
Abstract
Current guidelines recommend maintaining serum potassium levels between 4.0 and 5.0 mEq/L (1 mEq/L = mmol/L) in patients with acute myocardial infarction. However, these guidelines are based on studies conducted before the β blocker and reperfusion era. We retrospectively analyzed 6613 patients diagnosed with ST-segment elevation myocardial infarction (STEMI) who presented without renal insufficiency. Patients were categorized into 5 groups according to mean serum potassium levels: <3.5, 3.5 to <4.0, 4.0 to <4.5, 4.5 to <5.0, and ≥5.0 mEq/L. Patients with potassium levels of 4.0 to <4.5 mEq/L had the lowest predefined event rates, which were 6.4% for 7-day malignant arrhythmia, 3.7% for 7-day mortality, and 5.3% for 30-day mortality. Compared with the reference group (4.0 to <4.5 mEq/L), multivariate regression analysis revealed significantly higher 30-day mortality risk in patients with potassium level of 4.5 to <5.0 (hazard ratio [HR]: 1.52, 95% confidence interval [CI]: 1.17-1.98; P = .002) and even higher risk in patients with potassium level of ≥5.0 mEq/L (HR: 1.80, 95% CI: 1.22-2.66; P = .002). The lowest 30-day mortality was observed in patients with STEMI having potassium levels between 4.0 and 4.5 mEq/L, and a level >4.5 mEq/L significantly increased mortality risk.
Introduction
Potassium homeostasis is an important determinant of cardiac function, and a serum potassium level between 3.5 and 5.3 mEq/L (1 mEq/L = 1 mmol/L) is maintained by intracellular and extracellular shift and renal excretion. 1 Hypokalemia, generally defined <3.5 mEq/L, has been shown to increase the risk of early severe ventricular arrhythmias in patients with acute myocardial infarction (AMI). 2 –6 Based on previous studies, clinical practice guidelines recommend maintaining serum potassium levels between 4.0 and 5.0 mEq/L, 7,8 and some experts even advise a higher range of 4.5 to 5.5 mEq/L in patients with AMI. 1 However, this evidence was derived from small observational studies conducted prior to modern treatments with β blockers and early reperfusion. Recently, Goyal et al reported that the lowest in-hospital mortality was observed in patients with AMI having potassium levels of 3.5 to 4.0 mEq/L, and levels >4.5 mEq/L were associated with increased mortality. 9 Choi et al came to the same conclusion regarding long-term mortality. 10
The results mentioned previously pose substantial challenge to current guideline recommendations, and further research is needed to confirm the optimal range of serum potassium level with respect to clinical outcomes. Besides, given that the kidney is normally responsible for most potassium excretion and renal insufficiency is mainly responsible for most hyperkalemia in clinical settings 11,12 and the risk of death increases with the degree of renal insufficiency in patients with AMI, 13,14 it may be more reasonable to evaluate the effect of serum potassium in patients with well-preserved renal function. Therefore, we conducted this study to clarify the relationship between serum potassium levels and incidence of malignant arrhythmias and short-term mortality in patients with ST-segment elevation myocardial infarction (STEMI) who presented without renal insufficiency.
Methods
Study Population
A total of 6613 consecutive patients who were admitted to the emergency departments of 274 Chinese hospitals from June 2001 to July 2004 with a diagnosis of STEMI within 12 hours after the onset of symptoms were analyzed retrospectively. The original study protocol was set to evaluate the reperfusion treatment and short-term prognosis of patients with STEMI in a multicenter study, which included tertiary, secondary, and community hospitals with and without coronary intensive care units.
Diagnosis of STEMI was defined as the presence of chest pain or equivalent syndromes for myocardial ischemia, persistent ST-segment elevation (more than 0.1 mV in at least 2 contiguous extremity leads or 0.2 mV in at least 2 contiguous precordial leads) or new left bundle-branch block on electrocardiogram, and elevated biomarker troponin I or creatine kinase MB indicating myocardial necrosis. 15 Exclusion criteria of the original study were any history of hemorrhagic stroke within 12 months, gastrointestinal bleeding or active peptic ulcer within 3 months, major surgery or trauma within 2 weeks, coagulation disorders associated with bleeding tendency, renal insufficiency with creatinine >2.0 mg/dL or 175 µmol/L (serum creatinine >2.0 mg/dL was classified as renal insufficiency in this study), pregnancy, and life expectancy <1 month. This study was approved by the institutional review board of each participating center. All participants provided written informed consent.
Data Collection
After admission, patients received suitable medication to comply as much as possible with the guidelines for the treatment of STEMI. Reperfusion therapy including thrombolysis and percutaneous coronary intervention was performed according to local clinical circumstances. Baseline characteristics including demographic data, medical history, vital signs on admission, and hospital treatment were obtained from medical records. The Thrombolysis In Myocardial Infarction (TIMI) risk score for each patient was calculated according to the score criterion. 16 Serial serum potassium levels were measured at baseline, 6 ± 2 hours, and 24 ± 4 hours after admission. The mean serum potassium level was defined as the average of 3 measurements, and for any patient who had 1 extreme potassium measurement, the average of 2 other measurements was taken as mean level. Patients were categorized into 5 groups to determine the relation between mean serum potassium levels and short-term outcomes: <3.5, 3.5 to <4.0, 4.0 to <4.5, 4.5 to <5.0, and ≥5.0 mEq/L (1 mEq/L = 1 mmol/L). Hypokalemia was defined as serum potassium <3.5 mEq/L.
Study End Points
All patients received 30 days of follow-up, during which survival status and occurrence of malignant arrhythmia were assessed and recorded. The occurrence of malignant arrhythmia was only monitored and recorded during hospitalization, as each patient would stay in the hospital for at least 7 days. After discharge, follow-up information was obtained by office visit or telephone call with patients or their family.
The primary outcomes included 7-day malignant arrhythmia, 7-day all-cause mortality, and 30-day all-cause mortality. Malignant arrhythmia was defined as the composite of life-threatening arrhythmias including sustained ventricular tachycardia (the occurrence of tachycardia lasting more than 30 seconds and leading to hemodynamic collapse) or ventricular fibrillation, cardiac arrest with asystole, and high-degree atrioventricular block (Mobitz II second-degree or third-degree atrioventricular block).
In the current study, the diagnoses of STEMI and malignant arrhythmia were based on the local treating physician’s judgement according to the supplied criteria in the study protocol. While for each diagnosis, a corresponding electrocardiogram was required to be provided as evidence. All the data mentioned before were collected prospectively by local physicians using unified case report forms and were sent to the central administrative office of the study located at Fuwai Hospital, Beijing.
Statistical Analysis
Continuous variables with normal distributions were presented as mean ± standard deviation (SD) and were compared using 1-way analysis of variance. Continuous variables with skewed distributions were presented as median (with 25th and 75th percentiles) and were compared using the Kruskal-Wallis test. Categorical variables presented as numbers and percentages were compared using Pearson χ2 or Fisher exact test. Multivariate Cox proportional hazard regression models were performed to compare primary outcomes by categories of serum potassium level. The hazard ratios indicate the relative risk of arrhythmia or mortality in each potassium group compared with those in the lowest risk potassium group (4.0 to <4.5 mEq/L). The following models were built to assess the relative confounding effect of certain factors: unadjusted, adjusted for TIMI risk score, and adjusted for all covariates. Cumulative all-cause mortality curves were constructed using the Kaplan-Meier method. Log-rank tests were used to compare the curves of serial potassium groups. All statistical tests were 2 tailed, and P values <.05 were considered significant. Statistical analyses were carried out using SPSS version 19.0 (SPSS Inc, Chicago, Illinois).
Results
Figure 1 shows the distribution of the mean serum potassium levels measured within the first 24 hours of hospitalization, which was approximately a normal distribution with a mean level of 4.1 ± 0.4 mEq/L and a median level of 4.1 (3.9-4.4) mEq/L. Hypokalemia (<3.5 mEq/L) was observed in 834 (12.6%) patients at baseline, 410 (6.2%) patients at 6 hours, and 298 (4.5%) patients at 24 hours after admission. High serum potassium (≥5.5 mEq/L) was observed in 68 (1.0%) patients at baseline, 158 (2.4%) patients at 6 hours, and 229 (3.5%) patients 24 hours after admission.
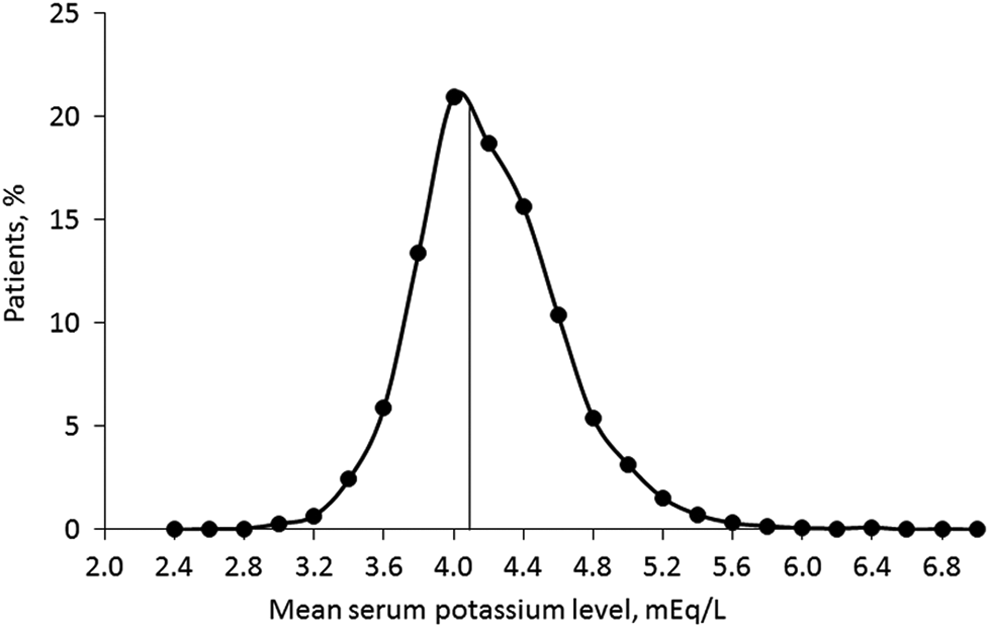
The distribution of mean serum potassium levels in patients with ST-segment elevation myocardial infarction (STEMI).
Baseline characteristics by mean serum potassium level are listed in Table 1. The relationship between potassium levels and baseline variables was complicated: age and percentage of diabetes mellitus increased gradually across all potassium level groups and patients at the extremes of serum potassium level (<3.5 or ≥5.0 mEq/L) were more likely to be female, have higher heart rate, blood pressure, Killip class, and longer onset-to-admission time. Those patients also tended to have a higher percentage of hypertension and heart failure histories. Patients at the level of <3.5 mEq/L presented more extensive anterior myocardial infarction and those at the level of ≥5.0 mEq/L had higher TIMI risk score. As for hospital treatments (Table 2), patients at the level of ≥5.0mEq/L were less likely to receive thrombolysis, clopidogrel, heparin, and angiotensin-converting enzyme inhibitor or angiotensin-receptor blocker, whereas those patients received more diuretic treatment.
Baseline Characteristics by Mean Serum Potassium Levels.a
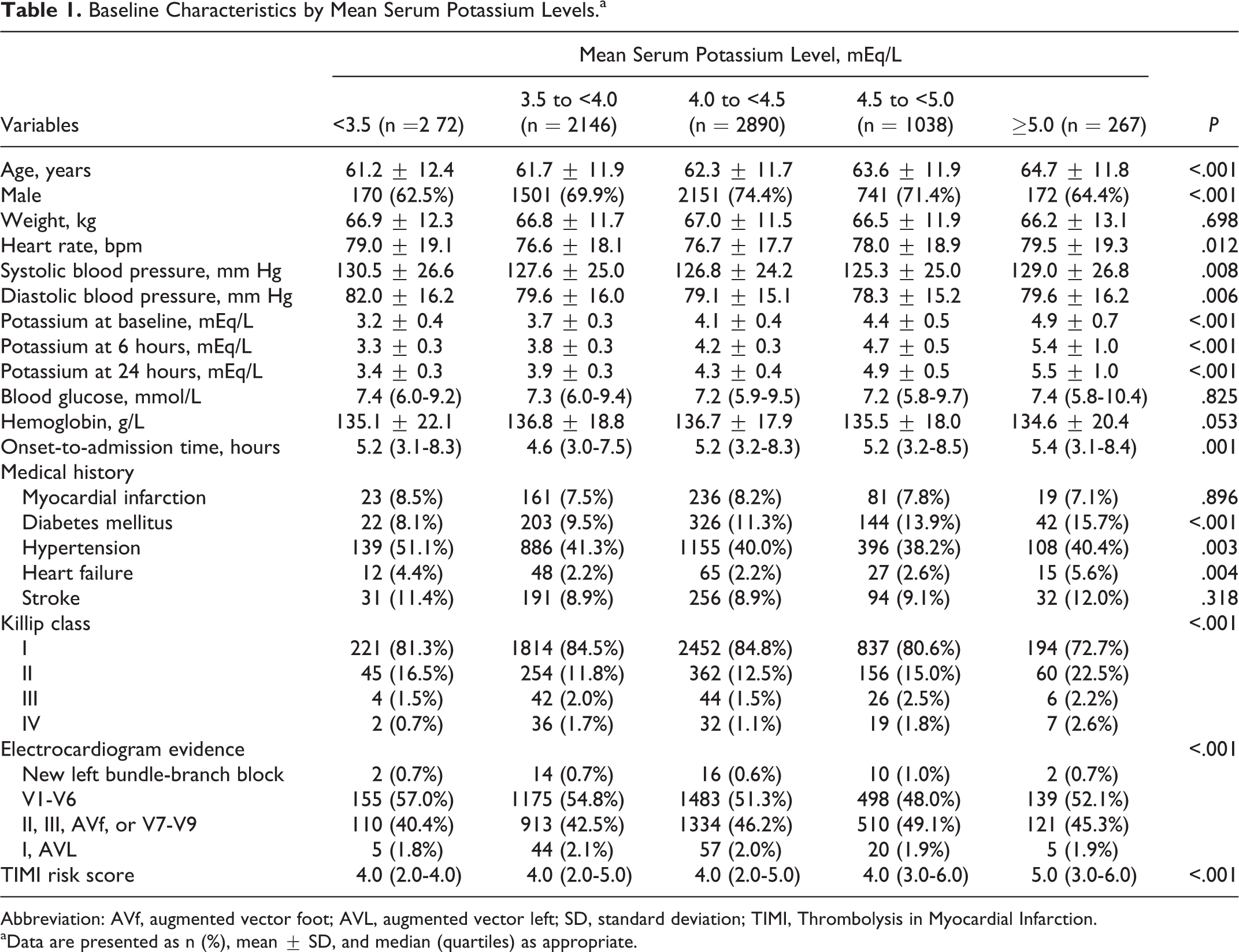
Abbreviation: AVf, augmented vector foot; AVL, augmented vector left; SD, standard deviation; TIMI, Thrombolysis in Myocardial Infarction.
aData are presented as n (%), mean ± SD, and median (quartiles) as appropriate.
Hospital Treatments by Mean Serum Potassium Levels.a
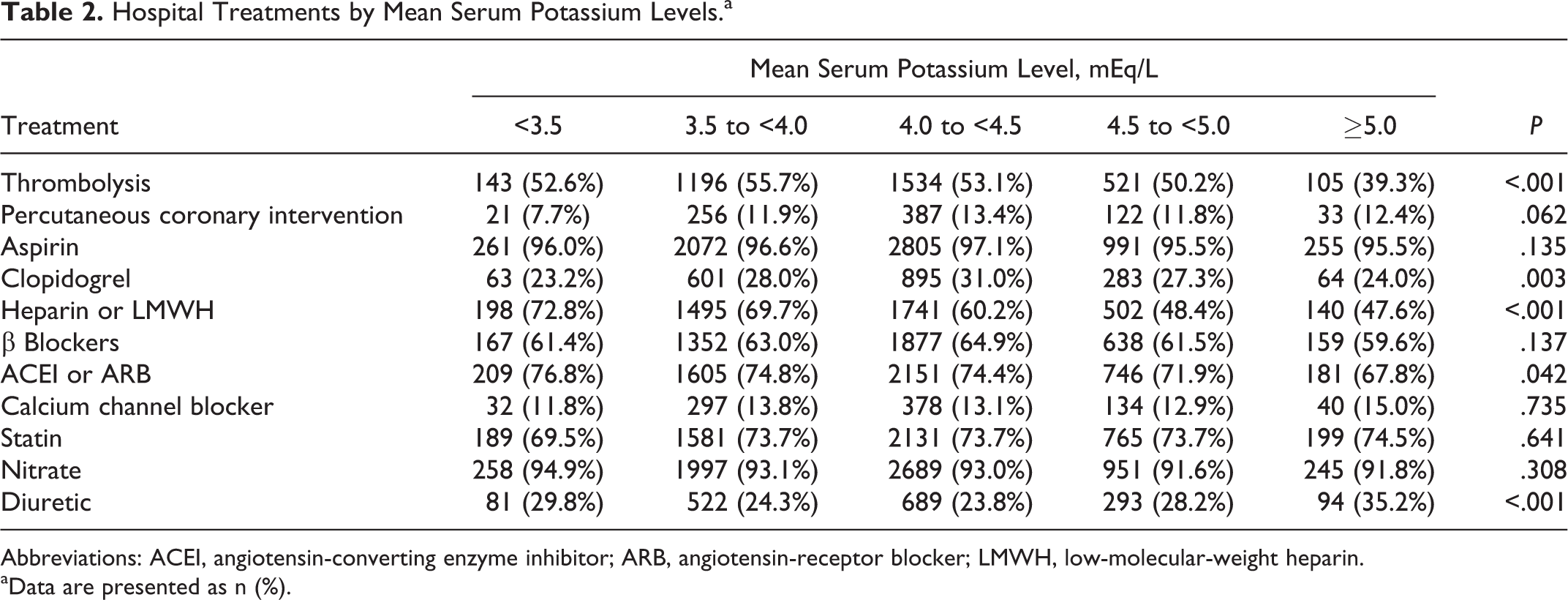
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker; LMWH, low-molecular-weight heparin.
aData are presented as n (%).
With regard to clinical outcomes, patients with mean serum potassium level of 4.0 to <4.5 mEq/L had the lowest predefined event rates compared with other potassium level groups, which were 6.4% for 7-day malignant arrhythmia (P = .042), 3.7% for 7-day mortality (P = .004), and 5.3% for 30-day mortality (P < .001; Table 3 and Figure 2). Life-threatening malignant arrhythmias were recorded in 464 (7.0%) patients during hospitalization. Compared with the reference group (4.0 to <4.5 mEq/L), unadjusted and adjusted Cox proportional regression analysis did not show significant increase in the risk of 7-day malignant arrhythmia according to the mean serum potassium levels (Table 3). Figure 3 shows the incidence distribution of separate type of malignant arrhythmia, and there was a trend that rates of ventricular arrhythmias, cardiac arrest, or high-degree atrioventricular block were consistently low and flat across a wide range of potassium levels (3.5 to <4.5 mEq/L).
Event Rates and Cox Proportional Hazard Models for Arrhythmia and Mortality by Mean Serum Potassium Levels.
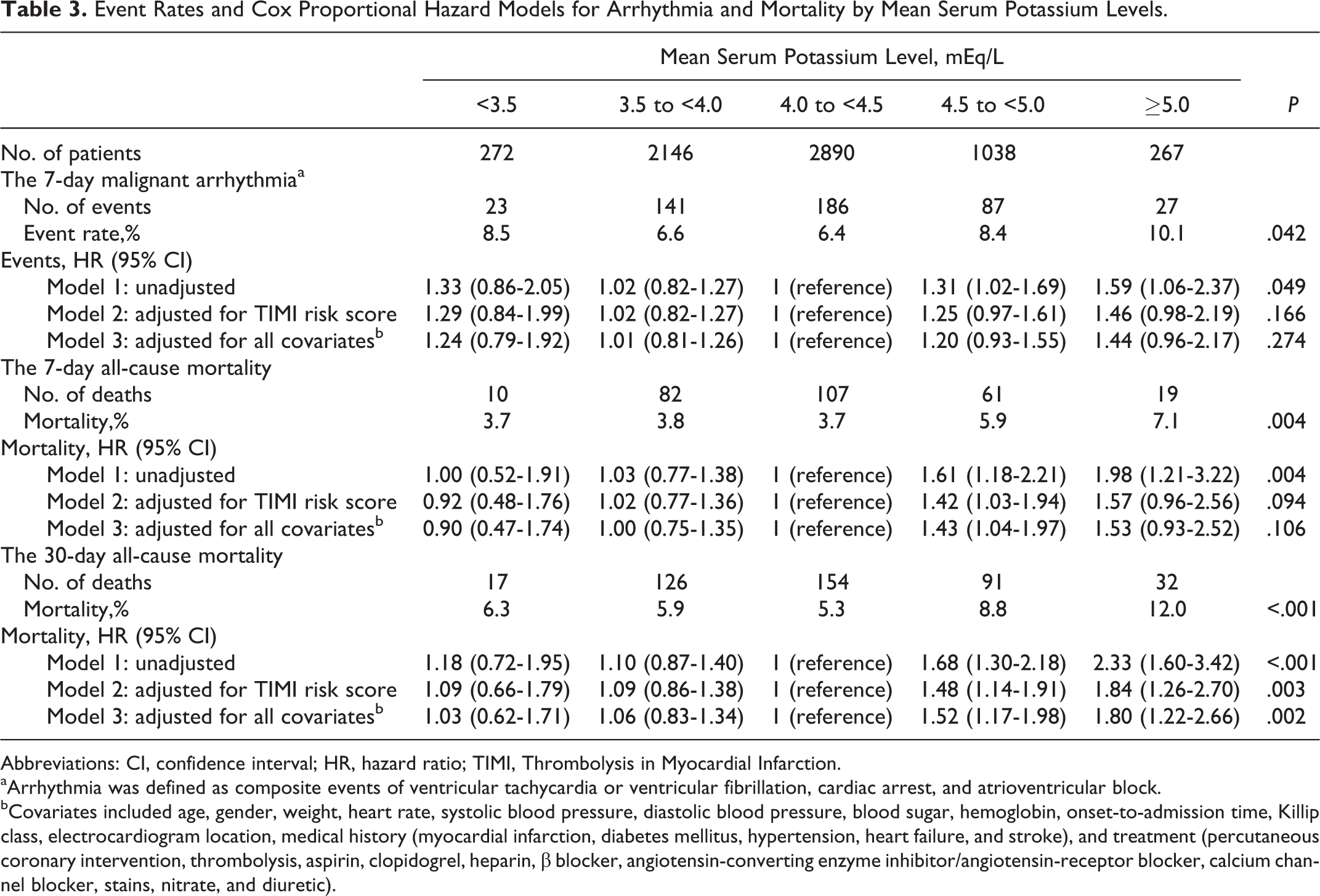
Abbreviations: CI, confidence interval; HR, hazard ratio; TIMI, Thrombolysis in Myocardial Infarction.
aArrhythmia was defined as composite events of ventricular tachycardia or ventricular fibrillation, cardiac arrest, and atrioventricular block.
bCovariates included age, gender, weight, heart rate, systolic blood pressure, diastolic blood pressure, blood sugar, hemoglobin, onset-to-admission time, Killip class, electrocardiogram location, medical history (myocardial infarction, diabetes mellitus, hypertension, heart failure, and stroke), and treatment (percutaneous coronary intervention, thrombolysis, aspirin, clopidogrel, heparin, β blocker, angiotensin-converting enzyme inhibitor/angiotensin-receptor blocker, calcium channel blocker, stains, nitrate, and diuretic).
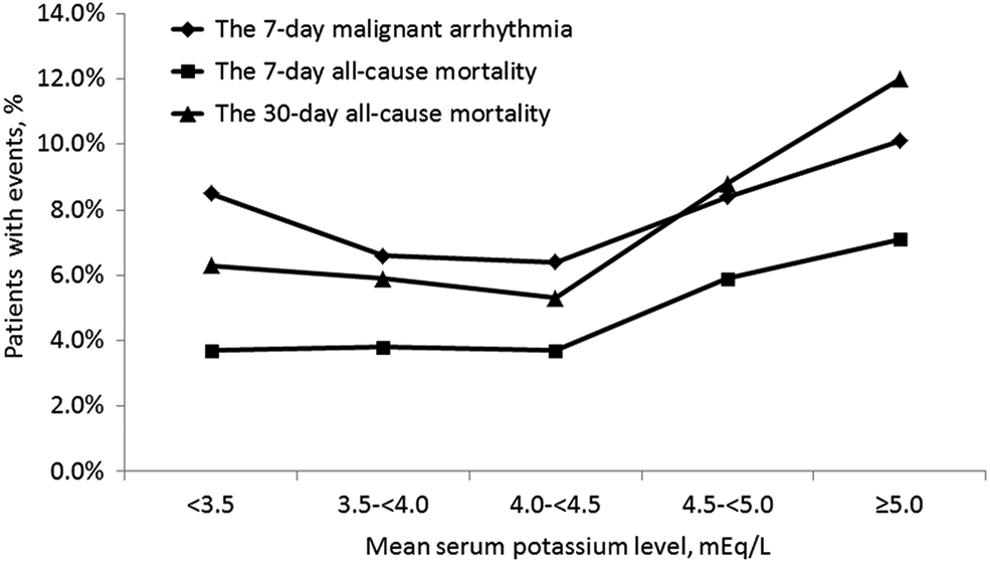
The incidence of short-term outcomes by mean serum potassium levels.
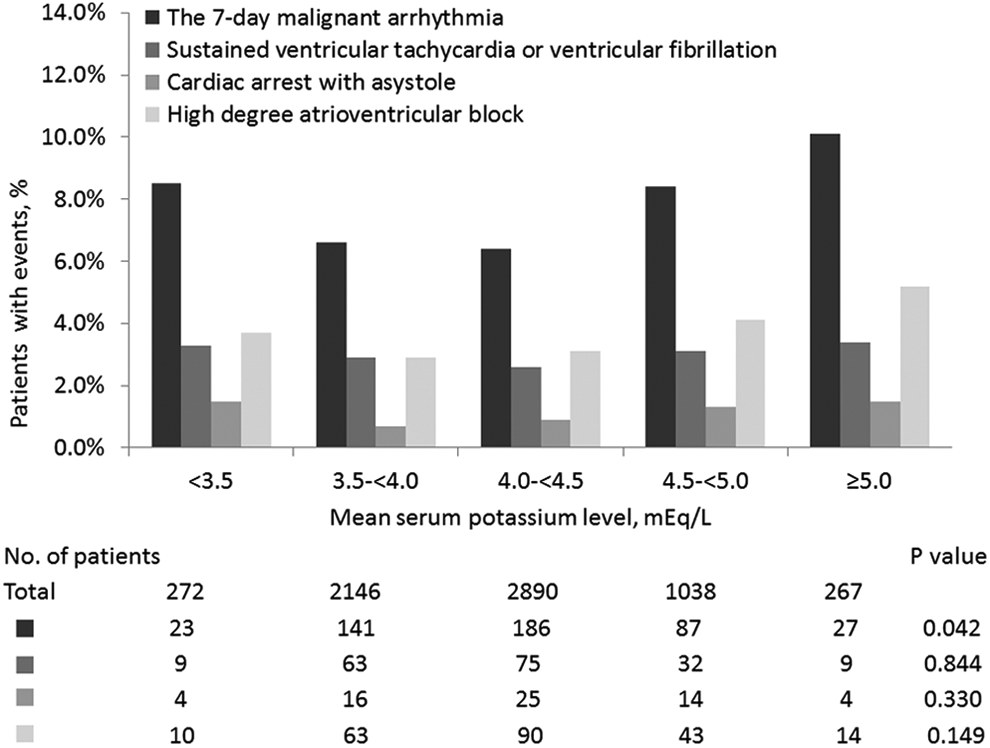
The incidence of separate type of malignant arrhythmia by mean serum potassium levels.
Of the 6613 patients with STEMI, 279 (4.2%) patients died within the first 7 days. Unadjusted Cox proportional regression analysis showed similar 7-day mortality rate in patients with potassium level of <3.5, 3.5 to <4.0, and 4.0 to <4.5 mEq/L and significantly higher mortality rate when the potassium level increased to >4.5 mEq/L (P = .004). However, this relationship did not reach statistical significance after we adjusted for TIMI risk score or included all covariates in the Cox models (Table 3). On the other hand, 420 (6.4%) patients died during the 30 days of follow-up. Unadjusted analysis showed a U-shaped relationship between 30-day mortality and serum potassium levels (P < .001), and this relationship was only slightly attenuated and persisted after adjustments for TIMI risk score (P = .003) or covariates (P = .002; Table 3). Figure 4 displays the Kaplan-Meier curves for 30-day mortality. Analysis using the log-rank test revealed significant difference among the serial potassium level groups (P < .001), with a significantly higher cumulative mortality rate at a level ≥5.0 and 4.5 to <5.0 mEq/L than in the other 3 low-level groups.
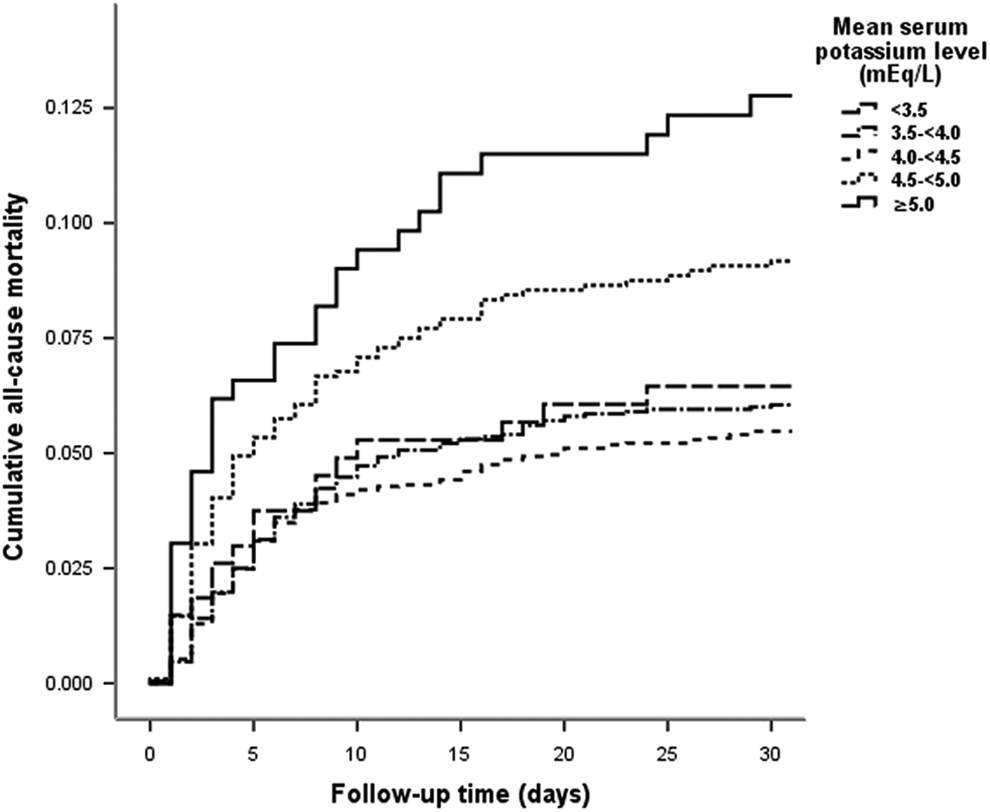
Kaplan-Meier curves for 30-day all-cause mortality by mean serum potassium levels.
Discussion
We demonstrated a significant U-shaped relationship between mean serum potassium levels measured within 24 hours after admission and 30-day all-cause mortality. The lowest mortality was observed among patients with STEMI having potassium level between 4.0 and 4.5 mEq/L who presented without renal insufficiency, and a high level of potassium >4.5 mEq/L was associated with significantly higher 30-day all-cause mortality. This relationship remained statistically significant after adjustment for TIMI risk score or potential covariates. However, no relationship was observed between the mean serum potassium levels and the occurrence of malignant arrhythmias or 7-day all-cause mortality in our study.
The ratio of transmembrane potassium concentrations is the primary determinant of the resting potential. Hypokalemia causes cellular hyperpolarization, increases resting potential, hastens depolarization, and increases automaticity and excitability. 1,17,18 Because cardiac repolarization relies on potassium influx, hypokalemia lengthens the action potential, increases QT dispersion (reflecting electrical inhomogeneity), and predisposes patients to potential fatal arrhythmias. 1,17,18 Baron et al found that adrenaline directly increases the active pumping of potassium into cells and sodium out of them, by a β2-adrenoceptor-dependent mechanism linked to Na-K-ATPase, in isolated human leukocytes in vitro. Their findings were supported by the adrenaline-induced effect being abolished by nonspecific (β1, β2) blockade using timolol, whereas the β1 receptor blocker, atenolol, had no effect. 19 Then, Turaihi et al came to similar results that active 86Rb (representing K) influx in human platelets is enhanced by the stimulation of β adrenoceptors of the β2 subtype, and the stimulatory effect of adrenaline was markedly inhibited by timolol (>80% inhibition at 30 nmol/L). 20 Thus, adrenaline stimulates the Na-K-ATPase pump via β2 receptors and shifts potassium intracellularly, and there may also be local effects of β blockers on ATPase activity. 19 –21 Raised concentration of circulating adrenaline has been suggested as a cause of transient hypokalemia during the acute presentation of AMI, 22 and many studies have proposed an increased risk of ventricular arrhythmias associated with such hypokalemia. 2 –6
Based on this evidence, guidelines recommend maintaining serum potassium at a level of 4.0 to 5.0 mEq/L in patients with AMI. 1,7,8 However, most of those studies were conducted prior to modern treatment with β blockers and early reperfusion. β Blockers increase serum potassium level and prevent the occurrence of ventricular arrhythmias by blocking adrenaline-induced hypokalemia derived by the stimulation of Na-K-ATPase pump via β2 receptors. 23 –25 In our study, more than one-half (63.4%) of patients used β blockers, and during hospitalization, malignant arrhythmia events occurred in 464 (7.0%) patients, among whom 188 (2.8%) patients experienced an episode of sustained ventricular tachycardia or ventricular fibrillation. Those figures are lower than those observed in prior studies mentioned before, which reported a 10% to 50% incidence rate of ventricular arrhythmias in patients with AMI during the pre–β blocker era. 2 –6 Our study did not show significant relationship between the mean serum potassium levels and the occurrence of malignant arrhythmias in patients with STEMI. This finding is similar to the study by Choi et al. 10
A high-volume study conducted by Goyal et al revealed that a mean serum potassium level >4.5 mEq/L was associated with increased in-hospital mortality, and a level between 3.5 and 4.0 mEq/L is the optimal range for acute patients with AMI. 9 Choi et al further extended this finding to an association with 3-year mortality in patients with AMI. 10 More recently, Peng et al reported similar results in patients with acute coronary syndrome: long-term mortality (28 months) risk was lowest in patients with potassium levels of 3.5 to <4.0 mEq/L, whereas patients with levels of 4.0 to <4.5 mEq/L showed a comparable all-cause mortality. 26 In our study, we included patients with STEMI who presented without renal insufficiency to explore the influence of serum potassium on short-term outcomes. The kidney is normally responsible for most potassium excretion, and both renal insufficiency and end-stage dialysis are strong risk factors for increased mortality. 27,28 We noted that patients in the study by Goyal et al with potassium level >4.5 mEq/L tended to have a low glomerular filtration rate (mean GFR <60 mL/min) and a relatively high percentage of dialysis treatment (5.4%-14.3%). 9 There may be more to those patients underlying confounding factors other than the GFR value and dialysis in contributing to the increased mortality. In contrast to their findings, 9,10 the lowest 30-day mortality rate was observed in our patient group with a mean serum potassium level of 4.0 to 4.5 mEq/L, rather than 3.5 to 4.0 mEq/L, and no association was found with respect to 7-day mortality in the present study. This optimal range of our study was in accordance with that reported in a recent observation of Shiyovich et al which associates serum potassium levels with long-term (up to 10 years) mortality in patients with AMI. 29
It seems that during the β blocker and reperfusion era, the occurrence of ventricular arrhythmia has substantially decreased and is not as clinically meaningful in terms of mortality in patients with AMI. 30,31 Given that higher baseline potassium levels have been suggested to be associated with a larger scintigraphic infarct size in patients with STEMI 32 and all limited evidence including our study has indicated that high serum potassium level >4.5 mEq/L significantly increases short- or long-term mortality, 9,10,26,29 physicians should be cautious with the use and dose of potassium supplements to patients with potassium levels between 4.0 and 4.5 mEq/L, the range associated with the lowest mortality.
During analysis, Goyal et al used the admission serum potassium level as well as the mean level, but levels were taken very frequently and the authors showed levels that were stable over time. 9 Choi et al 10 and Peng et al 26 used admission serum potassium level. Shiyovich et al used generalized estimating equations. 29 We were not sure what was the optimal methodology, and in the present study, we used a mean level of 3 tests taken at similar times following admission. The reasons were as follows: (1) 3 potassium measurements taken at similar times were available for each patient; (2) taking a mean level might reduce the measurement error; and (3) we used the measured potassium level at each time point doing the same categorizing, risk assessing, and regression analyzing and came to similar results (results not shown).
The present study has several limitations. First, it was a retrospective observational study, and it was impossible to definitively determine a causal relation between serum potassium levels and short-term mortality. Second, the original study excluded all patients with creatinine >2.0 mg/dL during recruitment. Considering that all enrolled patients in the present study were without renal insufficiency, our findings might not represent all patients with STEMI. Third, data reflecting myocardial necrosis and cardiac function such as the creatine kinase MB and troponin I levels as well as left ventricular ejection fraction are not available. In addition, some patients might have been administered potassium supplements or reduction therapy during hospitalization, and the serum potassium levels might change after discharge. Therefore, we were unable to explore the relation between changes in potassium level over time and clinical outcomes. Finally, owing to insufficient guideline implementation, the rate of primary percutaneous coronary intervention in the current study is extremely low (about 10%), whereas the rate of thrombolysis is about 50%. The latter could reduce the applicability of the findings. Thus, prospective studies in the contemporary era are needed to confirm our results.
Footnotes
Acknowledgments
The authors thank all the investigators and study coordinators from every participating center for their invaluable cooperation, as well as all the patients who participated in this multicenter study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.