
Abstract

Abdominal aortic aneurysm (AAA) is an important cause of mortality in older adults in both developed and in developing countries globally. 1 The ongoing search for medical therapies that are effective in the primary and secondary prevention of complications in patients who have AAAs has led to great interest in the pathogenesis of this condition. 2 –4 Traditionally, AAAs have been considered to arise as a result of atherosclerosis, most likely due to excessive positive arterial remodeling. 5 In support of this theory, patients with coronary and peripheral atherosclerosis are at increased risk of developing an AAA, most AAA biopsies have been found to have intimal atherosclerosis, and many of the risk factors for AAA are similar to those present in patients who develop complications of atherosclerosis. 2,5 It has however also been noted that some of the risk factors for AAA are more unique. For example, smoking and male sex are recognized as more powerful risk factors for AAA than atherosclerosis-associated occlusive disease. 2 The most notable distinction between the risk factors for AAA and atherosclerosis-associated occlusive disease is diabetes. 6 Diabetes has been repeatedly reported to be associated with reduced prevalence and incidence of AAA but is an important positive risk factor for atherosclerosis. 6 –8 A recent systematic review estimated that the prevalence of AAA in individuals with diabetes was lower (odds ratio: 0.80, 95% confidence intervals: 0.70-0.90) than that in persons who did not have diabetes based on data from 17 population studies. 7 Data from 6 prospective studies also suggested a lower incidence of new cases of AAA in individuals with diabetes (odds ratio: 0.54, 95% confidence interval: 0.31-0.91). 7
In this issue of Angiology, Takagi and Umemoto report a meta-analysis comparing the growth of small AAAs in patients with and without diabetes. 8 The report analyses data from 19 studies and 9777 patients and confirms the findings from previous studies that diabetes is associated with reduced AAA growth. 8 –10 It has also been reported by a number of groups that diabetes is associated with a reduced risk of AAA rupture. 11,12
What can this consistent association of diabetes with reduced AAA development, growth, and rupture tell us about the primary and secondary prevention approaches for AAA? In an attempt to define the pathophysiological mechanisms for this relationship at a molecular and cellular level, there has been significant interest in examining the effect of diabetes on the aorta. Some possible reasons for the negative association of diabetes with AAA are listed in Table 1. 13 –18 The most likely reason that diabetes is associated with reduced AAA-related complications appears to be secondary to changes in extracellular matrix remodeling. 18 It is well described that diabetes-associated kidney disease occurs as a result of accumulation of extracellular matrix because of both increased matrix formation and reduced matrix degradation. 18 It is possible that diabetes has a similar effect within the aorta as described in experimental models of diabetes-accelerated atherosclerosis in which accumulation of extracellular matrix proteins has been demonstrated. 19,20 Such promotion of vascular extracellular matrix accumulation would be predicted to counteract the excessive matrix remodeling, which is believed to be critical in AAA formation and growth. 2,3,5
Examples of Suggested Reasons for the Negative Association of Diabetes With AAA.
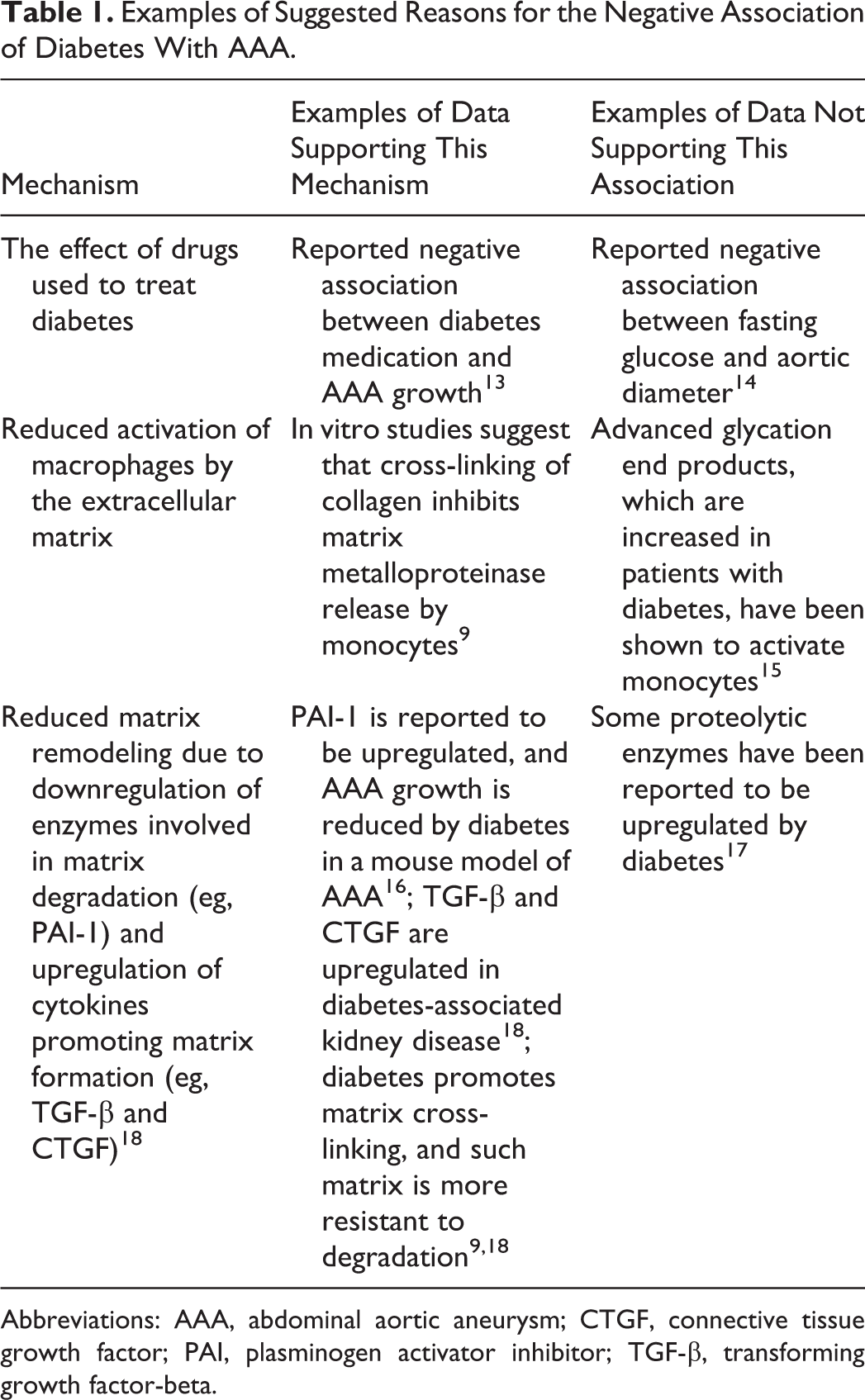
Abbreviations: AAA, abdominal aortic aneurysm; CTGF, connective tissue growth factor; PAI, plasminogen activator inhibitor; TGF-β, transforming growth factor-beta.
What are the implications of this for the treatment of AAA and diabetes? There is significant interest in the development of methods to limit excess matrix cross-linking and accumulation in diabetes. 21,22 For example, antifibrotic agents are under development (such as pirfenidone and tranilast derivatives) as well as agents that reduce advanced glycation end-product formation (a biochemical pathway that is enhanced in diabetes and promotes matrix cross-linking and fibrosis). 21,22 Such agents if used in patients with diabetes may theoretically increase the incidence and rate of progression of AAA, although this has not been specifically examined. In contrast, the development of agents that promote matrix formation or inhibit matrix degradation may be valuable in limiting AAA growth. However, such agents could also theoretically promote diabetic complications such as kidney disease. Despite much work aimed at understanding the pathogenesis of AAA, this has yet to be translated into the development of effective medications to limit AAA growth. 4,23,24 Further defining why diabetes inhibits AAA development may provide improved insight into AAA pathogenesis, which assists the better development of drugs that are effective at limiting AAA growth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JG holds a Practitioner Fellowships from the National Health and Medical Research Council, Australia (1019921) and holds a Senior Clinical Research Fellowship from the Queensland Government. MEC holds a Senior Principal Research fellowship from the Australian NHMRC.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from the Queensland Government and National Health and Medical Research Council supported this work.