
Abstract
Background:
A strong association exists between diabetes mellitus and critical limb ischemia.
Methods and Results:
We performed endovascular therapy on 1060 limbs in 884 patients with below knee lesions only. The patients were divided into diabetes (DG) and nondiabetes groups (NDG). Limb salvage was poorer in the DG (79% vs 89%, P = .0061). No significant difference was observed in mortality, amputation-free survival (AFS), and target vessel revascularization (TVR). Multivariate analysis revealed diabetes status, infection, poor activity of daily living (ADL), younger age, and procedure failure as independent predictors of major amputation in DG. In the NDG, procedure failure was the predictor, and younger age and poor ADL showed tendency of major amputation.
Conclusions:
Mortality, AFS, and TVR showed no significant difference between the 2 groups, but major amputation was more frequent in DG. Not only revascularization but also infection and diabetes control were very important for limb salvage in DG.
Background
There is a strong association between diabetes mellitus and critical limb ischemia (CLI). 1 The risk of major amputation is 5 to 10 times higher in patients with diabetes than in patients without, and some 7 million people have this disease in Japan. 2,3 Moreover, severe atherosclerotic lesions are often observed in patients with both diabetes and CLI, especially with disease below the knee (BK). 4,5 Patients with diabetes are also more susceptible to infection than healthy individuals. The close correlation between CLI, susceptibility to infection, and subsequent amputation means that revascularization is a critical factor in wound treatment if the limb is to be salvaged. Adequate blood flow is required for a wound to heal, 6 and this is particularly the case in BK lesions. However, the outcome in terms of patency of endovascular therapy (EVT) for BK lesions has been reported to be poor. 7 Therefore, surgical revascularization is often considered the gold standard in such cases, with EVT playing a more limited role only. 3,8
Recently, however, the range of techniques and devices available for EVT has expanded, and this approach has gained popularity. One study compared postoperative outcomes over a 2-year period between EVT and bypass surgery 9 and found that primary patency with bypass surgery was superior to that with EVT, although the limb salvage rate showed no significant difference between the 2 groups. In another study, the results indicated the superiority of bypass surgery, with a postoperative life expectancy of 2 years. 10 Although revascularization is critical in such patients, there is often a reluctance to resort to reconstructive surgical procedures due to comorbidity. This is where EVT may offer potential in offering a less invasive means of revascularization. The rate of EVT use is increasing, and the number of amputations is decreasing in many countries. 11 Meanwhile, the number of patients with diabetes is growing, and the risk of leg amputation in such patients is high. Takahara et al reported that poor diabetes control was associated with major amputation. 12 However, the amount of high-quality data available on longer outcome after EVT for BK lesions is small. Therefore, the purpose of this study was to investigate the results of EVT in patients with diabetes and CLI having BK lesions only.
Methods
Study Population
This was a physician-initiated, multicenter, retrospective cohort study. Data on intervention for BK lesions only in patients with CLI at 11 high-volume EVT centers in Japan between March 2004 and December 2011 were analyzed. A total of 3047 limbs were treated. Of these, 1461 were excluded as the lesions were above the knee; 170 because they were unsuitable for revascularization; and 359 due to distal bypass. Therefore, only a total of 1057 limbs in 884 patients with BK lesions were eligible for inclusion in the study (Figure 1). Rest pain or foot gangrene was observed in all the patients. Vascular specialists decided whether EVT was indicated. The patients were divided into a diabetes group (DG) and a nondiabetes group (NDG) for a comparison. Written informed consent was obtained from all the patients. The study was approved by the ethics committee of each institution concerned and registered with the University Hospital Medical Information Network-Clinical Trial Registry (UMIN-CTR) as recommended by the International Committee of Medical Journal Editors (no. UMIN000008761).
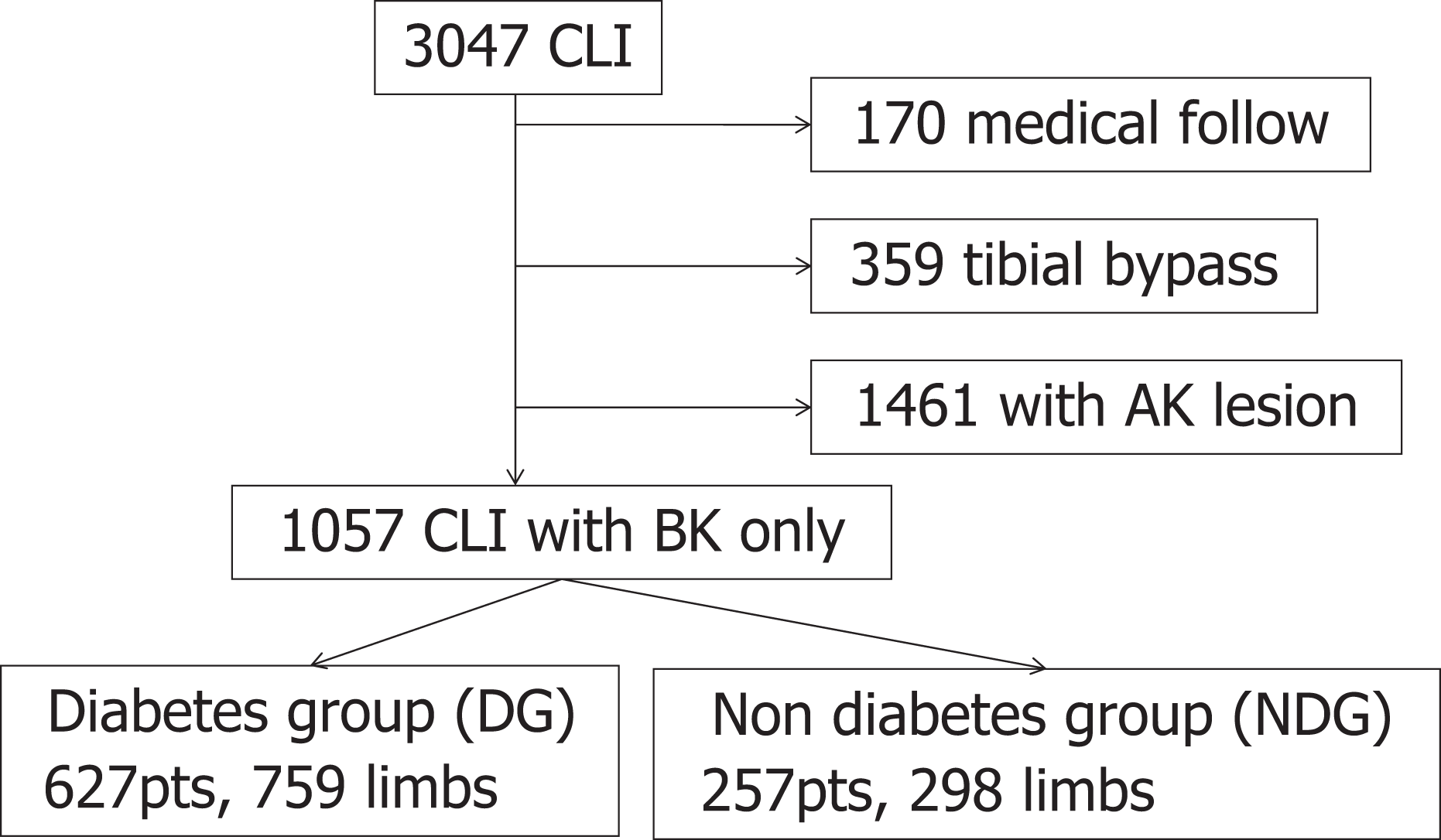
Participants flow.
Procedure Steps
Endovascular therapy was performed percutaneously, placing a 3 to 6F sheath. Prior to intervention, 3000 to 5000 units of unfractionated heparin was administered to maintain active clotting time at ≥200 seconds. A 0.035-, 0.018-, or 0.014-in guidewire was advanced to the target lesion with a 4F multipurpose or microcatheter and the lesion crossed. An optimally sized balloon was then dilated. Minimal balloon dilation time was 60 seconds. If severe dissection occurred, additional ballooning (over 3 minutes) was performed. Because stenting for BK lesions has not yet been approved in Japan, no bail out stenting was performed. All patients were placed on aspirin (100 mg/day) indefinitely and cilostazol or ticlopidine (200 mg/day) for at least 4 weeks. These drugs were initiated at least 2 days prior to the intervention.
If the patient had a wound, a plastic surgeon or vascular surgeon was consulted prior to performing EVT. If necessary, continuous care was given until wound healing was achieved.
Follow-Up and Outcomes
Assessment was mainly performed at outpatient clinics at baseline, at 1, 3, 6, and 12 months, and then at 12-month intervals thereafter. Factors investigated included major adverse events (death, major amputation, and target lesion revascularization), staging of peripheral arterial disease according to the Rutherford classification, ankle brachial index (ABI), lesion patency as evaluated by duplex ultrasonography, and skin perfusion pressure (SPP). The SPP was used as an objective measurement in the definition of CLI. 13 Repeat angiography was scheduled if restenosis was suspected (recurrent symptoms, lower SPP, or delayed tissue healing). Indications and decision for major amputation was decided by a plastic surgeon or vascular surgeon.
Definitions
The CLI was defined as Rutherford category 4, 5, or 6. Ischemic tissue loss was defined in accordance with Trans-Atlantic Inter-Society Consensus (TASC) as tissue loss associated with an ankle pressure <70 mm Hg or a toe pressure <50 mm Hg, and similarly, an ankle pressure <50 mm Hg or a toe pressure <30 mm Hg, for ischemic rest pain. When these measurements could not be obtained, SPP was measured at the dorsal and plantar sides of the foot. An SPP <40 mm Hg was defined as indicating ischemic tissue loss, <30 mm Hg for ischemic rest pain. Angiosome-oriented EVT was defined as successful revascularization to the location of gangrene. The angiosome concept has been reported previously. 14 Amputation above the ankle was defined as major by the vascular specialist or plastic surgeon concerned. The diagnosis of diabetes was based on World Health Organization criteria. Hypertension was defined as systolic blood pressure ≥ 140 mm Hg or diastolic pressure ≥ 90 mm Hg. Hyperlipidemia was defined as serum low-density lipoprotein cholesterol ≥ 100 mg/dL, high-density lipoprotein cholesterol ≤40 mg/dL, or triglycerides ≥ 150 mg/dL. Poor cardiac function was defined as an ejection fraction of less than 40%. Poor activities of daily living (ADLs) were defined as wheel chair or bedridden status. The procedure was considered successful if in-line flow to the foot, without <30% residual stenosis, was achieved.
Statistical Analysis
Statistical analysis was performed using SPSS (SPSS Inc, Chicago, Illinois). Values are reported as the mean ± standard deviation. Continuous variables were examined using an unpaired t test or the Mann-Whitney U test. Categorical variables were compared using the chi-square test. Time-dependent outcomes were analyzed by the Kaplan-Meier method and compared with the log-rank test. Multiple logistic regression analysis was used to determine independent factors associated with mortality and limb salvage rate. A probability value of <.05 was considered statistically significant. Variables identified as statistically significant in the univariate analysis (P < .05) were entered in the multivariate model.
Results
Patient characteristics are shown in Table 1. The patients were significantly younger in the DG than in the NDG (70.2 ± 9.7 vs 74.4 ± 10.8 years, respectively, P < .001). A trend toward a need for hemodialysis was observed in both the groups, although no significant difference was observed in the percentage of these patients (DG vs NDG, 64% vs 57%, P = .052). There were more Rutherford 4 patients in NDG (32% vs 17%, P < .001). No significant difference was observed between DG and NDG in ABI (0.81 ± 0.25 vs 0.78 ± 0.25, respectively, P = .126) or SPP (dorsal: 31.6 ± 16.8 vs 30.5 ± 17.2 mm Hg, respectively, P = .438; plantar: 35.2 ± 18.2 vs 33.3 ± 18.6 mm Hg, respectively, P = .241). Lesion characteristics are shown in Table 2. No significant difference was observed in lesion distribution between DG and NDG (anterior tibial artery [ATA], 91% vs 94%, P = .212; posterior tibial artery [PTA], 91% vs 91%, P = .930; and peroneal artery [PA], 67% vs 70%, P = .391, respectively). No significant difference was observed in chronic total occlusion between DG and NDG (ATA, 68% vs 74%, P = .103; PTA, 71% vs 73%, P = .570; PA, 43% vs 43%, P = .908, respectively). Lesion calcification, however, was more frequent in DG than in NDG (ATA, 75% vs 67%, P = .007; PTA, 75% vs 65%, P = .001; and PA, 63% vs 57%, P = .057, respectively).
Patient Characteristics.
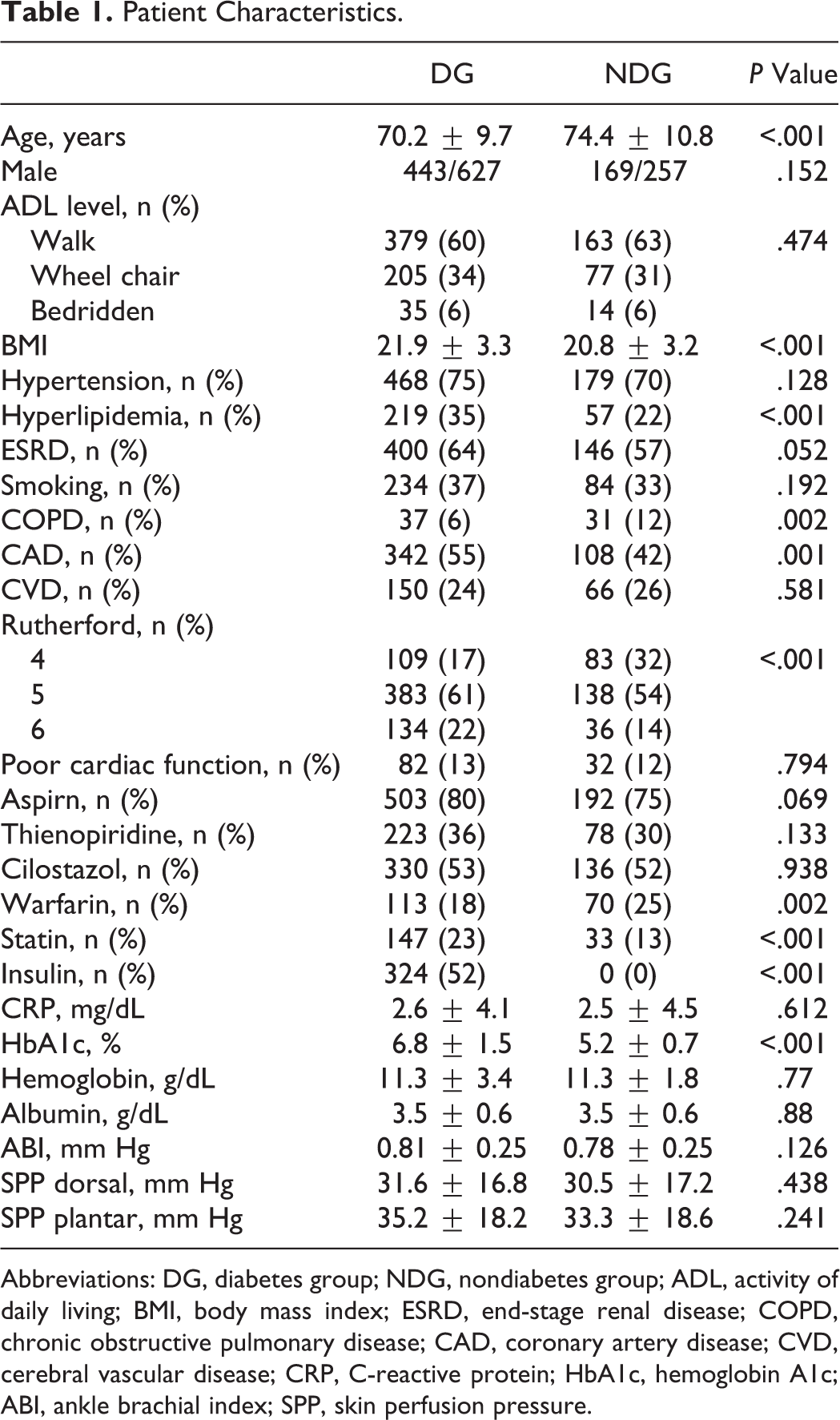
Abbreviations: DG, diabetes group; NDG, nondiabetes group; ADL, activity of daily living; BMI, body mass index; ESRD, end-stage renal disease; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; CVD, cerebral vascular disease; CRP, C-reactive protein; HbA1c, hemoglobin A1c; ABI, ankle brachial index; SPP, skin perfusion pressure.
Lesion Characteristics.
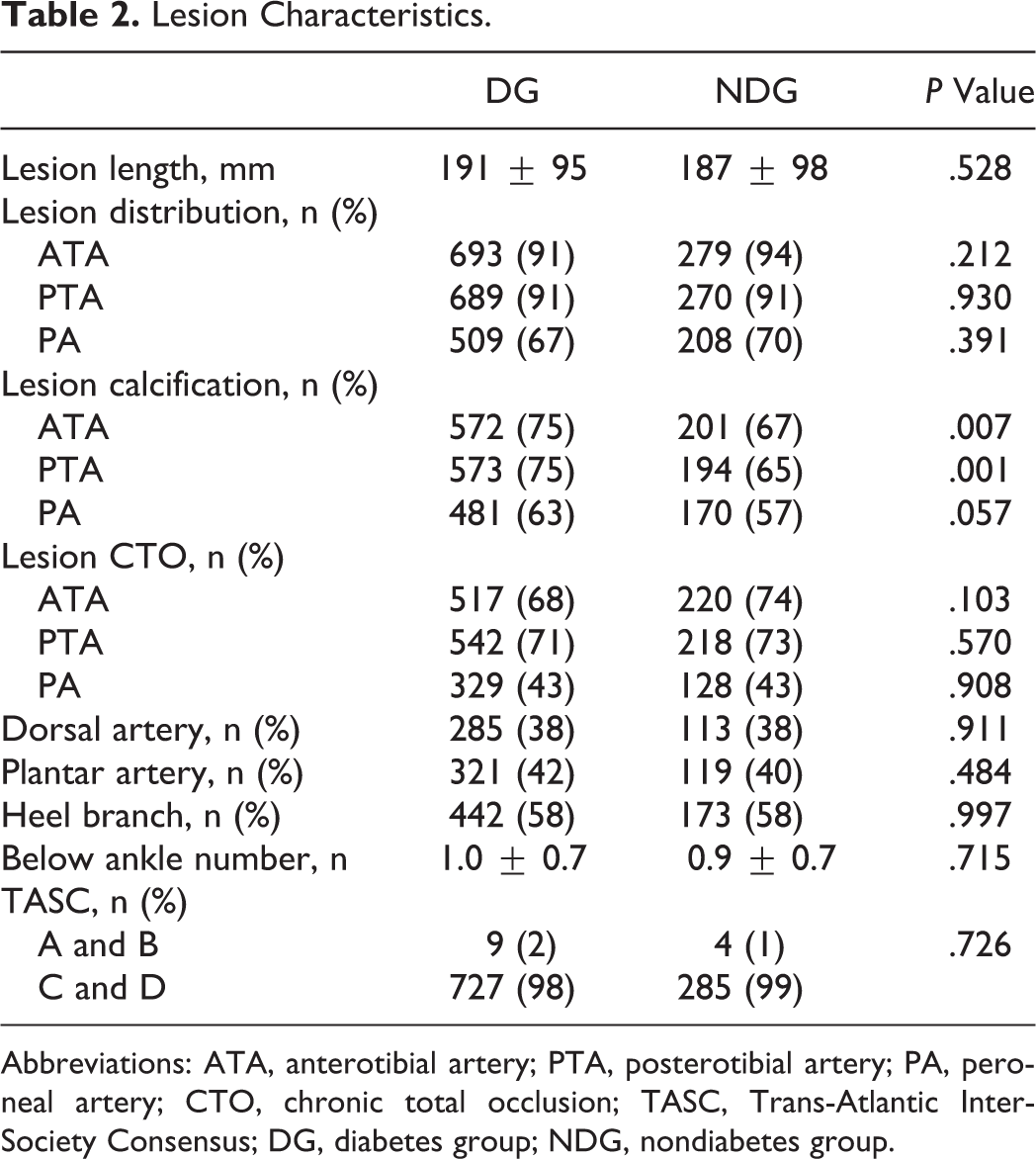
Abbreviations: ATA, anterotibial artery; PTA, posterotibial artery; PA, peroneal artery; CTO, chronic total occlusion; TASC, Trans-Atlantic Inter-Society Consensus; DG, diabetes group; NDG, nondiabetes group.
Wound status and procedure performed are shown in Table 3. Procedure success rate and angiosome-oriented EVT rate showed no significant difference between the 2 groups.
Wound and Procedure.
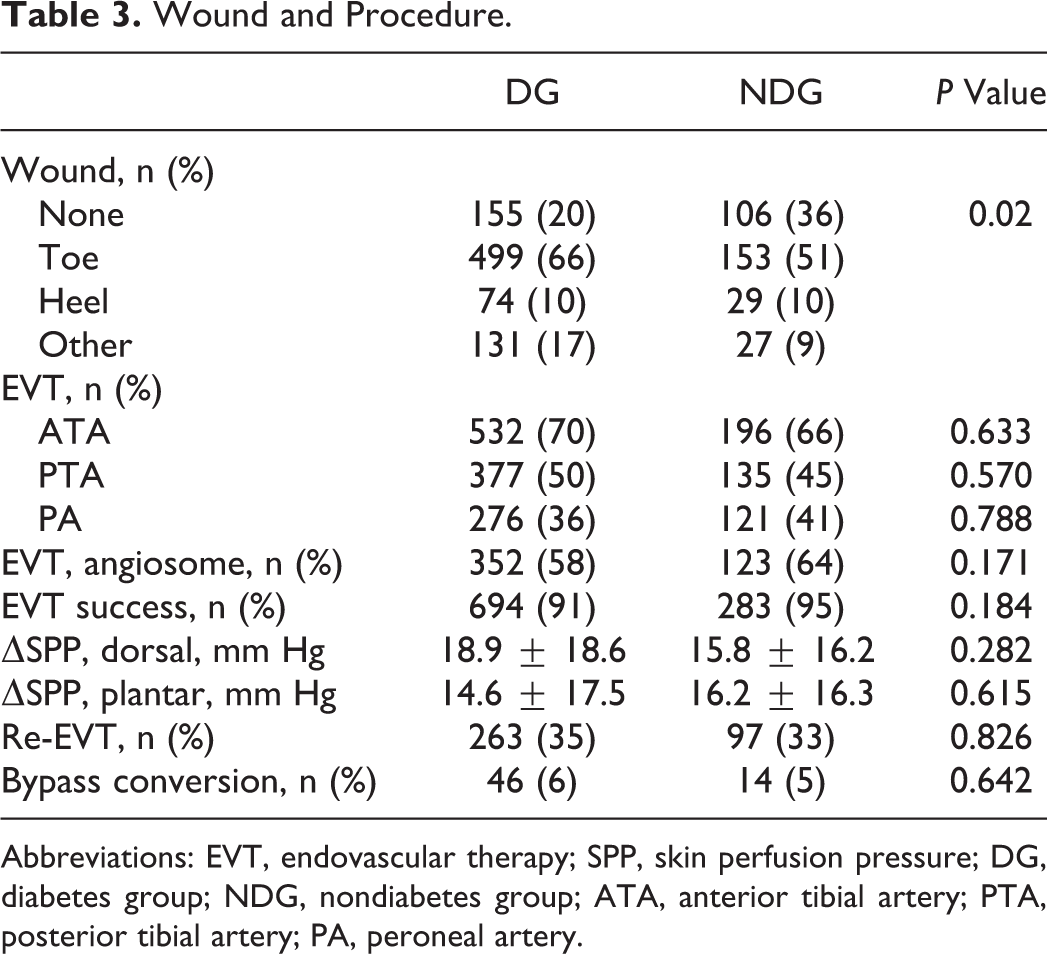
Abbreviations: EVT, endovascular therapy; SPP, skin perfusion pressure; DG, diabetes group; NDG, nondiabetes group; ATA, anterior tibial artery; PTA, posterior tibial artery; PA, peroneal artery.
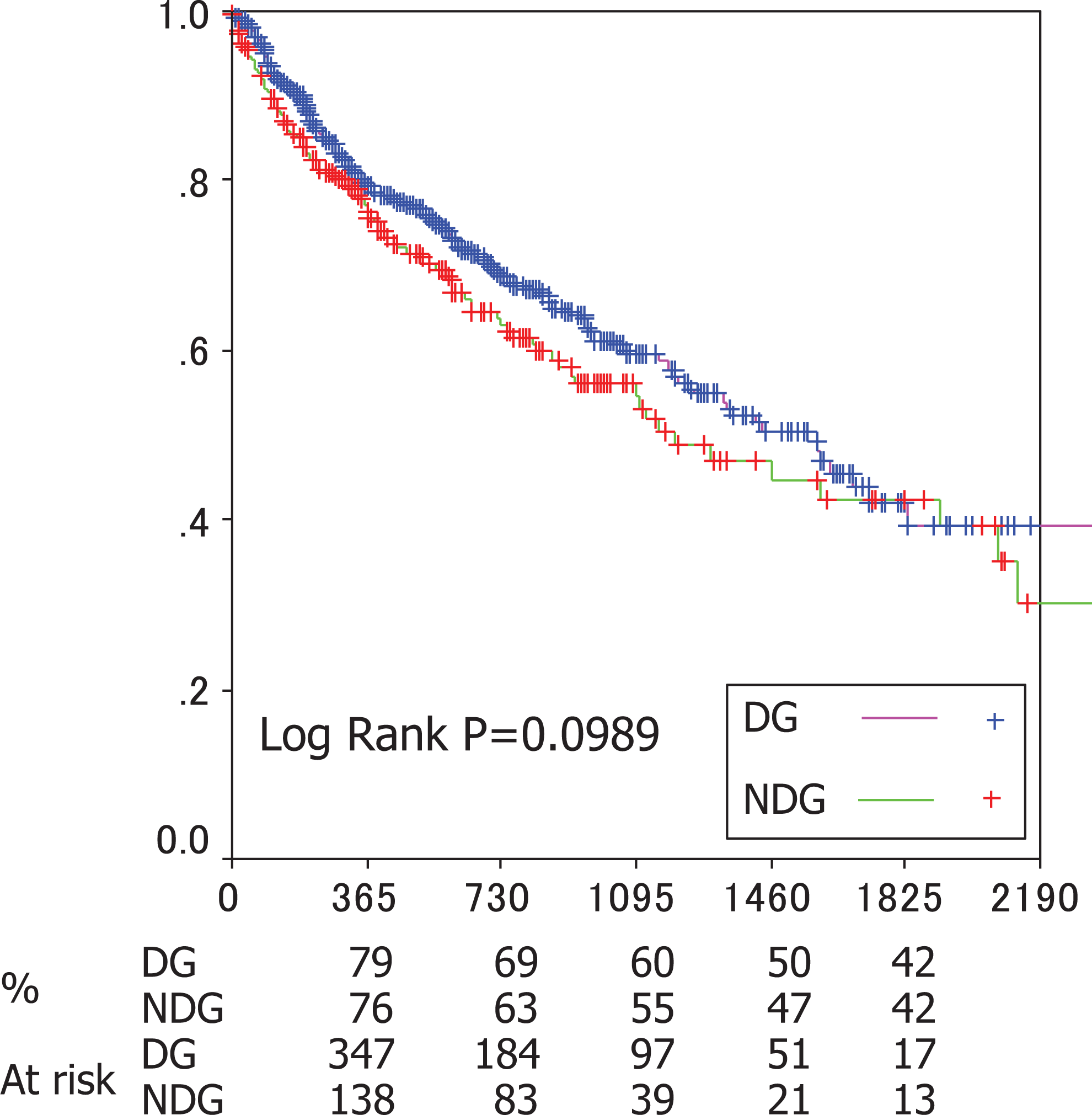
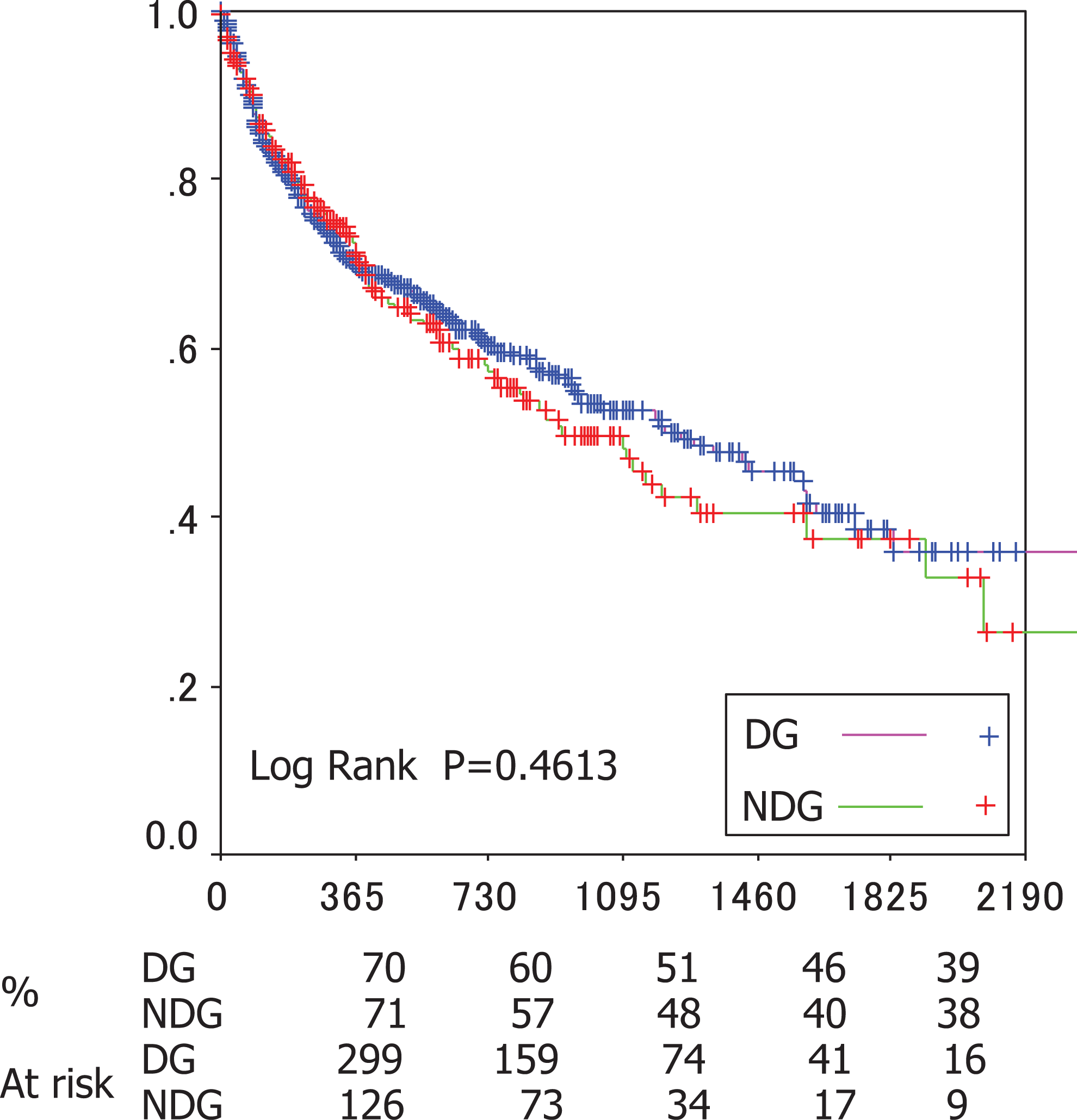
Follow-up of the outcome revealed that the limb salvage rate in the DG was poorer than that in the NDG (79% vs 89%, respectively, P = .0061; Figure 2). No significant difference was observed in mortality (Figure 3), amputation-free survival (AFS; Figure 4), and freedom from target vessel revascularization (TVR; Figure 5) between the 2 groups. The mean follow-up period was 532 ± 362 days (1-2133 days).
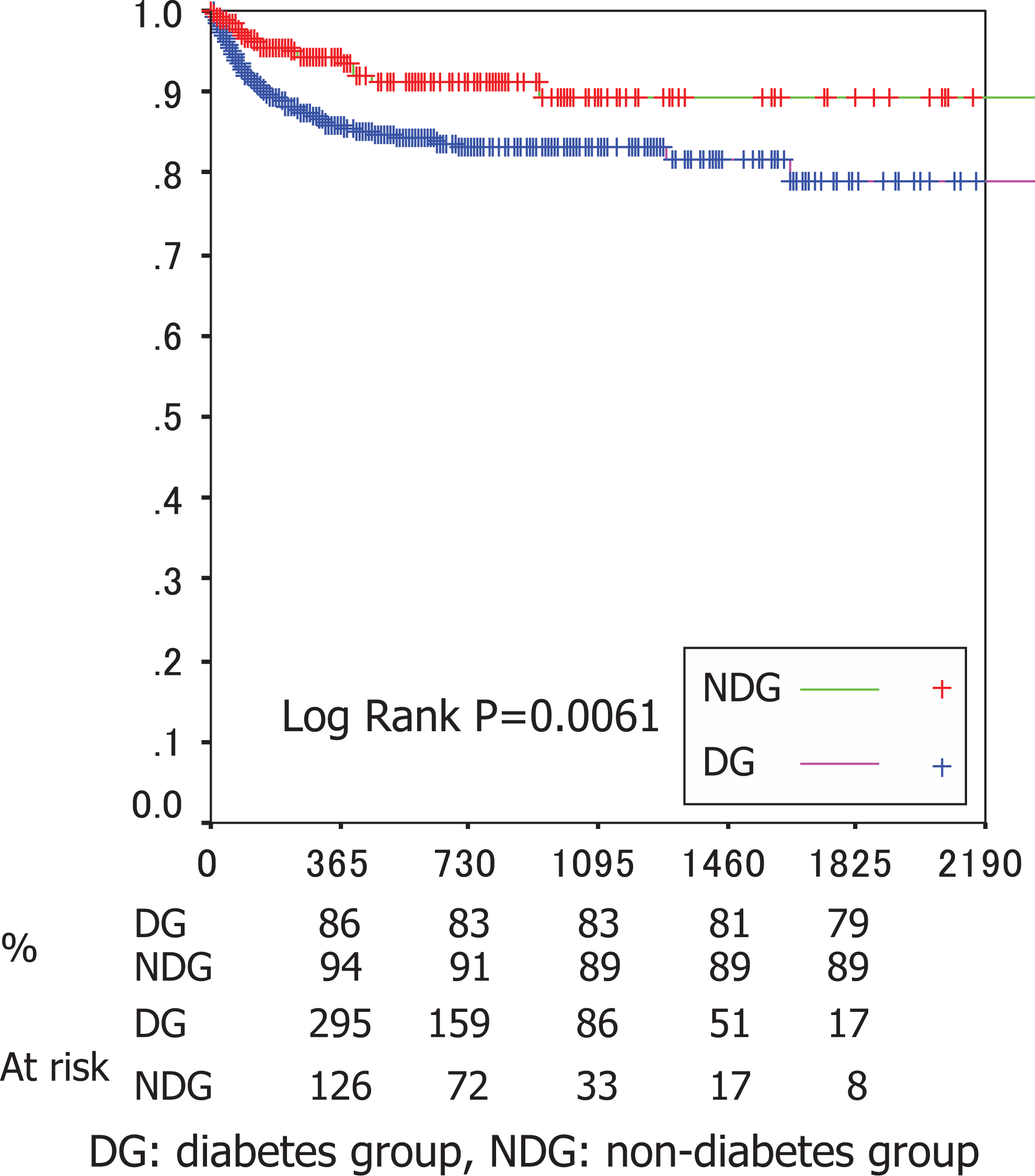
Limb salvage rate.
Mortality.
Amputation-free survival.
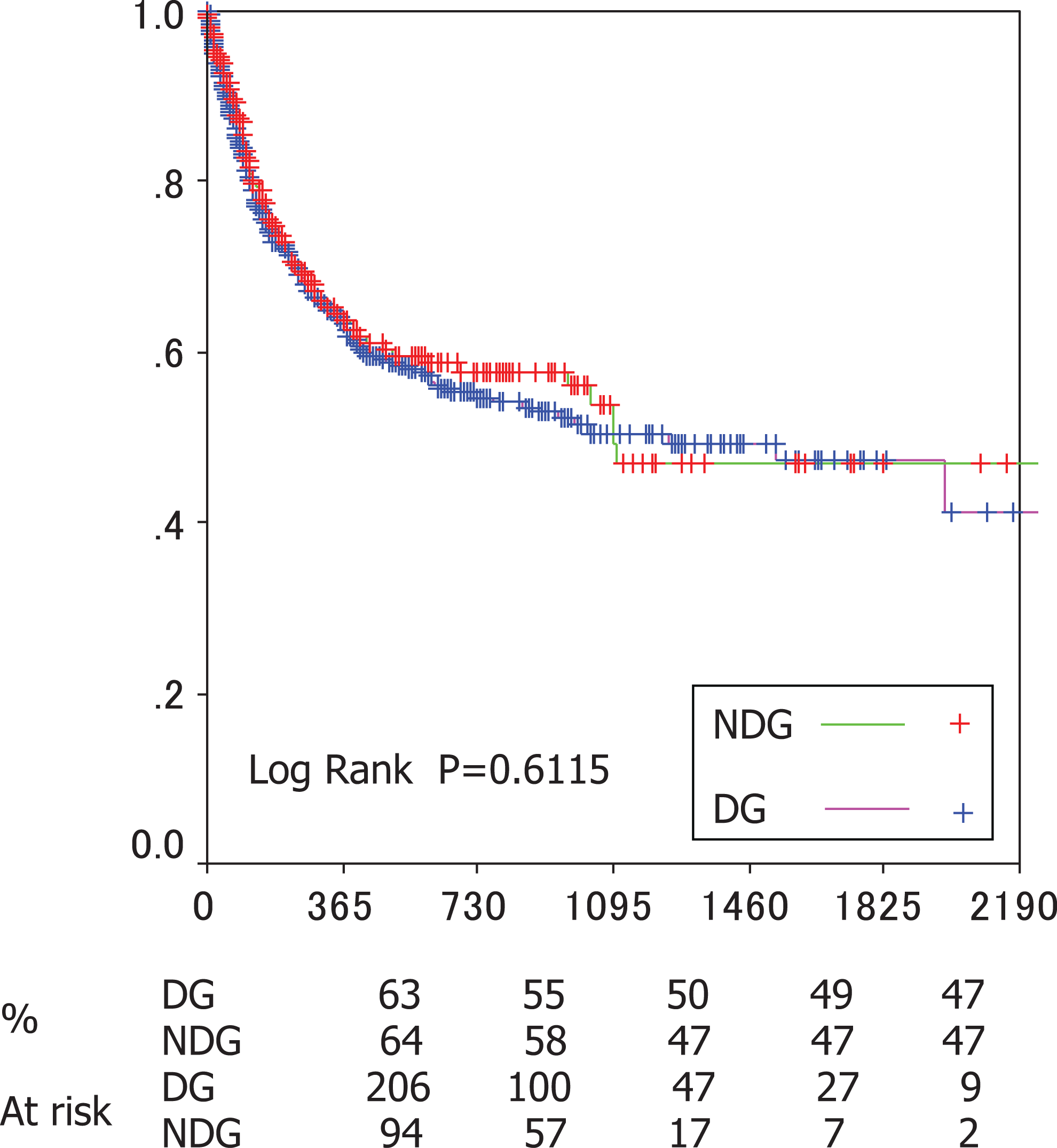
Freedom from target vessel revascularization.
Independent predictors of mortality and major amputation were also investigated using multivariate analysis. The independent predictors of major amputation in each group are shown in Tables 4 and 5, while those of mortality are given in Tables 6 and 7. Inflammation as indicated by serum C-reactive protein (CRP) level, diabetes control as indicated by HbA1c, younger age, procedure failure, and a low level of ADL were independent predictors of major amputation in the DG. Only procedure failure was an independent predictor of amputation in the NDG. Inflammation was not an independent predictor in the multivariate model of the NDG. Low body mass index, low serum albumin, warfarin administration, and poor ADL level were independent predictors of mortality in the DG; coronary artery disease (CAD) and low ADL level were independent predictors of mortality in the NDG.
Multivariate Analysis for Major Amputation.
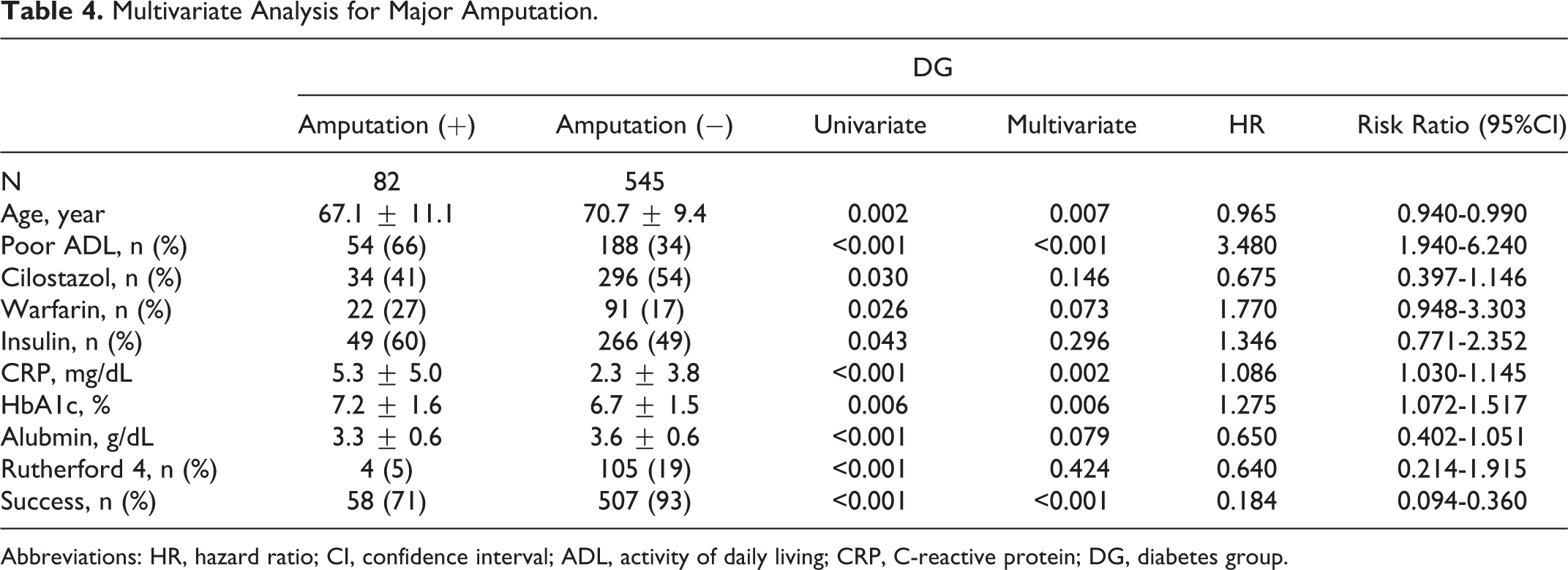
Abbreviations: HR, hazard ratio; CI, confidence interval; ADL, activity of daily living; CRP, C-reactive protein; DG, diabetes group.
Multivariate Analysis for Major Amputation.

Abbreviations: ADL, activity of daily living; NDG, nondiabetes group; CRP, C-reactive protein; CI, confidence interval.
Multivariate Analysis for Mortality.

Abbreviations: ADL, activity of daily living; CRP, C-reactive protein; DG, diabetes group; CI, confidence interval; CVD, cerebral vascular disease; COPD, chronic obstructive pulmonary disease; BMI, body mass index.
Multivariate Analysis for Mortality.
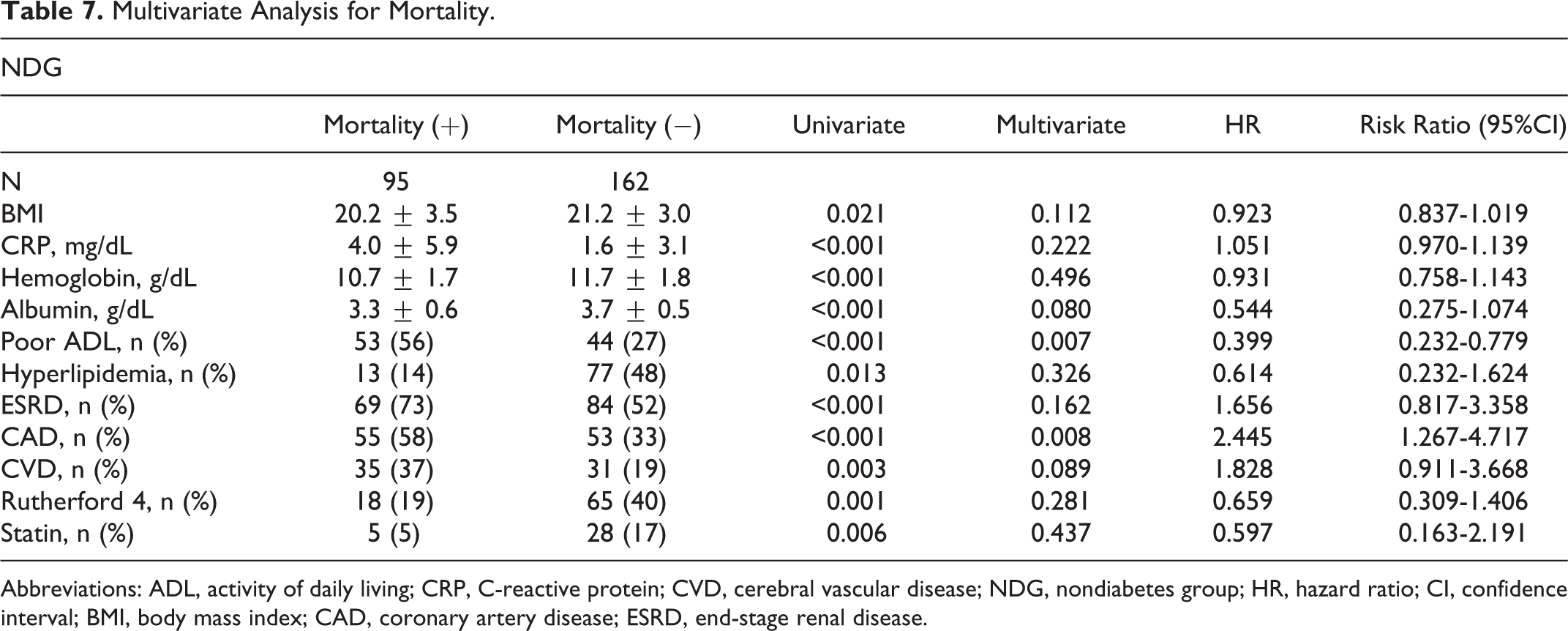
Abbreviations: ADL, activity of daily living; CRP, C-reactive protein; CVD, cerebral vascular disease; NDG, nondiabetes group; HR, hazard ratio; CI, confidence interval; BMI, body mass index; CAD, coronary artery disease; ESRD, end-stage renal disease.
Discussion
This study was a multicenter cohort study of BK angioplasty. We were able to show that EVT for BK lesion for diabetes in patients with CLI was feasible in terms of acute result and that success rate in the DG was similar to the NDG. Moreover, compared to the previous reports, 15 our results were reasonable. Follow-up results indicated major amputation was more frequent in the DG, and there were no significant differences between the 2 groups in terms of mortality, AFS, and TVR.
In this study, mortality in patients with CLI was very high, reaching 60% at 5 years postoperatively, which agrees with the rate of 71% observed in an earlier study. 16 In the bypass versus angioplasty in severe ischaemia of the leg (BASIL) study, bypass surgery offered better results than EVT in patients with a life expectancy of more than 2 years. 10 But many Japanese patients with CLI would be unlikely to benefit from bypass surgery because of their short-life expectancy and comorbidity.
No correlation was observed between diabetes and mortality, which agrees with the results of an earlier study which found that other factors such as age, dialysis, and hemoglobin level were more reliable prognostic indicators. 12 A previous study has also reported that diabetes CLI and nondiabetes CLI showed no significant differences in limb salvage rate and mortality. 13 The AFS also showed no difference between the 2 groups despite the fact that major amputation was more frequent in the DG. The DG was significantly younger than the NDG in this cohort, so mortality of the DG may have tended to be better. Another reason may be that the number of deaths was larger than that of major amputation (death = 280 and major amputation = 101). The TVR also showed no difference. Distal bypass data from Japan showed that patency rate of patients with diabetes was poor 17 ; however, data from EVT were not reported.
In this study, a significant correlation was found, however, between diabetes and major amputation. It is crucial to maintain adequate blood flow and control the general status of the patient, particularly with regard to infection and nutrition if the limb is to be salvaged. No significant difference was observed in lesion distribution between the 2 groups, although more lesion calcification was noted in DG. Although no routine follow-up angiography was performed, we cannot rule out the possibility that this calcification contributed to the poor vessel patency observed here.
A recent study reported that angiosome-oriented EVT was important for limb salvage. 14 In our cohort, in the DG and NDG, we failed to demonstrate that angiosome-oriented EVT was important for limb salvage. But in the whole cohort, there was a higher limb salvage rate for angiosome oriented (88.8%) versus nonangiosome oriented (83.7%, P = .022).
In many cases, we believe that stenting may offer one of the best option in BK revascularization. 18,19 Stenting is obviously effective in order to bail out of suboptimal balloon angioplasty. However, this procedure is yet to gain official approval for use in BK lesions in Japan. Moreover, recent studies have also reported favorable results for the primary use of a drug-eluting stent in BK lesions. 18,19 Schmidt et al also reported good results for the use of a drug-eluting balloon in BK lesions. 20
In DG here, CRP was one of the strongest predictors of major amputation. Moreover, poor ADL status, HbA1c, younger age, and procedure failure were related to poor outcome. It was reasonable that poor ADL patients, HbA1c, and procedure failure tended to be poor outcome, but our data indicated major amputation was more frequent in younger age. It would be difficult to assess it, because patency of distal bypass for old patients was poor. 17 Our cohort often had severe risk factors, so we often experienced old patients dying without wound healing. As a result, the number of major amputation might be small in old patients. On the other hand, procedure failure was the only independent predictor of major amputation in NDG. In addition, younger age and poor ADL status failed to indicate as independent predictors but showed tendency of major amputation. The CRP level was identified as a significant factor by univariate analysis, but it was not by multivariate analysis. So inflammation, indicated by CRP level, and diabetes control were the most important difference between DG and NDG. These results confirm that not only revascularization but also control of inflammation and diabetes are critical in limb salvage.
According to the multivariate analysis, mortality was strongly associated with ADL status, low serum albumin, and warfarin administration in DG. It is well known that poor ADL is related to poor outcome. The serum albumin level is an indicator of the patient’s nutritional status, with a low level correlating with a poor prognosis. Warfarin administration is a negative factor for prognosis. Warfarin is usually administered in patients at high risk of thrombosis such as those with poor cardiac function or atrial fibrillation. Warfarin administration was reported to be related to poor outcome in dialysis patients. 21 In this study, all the patients received antiplatelet agents. The combination of these antiplatelet agents and warfarin may have had some bearing on the poor outcome observed. Cilostazol has been reported to affect patients with CLI. 16,22 In the present study, cilostazol was associated with AFS in the DG by univariate but not multivariate analysis. Cilostazol had better effect for improving intermittent claudication 3 and preventing SFA in stent restenosis. But it might have less effect only to the BK lesion disease.
A relationship was also observed between ADL level or CAD and mortality in NDG. Comorbidity such as CAD, cerebral vascular disease, and chronic obstructive pulmonary disease was also a strong factor for mortality in both the groups according to the univariate model.
Limitation
This was a retrospective study, and a prospective trial is needed to validate these results. Moreover, all the patients in this trial received EVT. Further studies are needed to compare the results of EVT with those of surgical bypass and other medical therapies. Additionally, our procedure was only balloon angioplasty and drug-eluting devices, and stents were not available in Japan.
Conclusion
Endovascular therapy for BK lesion in patients with diabetes and CLI was feasible in terms of acute results. Follow-up data of mortality, AFS, and TVR showed no significant difference between the 2 groups, but major amputation was more frequent in the DG. Not only revascularization but also infection and diabetes control were very important for limb salvage in DG.
Footnotes
Acknowledgment
The authors would like to thank Jeremy Williams, Tokyo Dental College, for his assistance with the English of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.