
Abstract
We determined whether exercise performance and lower extremity microcirculation were associated with endothelial cell inflammation, oxidative stress, and apoptosis and with circulating biomarkers of inflammation and antioxidant capacity in 160 patients with symptomatic peripheral artery disease (PAD). In a multivariate regression model for peak walking time, significant independent variables included ankle–brachial index (P < .001), age (P = .017), hydroxyl radical antioxidant capacity (P = .008), and endothelial cell nuclear factor K-light-chain-enhancer of activated B cells (NF-κB) activity (P = .015). In multivariate analyses for time to minimum exercise calf muscle hemoglobin oxygen saturation (StO2), significant independent variables included endothelial cell NF-κB activity (P = .043) and calf muscle StO2 at rest (P = .007). Endothelial cell inflammation and circulating biomarkers of inflammation and antioxidant capacity were associated with exercise performance and microcirculation of the ischemic calf musculature during exercise. The clinical implication is that interventions designed to alleviate endothelial cell inflammation and circulating inflammatory biomarkers, such as antioxidant therapy, may improve exercise performance of symptomatic patients with PAD.
Introduction
Peripheral artery disease (PAD) is a highly prevalent, 1 –3 costly, 4 –7 and deadly condition. 8,9 Furthermore, PAD is debilitating, as patients have ambulatory dysfunction, 10 impaired functional performance, 11,12 low physical activity levels, 13,14 and increased rates of functional decline and mobility loss compared to those without PAD. 11,12,15 In addition, we have recently shown that patients with PAD have higher levels of inflammation and lower levels of vascular endothelial growth factor A (VEGF-A) than healthy controls 16 and in controls with a high burden of comorbid conditions and cardiovascular risk factors. 17 The higher levels of circulating inflammatory markers in patients with PAD are associated with low intensity of community-based daily ambulation (ie, cadence), 18 low amounts of daily ambulation, 18 poor functional performance at baseline, 19,20 and functional decline over time. 21 However, it is not clear whether a heightened proinflammatory state in the circulation of symptomatic patients with PAD is associated with impairments in key outcome measures of exercise performance during a standardized treadmill test, such as claudication onset time (COT), peak walking time (PWT), and lower extremity microcirculation, as measured by calf muscle hemoglobin oxygen saturation (StO2). One potential defense to guard against negative consequences of inflammation is having higher levels of antioxidant capacity, but the influence of antioxidant capacity on exercise performance measures in symptomatic patients with PAD has not been examined.
In addition to the roles that systemic inflammation and antioxidant capacity may have on exercise performance and the microcirculation, biomarkers from the vasculature may have a stronger association with symptoms in patients with PAD. Endothelial dysfunction is an early marker of structural vascular changes and clinical symptoms, 22 –28 contributes to the progression of atherosclerosis, 28 and increases the risk of coronary events. 22,24,28 –30 We 31 and others 28 have found that endothelial function is impaired in patients with PAD. However, the association that endothelial cell function has with exercise performance and the microcirculation of symptomatic patients with PAD is less clear.
The aim of the study was to determine whether exercise performance and lower extremity microcirculation were associated with endothelial cell inflammation, oxidative stress, and apoptosis and with circulating biomarkers of inflammation and antioxidant capacity. We hypothesized that worse exercise performance and impaired lower extremity microcirculation are associated with greater endothelial inflammation, cellular reactive oxygen species (ROS) production, and apoptosis and with higher levels of circulating inflammatory biomarkers and lower levels of circulating antioxidant capacity.
Methods
Patients
Approval and informed consent
The institutional review board at the University of Oklahoma Health Sciences Center (HSC) and the Research and Development committee at the Oklahoma City Veterans Affairs (VA) Medical Center approved the procedures of this study. Written informed consent was obtained from each patient at the beginning of investigation.
Recruitment
Vascular laboratories and vascular clinics from the University of Oklahoma HSC and the Oklahoma City VA Medical Center referred patients for possible enrollment into an exercise rehabilitation program to treat leg pain secondary to PAD. 32
Medical Screening Through History and Physical Examination
Patients were evaluated in the morning at the Clinical Research Center, at the University of Oklahoma HSC. Patients arrived fasted but were permitted to take their usual medications. To begin the study visit, patients were evaluated with a medical history and physical examination in which demographic information, height, weight, waist circumference, 33 cardiovascular risk factors, comorbid conditions, claudication history, ankle–brachial index (ABI), blood samples, and a list of current medications were obtained.
Inclusion and exclusion criteria
Patients with PAD were included in this study if they met the following criteria: (1) a history of ambulatory leg pain, (2) ambulatory leg pain confirmed by treadmill exercise, 10 and (3) an ABI ≤0.90 at rest 2 or ≤0.73 after exercise. 34 Although there has been recent debate regarding the value of ABI as a measure to screen for PAD, 35,36 our decision to measure ABI both at rest and after treadmill exercise increases the sensitivity for detecting PAD and differentiates between vascular claudication and pseudoclaudiction, supported by a class 1 recommendation with level B evidence. 2 Another commonly used noninvasive vascular test to assess PAD is the determination of pulse volume recordings via photoplethysmography, 37 –39 but this technique is only supported by a class IIa recommendation with level B evidence. 2
Patients were excluded for the following conditions: (1) absence of PAD (ABI > 0.90 at rest and ABI > 0.73 after exercise), (2) noncompressible vessels (ABI > 1.40), (3) asymptomatic PAD, (4) use of medications indicated for the treatment of claudication (cilostazol or pentoxifylline) initiated within 3 months prior to investigation, (5) exercise limited by other diseases or conditions, (6) active cancer, (7) end-stage renal disease defined as stage 5 chronic kidney disease, and (8) abnormal liver function. A consecutive series of 225 individuals were evaluated for eligibility, and 160 patients were deemed eligible for inclusion into the study and 65 patients were ineligible.
Measurements
Graded treadmill test: COT, PWT, and calf muscle StO2
Patients performed a graded treadmill test to determine study eligibility and to obtain outcome measures. 10 The COT and PWT were measured and are highly reliable, as previously described. 10 Calf muscle StO2 was measured with the treadmill test using a continuous-wave, NIRS unit (InSpectra model 325; Hutchinson Technology, Inc, Hutchinson, Minnesota), an optical cable attached to a 25-mm probe, InSpectra software (version 2.0), and a dedicated laptop computer as previously described. 40
Blood sampling
Blood was drawn by venipuncture from an antecubital vein, collected in vacutainers, and distributed in 0.5 mL aliquots. The samples were stored at −80°C and were subsequently batched for analysis in duplicate in our laboratory at the Reynolds Oklahoma Center on Aging.
Endothelial cell cultures
A cell culture-based bioassay approach utilizing cultured primary human arterial endothelial cells was used to characterize the endothelial effects of circulating factors present in the sera of patients. In brief, endothelial cells (purchased from Cell Applications, Inc, San Diego, California, after passage 4; age of the donors is unknown) were initially cultured in MesoEndo Endothelial Cell Growth Medium (Cell Applications, Inc) followed by endothelial basal medium supplemented with 10% fetal calf serum until the time of serum treatment, as described. 17,41 Cells were 80% to 90% confluent before treatment with sera. Interindividual variance is unlikely to contribute to observed differences because detector cells used for each in vitro study were from the same donor. For treatment, fetal calf serum was replaced with serum (10%; for 24-48 hours) collected from our patients. 17 Cells cultured in endothelial basal medium supplemented with 10% fetal calf serum served as an additional control.
Apoptosis assay
Cultured endothelial cells were treated with sera from patients for 24 hours. Caspase activities using Caspase-Glo 3/7 assay kit (Promega, Madison, Wisconsin) were measured to assess apoptotic cell death, as previously reported. 17
Cellular ROS production
Hydrogen peroxide production in detector endothelial cells was measured fluorometrically by a Tecan Inifinite M200 (Tecan Group Ag, Mannedorf, Switzerland) using the Amplex Red/horseradish peroxidase assay (Life Technologies, Grand Island, New York) to determine cellular oxidative stress induced by the factors present in the sera. 17
Transient transfection, nuclear factor K-light-chain enhancer of activated B cells reporter gene assay
Transcriptional activity of nuclear factor K-light-chain-enhancer of activated B cells (NF-κB) was tested in serum-treated detector endothelial cells by a reporter gene assay to determine cellular proinflammatory effects induced by factors in the sera. 17 Transfections in endothelial cells were performed using the Amaxa Nucleofector technology (Amaxa, Gaithersburg, Maryland), as we have previously reported. 17
Serum antioxidant capacity
Hydroxyl radical antioxidant capacity (HORAC) using the OxiSelect HORAC Activity Assay (Cell Biolabs Inc, San Diego, California) was measured from sera to determine the capacity of antioxidant enzymes and other redox molecules to counterbalance the deleterious effects of oxidative stress in the sera of patients. 17
Circulating inflammatory and vascular biomarkers
A Milliplex Human Adipokine Magnetic Bead Kit was used for determining tumor necrosis factor α, interleukin (IL) 1b, IL-6, IL-8, monocyte chemotactic protein 1, hepatocyte growth factor, and nerve growth factor. A Milliplex Human Cardiovascular Disease Panel 1 Kit was used for myeloperoxidase, matrix metallopeptidase 9 (MMP-9), E selectin, vascular cell adhesion molecule 1 (VCAM-1), intercellular cell adhesion molecule 1 (ICAM-1), and plasminogen activity inhibitor 1. A Milliplex Human Apolipoprotein Kit was used for apolipoprotein B and apolipoprotein CIII. The Millipore kits were purchased from EMD Millipore (Billerica, Massachusetts). Affymetrix Procarta Immunoassay was used to detect serum amyloid A, VEGF-A, and adiponectin. These assays were performed according to manufacturer’s protocols by a Bio-Plex 200 System (Bio-Rad, California) at the Core Facility, University of Oklahoma HSC). Sample protein content was determined for normalization purposes by a spectrophotometric quantification method using BCA reagent (Pierce Chemical Co, Rockford, Illinois).
High-sensitivity C-reactive protein
Concentration of high-sensitivity C-reactive protein (HsCRP) was quantified from 300 μL of sera using a high-sensitivity near infrared particles immunoassay. The SYNCHRON LX-20 (Beckman-Coulter, California), a commercially available device, was used to perform the assay. Prior to performing each assay, the SYNCHRON system was calibrated, and a calibration curve was established. 42
Statistical Analyses
Measurement variables were summarized in Tables 1 and 2 by reporting means and standard deviations and dichotomized variables by reporting percentages. Associations reported in Table 3 are Pearson partial correlation coefficients or Spearman partial correlation coefficients (indicated in italics), controlled for age, sex, race, ABI, current smoking, body mass index, and obesity. Spearman was reported if the 2 correlations differ by more than .1. A stepwise regression procedure with entry P value set at .05 was used to obtain regression models of Table 4.
Clinical Characteristics of 160 Symptomatic Patients With Peripheral Artery Disease.a
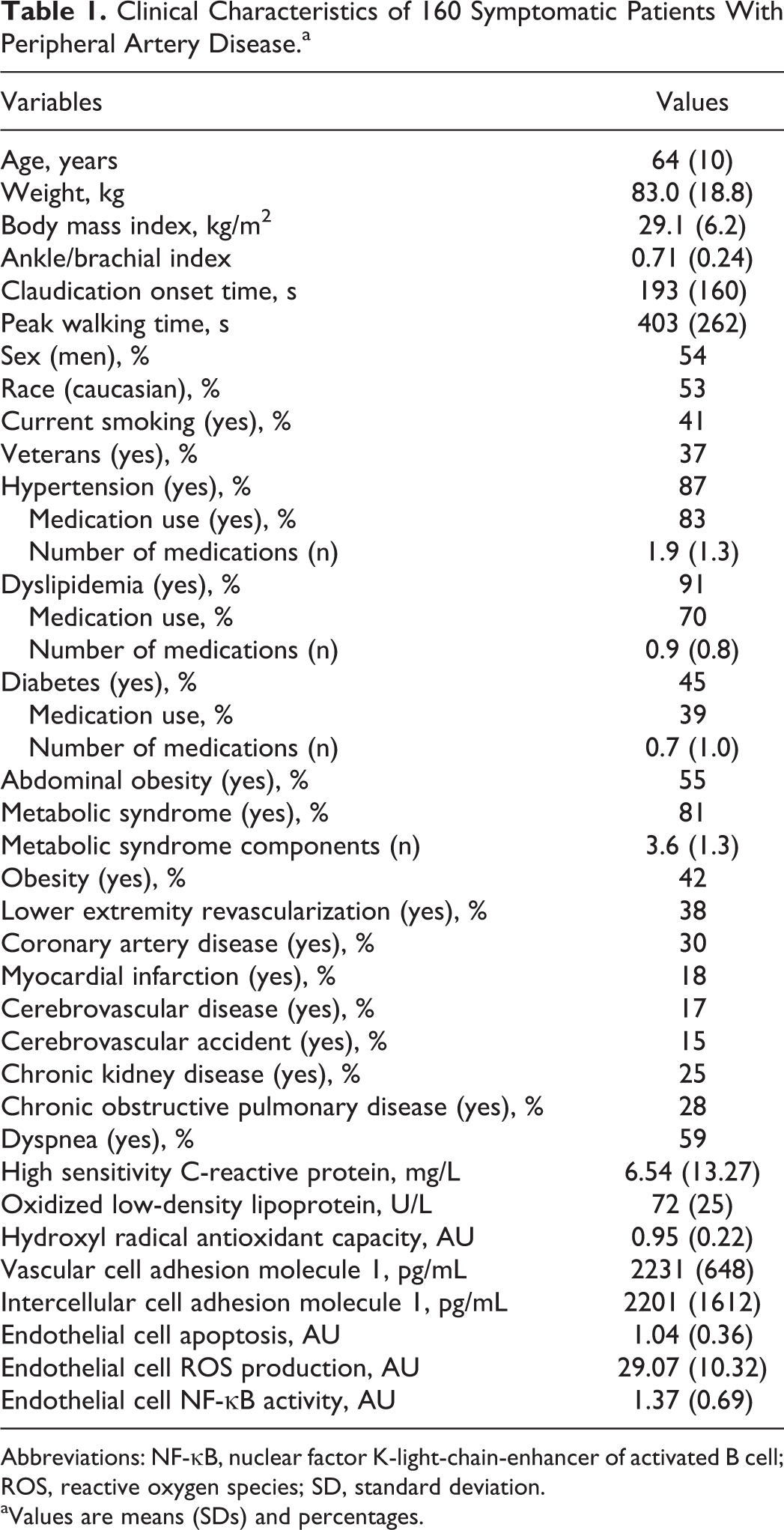
Abbreviations: NF-κB, nuclear factor K-light-chain-enhancer of activated B cell; ROS, reactive oxygen species; SD, standard deviation.
aValues are means (SDs) and percentages.
Measures of Calf Muscle Hemoglobin Oxygen Saturation (StO2) During Treadmill Evaluation in Symptomatic Patients With Peripheral Artery Disease.a
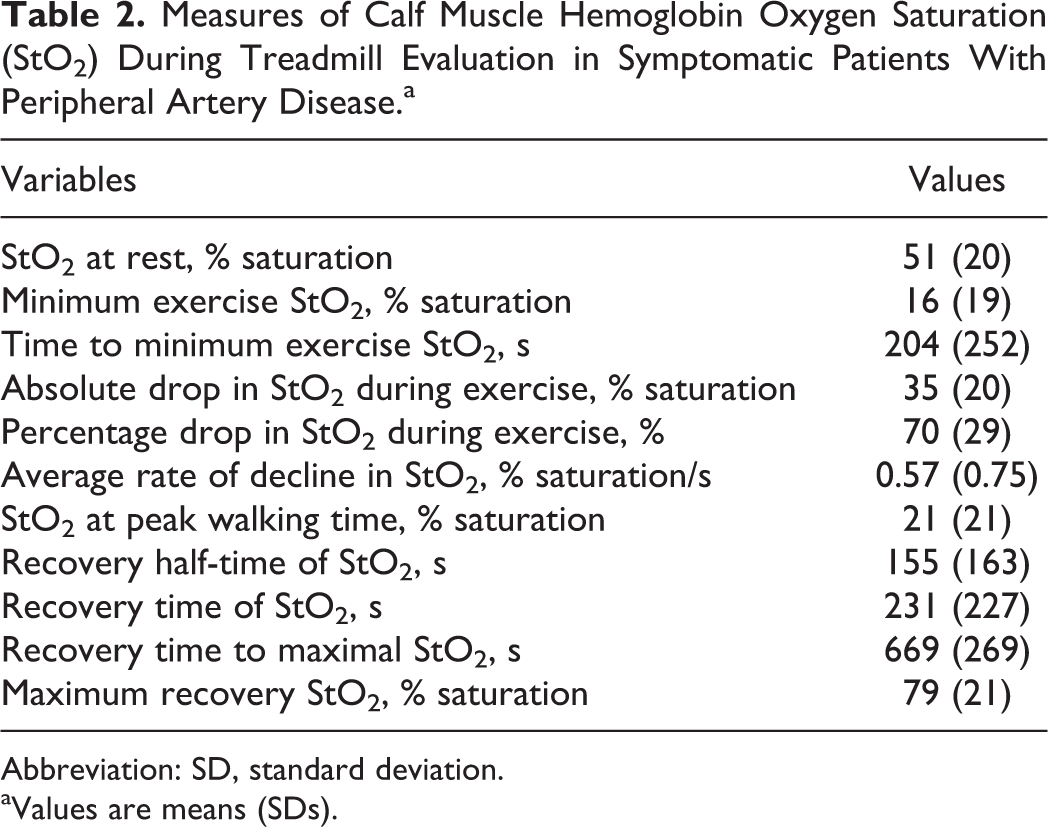
Abbreviation: SD, standard deviation.
aValues are means (SDs).
Associations Among Measures of Exercise Performance, Microcirculation, and Measures of Circulating Antioxidant Capacity, Inflammation, and Cultured Endothelial Cells Treated With Sera in Symptomatic Patients With Peripheral Artery Disease.a
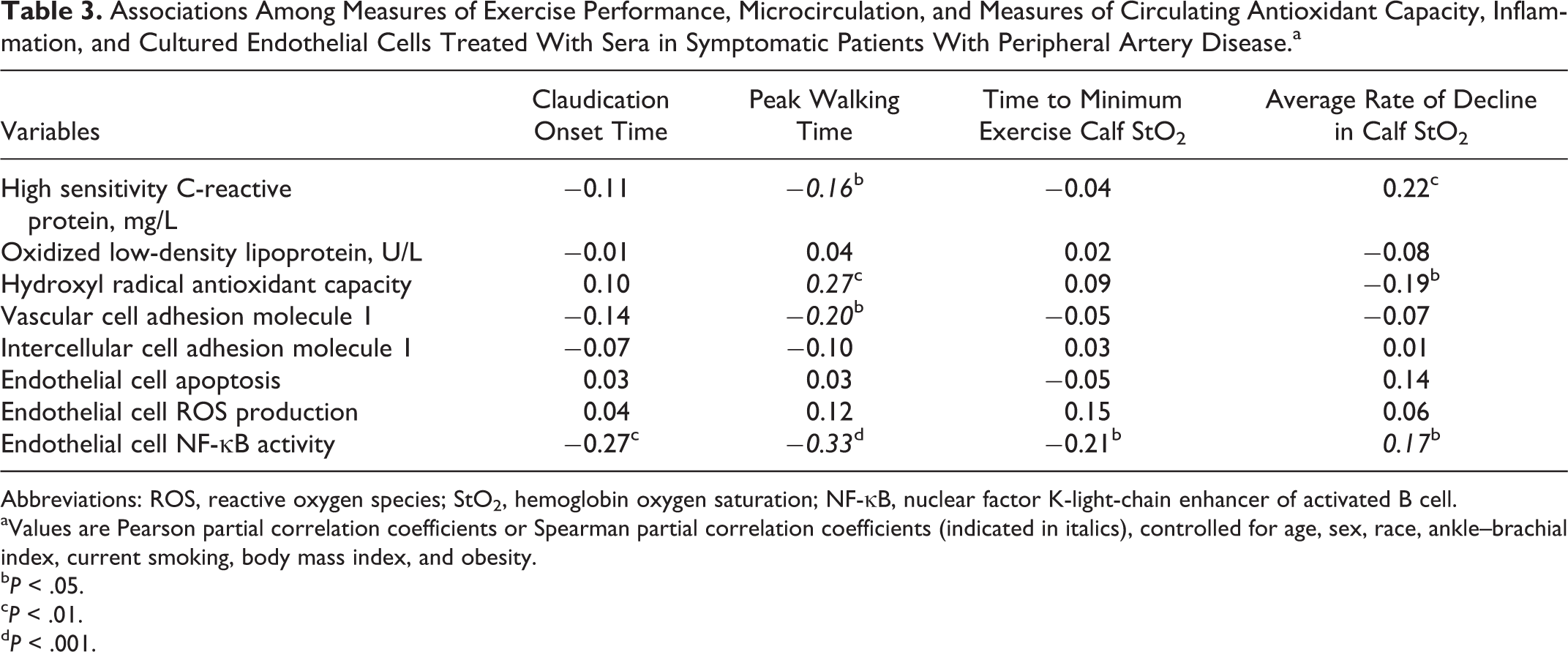
Abbreviations: ROS, reactive oxygen species; StO2, hemoglobin oxygen saturation; NF-κB, nuclear factor K-light-chain enhancer of activated B cell.
aValues are Pearson partial correlation coefficients or Spearman partial correlation coefficients (indicated in italics), controlled for age, sex, race, ankle–brachial index, current smoking, body mass index, and obesity.
b P < .05.
c P < .01.
d P < .001.
Regression Coefficient Summary for Independent Variables Included in Multivariate Regression Models for Exercise Performance and Microcirculation-Dependent Variables in Symptomatic Patients With Peripheral Artery Disease.
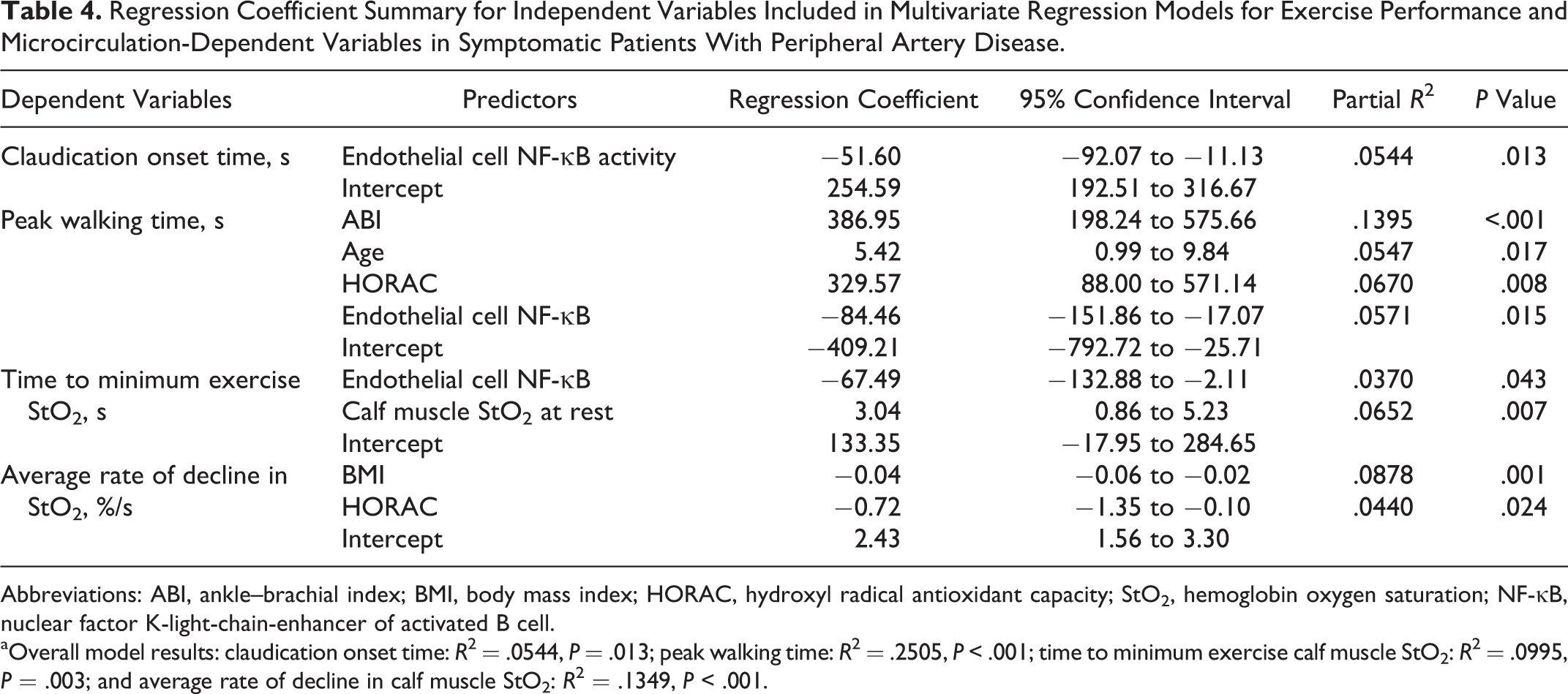
Abbreviations: ABI, ankle–brachial index; BMI, body mass index; HORAC, hydroxyl radical antioxidant capacity; StO2, hemoglobin oxygen saturation; NF-κB, nuclear factor K-light-chain-enhancer of activated B cell.
aOverall model results: claudication onset time: R 2 = .0544, P = .013; peak walking time: R 2 = .2505, P < .001; time to minimum exercise calf muscle StO2: R 2 = .0995, P = .003; and average rate of decline in calf muscle StO2: R 2 = .1349, P < .001.
Results
The clinical characteristics of 160 patients with claudication are shown in Table 1. The group consisted of a mix of older, abdominally obese caucasian and African American men and women. Cardiovascular risk factors were highly prevalent in the group, particularly hypertension, dyslipidemia, and metabolic syndrome. Consequently, 83% of patients were treated for hypertension, 70% were treated for dyslipidemia with statin medication, and 39% were treated for diabetes.
The calf muscle StO2 measures of the group are shown in Table 2. On average, calf muscle StO2 decreased 70% from rest to the mean minimum value attained 204 seconds after the initiation of exercise. At the completion of exercise, the mean time for calf muscle StO2 to increase to half of the resting value was 155 seconds, whereas full recovery was reached at 231 seconds. Calf muscle StO2 continued to increase to an average maximum value of 79% saturation 669 seconds after completion of exercise.
The correlation coefficients between measures of exercise performance and measures of circulating antioxidant capacity, inflammation, and cultured endothelial cells treated with sera in patients with PAD are shown in Table 3. After adjusting for age, sex, race, ABI, current smoking, BMI, and obesity, PWT was correlated with HsCRP (P < .05), HORAC (P < .01), VCAM-1 (P < .05), and endothelial cell NF-κB activity (P < .001). Furthermore, COT and the time to minimum exercise calf StO2 were correlated with endothelial cell NF-κB activity (P < .01 and P < .05, respectively), and the average rate of decline in calf StO2 was correlated with hsCRP (P < .01), HORAC (P < .05), and endothelial cell NF-κB activity (P < .05).
Multivariate regression models to predict exercise performance are shown in Table 4. For COT, the significant independent variable was endothelial cell NF-κB activity (P = .013), and for PWT, the significant independent variables included ABI (P < .001), age (P = .017), HORAC (P = .008), and endothelial cell NF-κB activity (P = .015). For the time to minimum exercise calf muscle StO2, the significant independent variables included the calf muscle StO2 measured at rest (P = .007), and endothelial cell NF-κB activity (P = .043), and for the average rate of decline in calf muscle StO2, the significant independent variables included BMI (P < .001) and HORAC (P = .024).
Discussion
The primary novel finding was that higher endothelial cell NF-κB activity was associated with lower PWT, lower COT, and shorter time to minimum calf muscle StO2 during exercise. Another novel finding was that higher levels of circulating hsCRP and VCAM-1 were associated with lower PWT, and that higher circulating HORAC was associated with higher PWT and with slower average rate of decline in calf muscle StO2 during exercise. The clinical significance is that new treatments designed to reduce endothelial cell inflammation and circulating inflammatory biomarkers and to increase antioxidant capacity, might be efficacious to improve microvascular function and ambulation in patients with PAD. New treatments could include various antioxidant supplements to reduce inflammation and oxidative stress, to be taken in combination with, or separate from, exercise therapy. Increased intake of antioxidants could also occur from dietary intervention designed to consume fruits and vegetables rich in antioxidants. Statin medications could be another treatment approach, as they have been found to improve ambulation in patients with PAD, 43 and we have found that apolipoprotein subparticle profiles are better in patients with PAD who are prescribed statins. 44 However, it is not clear whether statin therapy would alter the inflammatory biomarkers measured in this study. The methodology of this study utilizing the Gardner-Skinner-graded treadmill protocol to measure COT and PWT 10 with concomitant measurement of calf muscle oxygenation using near-infrared spectroscopy, along with the assays described in this report, would be appropriate techniques to assess efficacy of new treatments designed to improve inflammation, ambulation, and microvascular function in patients with PAD.
Endothelial Cell NF-κB Activity was Negatively Associated With Exercise Performance and Calf Muscle StO2
This is the first study to report that endothelial cell NF-κB activity was associated with PWT and COT during standardized treadmill exercise in symptomatic patients with PAD, as well as with calf muscle StO2 during exercise. Thus, endothelial cell inflammation is associated with worse leg symptoms and microcirculation of the ischemic calf musculature. The negative association between endothelial cell NF-κB activity and PWT was significant even after adjusting for ABI, age, and HORAC levels. This finding suggests that endothelial cell NF-κB activity may be associated with peak exercise performance independent of the severity of PAD in the large arteries, age, and antioxidant capacity. This observation was confirmed by noting that higher endothelial cell NF-κB activity was also associated with shorter COT and with faster oxygen desaturation of the calf musculature during exercise. Collectively, our results indicate that endothelial cell inflammation was negatively associated with exercise performance in symptomatic patients with PAD.
Circulating Inflammatory Biomarkers Were Negatively Associated With Exercise Performance and Calf Muscle StO2
Another observation was that after adjusting for age, sex, race, ABI, current smoking, BMI, and obesity, PWT was correlated with HsCRP and VCAM-1, and the average rate of decline in calf StO2 was also associated with HsCRP. Our results indicate that circulating inflammatory biomarkers were negatively associated with both leg symptoms and the microcirculation of the ischemic calf musculature. These findings support an earlier study from our laboratory that daily ambulatory cadence as well as the total number of daily strides and minutes spent ambulating were associated with HsCRP in symptomatic patients with PAD.
18
The current study also supports work that higher levels of circulating inflammatory biomarkers consisting of hsCRP, IL-6, VCAM-1, ICAM-1, homocysteine, and
Circulating Antioxidant Capacity was Positively Associated With Exercise Performance and Calf Muscle StO2
This is the first study to report that higher circulating HORAC values were correlated with PWT during standardized treadmill exercise and with a slower average rate of decline in calf muscle StO2 during exercise. Thus, circulating antioxidant capacity was positively related to both leg symptoms and the microcirculation of the ischemic calf musculature during exercise. For PWT, the positive association with HORAC was evident after adjusting for ABI, age, and endothelial cell NF-κB activity. Consequently, higher circulating HORAC levels were associated with better ambulation independent of the severity of PAD, age, and endothelial cell inflammation in symptomatic patients. Furthermore, higher circulating HORAC levels were correlated with slower oxygen desaturation of the calf musculature during exercise after adjusting for BMI, suggesting that antioxidant capacity was positively related to the microcirculation of the calf musculature in symptomatic patients regardless of whether they were obese, overweight, or of normal weight. Collectively, our results suggest that interventions designed to increase HORAC levels may improve claudication and the calf microcirculation. An important source of antioxidants is dietary intake of fruits and vegetables. We have previously reported that patients with PAD have diets low in fruits and vegetables, indicated by low intake of fiber, as only 26% of patients met the daily recommendation for dietary fiber. 45 There is a relationship between increased fiber intake and lower hsCRP, 46 suggesting that greater fruit and vegetable consumption may enhance HORAC and thereby lower inflammation.
Limitations
There are limitations to this study. A self-selection bias may exist regarding study participation, as patients who participated in this trial were volunteers. Therefore, they may represent those who were more interested in participation, who had better access to transportation to the research center, and who had relatively better health than patients who did not volunteer. Furthermore, the results of this study are only applicable to symptomatic patients with PAD and may not be generalized to asymptomatic patients and patients with more severe forms of PAD, such as critical limb ischemia. Another limitation is that we did not have a healthy control group to examine whether relationships exist among inflammation, antioxidant capacity, exercise performance, and microcirculation or whether these relationships are unique to patients with PAD. Finally, there are limitations associated with the design of the study. Significant association found among variables in the patients measured at baseline does not provide evidence of causality. Although these limitations exist, we believe that the findings of the present study are generalizable to the large number of symptomatic patients with PAD because women and African Americans are well represented, and typical risk factors for PAD such as dyslipidemia, hypertension, obesity, diabetes, and smoking are highly prevalent.
Conclusion and Clinical Significance
Endothelial cell inflammation and circulating biomarkers of inflammation and antioxidant capacity were associated with exercise performance and microcirculation of the ischemic calf musculature during exercise. The clinical implication is that interventions designed to alleviate endothelial cell inflammation and circulating inflammatory biomarkers, such as antioxidant therapy, may improve exercise performance of symptomatic patients with PAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by grants from the National Institute on Aging (R01-AG-24296 to AWG, AG031085 to AC, and AG038747 to WES), Oklahoma Center for the Advancement of Science and Technology (to AWG, AC, WES, and ZU), and General Clinical Research Center (M01-RR-14467), the American Heart Association (to AC and ZU), the National Center for Complementary and Alternative Medicine (R01-AT006526 to ZU), and the Ellison Medical Foundation (to WES).