
Abstract
We investigated the association between serum bilirubin level and thoracic aortic intima–media thickness (IMT). The study population consisted of 417 patients without coronary artery disease, who underwent transesophageal echocardiography examination for various indications. The highest aortic IMT values were observed in the bilirubinlow group compared with the bilirubinhigh group (P < .001). Serum bilirubin level was associated with high-density lipoprotein cholesterol level (r = .162, P = .001), high-sensitivity C-reactive protein (hsCRP; r = −.265, P < .001), and aortic IMT (r = −.551, P < .001) in bivariate analysis. Multivariate linear regression analysis showed that serum bilirubin level was independently and negatively associated with hsCRP (β = −.095, P = .028) and aortic IMT (β = −.513, P < .001). Serum bilirubin level may be an independent predictor of the extent of subclinical aortic atherosclerosis assessed by thoracic aortic IMT.
Introduction
Bilirubin, the end product of heme catabolism, has antioxidant properties as indicated by its ability to scavenge peroxyl radicals and to inhibit oxidation of low-density lipoprotein (LDL). 1 –3 Bilirubin may protect against atherosclerosis development risk of cardiovascular disease (CVD). 3 –8
Although there have been numerous studies on the association between serum bilirubin level and CVD, 3 –6,9,10 there is lack of research on direct investigation of relevance between serum bilirubin level and thoracic aortic intima–media thickness (IMT). Aortic atherosclerotic lesions detected on transesophageal echocardiography (TEE) are markers of diffuse atherosclerotic disease, 11,12 and thoracic aortic IMT has been reported as an earlier marker of preclinical atherosclerosis than carotid IMT. 13 The primary purpose of this study was to investigate the association between serum bilirubin and aortic atherosclerosis in patients undergoing TEE examination for various indications.
Methods
Study Population
Of the 1083 TEE procedures performed between January 2011 and July 2013 in our clinic, we evaluated 417 patients who had nonatherosclerotic heart disease and who underwent TEE examination for various indications (207 men, 210 women; mean age 40.5 ± 11.4 years), which included evaluation and management of atrial fibrillation (86 patients), valvular heart disease (62 patients for mitral valve disease, 23 patients for aortic valve disease), and suspected atrial septal defect (256 patients). Of the 108 patients, 666 with known coronary artery disease (CAD) or clinical signs of CAD, heart failure, peripheral artery disease, kidney diseases, hepatobiliary disease, excessive alcohol consumption, malignancy, hypertension, diabetes mellitus, and patients with history of carotid artery surgery or stroke were excluded from the study. We also excluded patients with familial hypercholesterolemia, aortic dissection, or aortic aneurysm as well as patients with poor ultrasonographic recording quality with no clear delineation of the intima–media complex. In addition, patients taking any medical treatment in the last week were also excluded from the study. A positive exercise treadmill test was also an exclusion criterion in our study. The institutional ethics committee approved the study, and written informed consent for participation in the study was obtained from all individuals.
Age and gender were recorded, and body mass index was calculated as weight divided by height squared (kg/m2).
Blood Samples
Fasting blood samples were collected 1 day before TEE for the evaluation of LDL cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride, serum bilirubin level, and high-sensitivity C-reactive protein (hsCRP) levels. Plasma triglyceride, total cholesterol, LDL-C, HDL-C concentrations, and fasting glucose were measured using an automated chemistry analyzer (Aeroset; Abbott, Holliston, Minnesota) with commercial kits (Abbott). The hsCRP was measured using an autoanalyzer (Aeroset; Abbott) with a spectrophotometric commercial kit (Scil Diagnostics GmbH, Viernheim, Germany). Serum bilirubin levels were determined by colorimetric diazo method on the Aeroset System (Abbott Laboratories, Abbott Park, Illinois).
Transthoracic Echocardiography and TEE
Transthoracic echocardiography and TEE were performed on all study patients using a commercially available system (Vivid 7, GE Medical Systems, Horten, Norway). Left ventricular ejection fraction was determined using the modified Simpson method. 14 All patients underwent TEE with a multiplane transesophageal transducer after 4 hours of fasting prior to the procedure. Patients were placed in the left decubitus position with the left arm under the head, which was kept in a flexed position after oropharyngeal anesthesia with lidocaine spray. The transducer was introduced for visualization of the cardiac and aortic structures into the esophagus and gastric cavity through the mouth. An experienced cardiologist blinded to other laboratory results performed TEE. The TEE was well tolerated by all patients, and there were no complications. All studies were recorded and interpreted independently by an experienced observer.
Thoracic aortic IMT was defined as the distance from the leading edge of the lumen–intima interface to the leading edge of the media–adventitia interface of the far wall. The measurement of IMT in the thoracic aorta was made in 6 separate segments (length of 1 segment, 5 cm): ascending aorta, arch, from 0 to 5 cm distal to the arch, from 5 to 10 cm distal to the arch, from 10 to 15 cm distal to the arch, and from 15 to 20 cm distal to the arch. The maximum IMT was measured in each segment, and the mean value for the maximum IMT among the 6 segments was taken as the evaluable IMT of the thoracic aorta. 15 Sample measurement of the thoracic aortic IMT is shown in Figure 1.
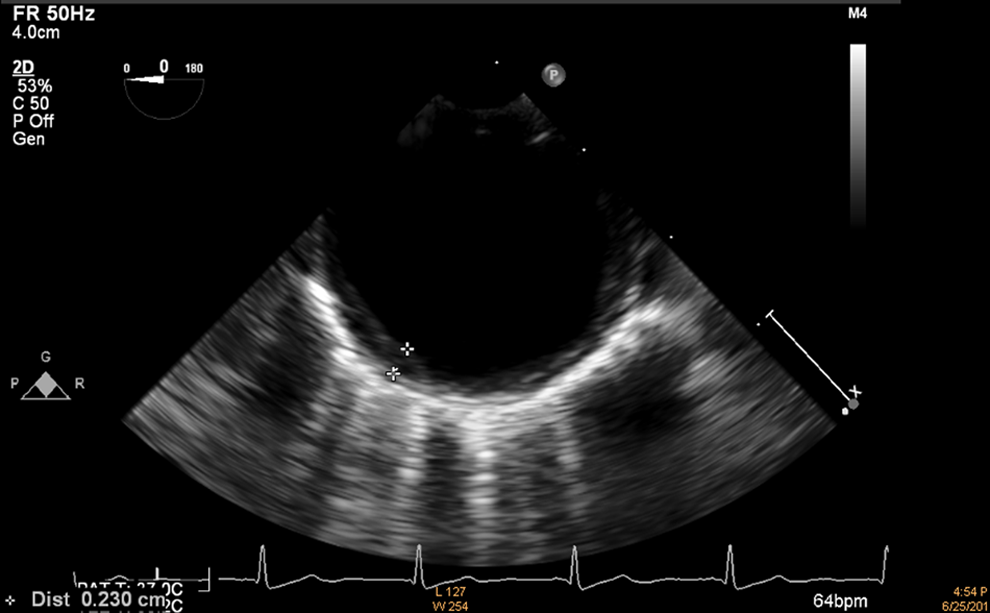
Measurement of thoracic aortic intima–media thickness.
Statistical Analysis
All analyses were conducted using SPSS 17.0 (SPSS for Windows 17.0, Chicago, Illinois). Comparison of categorical variables between the groups was performed using the chi-square test. Analysis of normality was performed using the Kolmogorov-Smirnov test. Independent samples t test was used for the analysis of continuous variables. The correlations between bilirubin and laboratory, hemodynamic, and echocardiographic parameters were assessed by the Pearson correlation test. A multivariate stepwise linear regression analysis was performed to identify the independent associations of bilirubin. All significant (P < .05) parameters in the univariate analysis (HDL-C level, hsCRP, and aortic IMT) were selected in the multivariate model. A 2-tailed P < .05 was considered significant.
Results
The baseline, clinical, laboratory, and echocardiographic characteristics of the groups are shown in Table 1. The highest aortic IMT values were observed in the bilirubinlow group compared with the bilirubinhigh group (23.3 ± 13.4 vs 13.5 ± 5.7 mm, P < .001). The hsCRP levels were significantly higher in the patients with lower serum bilirubin levels than in the patients with higher serum bilirubin levels (0.68 ± 0.42 vs 0.58 ± 0.34 mg/L, P = .012). The HDL-C levels were significantly higher in the bilirubinhigh group than in the bilirubinlow group (42.6 ± 9.2 vs 45.0 ± 12.2 mg/dL, P = .025).
Comparison of Baseline, Laboratory, Echocardiographic and Clinical Characteristics.
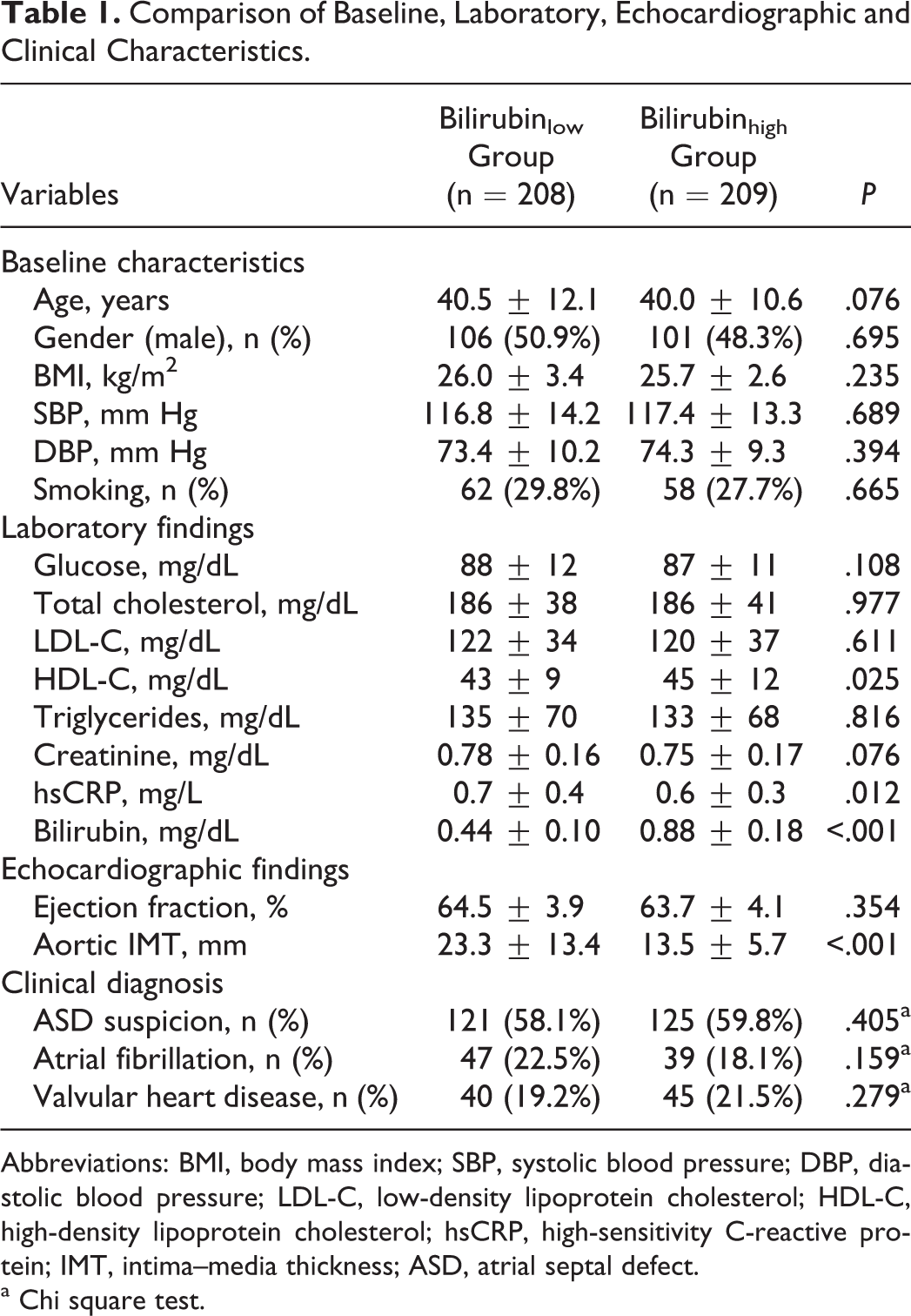
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; IMT, intima–media thickness; ASD, atrial septal defect.
a Chi square test.
Bivariate and multivariate relationships of serum bilirubin level were demonstrated in Table 2. Serum bilirubin level was found to be associated with HDL-C level (r = .162, P = .001), hsCRP (r = −.265, P < .001), and aortic IMT (r = −.551, P < .001) in bivariate analysis. The relationship between serum bilirubin level with aortic IMT is shown in Figure 2.
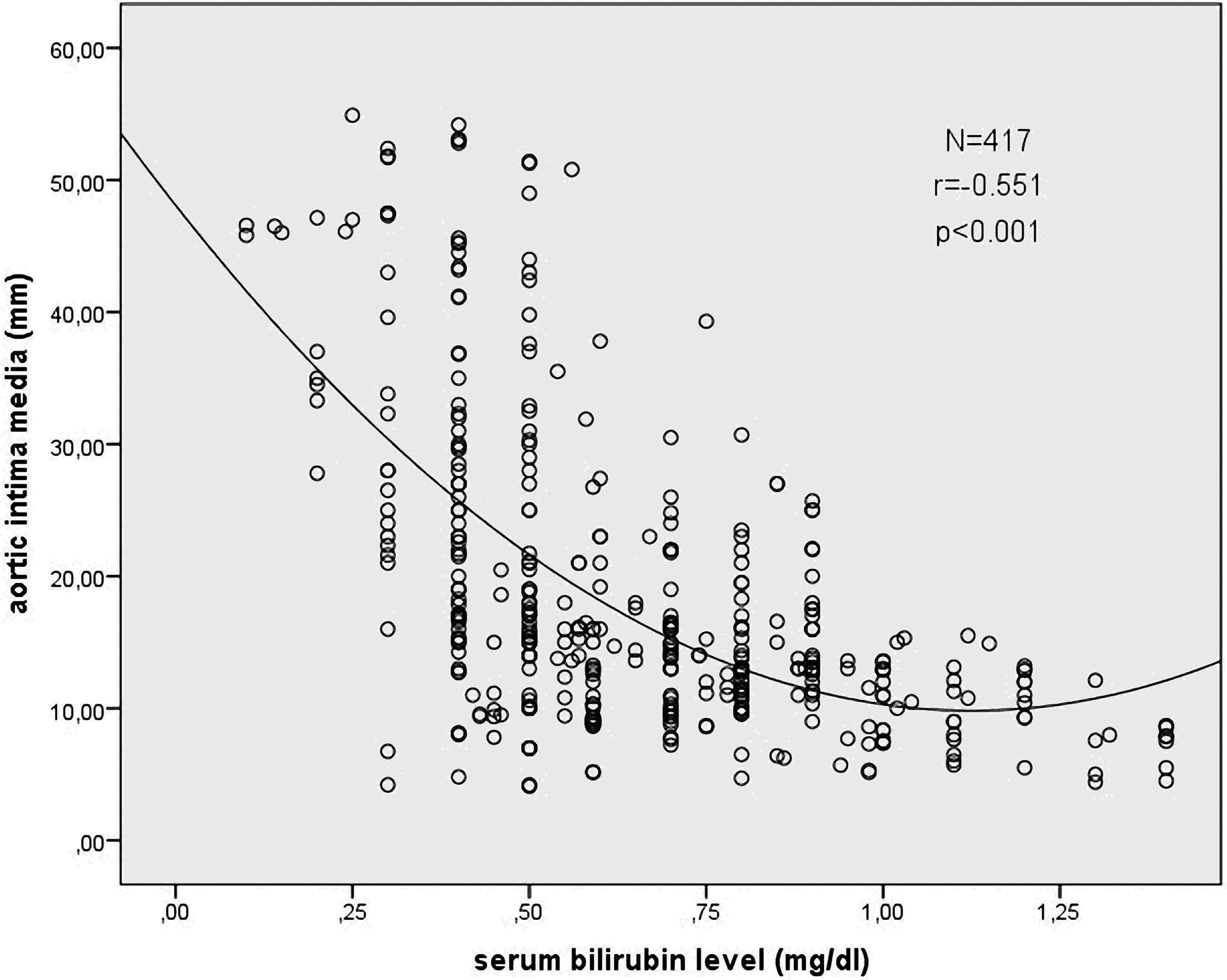
Relationship between serum bilirubin level and aortic intima–media thickness.
Bivariate and Multivariate Relationships of Serum Bilirubin Level.
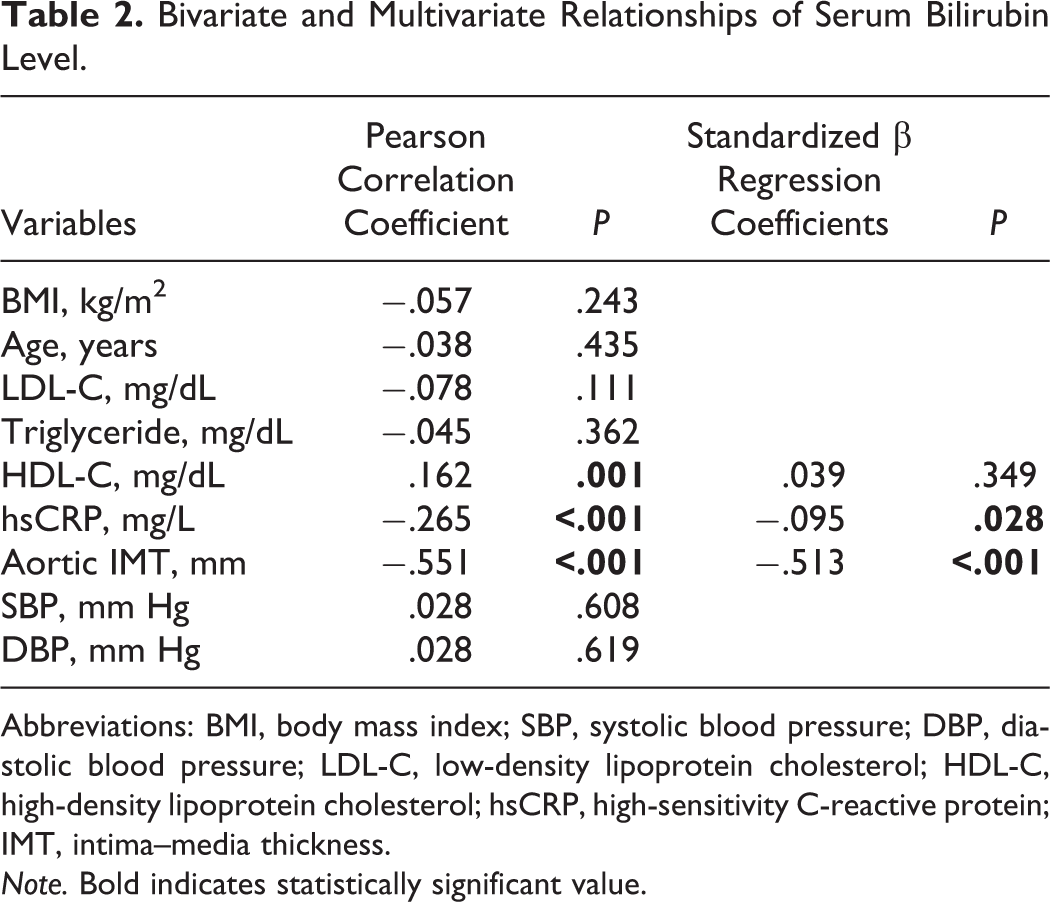
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; IMT, intima–media thickness. Note. Bold indicates statistically significant value.
Multivariate linear regression analysis showed that serum bilirubin level was independently related to hsCRP (β = −.095, P = .028) and aortic IMT (β = −.513, P < .001).
Discussion
This is the first study that investigated the relationship between serum bilirubin level and thoracic aortic IMT in patients without clinical manifestation of CVD. Our results showed that serum bilirubin level was independently associated with extent of thoracic aorta IMT as well as hsCRP.
Different circulating forms of bilirubin were found to be powerful antioxidants in several studies: Free bilirubin, albumin-bound bilirubin, conjugated bilirubin, and unconjugated bilirubin were all noted to be effective against peroxyl radicals and to be able to protect human LDL against peroxidation. 1,16 –19 Increased physiological concentrations of plasma bilirubin may reduce atherogenic risk because of its ability to serve as a potent lipid antioxidant under physiological conditions. 20,21 Supporting these findings, we observed an independent and inverse association between serum bilirubin level and thoracic aortic IMT. This finding is important even in the absence of clinical manifestations of CVD, because it may indicate a tendency to enhanced atherosclerosis in patients with lower serum bilirubin levels. In addition, we have shown that lower serum bilirubin levels are independently and inversely associated with an increased risk of developing atherosclerosis.
There is evidence that serum bilirubin level is a potential biochemical marker for the preclinical development of atherosclerosis. A relationship between serum bilirubin level and coronary and carotid atherosclerosis has been reported. 3 –10,22 Moreover, others 23 found a negative association between serum bilirubin level and peripheral arterial atherosclerosis. On the other hand, the present study showed that serum bilirubin levels within the “normal” range are associated with the extent of thoracic aortic IMT, which is a marker of preclinical systemic atherosclerosis. The thoracic aortic IMT was reported as an earlier marker of preclinical atherosclerosis than carotid IMT. 13 Mechanisms that explain the contribution of serum bilirubin level to the atherosclerotic process have not been fully clarified. Lipoproteins, and particularly LDL, are highly susceptible to oxidation, and it is known that the atherogenic process involves uptake of oxidized LDL by intimal macrophages, leading to the accumulation of lipid-rich foam cells. Given the antioxidant capacity of bilirubin, it is plausible that bilirubin protects lipids and lipoproteins against oxidation and thereby offers protection against atherogenesis. Accordingly, low bilirubin concentrations may be associated with increases in oxidized lipids and lipoproteins and, therefore, with enhanced atherogenic plaque formation. 7,24
In the present study, serum bilirubin level was independently associated with hsCRP levels. Atherosclerosis is generally accepted as a chronic inflammatory disorder. 25 Inflammation and oxidative stress are essential to the pathogenesis of atherosclerosis. 25 –27 Bilirubin is an antioxidant under physiological conditions. 1,28 With these properties, bilirubin may be able to inhibit multiple steps in atherogenesis. It is worth noting that we observed a strong inverse correlation between bilirubin and hsCRP, supporting the theory that bilirubin suppresses atherogenesis through inhibition of systemic inflammatory activity or that hsCRP levels fall because the process of atherosclerosis is attenuated.
The present study showed that there was a positive correlation between total bilirubin and HDL-C. However, this relationship was not observed in multivariate regression analysis. Furthermore, HDL-C levels were significantly higher in the higher serum bilirubin group than in the lower serum bilirubin group. Vitek et al 29 reported that bilirubin, total antioxidant capacity, and HDL-C were significantly higher in patients with Gilbert syndrome than in control patients. In addition, Yoshino et al 30 observed that the bilirubin level correlated positively with HDL-C level in patients without CAD. Because of its antioxidant properties, elevated bilirubin levels could protect LDL and lipids from being oxidized, so it reduces the catabolic rate mediated by the HDL receptor. 31 Thus, the beneficial effects of bilirubin can be thought as additive or synergistic to that of HDL-C.
Plasma bilirubin concentrations were found to be inversely correlated with several known CAD risk factors, such as age, obesity, smoking, systolic blood pressure, total cholesterol, HDL-C, and LDL-C in several studies. 32,33 Based on these findings, low bilirubin concentrations were suggested as an independent risk factor for CAD. Our study showed that lower serum bilirubin concentrations are an independent risk factor for subclinical thoracic aortic atherosclerosis.
In our study, the patient groups were enrolled from a diverse population with several disease states; however, bilirubin level was not related to the diagnosis of these patients. Additionally, coronary angiography was not performed in our patients although the diagnosis of CAD was excluded according to clinical characteristics and patient history, electrocardiography, and treadmill exercise test results. In addition, oxidative stress parameters were not investigated in the present study. This is a single-center and relatively small-scale cross-sectional study, and further investigations are needed to confirm our findings.
Serum bilirubin level is independently associated with both thoracic aortic IMT and hsCRP levels. Lower serum bilirubin level might be an independent predictor of subclinical thoracic atherosclerosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.