
Abstract
Peripheral arterial disease (PAD) and chronic kidney disease (CKD) are associated with increased mortality rates. We assessed long-term outcomes of patients with PAD and CKD. Patients with PAD undergoing invasive angiography and/or endovascular revascularization between 2005 and 2010 were retrospectively classified into 5 CKD stages. A follow-up was performed and 572 patients were included, 116 patients (20%) had normal renal function, 245 were in CKD stage 2 (43%), 156 in CKD stage 3 (27%), and 55 in CKD stages 4 + 5 (10%). Diabetes mellitus, hypertension, and anemia were more frequent in higher CKD stages (P < .03). During follow-up (mean 1135 days; 95% confidence interval 1159-1259), cumulative mortality was 21% and increased with advanced CKD stages (9%, 16%, 29%, and 47%, respectively, P < .001). In multivariate Cox regression models, higher CKD stages were significantly associated with poor survival. Medication adherence for secondary prevention was significantly lower than recommended but irrespective of CKD stages. Kidney function is an independent predictor of worse long-term survival in patients with PAD. While standard medications were used less often than recommended, no differences between CKD stages were noted.
Keywords
Introduction
Peripheral arterial disease (PAD) affects large proportions of the general population. Prevalence ranges from 4.5% to 14.5%, increasing with advancing age. 1 –3 Major implications include increased amputation rates, elevated cardiovascular (CV), and overall mortality involving serious economic consequences due to the need for frequent and prolonged hospital stays including invasive treatment strategies. 4
Chronic kidney disease (CKD) is another common morbidity predominantly occurring in the elderly population with a prevalence varying from 23% to 36%. 5 Chronic kidney disease results in high morbidity and mortality rates 5 and is an independent risk factor for both CV and overall mortality. 6 –11 Further, CKD has been shown to be an independent risk factor for PAD. 1,12 The combined occurrence of PAD and CKD together may lead to a cumulative unfavorable outcome including increased mortality.
Previously published studies have demonstrated worse survival rates in patients with PAD having impaired kidney function. 13 –15 No data concerning long-term mortality in an all stages cohort of patients with PAD with respect to exact CKD stages are available to date. This might be due to the fact that patients with risk factors affecting survival are often excluded from randomized trials, and therefore conclusions concerning mortality rates are only valid for a trial-specific patient population.
Additionally, adherence to medication recommendations concerning secondary prevention of disease progression has been shown to be poor in patients with CKD. 16 –20 Again, data for long-term medication adherence according to recent guideline recommendations are lacking. In this study, we investigated the stage-specific impact of CKD on the outcome of patients with PAD, including a long-term follow-up. In addition, guideline adherence with respect to secondary prevention medication was examined.
Methods
A total of 582 consecutive patients with symptomatic PAD underwent diagnostic catheter-based angiography and, if necessary, angioplasty in our institution between January 2005 and January 2010. According to the institution policy, written informed consent was obtained from each patient prior to treatment. All patients received blood sampling for sodium, potassium, gamma-glutamyl transpeptidase, urea, creatinine, thyroid-stimulating hormone, hemoglobin, hematocrit, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, thrombocyte count, thromboplastin time, and partial thromboplastin time 1 day prior to the procedure. Patients with previously impaired kidney function (estimated glomerular filtration rate, eGFR, <60 mL/min/1.73m 2 ) received intravenous prehydration consisting of 0.9% saline supplemented with 1200 mg of n-acetyl-cysteine both 12 hours before and 12 hours after the procedure.
Angiography and all angioplasty treatments were performed under local anesthesia. All procedures were performed in the catheter laboratory using fluoroscopic guidance and nonionic iso-osmolar contrast media iopromide (Ultravist 370 (TM), Schering AG, Berlin, Germany).
Peripheral arterial disease was classified according to Fontaine stages I to IV. Information about previously underlying comorbidities was retrieved from the electronic patient record system of our institution.
Determination of Renal Function
Renal function at baseline was determined from serum creatinine measured by the method of Jaffé. 21 Since creatinine is known to be an insufficient marker of renal function but eGFR is considered most suitable, we used the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation for calculation 22 :
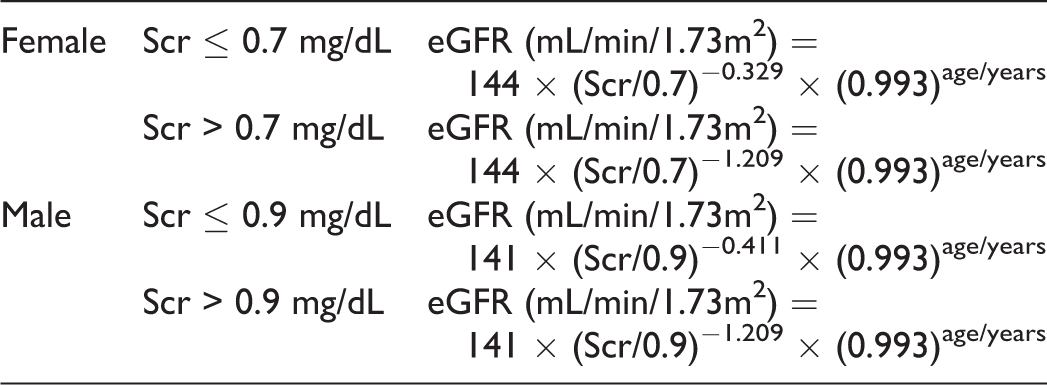
Based on the results of the eGFR, patients were classified into 5 groups of CKD in accordance to the classification of the National Kidney Foundation 23 as follows: stage 1: eGFR ≥90 mL/min/1.73m2; stage 2: eGFR 60 to 89 mL/min/1.73m2; stage 3: eGFR 30 to 59 mL/min/1.73mL 2 ; and stage 4 + 5: eGFR <30 mL/min/1.73m2. Since information about proteinuria was missing, we cannot exclude those patients in CKD stage 1 who had no CKD.
Follow-Up
Each patient was contacted by postal mail and asked to fill out a questionnaire concerning recent PAD symptoms such as pain-free walking distance or the implementation of recurrent percutaneous transluminal angioplasty (PTA), peripheral bypass surgery, or amputation. Additional follow-up information was retrieved from medical records of our institution or, if necessary, by contacting referring physicians. Further, major CV clinical end points, such as recent history of myocardial infarction, new onset of malignancy, were evaluated.
Ethical approval of the questionnaire was obtained from the Ethics Committee Landesaerztekammer Westfalen-Lippe, Muenster, Germany (AZ.:2010-208-f-S). If no response was obtained, patients or their referring general practitioners were contacted by telephone in order to complete missing follow-up information.
Blood Pressure Measurement for Ankle Brachial Index Calculation
Systolic blood pressure (BP) was measured bilaterally on brachial, tibial, and dorsal pedal arteries in the supine position with MultiDop Pro (Compumedics, Germany GmbH) Doppler ultrasound using a 8 MHz probe. Occluding cuffs were positioned right above the malleoli for ankle pressure measurement.
The ankle brachial index (ABI) values were calculated by the highest pressure on the dorsal pedal and posterior tibial artery and by the brachial artery pressure on either side. The lowest ABI values were used for analysis. The ABI values <0.9 and >1.4 were considered pathological.
Statistics
Differences in basic clinical characteristics between groups were tested by chi-square test for categorical variables and by analysis of variance F test for continuous variables. The P values for all tests are shown in Tables 1- 3. Differences among groups concerning concomitant medication were evaluated by the McNemar test.
Baseline Characteristics Depending on CKD stages.a
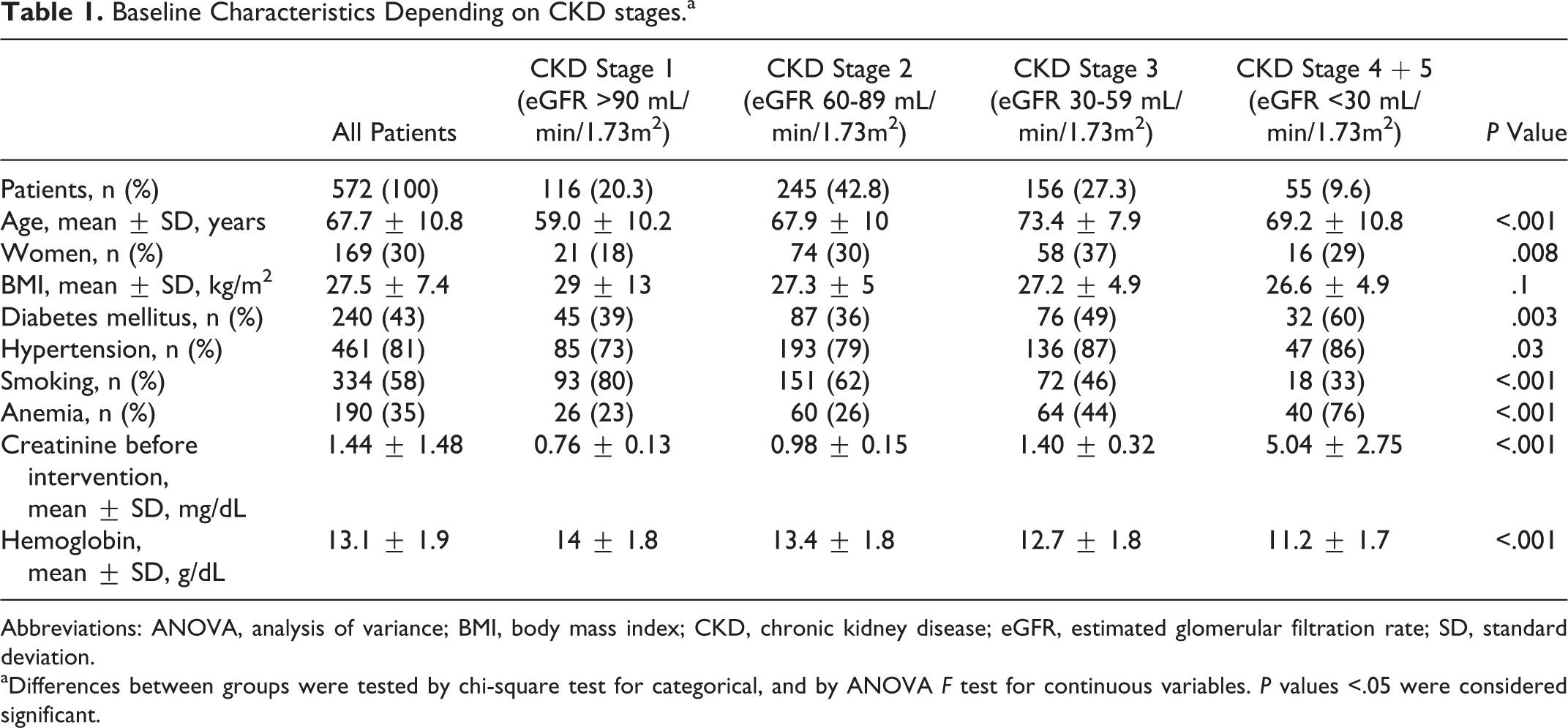
Abbreviations: ANOVA, analysis of variance; BMI, body mass index; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; SD, standard deviation.
aDifferences between groups were tested by chi-square test for categorical, and by ANOVA F test for continuous variables. P values <.05 were considered significant.
Univariate predictors of mortality during follow-up were analyzed by Cox regression, and calculation of hazard rate ratios (HRRs) with 95% confidence intervals (95% CIs) was carried out. Multivariate analysis of mortality was performed by Cox regression analyses with potential covariates (sex, age, diabetes, anemia, and PAD stages; adjusted HRR). For all tests, 2-sided P values <.05 were considered significant. All statistical analyses were performed with PASW 20.0 for Windows or MedCalc 12.7.4.0.
Results
This study includes 582 consecutive patients with symptomatic PAD undergoing invasive diagnostic and if necessary endovascular revascularization between 2005 and 2010. Creatinine values were missing in 10 patients, and these patients were excluded from the analysis. Since only few patients were in CKD stage 4 (n = 19) and stage 5 (n = 36), these subgroups were merged into one group. Patient selection and classification are depicted in Figure 1.
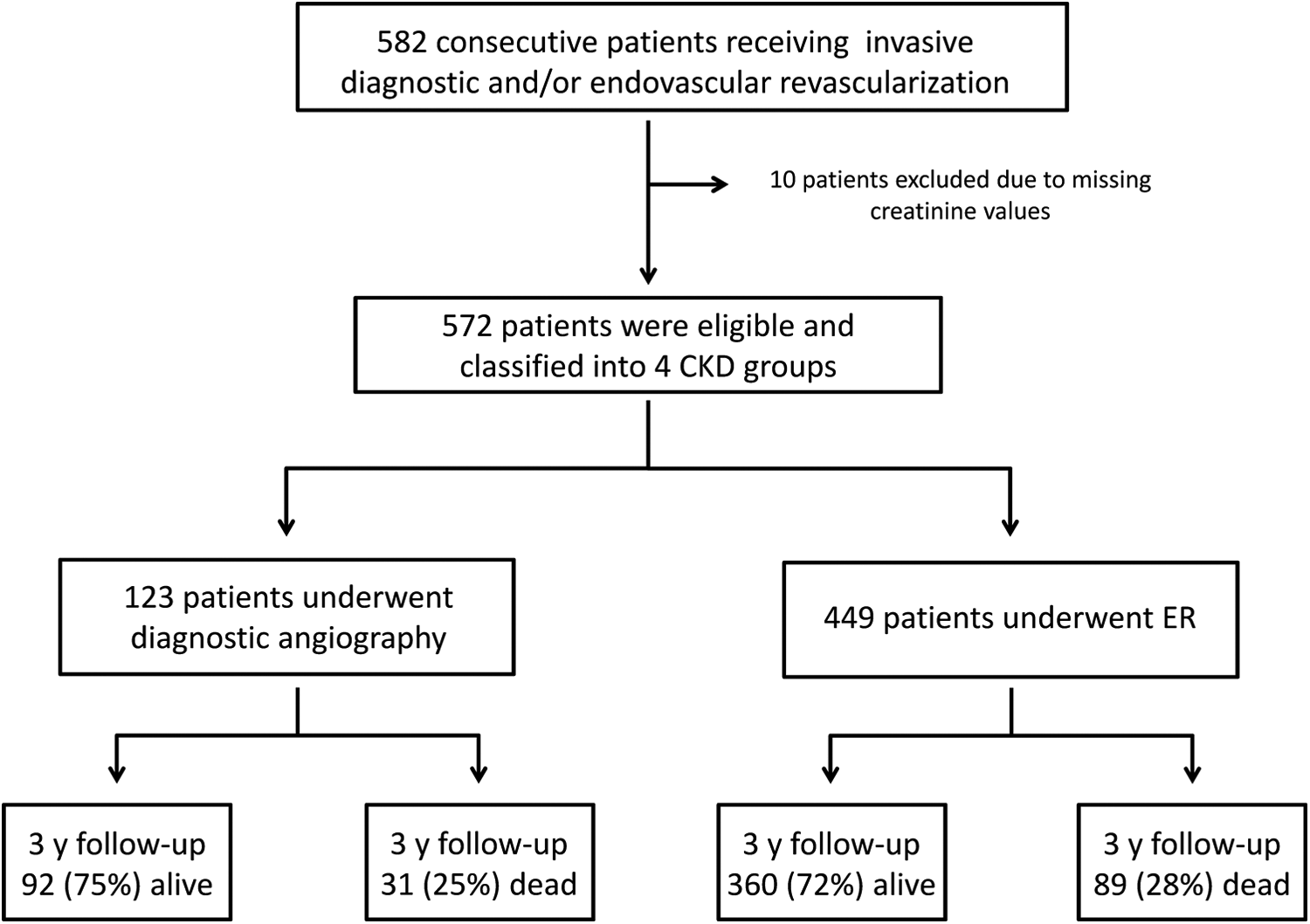
Flowchart depicting the classification of the patients according to chronic kidney disease (CKD) stages and intervention. ER, endovascular revascularization; y, years.
Baseline characteristics depending on CKD stages are shown in Table 1. The mean age in the entire cohort (n = 572) was 67.7 ± 10.8 years, and 30% of the patients were female, each with significant distribution among CKD stages 1 to 4. There were no significant differences concerning patient height and weight among all CKD stages.
Diabetes mellitus was present in 43%, hypertension in 81%, 58% were smokers, and 35% were anemic (P < .05 for all comorbidities, differences among CKD groups). More advanced stages of CKD had significantly more diabetics, anemia, and hypertension than early CKD stages, whereas the number of smokers declined with each CKD stage. Hemoglobin and serum creatinine values differed significantly among CKD groups (Table 1), and the amount of contrast media for angiography was lowest in CKD stages 4 + 5 (P = .031; Table 2).
Periprocedural Characteristics and Location and Success of Intervention Depending on CKD Stages.a
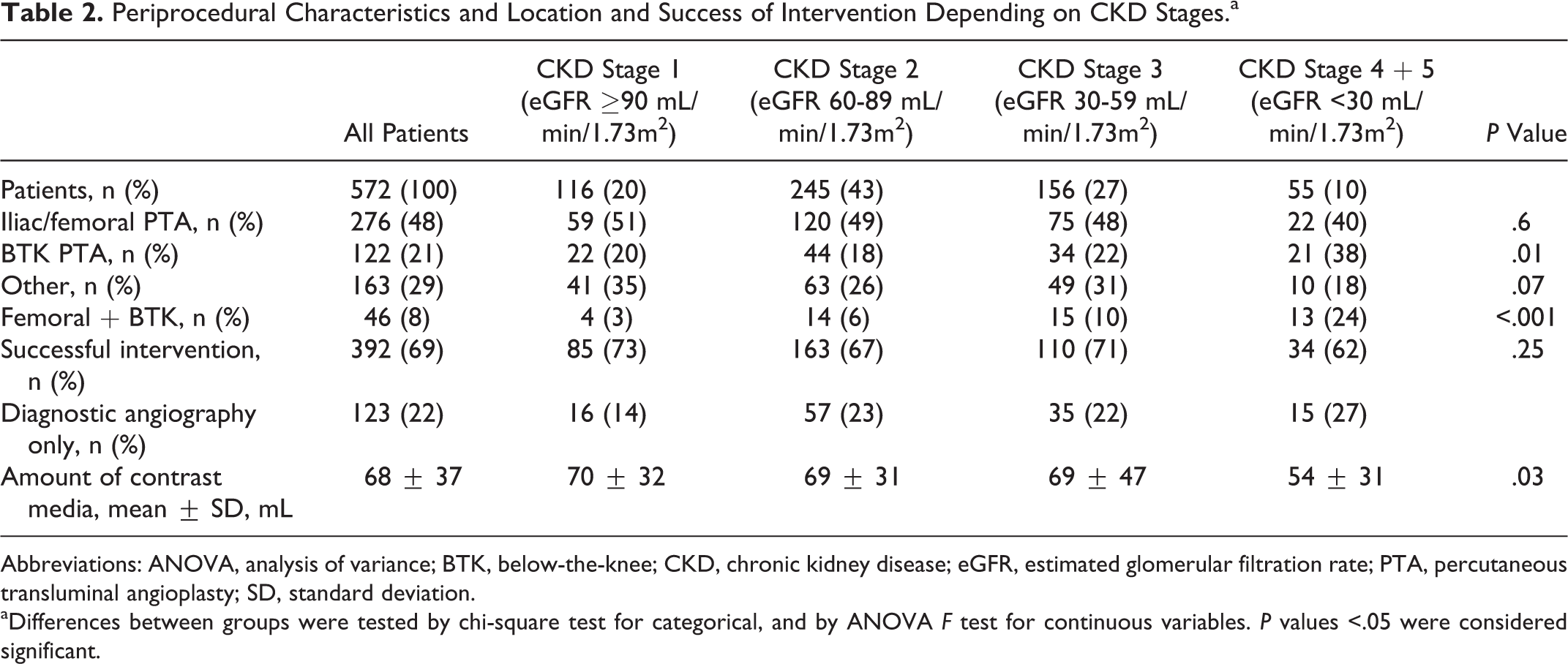
Abbreviations: ANOVA, analysis of variance; BTK, below-the-knee; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; PTA, percutaneous transluminal angioplasty; SD, standard deviation.
aDifferences between groups were tested by chi-square test for categorical, and by ANOVA F test for continuous variables. P values <.05 were considered significant.
Baseline characteristics for patients according to their CKD stage and depending on diagnostic angiography or endovascular revascularization are presented as supplementary material (Supplemental Tables 1-5).
Distribution of PAD According to Fontaine Classification
In the entire cohort, 10% of patients presented with Fontaine stages I and IIa, 50% stage IIb, and 40% stages III and IV, representing the group with critical limb ischemia (CLI; Figure 2). In Fontaine stage I, there was one clinically asymptomatic patient with impaired ABI values who received angiography of both coronary arteries and peripheral vessels. Another Fontaine stage I patient without clinical symptoms and normal ABI values presented with moderate iliac vessel stenosis during angiography, and finally, one patient with microangiopathy related to essential thrombocythemia was lacking any significant stenosis.
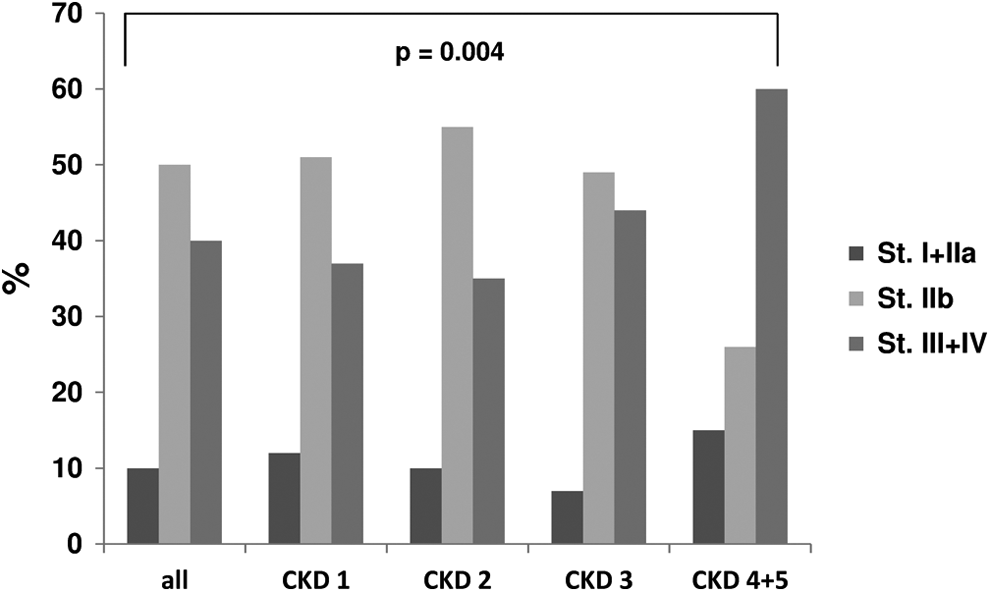
Distribution of Fontaine stages according to chronic kidney disease (CKD) stages 1-4 + 5, dark gray bars representing Fontaine stages I and IIa, light gray bars representing Fontaine stage IIb, and mid gray bars representing Fontaine stages III and IV.
In CKD stages 1 through 3, the distribution pattern of Fontaine stages was similar, showing stages I and IIa in 12%, 10%, and 7%, respectively, whereas stage IIb was present in 51%, 55%, and 49% accordingly. Stages III and IV could be detected in 37%, 35%, and 44%. In the most advanced CKD stages 4 and 5, the group of patients with CLI rose to 60% (P < .05), diminishing the proportion of Fontaine stage IIb to 26%, almost only half of the number present in earlier CKD stages.
Location and Success of Intervention
Of all patients, 22% underwent diagnostic angiography only. The percentage of patients with PAD having catheter-based interventions was 78% with no differences between CKD groups (Table 2). Concerning the locations of intervention, there were significantly more below the knee (BTK) procedures performed in CKD 4 + 5 group (38% vs 22% in CKD 3 vs 18% in CKD 2 vs 20% in CKD 1, respectively; P = .01, Table 2).
Medication at Time of Discharge and at Follow-Up
Prescriptions of medication for secondary prevention of CV events and disease progression at discharge and at follow-up are displayed in Figure 3. For follow-up, 24 (4.4%) patients could either not be contacted or refused to give information about their recent health condition and therefore they were excluded from further analysis.
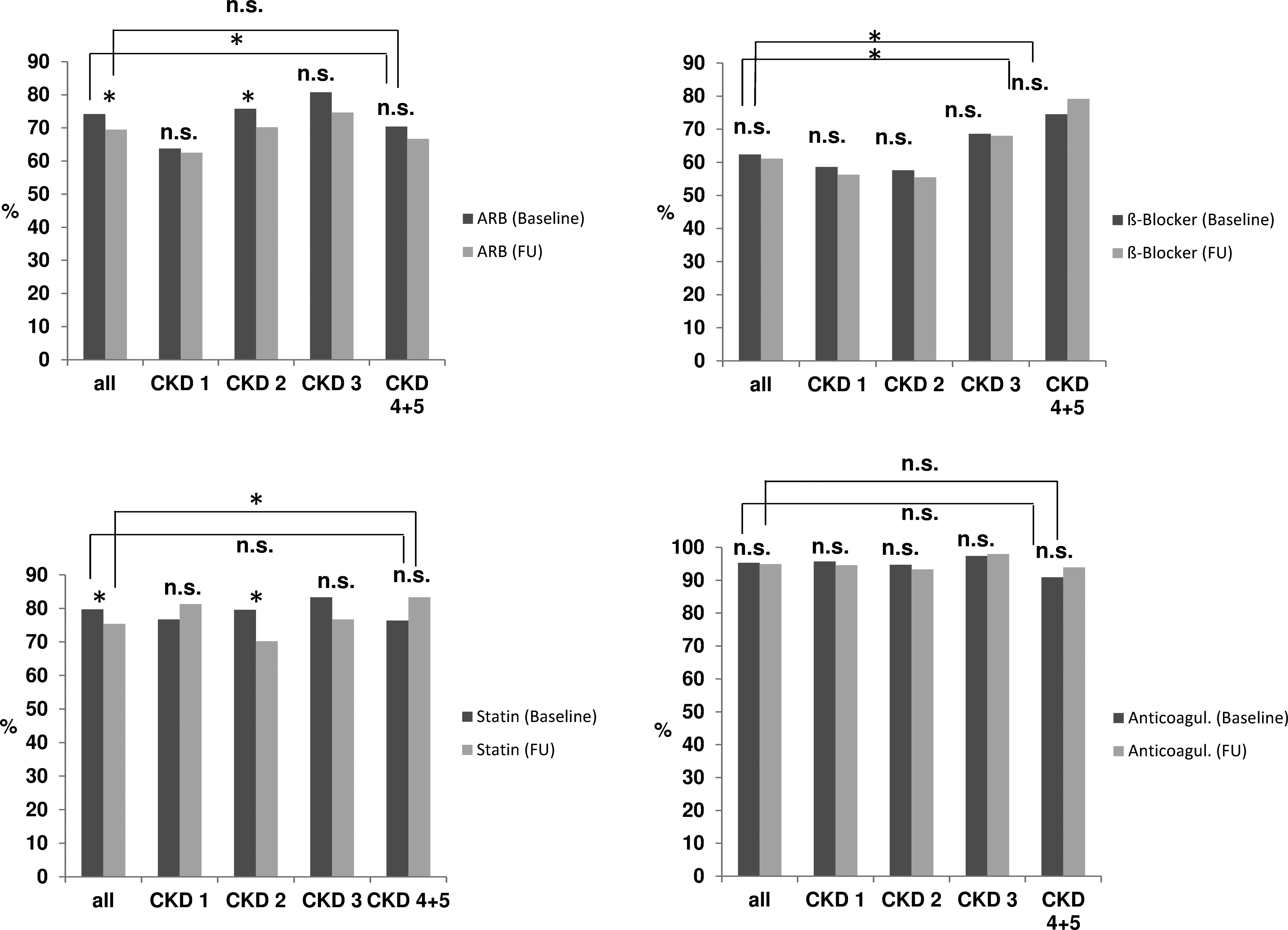
Medication at discharge and after follow-up according to chronic kidney disease (CKD) stages, dark gray bars representing baseline and light gray bars representing follow-up (FU) values. Angiotensin receptor blockers (ARB) including angiotensin-converting enzyme (ACE) inhibitors and AT1-receptor (AT1) blockers, anticoagulation including acetylsalicylic acid (ASA), clopidogrel, and vitamin-K-antagonists, P values for differences between baseline and follow-up data and among each chronic kidney disease (CKD) stage are displayed within the figure. *P < .05. ns indicates not significant.
The use of angiotensin receptor blockers and angiotensin converting enzyme (ACE) inhibitors differed significantly among all CKD stages at time of discharge. However, significant differences between time of discharge and follow-up were exclusively found in CKD stage 2. Concerning beta-blockers, there were significant differences among all CKD stages both at discharge and at follow-up. For statins, significant differences at follow-up among all CKD stages could be detected, whereas in CKD stage 2 again significant differences between discharge medication compared with follow-up appeared.
With regard to antithrombotic (acetylsalicylic acid [ASA], warfarin, and clopidogrel), no differences among CKD stages neither between discharge nor between follow-up medication could be revealed from our data.
Long-Term Survival of Patients With PAD
Cumulative mortality after a median follow-up of 1135 days (95% confidence interval [CI] 1159-1259, P < .001) was significantly higher in patients with advanced CKD stages (9%, 16%, 29%, and 47% in CKD stages 1, 2, 3, and 4 + 5, respectively; P < .001).
After adjusting for sex, age, diabetes, anemia, and PAD categories, CKD stages 4 + 5 were associated with significantly worse survival (HRR 2.6, 95% CI 1.1-5.8; P = .05) but also age (HRR 1.04, 95% CI 1.0 -1.1; P = .004), anemia (HRR 2.4, 95% CI 1.6-3.6; P < .001), and PAD stages 3 and 4 according to the Fontaine classification (HRR 2.2, 95% CI 1.0-4.8; P = .05) independently predicted elevated risk of mortality in this model. A second analysis including sex, age, BMI, diabetes mellitus, hypertension, and smoking as covariates revealed age, sex, and diabetes mellitus to be independently associated with worse long-term survival, whereas BMI, smoking, and hypertension had no effect on mortality (Supplemental Table 6). Crude and adjusted cumulative survival rates are shown in Figure 4.
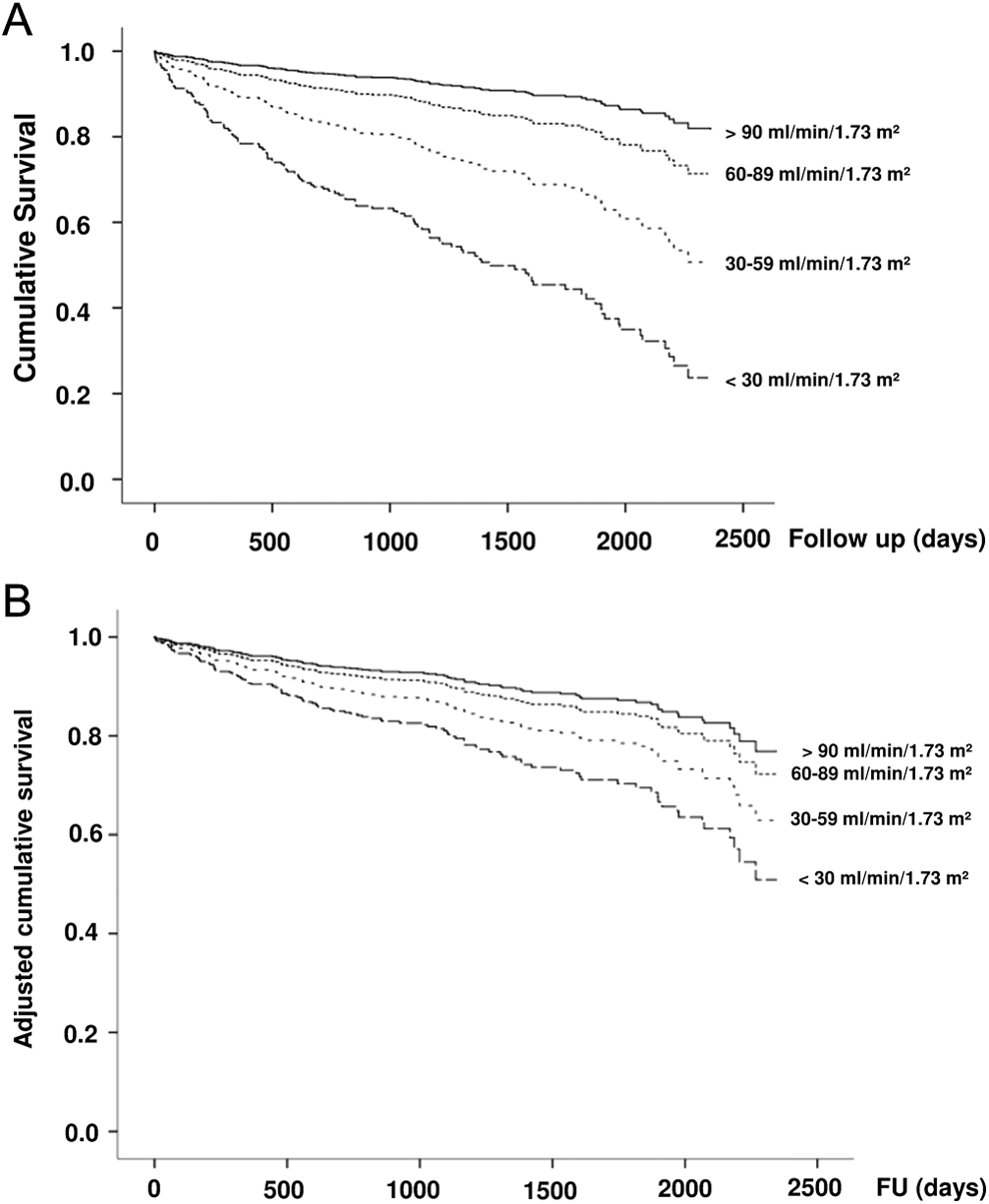
Cumulative and adjusted survival in patients according to chronic kidney disease (CKD) stages. Panel A, crude cumulative survival (days; CKD stage 2 HRR 1.7, 95% CI 0.8-3.4; CKD stage 3 HRR 3.4, 95% CI 1.7-6.8, P < .01; CKD stages 4 + 5 HRR 7.2, 95% CI 3.5-15, P < .01). Solid lines indicate estimated glomerular filtration rate (eGFR) > 90 mL/min/1.73m2, narrow dotted lines indicate eGFR 60-89 mL/min/1.73m2, wide dotted lines indicate eGFR 30-59 mL/min/1.73m2, and hyphenated lines eGFR <30 mL/min/1.73m2. Panel B, Adjusted cumulative survival (days; CKD stage 2 HRR 1.2, 95% CI 0.6-2.6; CKD stage 3 HRR 1.8, 95% CI 0.8-3.8; CKD stages 4 + 5 HRR 2.6, 95% CI 1.0-5.8, P = .05), adjusted for sex, age, anemia, diabetes, and PAD stages. Solid lines indicate eGFR >90 mL/min/1.73m2, narrow dotted lines indicate eGFR 60-89 mL/min/1.73m2, wide dotted lines indicate eGFR 30-59 mL/min/1.73m2, and hyphenated lines indicate eGFR <30 mL/min/1.73m2. HRR indicates hazard rate ratio; CI, confidence interval.
Cardiovascular and Other Events at Follow-Up
Of 433 patients who returned a completed follow-up questionnaire, 5% experienced myocardial infarction during follow-up, in 10% there was need for bypass limb surgery, and amputation was necessary in 7%. New onset of malignancy occurred in 10%. No significant differences with regard to CKD stages could be detected (Table 3).
Events After PTA at Follow-Up Depending on CKD Stages.a
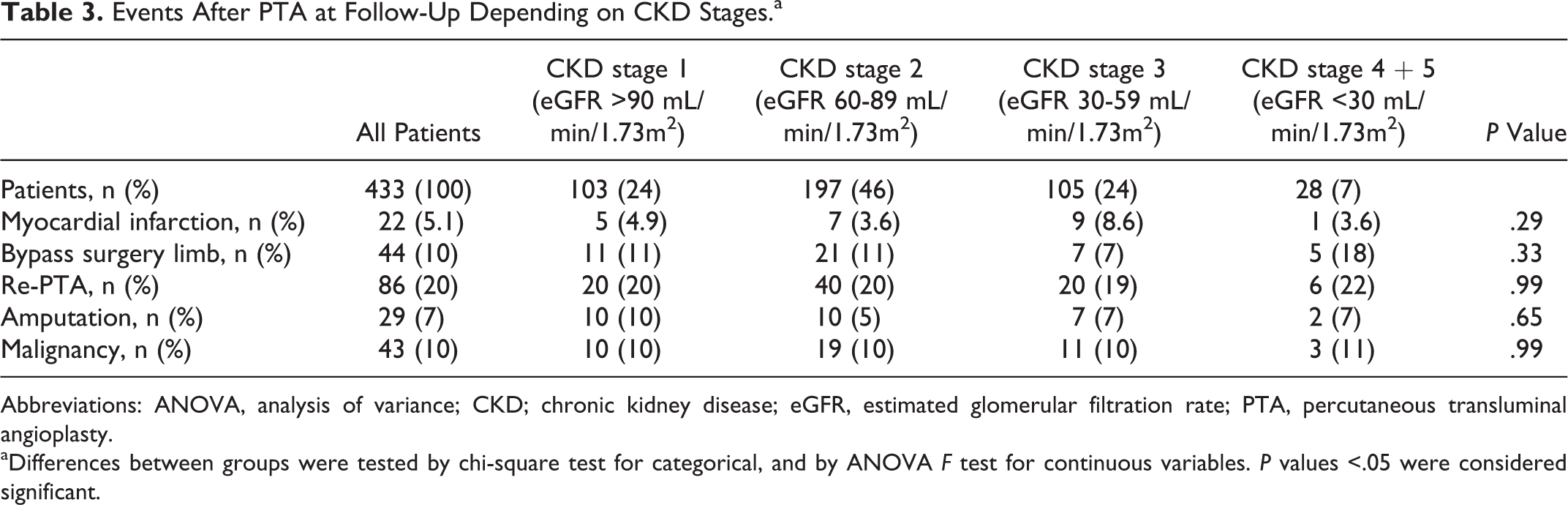
Abbreviations: ANOVA, analysis of variance; CKD; chronic kidney disease; eGFR, estimated glomerular filtration rate; PTA, percutaneous transluminal angioplasty.
aDifferences between groups were tested by chi-square test for categorical, and by ANOVA F test for continuous variables. P values <.05 were considered significant.
Discussion
So far, to our best knowledge, no data concerning long-term mortality with respect to exact CKD stages in an all stages cohort of patients with PAD exist to date. The main message from this study is the significant deterioration of survival with rising CKD stages after long-term follow-up. Almost half of the patients in CKD stages 4 + 5 were deceased during follow-up, and even after adjusting for common confounders, advanced CKD stages were associated with increased mortality rates.
Other studies have elucidated the adverse effect of underlying CKD in a population of patients with PAD. Liew et al 13 found a significantly increased mortality rate (45%) in 210 patients having both PAD and CKD after a 6-year follow-up period, but in this study, patients with end-stage renal disease (ESRD; eGFR <15 mL/min/1.73m2) were excluded and patients were only categorized into eGFR ≥60 and <60 mL/min/1.73m2, whereas we used the more distinct classification of the National Kidney Foundation in our cohort.
Luo et al 14 examined 3610 Chinese patients among which 287 presented with both PAD and CKD. In this study, CKD was classified into mild, moderate, and severe disease based on eGFR (mild CKD 45-60 mL/min/1.73m2, moderate 30-45 mL/min/1.73m2, and severe 15-30 mL/min/1.73m2), again excluding patients with ESRD, a high-risk patient population. 24,25 All-cause mortality in the CKD and PAD groups after a mean follow-up of 37.64 ± 1.54 months was 38.5% and differed significantly from the other groups with PAD or CKD alone or neither of these conditions. Moreover, in agreement with our results, this study identified CKD as an independent risk factor for PAD after adjusting for potential confounders. The comparably low mortality rate of 38.5% versus 47% in our data can be explained by omitting patients with ESRD and differences in traditional risk factors such as diabetes mellitus, hypertension, and smoking present among the baseline characteristics.
Another study 15 analyzed 1010 consecutive patients with PAD having Rutherford grade ≥3 (= Fontaine Stage IIb) with respect to renal function. Classification of eGFR stages was done in accordance to the classification of the National Kidney Foundation, including patients on a chronic hemodialysis program. However, in this study as in all previous ones, eGFR was calculated by the Modification of Diet in Renal Disease formula. 26 In contrast, we applied the more recent CKD-EPI formula being more accurate, especially at higher eGFR levels. 27 Lacroix et al 15 provided 1-year mortality rates that were even higher for CKD groups 1 to 4 (16%, 18%, 31.7%, and 44.3%, P < .05, respectively) compared with our data of cumulative survival after long-term follow-up. It has to be emphasized that in contrast, in our cohort, 10% of all patients with mild to moderate claudication were also included, thus representing a patient subgroup with less severe disease presentation and consequently lower hazard of death. Additionally, our patients were younger (67.7 vs 70.7 years) and had a higher hemoglobin value (13.1 vs 12.5 g/dL) at baseline which may have contributed to a more favorable long-term survival rate in contrast to the French patient cohort.
More importantly, discharge medication for secondary prevention of both PAD and CV events was more frequently found in our patient group. At discharge, statins were administered in 79.7% versus 64.7% in the French patient population, renin–angiotensin system inhibitors in 74.2% versus 54.0%, and beta-blockers in 62.4% versus 26.4%, respectively. 15 It has been shown previously that statin use improves renal function, contributes to prevention of renal decline, 28 –31 and results in significantly lower rates of CV events 32 –34 and death, 34 so the finding of better survival rates in our patients may be due to the higher prescription rates of statins in all CKD groups.
Revisiting the European Society of Cardiology (ESC) Guidelines on the diagnosis and treatment of PAD, 35 statin use in PAD, with and without underlying CAD, is strongly recommended. Moreover, use of ACE inhibitors has beneficial effects on survival in patients with PAD irrespective of left ventricular function. 36
The most striking differences concerning discharge medication could be found in the use of beta-blockers, which are not contraindicated in patients with PAD but in contrast are highly advised to be part of perioperative medication regimen in patients designated for vascular surgery. The adjuvant effects of the previously mentioned concomitant medication could be another reason for only slightly worse survival data after an extended follow-up period of 3.1 years in our patient group compared to those of Lacroix et al 15 after 1-year follow-up only. Moreover, guideline adherence concerning secondary prevention medication has been shown to be worse with decreasing eGFR. 16,17,19 Although there have been trends for improvements over time concerning efficacious medication, 18,37 prescription patterns are far from being close to the ESC guideline recommendations even in our cohort. Nevertheless, evidence-based medication therapy at discharge and at follow-up was prescribed more frequently in our cohort than in previous studies, and more importantly, in contrast to all previous studies, secondary prevention strategies even after long-term follow-up were not less frequently used in advanced CKD stages. 15
Finally, we and others 15 could not detect an independent association between severity of CKD and risk of amputation, although the percentage of amputation differed dramatically compared to those of Lacroix et al, 15 with markedly lower amputation rates in our patients.
Our study has several limitations. First, the analysis with regard to long-term mortality and adjustment for confounders was performed retrospectively. Second, other potentially relevant factors for survival impairment such as chronic inflammation caused by uremia, hyperlipidemia, and a possible correlation with irregular calcium-phosphate metabolism could not be evaluated. Finally, although the study comprised a sizable number of patients with PAD, it reflects only a single-center experience, and a much larger population is required to perform extensive multivariate analyses in order to reveal more risk factors for mortality and impact of CKD on survival rates with relevance on the decision making in clinical practice.
In conclusion survival in patients with PAD deteriorates with declining renal function. Age, anemia, and advanced PAD stages have been shown to be independent predictors for increased risk of all-cause mortality. Other more renal impairment-specific conditions like chronic inflammation caused by uremia or abnormal bone metabolism may have further contributed to an increased mortality risk in advanced CKD stages.
Medication adherence for secondary disease prevention according to guideline recommendations still did not reach recent targets, but prescription patterns appeared to be unrelated to CKD stage.
Footnotes
Authors’ Note
All authors have met the following criteria: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published Holger Reinecke contributed to statistical analysis, writing, revising it critically for important intellectual content, and final approval of the version to be published. Abstracts and their contents were presented at the 16th tricountry congress of the Austrian, German and Swiss societies for angiology, Graz, September 15-18, 2013, and at the 80th annual conference of the German Society of Cardiology (Deutsche Gesellschaft fuer Kardiologie), Mannheim, April 27-30, 2011. Katrin Gebauer contributed to study design, literature search, writing, and final approval of the version to be published. Christiane Engelbertz contributed to literature search, revising the text, and final approval of the version. Nasser M. Malyar contributed to revising the text, and final approval of the version to be published. Matthias Meyborg contributed to revising the text, and final approval of the version to be published. Florian Lüders contributed to revising the text, and final approval of the version to be published. Eva Freisinger contributed to revising the text, and final approval of the version to be published.
Acknowledgments
We thank Lilly H. Wagner, MD, for careful and professional revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.