CAD, and controls in terms of age, gender, presence of hypertension and diabetes, smoking habit, fasting glucose, creatinine, hemoglobin, platelet count, total cholesterol, and plasma triglyceride levels. Low-density lipoprotein cholesterol level was significantly higher in patients with CAD than in patients with NCA (132 ± 41 to 116 ± 44 mg/dL, P = .01) and high-density lipoprotein cholesterol level was significantly lower in patients with CAD than in patients with CAE and NCA (35 ± 6 to 40 ± 11 and 39 ± 9 mg/dL, P = .001 and .009, respectively). There were 29 (13%) patients with type 1 ectasia, 60 (23%) patients with type 2 ectasia, 54 (26%) patients with type 3 ectasia, and 86 (38%) patients with type 4 ectasia (Table 1).
Clinical and Laboratory Features of the Study Groups.
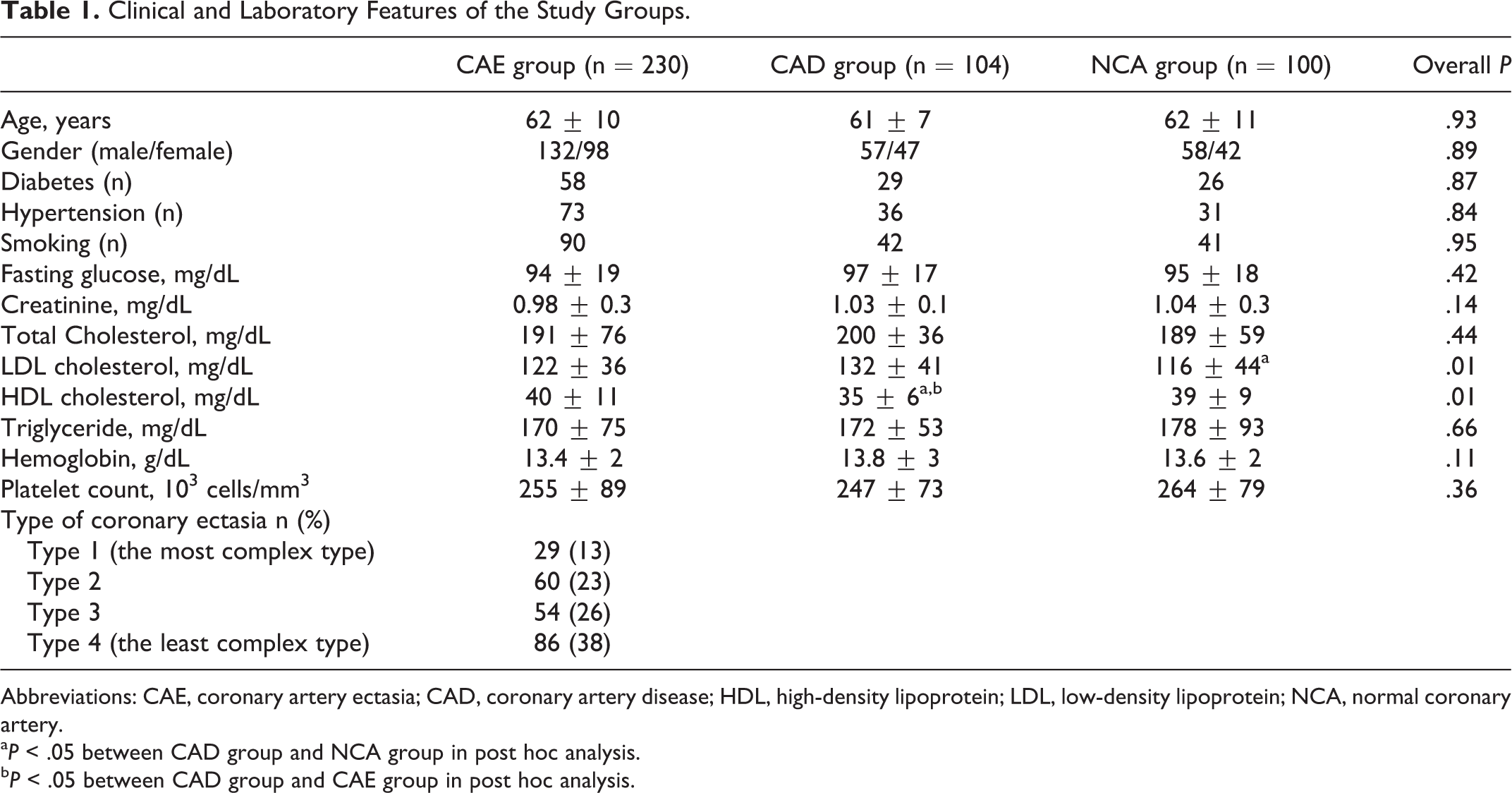
Abbreviations: CAE, coronary artery ectasia; CAD, coronary artery disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NCA, normal coronary artery.
a P < .05 between CAD group and NCA group in post hoc analysis.
b P < .05 between CAD group and CAE group in post hoc analysis.
Post hoc analysis revealed that, white blood cell (WBC) count (8.1 ± 1.9 × 103 to 6.9 ± 1.3 × 103/µL, P < .001), neutrophil count (4.6 ± 2.1 × 103/µL to 2.5 ± 1.3 × 103/µL, P < .001), and hsCRP levels (2.9 ± 1 and 2.7 ± 0.8 to 1.7 ± 0.7 mg/L, P < .001) were significantly higher in patients with CAE and CAD, compared toh patients with NCA (Table 2). Also, NLR (2.2 ± 0.6 and 2.1 ± 0.6 to 1.3 ± 0.6, P < 0001) was significantly higher in patients with CAE and CAD compared to patients with NCA (Figure 1). However, there were no significant differences between CAE group and CAD group regarding WBC count, neutrophil count, hsCRP levels, and NLR (Table 2).
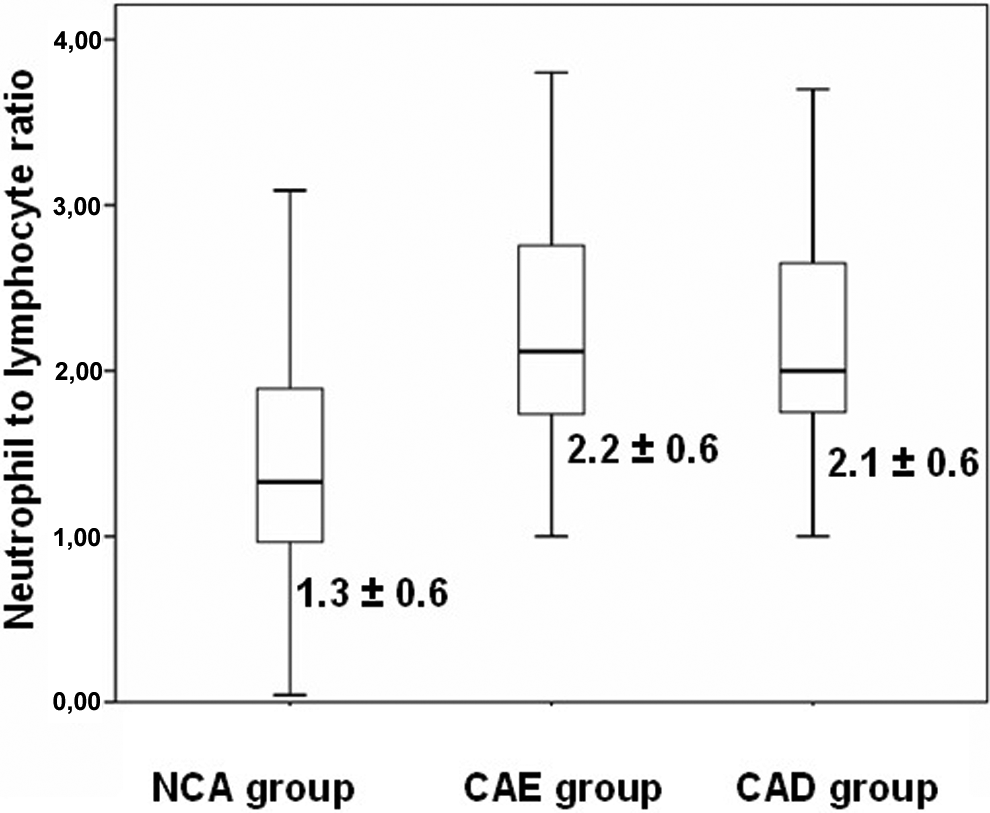
Graphics demonstrating the significant differences in neutrophil-to-lymphocyte ratio (NLR) in patients with coronary artery ectasia, coronary artery disease, and normal coronary arteries.
Comparison of Neutrophil-to-Lymphocyte Ratio and Several Markers of Inflammation in the Study Population.
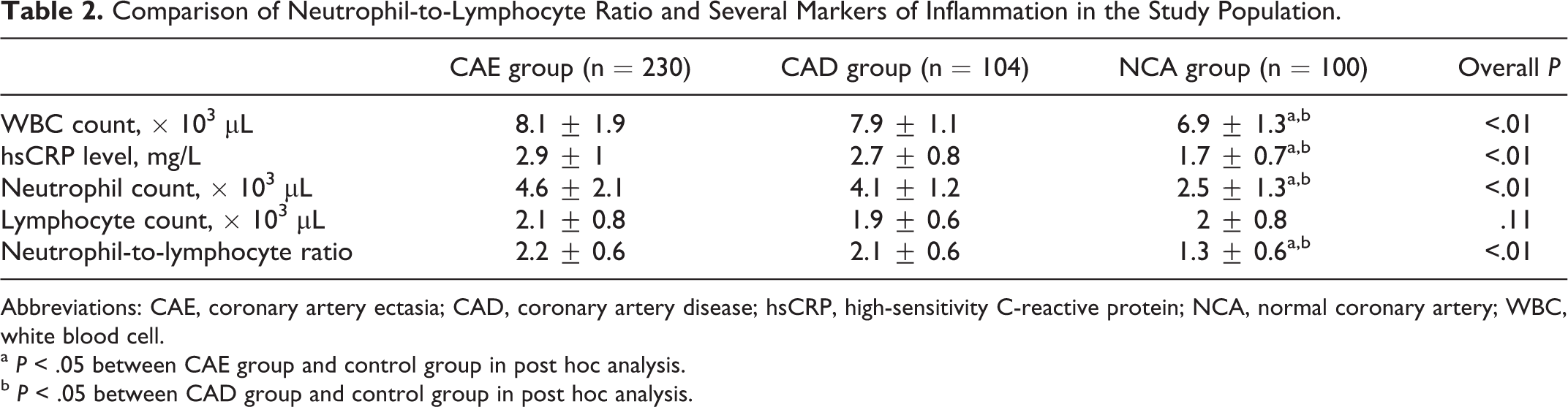
Abbreviations: CAE, coronary artery ectasia; CAD, coronary artery disease; hsCRP, high-sensitivity C-reactive protein; NCA, normal coronary artery; WBC, white blood cell.
a P < .05 between CAE group and control group in post hoc analysis.
b P < .05 between CAD group and control group in post hoc analysis.
The NLR was 3.1 ± 0.6 in patients with type 1 CAE, 2.58 ± 0.5 in type 2 CAE, 2.29 ± 0.4 in type 3 CAE, and 1.79 ± 0.5 in type 4 CAE, which is the least complex type of CAE (Figure 2). Linear regression analysis revealed that smoking history (coefficient β = .14, P = .007), WBC count (coefficient β = .13, P = .022), hsCRP level (coefficient β = .14, P = .009), and NLR (coefficient β = .61, P < .001) were significantly associated with severity of CAE (Table 3). In patients with CAE, there was a weak correlation between NLR and smoking (r = .053, P = .004) and between NLR and hsCRP (r = .323, P < .001).
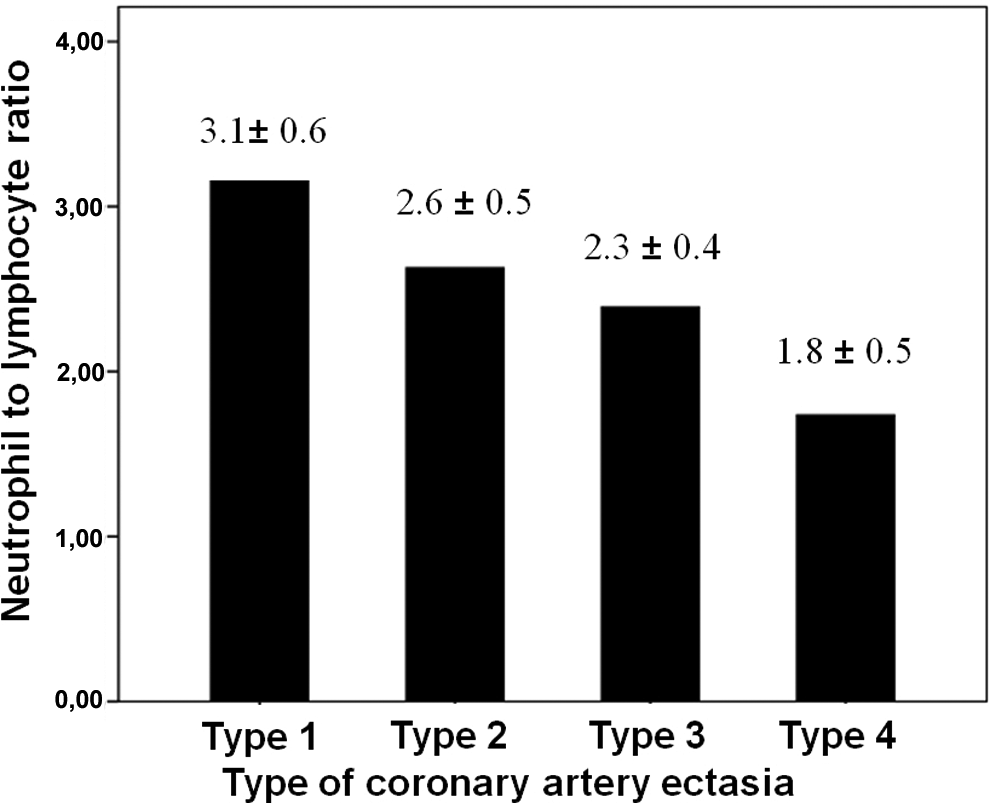
The NLR is highest in patients with the most severe type of CAE (Type 1 CAE) and lowest in patients with the least severe type of CAE (Type 4 CAE). CAE indicates coronary artery ectasia, NLR, neutrophil to ratio.
Linear Regression Analysis Demonstrating the Relationship Between Selected Variables and Severity of Coronary Artery Ectasia (CAE).
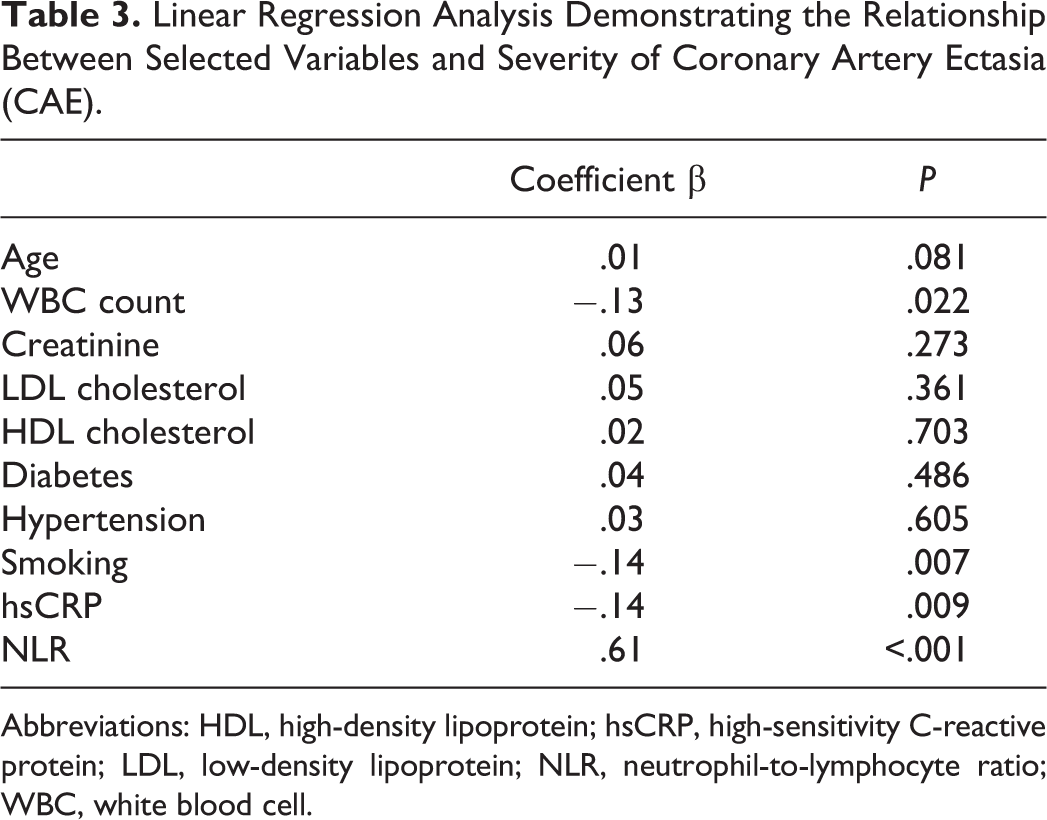
Abbreviations: HDL, high-density lipoprotein; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; NLR, neutrophil-to-lymphocyte ratio;, WBC, white blood cell.
Discussion
Neutrophil-to-lymphocyte ratio was significantly higher in patients with CAE than in patients with NCA. This study demonstrates a significant association between severity of CAE and NLR.
Current data are limited in clearly identifying the precise mechanism leading to luminal dilatation in patients with CAE. Coronary atherosclerosis is present in almost 50% of the patients with CAE, suggesting a common causative mechanism in the formation of both CAD and CAE.
The role of inflammation in the initiation and progression of coronary atherosclerosis is well described. 13 –18 Increased levels of inflammatory markers have been found in association with the severity of coronary atherosclerosis, prognosis in acute coronary syndromes, and prognosis after coronary interventions. 9 –11 In the early stages of atherosclerotic plaque development, inflammatory monocytes are provoked to move into the vascular wall by various adhesion and chemoattractant molecules expressed from endothelial cells. 19 In advancing stages of plaque development, these monocytes differentiate to macrophages to play role in the formation of lipid cores. Also, in a mature atherosclerotic plaque, inflammatory mediators lead to expression of proteolytic enzymes and weaken the fibrous cap that may result in plaque rupture and total or partial occlusion of the vessel. 20
The role of inflammation has also been studied in patients with isolated CAE. Association between CAE and inflammatory vasculitides such as Kawasaki disease, Takayasu arteritis, Behçet disease, and connective tissue diseases support the inflammatory origin of CAE. 21 Plasma E-selectin, intercellular adhesion molecule-1, and vascular cell adhesion molecule-1 were significantly higher in patients with isolated CAE. 22 In a study, higher levels of inflammatory markers including tumor necrosis factor α and interleukin 6 (IL-6)were increased in patients with CAE. 23 Furthermore, Turhan et al 24 found that CRP, an indicator of systemic inflammatory response, was also significantly higher in patients with isolated CAE than in those with NCA. Accumulation of inflammatory cells in the medial layer of coronary arteries was also reported in histopathological examinations of patients with CAE. 25,26 In addition, the levels of cellular adhesion molecules CD 11b and CD 45 were higher in patients with CAE. 27
The WBC count and some of its subtypes were previously studied in patients with CAE. Leukocyte count and its subtypes were significantly higher in patients with CAE and obstructive CAD compared to patients with NCA. 28 Li et al found an increased number of leukocytes, neutrophils, and increased levels of hsCRP and IL-6 in patients with CAE compared with controls with normal coronary arteries. 29 In our study, we investigated NLR—an indicator of systemic inflammatory response 30 —in patients with CAE and found a higher NLR in patients with CAE and CAD compared to patients with NCA.
The underlying mechanism associating NLR and CAE is not clearly established. However, the most probable pathogenic mechanism is the preexisting systemic inflammatory response on vascular tissue in which neutrophils play a major role by mediating the release of arachidonic acid metabolites, cytotoxic oxygen-derived-free radicals, myeloperoxidase, elastase, and various hydrolytic enzymes . 31,32 Similar histopathological findings of patients with CAE and atherosclerosis suggest that ectatic process may be a stage of ongoing atherosclerosis. With this background in mind, we suggest that the inflammatory state, represented by NLR, contributes to the formation of ectatic segments in coronary arteries as seen in atherosclerotic arteries.
In conclusion, the present study demonstrates that NLR is significantly higher in patients with CAE compared to patients with NCA. The NLR is also significantly associated with the severity of CAE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.