
Abstract
The optimal treatment for in-stent restenosis (ISR) of both bare-metal stent (BMS) and drug-eluting stent (DES) is currently unclear. The aim of this meta-analysis was to assess the role of drug-eluting balloon (DEB) as an optional treatment for ISR. We searched PubMed, MEDLINE, EMBASE, BIOS, and Web of Science from 2005 to July 2014. Eight studies, enrolling 1413 patients were included. Main end points were late lumen loss (LLL), binary in-segment restenosis (BR), major adverse cardiac events (MACEs), target lesion revascularization (TLR), death, myocardial infarction (MI), and stent thrombosis (ST). When compared to plain old balloon angioplasty (POBA), DEB treatment significantly reduced the risk of MACE (risk rato [RR] 0.37, P < .01), death (RR 0.44, P = .04), TLR (RR 0.27, P < .01), BR (RR [95% CI]: 0.23[0.12 to 0.43], P < .01) and associated with better outcomes of LLL ( 0.50 [ 0.65 to 0.35] mm, P < .01). However, the differences were not significant between DEB treatment and DES treatment in all primary and secondary end points. The DEB was a better option to treat ISR when compared to POBA. However, it had similar effects as DES.
Keywords
Introduction
Percutaneous coronary intervention (PCI) has become the more commonly used revascularization method compared with coronary artery bypass grafting (CABG). 1 However, PCI presents an obvious limitation of high-risk target lesion revascularization (TLR) due to in-stent restenosis (ISR). Although the risk of ISR has decreased with the use of newer generation drug-eluting stents (DES), currently, there is no optimal treatment for ISR for both bare-metal stent (BMS) restenosis and DES restenosis.
Drug-eluting balloons (DEBs) may be a promising approach to treat ISR because of the absence of a need for an additional metal scaffold. The DEB involves the use of a balloon coated with antiproliferative drug, which is released as the balloon is inflated. 1 Studies have found DEBs were not only safe to use but also able to release 80% of the drug during inflation and effectively reduce neointimal proliferation. 2 –4 Some studies have shown that DEB is associated with poorer outcomes for DES-ISR compared with BMS-ISR. 5 Thus, the exact value of DEBs in treating ISR has not been determined. We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) to assess the role of DEB as an optional treatment for both DES-ISR and BMS-ISR.
Methods
Search Strategy
We searched PubMed, MEDLINE, EMBASE, BIOS, and Web of Science from 2005 to July 2014 using the following key words with search filters for human studies and randomized trials. Key words: “drug eluting balloon,” “drug coated balloon,” “drug eluting balloon angioplasty,” “drug eluting balloon catheter,” “drug coated balloon angioplasty,” “drug coated balloon catheters,” “paclitaxel eluting balloon,” “paclitaxel eluting balloons,” “paclitaxel eluting balloon treatment,” “restenosis,” “in-stent restenosis,” “ISR,” “in-stent restenosis lesion,” “in-stent restenosis lesions,” “in-stent restenosis treatment,” “in-stent restenotic lesion,” “in-stent restenotic lesions.” We also considered reference lists, reviews, and letters for other potentially relevant citations. No language restrictions were applied. We used NoteExpress for management of the studies.
Study Selection
We had a 2-step selection procedure. In the first step, the titles and abstracts of all studies were reviewed independently by 2 researchers (Shen, Gao and Muzina, Akhtar) and included potentially relevant citations. The disagreements of the 2 researchers were resolved by discussion. In the second step, potentially relevant studies were reviewed in full text to confirm if they met the following inclusion criteria: (1) RCTs; (2) clinical trials; (3) adult patients (
Data Extraction and Quality Assessment
Relevant information, including baseline characteristic and outcome measures, were extracted independently by the two researchers using a prepared standardized database (Microsoft EXCEL).
The main characteristics of the included studies are outlined in Table 1. We used the Cochrane Collaboration tool 13 for assessing risk of bias to evaluate the quality of included trials on the following domain: (1) random sequence generation; (2) allocation concealment; (3) blinding; (4) incomplete outcome data; and (5) selective reporting. We judged each trial using the categories “low risk,” “high risk,” or “unclear risk”.
Characteristics of Included Studies.
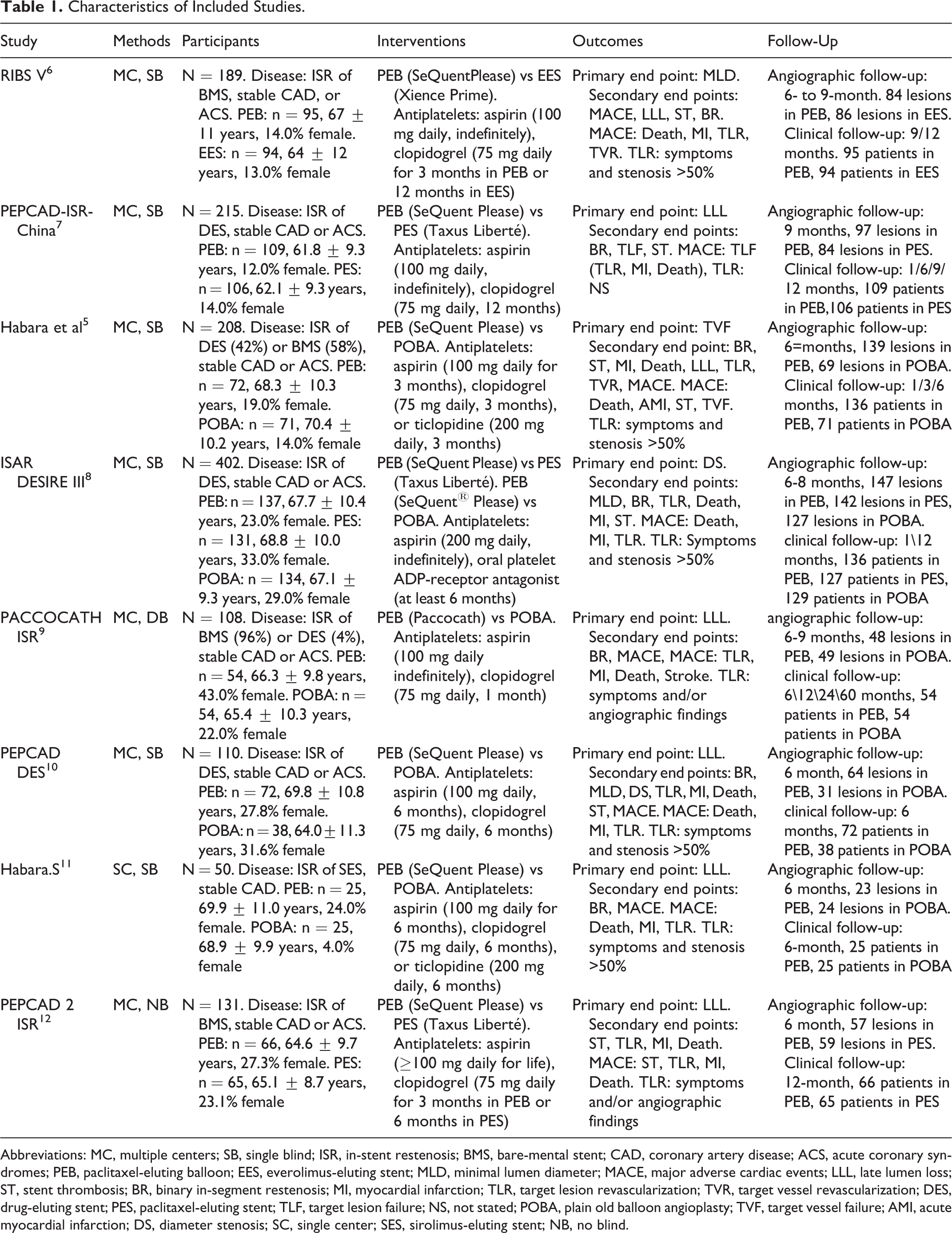
Abbreviations: MC, multiple centers; SB, single blind; ISR, in-stent restenosis; BMS, bare-mental stent; CAD, coronary artery disease; ACS, acute coronary syndromes; PEB, paclitaxel-eluting balloon; EES, everolimus-eluting stent; MLD, minimal lumen diameter; MACE, major adverse cardiac events; LLL, late lumen loss; ST, stent thrombosis; BR, binary in-segment restenosis; MI, myocardial infarction; TLR, target lesion revascularization; TVR, target vessel revascularization; DES, drug-eluting stent; PES, paclitaxel-eluting stent; TLF, target lesion failure; NS, not stated; POBA, plain old balloon angioplasty; TVF, target vessel failure; AMI, acute myocardial infarction; DS, diameter stenosis; SC, single center; SES, sirolimus-eluting stent; NB, no blind.
End Points and Definitions
Primary end points were (1) late lumen loss (LLL) and (2) major adverse cardiac events (MACEs). Secondary end points were (1) binary in-segment restenosis (BR), (2) target lesion revascularization (TLR), (3) myocardial infarction (MI), (4) stent thrombosis (ST), and (5) death. Since minimal lumen diameter (MLD) was only the primary end point of 1 trial, 6 we did not consider it as the end point in our study. Definitions in the individual trials are shown in Table 1.
Statistical Analysis
We described dichotomous and continuous variables by risk ratios (RRs) and mean differences (MDs), respectively, with their 95% confidence intervals (CIs). Calculations were based on a Mantel-Haenszel random effects model to perform the aggregation of all RRs or MDs. The heterogeneity of the studies was assessed using the chi-square test and I 2 statistic. I 2 >50% was considered as at least moderate heterogeneity, and P < .10 was considered significant. We performed a subgroup analysis between different comparator interventions (DEB vs POBA and DEB vs DES). Results were considered to be significant at 2-tailed P < .05. We also performed subgroup analysis for different ISR (BMS-ISR vs DEB-ISR). The whole analysis was performed using Review Manager (RevMan 5.2) software.
Results
Description of Included Studies
The selection process is illustrated in Figure 1—a flow diagram followed the PRISMA principle as outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) statement. 14 A total of 447 potential relevant studies were searched initially, and 8 studies including 1413 patients met the inclusion criteria. 5 –12 Only 1 study was single center, and the others were multicentered. Of these 8 studies, 6 were single blinded, 1 was double blinded, and 1 was nonblinded. One study enrolled 50 patients with only stable coronary artery disease and 7 studies enrolled 1363 patients who also included acute coronary syndromes.
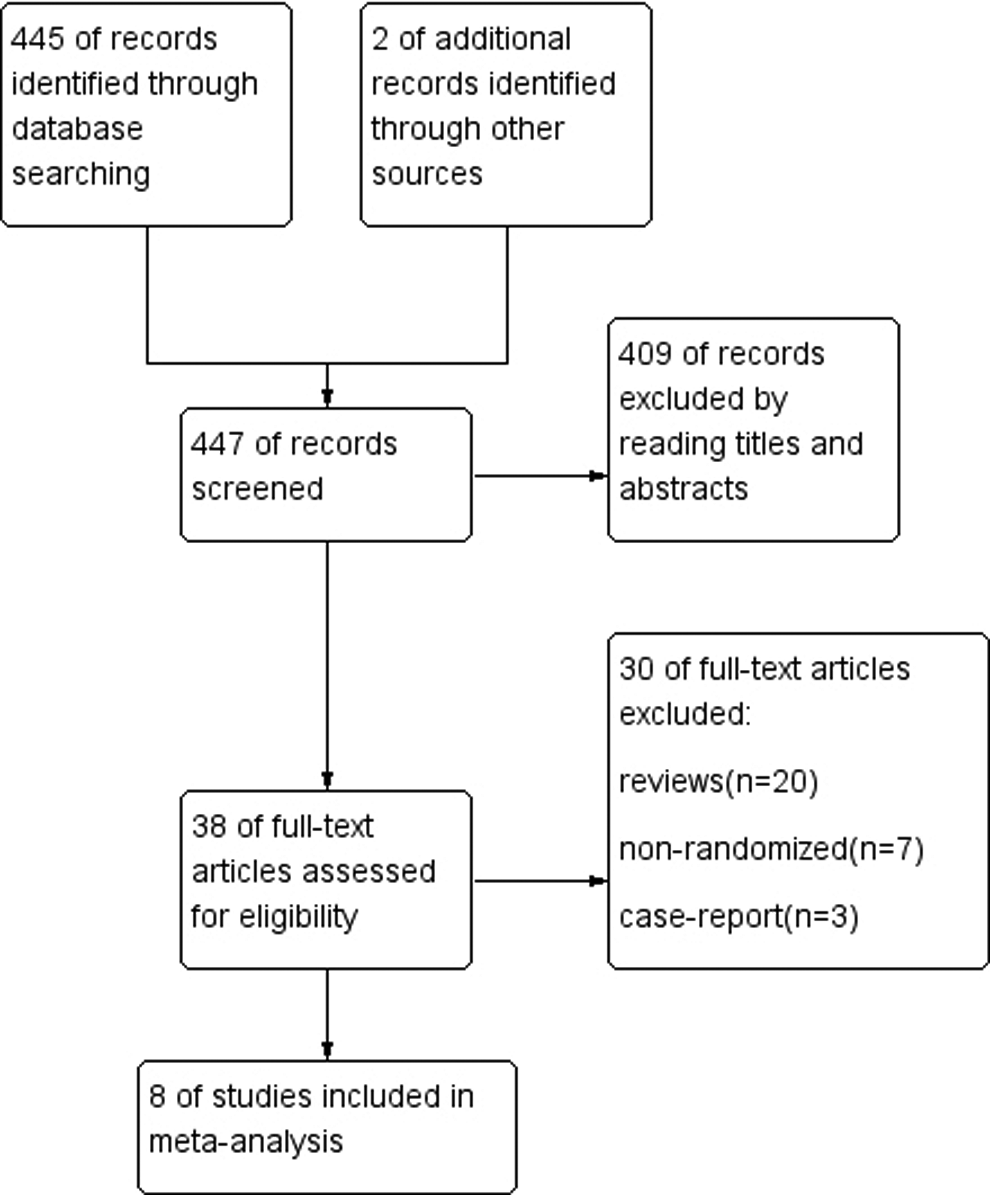
Studies selection process.
Studies using DEB for de novo stenosis were not considered. All 8 trials used PEB (paclitaxel, 3 μg/mm2) devices. The devices of PEB were SeQuentPlease (B.Braun Surgical, Melsungen AG, Vascular Systems, Berlin, Germany) in 7 trials, and only 1 trial used PACCOCATH (Bayer AG, Leverkusen, Germany). Control interventions included were POBA in 4 trials and DES in 3 trials (2 trials used TaxusLiberté [Boston Scientific, Natick, Massachusetts] and 1 trial used Xience Prime [Abbott Vascular, Abbott Park, Illinois]). In addition, the ISR-DESIRE trials compared DEB with either POBA or DES (TaxusLiberté, Boston Scientific, Natick, Massachusetts). While 4 studies included 777 patients with DES-ISR, 2 studies included 320 patients with BMS-ISR. Two studies included patients with both DES-ISR (92 patients) and BMS-ISR (224 patients). Overall, the trials used aspirin and clopidogrel or ticlopidine as postinterventional antiplatelet therapy.
In total, clinical follow-up was completed in 1402 patients, and angiographic follow-up was completed for 1330 lesions. The mean duration of clinical and angiographic follow-up was 15.75 months and 7.38 months, respectively. Overall risk of bias in the included studies was good (Figure 2). More details of the characteristics of 8 studies are shown in Table 1.
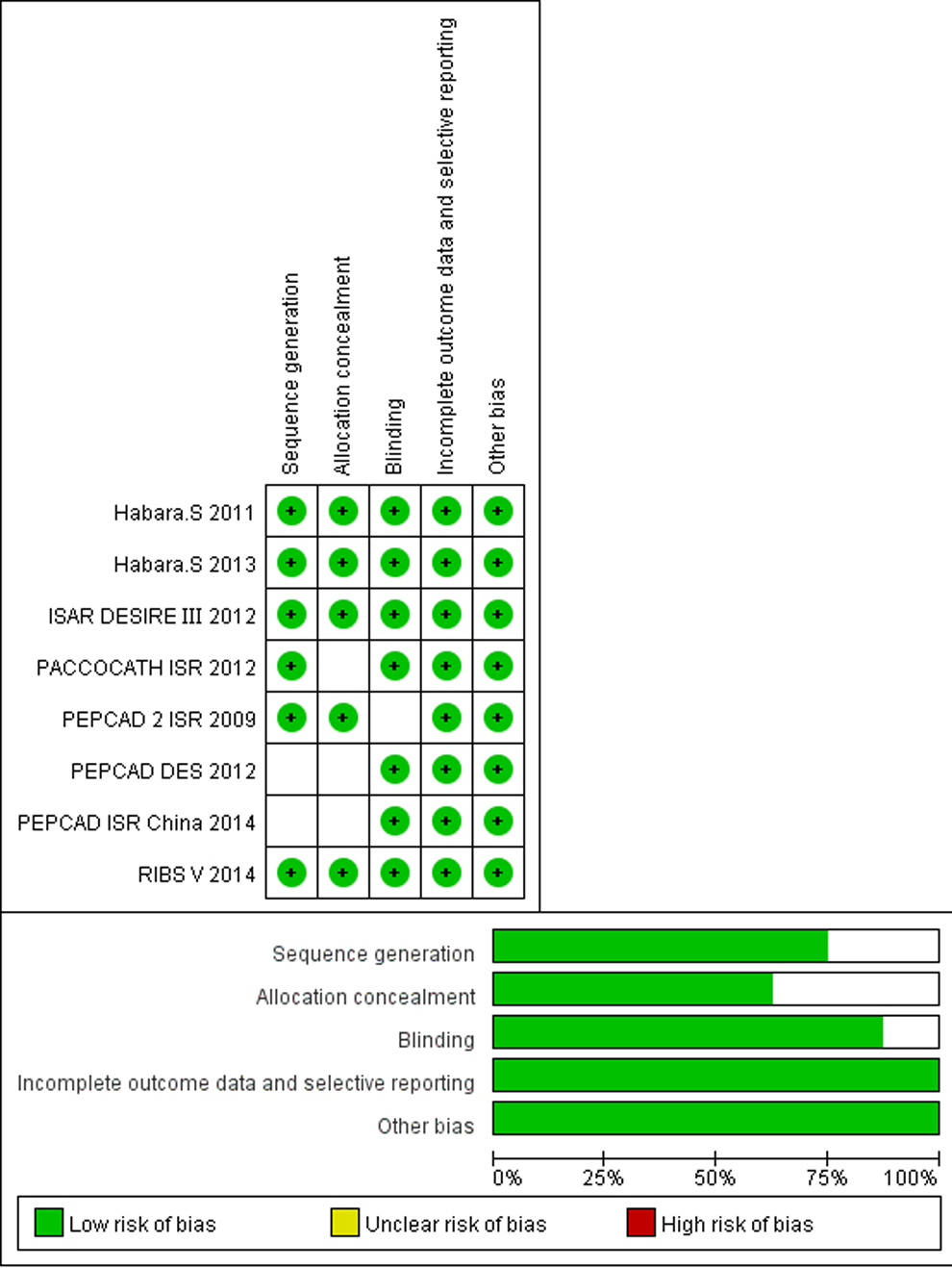
Risk of bias assessment.
Angiographic End Points in the DEB Versus POBA and DEB Versus DES Groups, Respectively
Late lumen loss
Late lumen loss was reported in 8 trials. As shown in Figure 3, the DEB group had significantly less in-segment LLL than the POBA group (MD [95% CI]: −0.50 [−0.65 to −0.35] mm, P < .01), while there was a nonsignificant difference in LLL between the DEB and the DES groups (MD [95% CI]: −0.04 [−0.18 to 0.10] mm, P = .55). Without subgroup analysis, the DEB group had significantly less LLL than the control group (MD [95% CI]: −0.3 [−0.48 to 0.12] mm, P < .01).
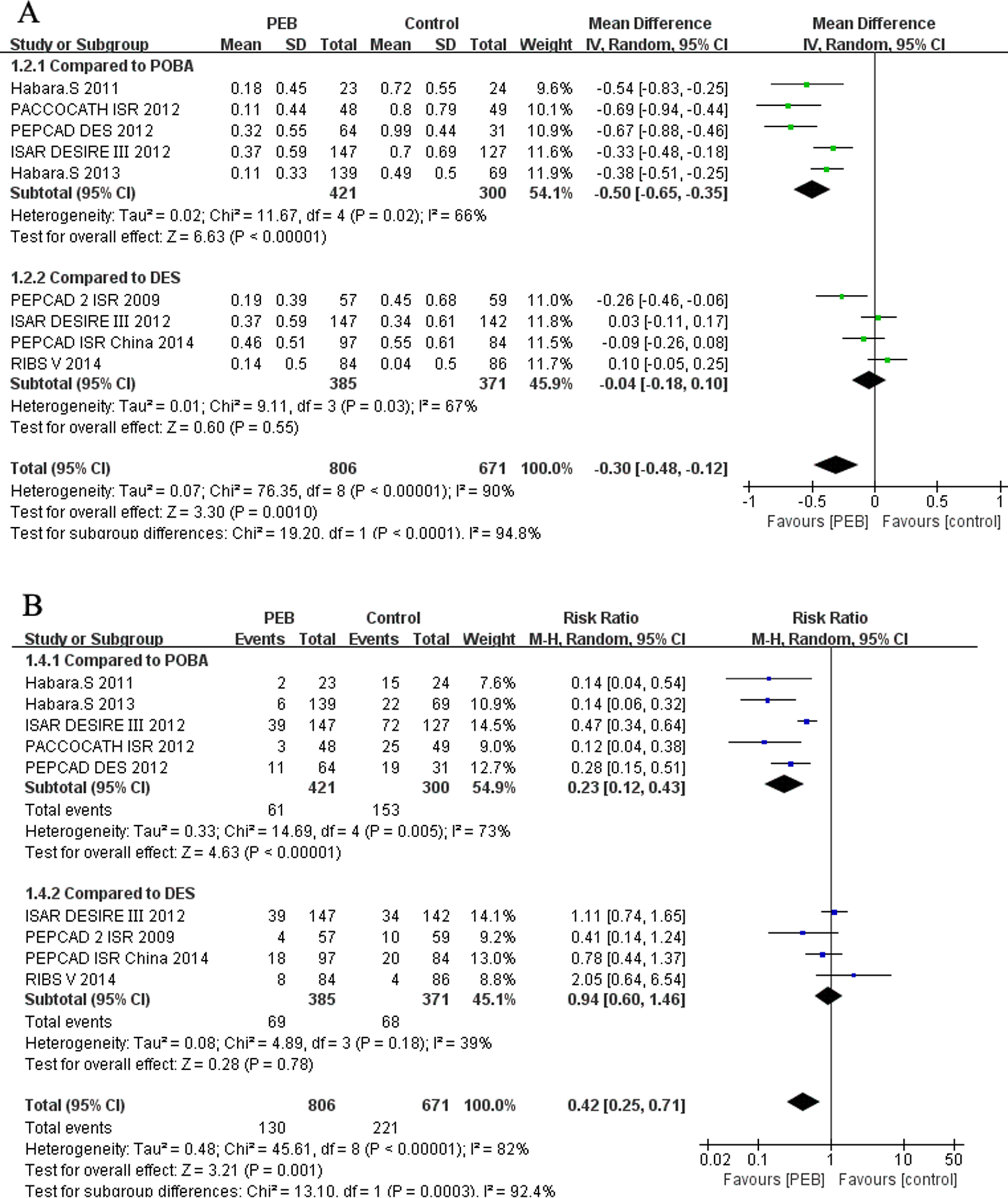
Forest plot of risk ratio (RR) or mean difference (MD) of angiography outcomes: late lumen loss (LLL; A), binary in-segment restenosis (BR; B).
Binary in-segment restenosis
Binary in-segment restenosis was reported in 8 trials. As shown in Figure 3, BR restenosis was significantly reduced in the DEB group when compared with the POBA group (RR [95% CI]: 0.23 [0.12, 0.43], P < .01), while the difference was not significant between the DEB and the DES groups (RR [95% CI]: 0.94 [0.60, 1.46], P = .28). Without subgroup analysis, BR was significantly reduced in the DEB group (RR [95% CI]: 0.42 [0.25, 0.71], P < .01).
Clinical End Points in the DEB Versus POBA and DEB Versus DES Groups, Respectively
Major adverse cardiac events
Major adverse cardiac events were reported in 8 trials. As shown in Figure 4, MACEs were significantly reduced in the DEB group compared with the POBA group (RR [95% CI]: 0.37 [0.26-0.54], P < .01), while the difference was not significant between the DEB and DES groups (RR [95% CI]: 0.97 [0.64-1.48], P = .89). Without subgroup analysis, MACE were significantly reduced in the DEB group (RR [95% CI]: 0.53 [0.35-0.81], P < .01).
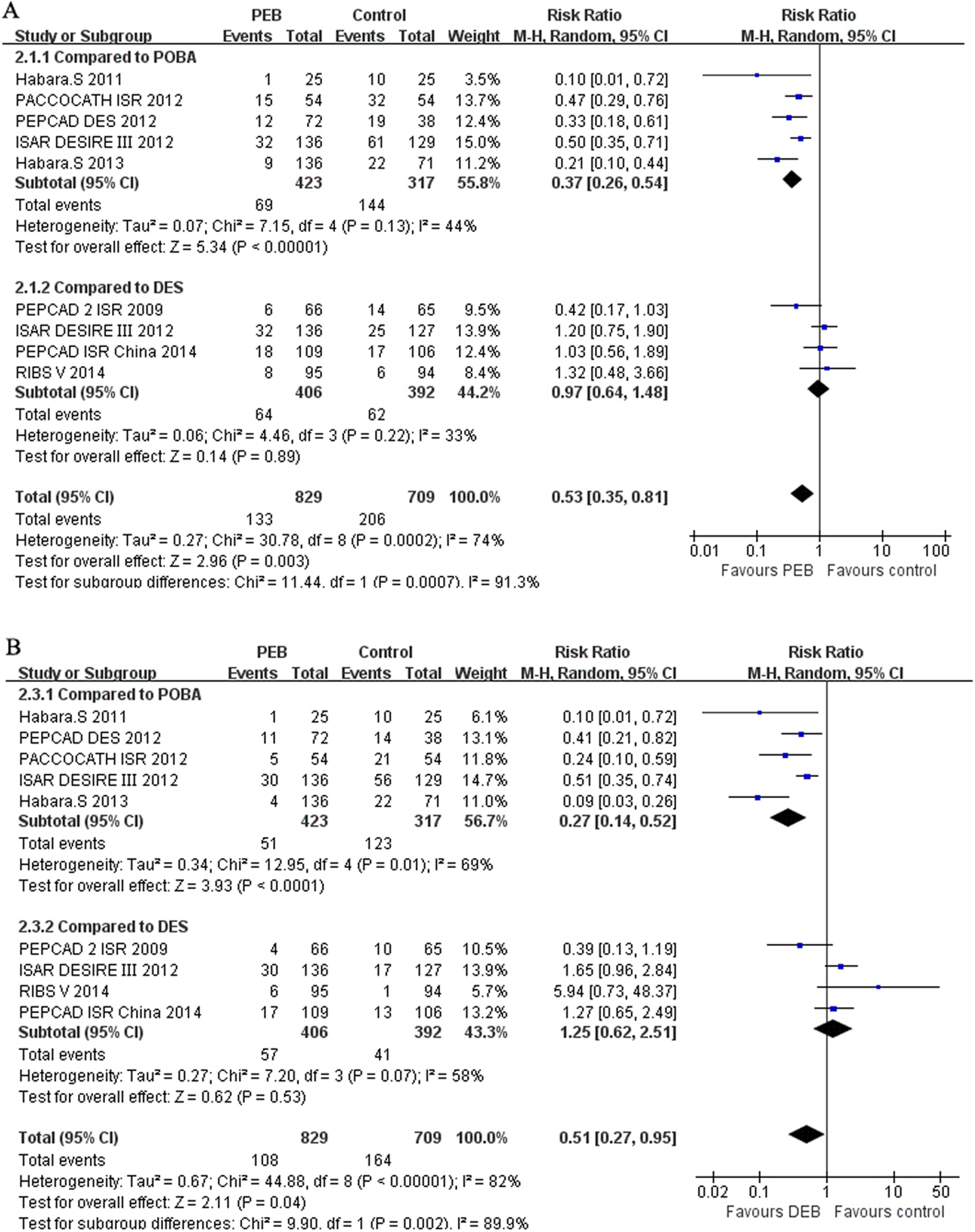
Forest plots of risk ratio (RR) of clinical outcomes: major adverse cardiac events (MACEs; A), target lesion revascularization (TLR; B), mortality (C), myocardial infarction (MI; D) and stent thrombosis (ST; E).
Target lesion revascularization
Target lesion revascularization was reported in 8 trials. As shown in Figure 4, TLR was significantly reduced in the DEB group compared with the POBA group (RR [95% CI]: 0.27 [0.14, 0.52], P < .01), while the difference was not significant between the DEB and the DES groups (RR [95% CI]: 1.25 [0.62-2.51], P = .53). Without subgroup analysis, TLR was significantly reduced in the DEB group (RR [95% CI]: 0.51 [0.27-0.95], P = .04).
Mortality
Mortality was reported in 8 trials. As shown in Figure 4, mortality was significantly reduced in the DEB group compared with the POBA group (RR [95% CI]: 0.44 [0.21-0.96], P = .04), while the difference was not significant between the DEB and the DES groups (RR [95% CI]: 0.70 [0.21-2.34], P = .57). Without subgroup analysis, mortality was significantly reduced in the DEB group (RR [95% CI]: 0.51 [0.27-0.95], P = .04).
Myocardial infarction
Myocardial infarction was reported in 8 trials. As shown in Figure 4, difference was not significant between DEB and POBA (RR [95% CI]: 1.32 [0.55-3.15], P = .30) or DEB and DES (RR [95% CI]: 0.66 [0.30-1.44], P = .57) groups. Without subgroup analysis, the difference between DEB and control groupd was not significant (RR [95% CI]:0.9 [0.50-1.60], P = .72).
Stent thrombosis
Stent thrombosis was reported in 8 trials. As shown in Figure 4, the difference was not significant between the DEB and the POBA (RR [95% CI]: 0.49 [0.02-9.55], P = .63) or DEB and DES (RR [95% CI]: 1.86 [0.32-10.66], P = .63) groups. Without subgroup analysis, the difference between the DEB and the control groups was not significant (RR [95% CI]: 0.88 [0.23-3.38], P = .85).
Sensitivity Analysis
The results of sensitivity analysis of major outcomes are shown in Table 2, and they were similar to the results of main analysis. Both in sensitivity analysis and in main analysis, the results showed that when compared to the POBA, DEB can significantly reduce the risk of BR, MACE, and TLR. However, this superiority of DEB was not significant when compared with DES.
Characteristics of Included Studies.
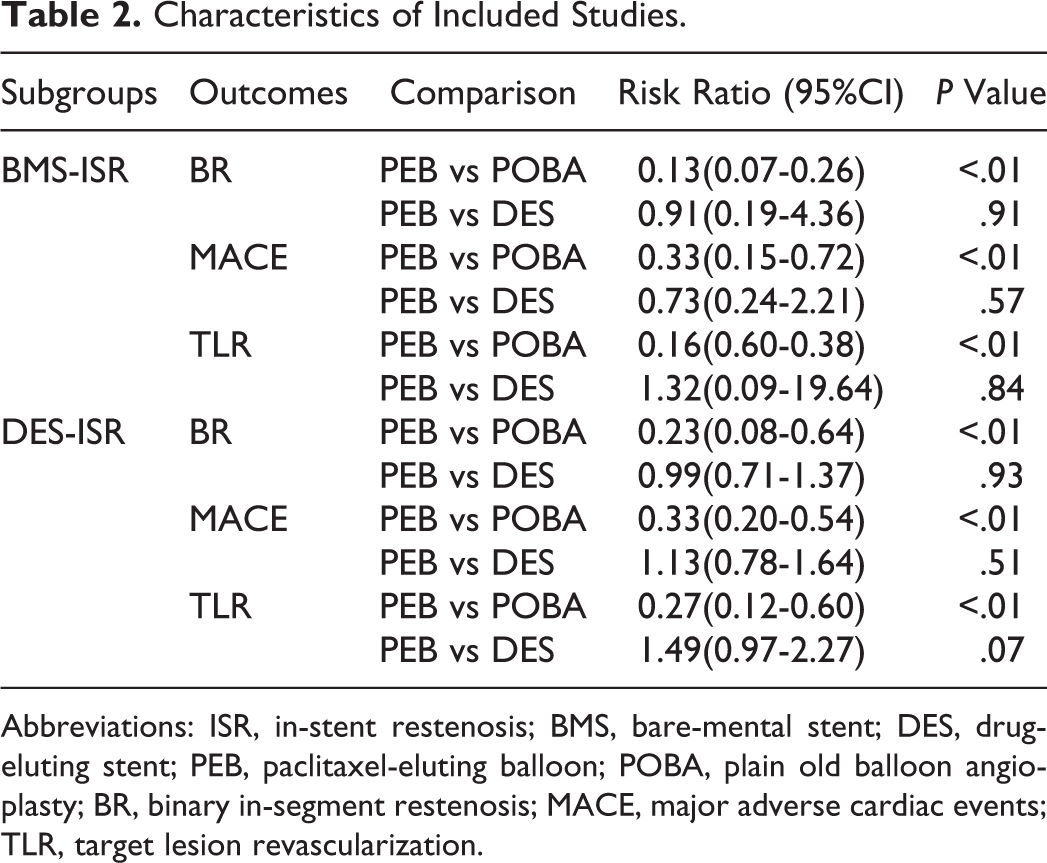
Abbreviations: ISR, in-stent restenosis; BMS, bare-mental stent; DES, drug-eluting stent; PEB, paclitaxel-eluting balloon; POBA, plain old balloon angioplasty; BR, binary in-segment restenosis; MACE, major adverse cardiac events; TLR, target lesion revascularization.
Discussion
This meta-analysis, including 1413 patients from 8 randomized control trials, examined the effectiveness of DEB for the treatment of ISR compared with POBA and DES. The principal findings were (1) DEB and DES are clearly superior to current standard therapy using POBA; (2) DEB was noninferior to current standard therapy using DES; (3) overall, DEB can reduce mortality compared with POBA in treating ISR. A prior meta-analysis supports our conclusion to some extent. 15 However, the RIBS V Clinical Trial drew a different conclusion that DEB provides inferior late angiographic findings when compared with everolimus-eluting stents (EES). 6 This distinction may be caused by the bias between first- and second-generation stents, since previous studies have demonstrated the superiorities of second-generation stents compared with first0generation stents. 16,17
Currently, the management of ISR continues to represent a major clinical problem, and the treatment strategies are still unsettled. 18 Balloon angioplasty was one of the earliest strategies used in patients with ISR. However, treatment of ISR with POBA is limited, as it may be associated with high recurrent restenosis rates. 19 Several past studies have supported our conclusion that DEB is superior to POBA in treating ISR. 5,8 –11 These studies have confirmed this superiority not only for BMS-ISR 5,9 but also for DES-ISR. 8 –11 Meanwhile, a prior meta-analysis has drawn the same conclusion that DEB is a promising treatment option in treating ISR compared with POBA. 15 The reason leading to this kind of distinction may include subacute tissue reintrusion back to the lumen, edge-related complications, and the slippage of the balloon outside the stent (“watermelon seeding” phenomenon), which are limitations of POBA in treating ISR. 19 –21
Repeat stenting is another strategy for patients with ISR which can reduce the risk of restenosis. Compared with conventional strategies such as POBA or cutting balloon angioplasty, DES had been shown to result in superior angiographic and clinical outcomes. 22 –25 However, there are reasonable queries about whether the stent-in-stent strategy is the best option, since the multiple layers of stents may result in excessive inflammation, tissue ingrowth, and injury to the vessel wall. 19 In addition, using stent sandwich technique for the treatment of DES-ISR is still a confusing issue. Fibrotic tissues between 2 layers of DES may increase the risk of tissue protrusion and further decrease MLD, which might lead to more TVR and potential risk of ST. 26 Our study has confirmed that DEB has similar effects with DES, while a prior meta-analysis has shown that DEB is an optimal strategy among patients with ISR when it is compared with Taxus Liberte DES. 15 Several previous studies have presented that whether in patients with DES-ISR or patients with BMS-ISR, the use of DEB leads to preferable or at least analogous outcomes compared with DES. 5,7,12 Although the RIBS V Clinical Trial 6 drew a different conclusion that in patients with BMS-ISR, DEB provides inferior late angiographic findings when compared to EES, that did not translate into an inferior long-term clinical outcome. It was suggested that the relative large residual lumens post-DEB provide enough room to prevent any clinical consequence. A recent published study RIBS IV concluded that in patients with DES-ISR, EES provided superior not only in long-term clinical end points but also in angiographic results compared with DEB. 27 Further studies including a larger number of patients and a longer follow-up period would be needed to clarify the superiority of second-generation stents.
Compared to DEB, prior studies failed to demonstrate the superiority of restenting implantation in patients with ISR. Additionally, studies have observed that DES application in treating ISR may be associated with increased long-term ST rates. 28 Apart from the evidence mentioned earlier, using DES requires an increased period of antiplatelet therapy which may be associated with higher risk of postoperative bleeding. This factor also needs to be considered.
Currently, first-generation DEB is coated with paclitaxel, a highly lipophilic drug, which has rapid uptake and prolonged retention and can exert a sustained effect, despite a short contact time with the vessel wall. 29 The conclusion from a meta-analysis is that DEB is the optimal strategy in treating patients with ISR, principally as it can reduce the risk of MACE. 15 Beyond all that, our meta-analysis also found that DEB can reduce the risk of mortality in general. When compared with DES, we found that DEB has similar outcomes. The factors we speculate that may contribute to this noninferiority are as follows. Drug-eluting balloons, as nonstent options, avoid injuries from second layers of metal in a coronary artery. Furthermore, a low systemic exposure is achieved with an effective local drug concentration by the coating drug onto the surface of a conventional balloon. 2,30,31 Meanwhile, compared with DES therapy, a shorter period of antiplatelet therapy is another advantage of using DEB in patients with ISR, since this may be associated a lower bleeding risk. 12 In addition, compared with DES, DEB avoids the potential risk of corrosion of the stent and prevents inflammation or tissue ingrowth caused by permanent implant. 15 Based on the above-mentioned findings, we concluded that DEB may be an optimal strategy when compared to either POBA or DES.
Limitations
This meta-analysis is only based on 8 relatively small and heterogeneous randomized control trials. Although the pooling and formal statistical methods increase the power, it is still inefficient. We did not separate the patients with ISR into BMS-ISR and DES-ISR because of the number limitation which may lead to a higher clinical heterogeneity. In addition, the period of clinical follow-up in the PACCOCATH ISR study 9 is 60 months, which varies considerably with other studies. This factor may result in the heterogeneity of long-term results. It has to be considered that postoperative application of antiplatelet agents were not completely equivalent in included studies, leading to variance of bleeding risk in long-term follow-up.
Conclusion
Overall, DEB and DES are clearly superior to POBA in treating ISR. In addition, DEB can reduce mortality compared with POBA. However, when compared to DES, DEB had similar effectiveness.
Footnotes
Authors’ Note
Shen Gao, Jing Shen, Venkata Kishore Mukku, Mei Jia Wang, Muzina Akhtar, Wei Liu contributed to (1) conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published. Shen Gao and Wei Liu were Guarantor of integrity of entire study; Wei Liu contributed to Study concepts; All authors contributed to Study design; Shen Gao, Jing Shen, and Mei Jia Wang contributed to Literature research; Shen Gao and Muzina Akhtar contributed to data acquisition; Shen Gao, Jing Shen, and Muzina Akhtar contributed to data analysis/interpretation; Shen Gao and Mei Jia Wang contributed to statistical analysis; Shen Gao, Jing Shen, Venkata Kishore Mukku, Mei Jia Wang, Muzina Akhtar, and Wei Liu contributed to manuscript preparation; Shen Gao, Jing Shen, Venkata Kishore Mukku, and Wei Liu contributed to manuscript definition of intellectual content; Shen Gao, Jing Shen, Venkata Kishore Mukku, and Wei Liu contributed to manuscript editing; Shen Gao, Jing Shen, Venkata Kishore Mukku, and Wei Liu contributed to manuscript revision/review; all authors contributed to manuscript final version approval; and Shen Gao and Jing Shen contribute equally to the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by National Nature Science funding: 81470429.