
Abstract
Endothelial cell-specific molecule-1 (endocan) is an immunoinflammatory marker linked to endothelial activation and dysfunction. We investigated the relationship between obstructive coronary artery disease (CAD), microvascular angina (MVA), and plasma levels of endocan. We included 53 healthy individuals as controls, 40 MVA patients, and 120 patients with obstructive CAD. The severity of CAD was assessed by the Gensini and SYNergy between percutaneous coronary intervention with TAXUS and Cardiac Surgery (SYNTAX) scores. Endocan levels were 382.7 (313.8-470.2) pg/mL in patients with obstructive CAD; 324.3 (277.1-460.7) pg/mL in MVA group, and 268.0 (226.4-336.5) pg/mL (P < .001) in controls. Endocan levels in obstructive CAD and MVA groups were similar but both were significantly higher than for the control group (P < .001 and P = .002, respectively). In subgroup analysis, similar to the hypertensive subgroup results, endocan was still an independent predictor of presence of obstructive CAD in normotensives (odds ratio = 1.005, 95% confidence interval = 1.001-1.010, P = .024). There was also an independent positive correlation between endocan levels and SYNTAX score both in the hypertensives (β = 0.414, t = 3.21, P = .002) and in the normotensives (β = .301, t = 2.23, P = .031). In conclusion, endocan could be a common predictor of the endothelium-dependent inflammatory processes, rather than related with specific risk factors.
Introduction
Endothelial dysfunction is the initial lesion regarding the development of coronary artery disease (CAD). 1 The role of inflammation and endothelial dysfunction markers in the progression of atherosclerosis was investigated in several studies. 2 Endocan is a dermatan sulfate proteoglycan, and its role in inflammation and tumor progression has been described. 3,4 It competes with intercellular adhesion molecule 1 (ICAM-1) for leukocyte function-associated antigen 1 (LFA-1) and participates in the cellular adhesion process. Endocan is an immunoinflammatory marker linked to the endothelial dysfunction and may be a useful predictor of cardiovascular (CV) disease events. 5 Hypertension (HT) is an important risk factor for CV diseases. It is believed that endothelial dysfunction plays a role in the development of HT. 6 The impairment of the endothelium-dependent vasodilatation and endothelial inflammatory activation is considered as the responsible factors for the pathogenesis of HT. Probably, the risk of CAD is increased in patients with HT due to these common pathways. 7 It has been reported that blood levels of endocan are elevated in patients with hypertensive CAD. 8 Furthermore, endocan is independently correlated with the presence and severity of CAD in hypertensives. 9 Endocan levels in normotensive and patients with stable CAD are not sufficiently documented.
Microvascular angina (MVA) is described in a subgroup of patients with exertional chest pain associated with documented stress-induced myocardial ischemia and angiographically nonobstructive atherosclerotic CAD. 10,11 Abnormal epicardial and/or microvascular coronary dysfunction can be detected in a large portion (up to 60%) of patients without obstructive CAD. 12 Microvascular angina accounts for at least one-third of the cases of angina in the absence of obstructive CAD. Endothelium-dependent and -independent coronary microvascular dysfunction is the main cause of MVA. 13,14 Among the other contenders are smooth muscle dysfunction, inappropriate sympathetic tone, microvascular atherosclerosis, and inflammation. 15 Although the cause of endothelial dysfunction in MVA is not well known, chronic inflammation can induce vascular dysfunction. Similar to patients with CAD, inflammatory markers and ICAM-1 levels are elevated in this group of patients. 16,17
Previous studies have shown that blood levels of endocan are associated with the presence and severity of CAD in hypertensives. 8,9 But to our knowledge, there are not enough data regarding its utility in patients with normotensive CAD and documented myocardial ischemia with normal coronaries. Because both conditions are characterized by the presence of endothelial dysfunction, we investigated the relationship between obstructive CAD, MVA, and plasma levels of endocan.
Methods
Study Population
Two hundred and seventy-four patients were evaluated for this study between November 2014 and June 2015. We carried outcoronary angiography in 221 patients, who have a documented positive stress test with typical stable exertional angina. Horizontal > 0.1 mV or downsloping ST-segment depression or reversible ischemic defect in the single-photon emission computed tomography (SPECT) were the accepted criteria for the positive stress test. One hundred and sixty patients were included into the study; 120 of them were diagnosed with obstructive CAD by means of coronary angiography, and the remaining 40 were angiographically normal MVA patients without any coronary luminal irregularity. All patients had myocardial ischemia on SPECT in the MVA group. In patients with normal coronary arteries, epicardial coronary artery spasm was excluded by prolonged hyperventilation during coronary angiography. Sixty-one patients were excluded from the study because of the nonobstructive CAD determined by their coronary angiograms. Fifty-three participants with atypical chest pain and normal perfusion on SPECT were included in the study as the control group. Patients with the following conditions were excluded: acute coronary syndrome; history of the previous myocardial infarction, coronary artery bypass grafting, or percutaneous coronary intervention (PCI); secondary HT; severe valvular diseases; congestive heart failure (New York Heart Association Class III to IV); renal and hepatic dysfunction; any active inflammatory disease; and atrial fibrillation and malignancy. All the participants included in the study were informed about the study, and written consents were obtained from all individuals. The institutional ethics committee approved the study. The study was carried out in accordance with the Helsinki Declaration.
Laboratory Analysis
Venous blood samples were obtained from patients with a period of at least 12 hours of fasting on the day of coronary angiography. Serum levels of high-sensitivity C-reactive protein (hs-CRP), fasting blood glucose levels, creatinine levels, complete blood count, and fasting serum lipid status including total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol (HDL-C), and triglyceride levels were evaluated with standard laboratory tests. Additional blood samples were collected using EDTA as an anticoagulant and were centrifuged for 15 minutes at 1500 g within 30 minutes of collection. Samples were kept at −80°C until the assays were performed. One night before testing, the serum samples were stored at +4°C to thaw. Endocan levels were measured by enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s protocol (Human ESM1/Endocan PicoKine ELISA Kit, Boster Biological Technology Co. Ltd, Pleasanton, California). The detection limit for endocan was 31.2 pg/mL. The intraassay and interassay coefficients of variation were ranged from 3.7% to 5.1% and 4.6% to 6.1%, respectively.
Transthoracic echocardiography was performed, and biplane Simpson’s ejection fraction (%) was calculated before coronary angiography (iE33, xMATRIX Echocardiography System with a 2.5 to 3.5 MHz transducer, Phillips Medical System, Bothell, Washington). Body mass index (BMI) values were calculated based on the height (m) and weight (kg) of each patient. Medications used before coronary angiography were noted.
SYNergy Between PCI With TAXUS and Cardiac Surgery and Gensini Scores
The coronary angiograms were evaluated by 2 experienced and independent observers, who were blind to the clinical data of the patients. Each coronary lesion with a diameter stenosis ≥ 50% in vessels ≥ 1.5 mm was scored, and SYNergy between PCI with TAXUS and Cardiac Surgery (SYNTAX) score were calculated. For SYNTAX scores, the online version was used. 18 The severity of the CAD was also calculated with Gensini score, which grades narrowing of the coronary artery lumen as 1 for 1% to 25% narrowing, 2 for 26% to 50% narrowing, 4 for 51% to 75% narrowing, 8 for 76% to 90% narrowing, 16 for 91% to 99% narrowing, and 32 for total occlusion. This score was then multiplied by a factor from 0.5 to 5 that takes into account the importance of the lesion’s position in the coronary arterial system. 19
Statistical Analysis
Statistical analyses were conducted using the Statistical Package for Social Sciences for Windows 21.0 (SPSS, Chicago, Illinois). The Kolmogorov-Smirnov test was used in determining whether the continuous variables were normally distributed or not. Continuous variables were expressed as mean ± standard deviation or median (interquartile range) values, whereas categorical variables were presented as percentages. For categorical variables, the differences between the 2 groups were tested by chi-square test. Where appropriate, one-way analysis of variance or Kruskal-Wallis test was used for the comparison of the 3 groups for continuous variables. Bonferroni multiple comparison post hoc test (for data with normal distribution) and Mann-Whitney U test (for data without normal distribution) were used for pairwise comparison. Univariate and multivariate logistic regression analysis was used for the determination of the independent predictors of the presence of CAD. Statistical subgroup analysis was performed for patients with and without HT. The standardized parameters that were found having a significance (P < .20) in the univariate analysis were evaluated by stepwise logistic regression analysis. Spearman test was used for correlation analysis between endocan levels and CAD severity scores. Multivariate linear regression analysis was conducted to assess the independent predictors of SYNTAX and Gensini scores. All P values were 2 sided, and a P < .05 was regarded as significant.
Results
The baseline demographic and laboratory data of the patients are shown in Table 1. High-density lipoprotein cholesterol levels were significantly higher in the control group (P < .001). As expected, left ventricular ejection fraction (LVEF) was lower in the CAD group (P < .01 compared with other groups). Besides these, there was no significant difference among the groups in regard to age, gender, BMI, risk factors for CAD, medications, and blood parameters.
Baseline Characteristics of the Study Population.a
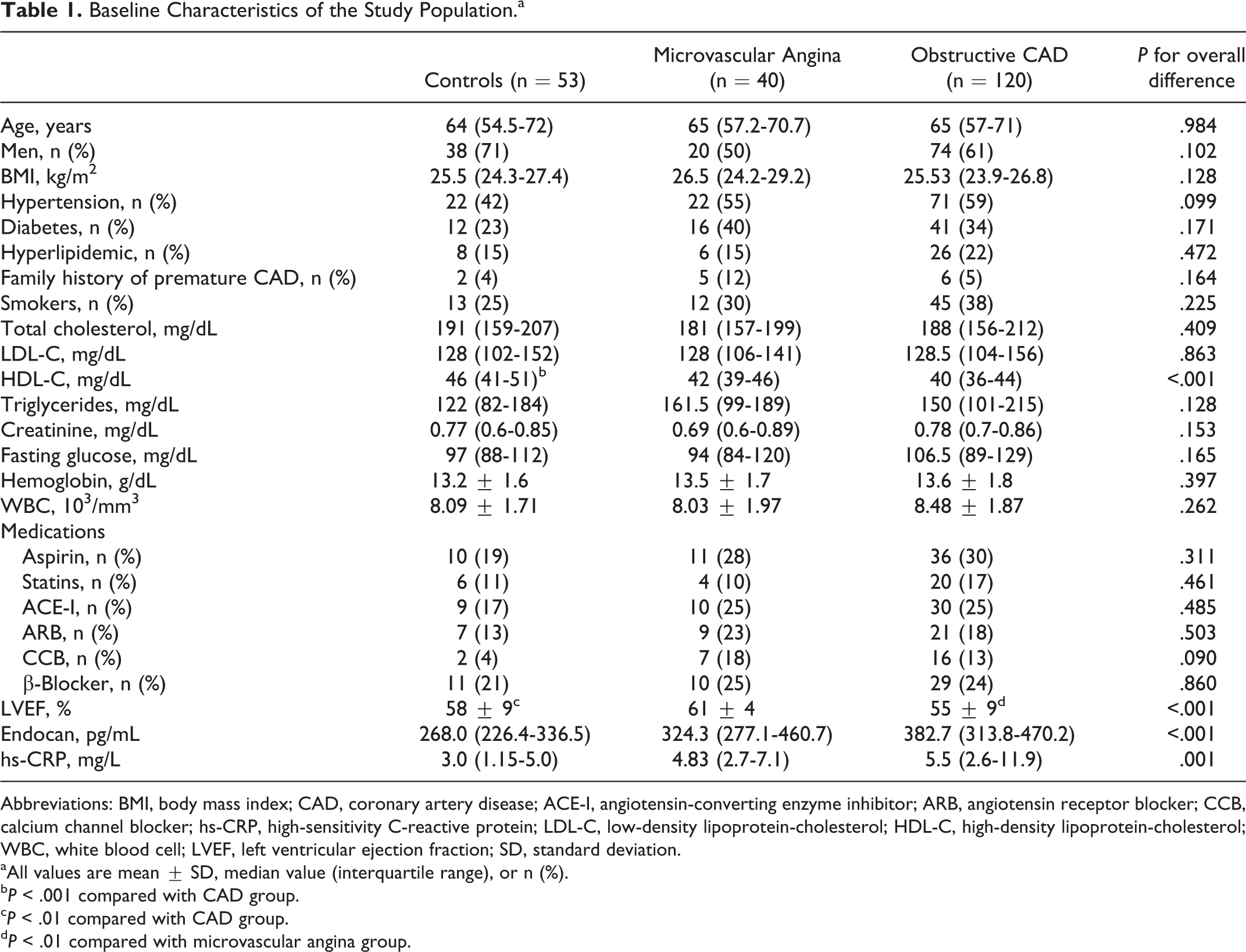
Abbreviations: BMI, body mass index; CAD, coronary artery disease; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein-cholesterol; HDL-C, high-density lipoprotein-cholesterol; WBC, white blood cell; LVEF, left ventricular ejection fraction; SD, standard deviation.
aAll values are mean ± SD, median value (interquartile range), or n (%).
b P < .001 compared with CAD group.
c P < .01 compared with CAD group.
d P < .01 compared with microvascular angina group.
Plasma endocan levels were 382.7 (313.8-470.2) pg/mL in patients with obstructive CAD; 324.3 (277.1-460.7) pg/mL in the MVA group, and 268.0 (226.4 – 336.5) pg/ml in the control group (P < .001). Paired comparisons showed that the endocan levels in obstructive CAD and MVA groups were comparable but both were significantly higher than the control group (P < .001 and P = .002, respectively; Figure 1A). Similarly, hs-CRP levels in patients with obstructive CAD and MVA patients are comparable, but both were higher than the control group (P < .001 and P = .006, respectively; Figure 1B). Plasma endocan levels showed a positive correlation with hs-CRP levels (r = .266, P < .001).
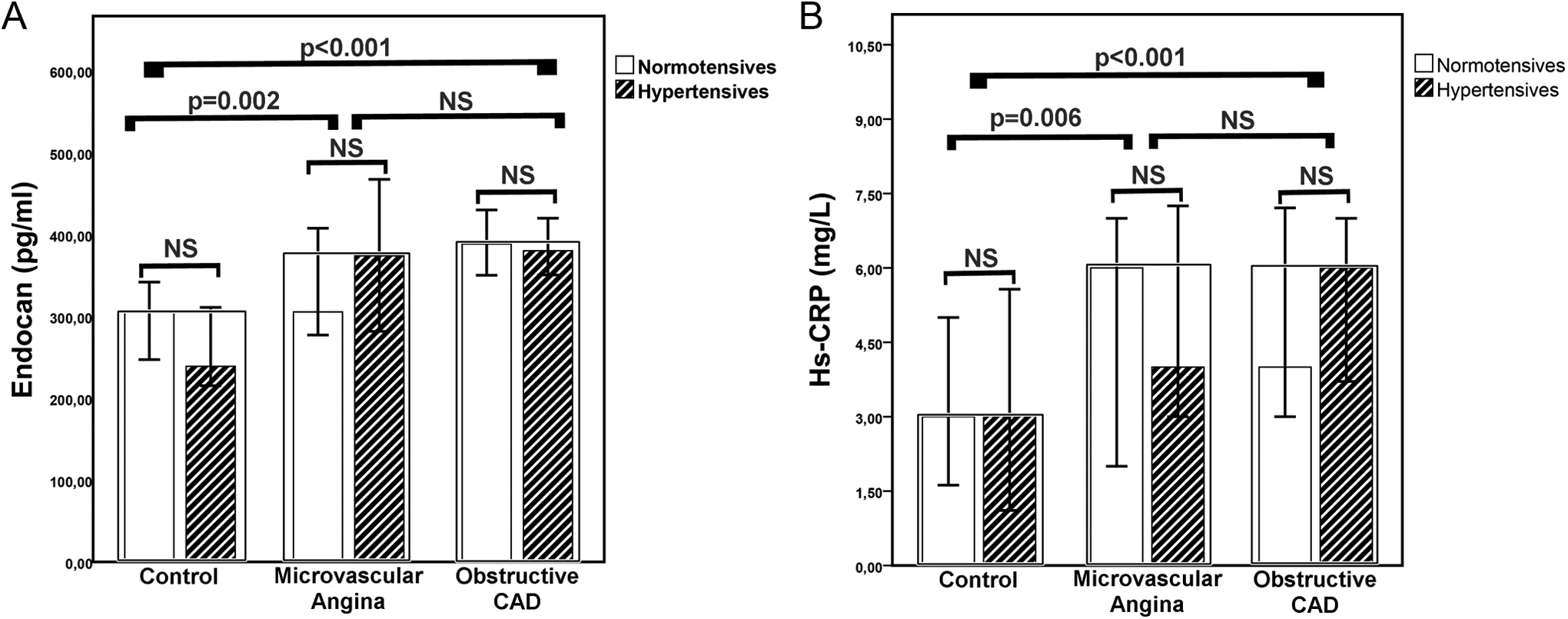
Comparison of endocan (A) and hs-CRP (B) levels in groups. hs-CRP indicates high-sensitivity C-reactive protein.
We planned regression analysis in order to determine the predictability of the presence of CAD with endocan levels. In the first analysis (where all patients are included), the parameters showing significance in the univariate analysis (HT, smoking, endocan, hs-CRP, white blood cell (WBC), fasting blood glucose, triglycerides, HDL-C, BMI, and LVEF) were evaluated by multivariate analysis to determine the independent predictors of CAD presence. In the multivariate analysis, BMI, LVEF, hs-CRP, and endocan were found to be independent predictors of CAD (Table 2). Receiver operating characteristic curve analysis showed that a serum endocan level above 323 pg/mL demonstrated a sensitivity of 74% and a specificity of 74% for the prediction of CAD (area under the curve 0.751, P < .001).
Logistic Regression Analysis for the Presence of Obstructive CAD.
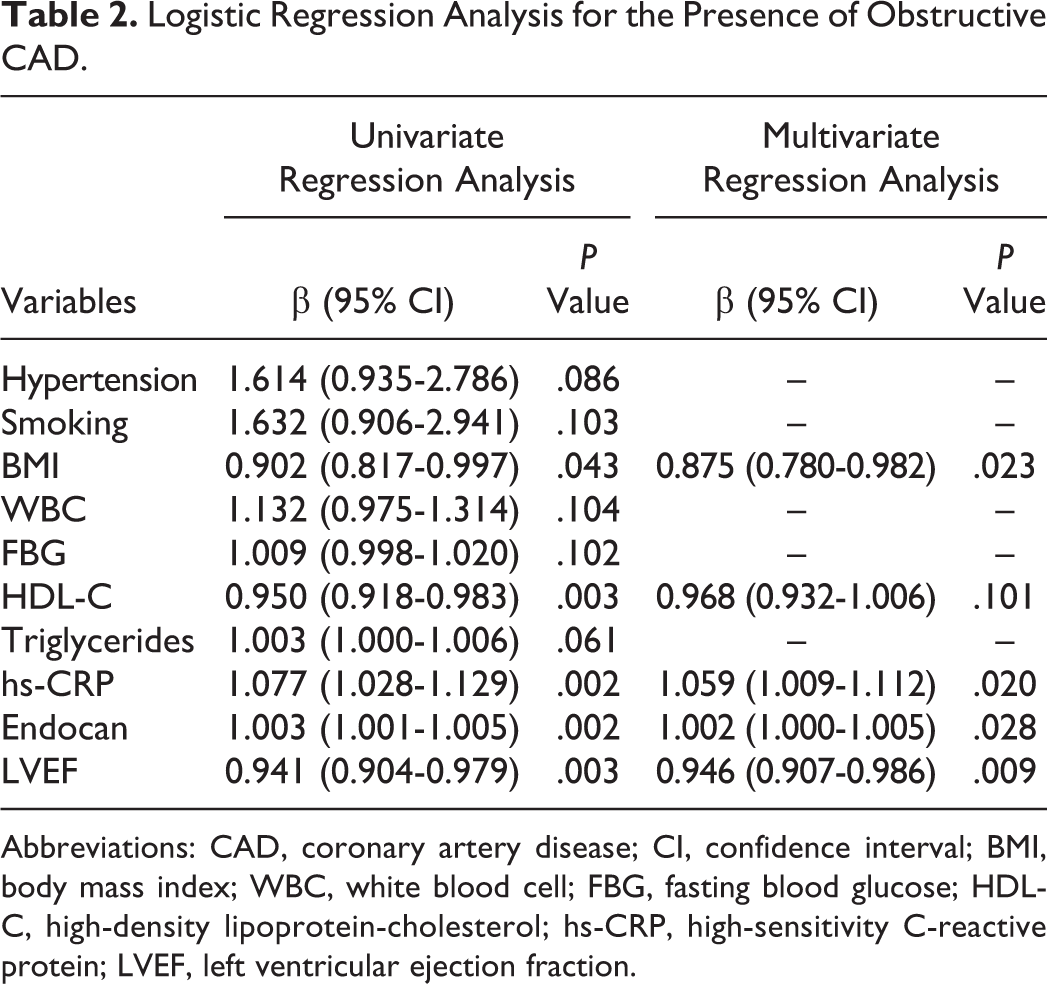
Abbreviations: CAD, coronary artery disease; CI, confidence interval; BMI, body mass index; WBC, white blood cell; FBG, fasting blood glucose; HDL-C, high-density lipoprotein-cholesterol; hs-CRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction.
In secondary analysis, we showed that in patients having HT with simple logistic regression, CAD presence is correlated with male gender (odds ratio [OR] = 1.9, 95% confidence interval [CI] = 0.9-4.3, P = .083), WBC (OR = 1.2, 95% CI = 0.9-1.4, P = .075), hs-CRP (OR = 1.06, 95% CI = 1.0-1.13, P = .052), LVEF (OR = 0.95, 95% CI = 0.90-1.0, P = .090), and endocan (OR = 1.003, 95% CI = 1.000-1.005, P = .042). When these parameters were evaluated with multivariate analysis, male gender (OR = 2.9, 95% CI = 1.1-7.1, P = .021), WBC (OR = 1.2, 95% CI = 1.0-1.5, P = .032), and endocan (OR = 1.003, 95% CI = 1.000-1.006, P = .032) were found to be independent predictors for obstructive CAD in hypertensives.
In normotensive subgroup, the parameters that showed significance in the univariate analysis were male gender (OR = 2.6, 95% CI = 1.1-6.6, P = .031), BMI (OR = 0.8, 95% CI = 0.6-0.9, P = .017), triglycerides (OR = 1.006, 95% CI = 1.001-1.011, P = .023), HDL-C (OR = 0.9, 95% CI = 0.85-0.96, P = .003), hs-CRP (OR = 1.09, 95% CI = 1.01-1.16, P = .014), LVEF (OR = 0.92, 95% CI = 0.86-0.98, P = .017), and endocan (OR = 1.004, 95% CI = 1.001-1.007, P = .021). In the multivariate analysis, male gender (OR = 3.9, 95% CI = 1.2-13.0, P = .022), BMI (OR = 0.68, 95% CI = 0.53-0.88, P = .003), HDL-C (OR = 0.862, 95% CI = 0.78-0.94, P = .001), and LVEF (OR = 0.86, 95% CI = 0.77-0.95, P = .006) were found to be independent predictors of presence of obstructive CAD. Endocan, similar to the hypertensive subgroup results, was still an independent predictor of presence of obstructive CAD in normotensives (OR = 1.005, 95% CI = 1.001-1.010, P = .024).
Univariate correlation analysis revealed a positive correlation between plasma levels of endocan and CAD severity scores (for SYNTAX: r = .402, P < .001; for Gensini: r = .403, P < .001; Figure 2A and B). After controlling for potential confounders, endocan had a positive independent association with SYNTAX score (β = 0.394, t = 4.075, P < .001). Additionally, multivariate linear regression revealed that the Gensini score was also correlated with endocan levels (β = 0.289, t = 2.98, P = .004). In subgroup analysis, both in the hypertensive (Figure 2C and D) and normotensive (Figure 2E and F) subgroups, endocan levels displayed significant positive correlation with CAD severity scores. In patients with HT, the correlation coefficient for SYNTAX score was 0.441 (P < .001) and for the Gensini score 0.450 (P < .001). In the normotensive subgroup, endocan levels correlated with the SYNTAX score (r = .385, P = .006) and with the Gensini score (r = .359, P = .011), similar to the hypertensive group. After controlling for the potential confounders, we showed that endocan was in an independent positive correlation with SYNTAX score both in the hypertensive subgroup (β = 0.414, t = 3.21, P = .002) and in the normotensive subgroup (β = 0.301 t = 2.23, P = .031). The results of the multivariate linear regression analysis confirmed that the correlation between the Gensini score and endocan was maintained only in the hypertensive subgroup (β = 0.301, t = 2.29, P = .026).
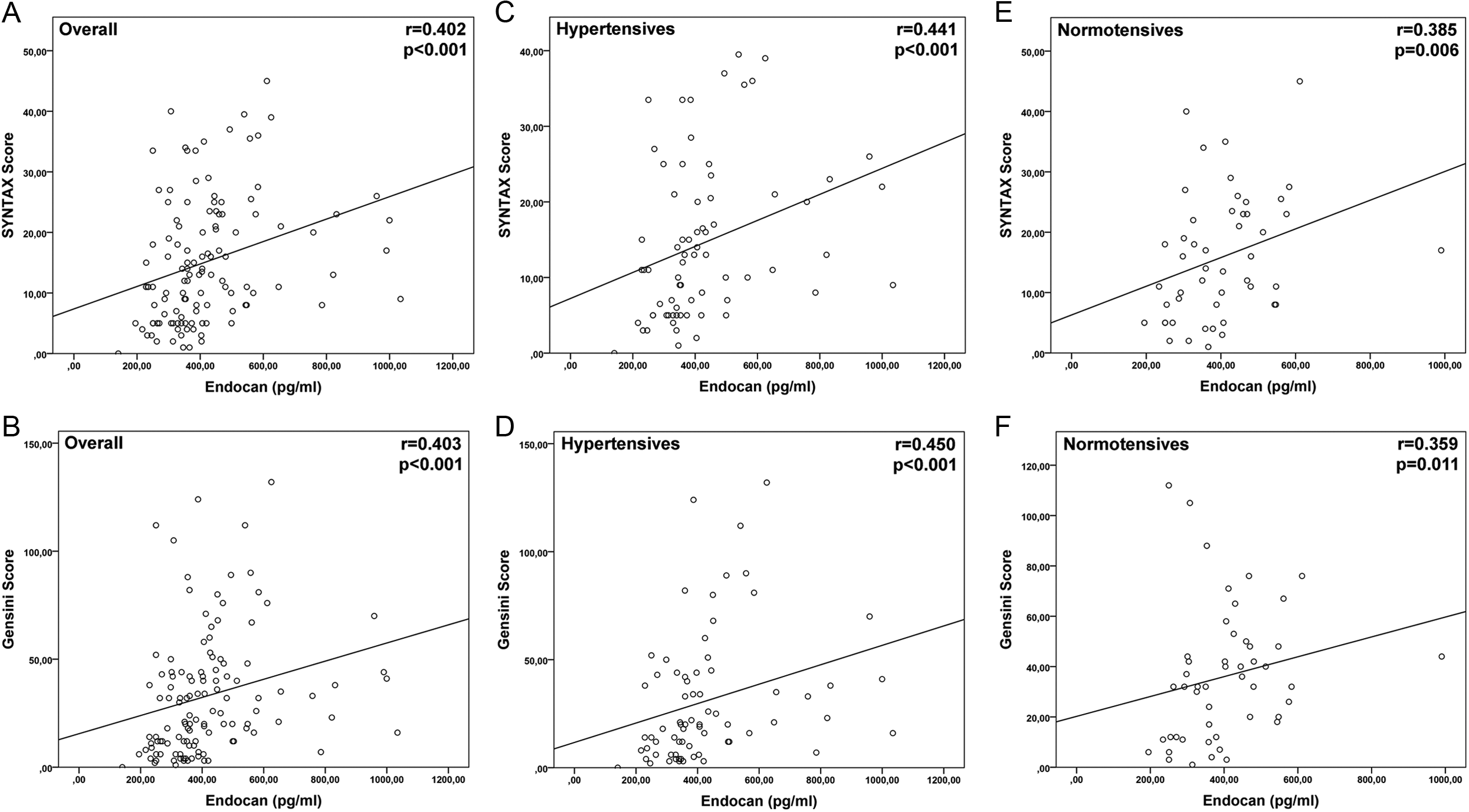
Relationship between serum endocan levels and the coronary artery disease severity scores in all patients (A and B), hypertensives (C and D), and normotensives (E and F).
Discussion
In this study, for the first time it is shown that endocan is an independent predictor of the presence and severity of CAD irrespective of HT presence. Besides this, we showed that the plasma endocan levels are also significantly high in the MVA patients similar to the patients with obstructive CAD.
Endocan may be interpreted as a marker of endothelial activation. Its interaction with the LFA-1 decreases the interaction of leukocytes with the endothelium and thus it can have a protective effect. 20 The levels of tumor necrosis factor α and interleukin 1β (IL-1β), which are increased by the endothelial activation, also increase the expression of endocan. 21 Proinflammatory cytokines affect endothelial function starting in the early phases of atherosclerosis. Tumor necrosis factor α and IL-1β show a proatherogenic effect because of their role in pathways like endothelial dysfunction, leukocyte recruitment, and vascular cell activation. 22 Cytokine levels in the circulation are also increased in patients with HT. 23 It is also shown that endocan levels are increasing concomitantly in hypertensives. 24 In any condition seen with the inflammation and endothelial activation, endocan may have a role. 25 –27 Coronary microvascular dysfunction is usually seen with MVA. 28 There are several studies reporting that MVA correlates with increased proinflammatory cytokines and hs-CRP. 29 –31 Even though the pathogenesis of MVA is uncertain, there are data showing that endothelial dysfunction plays an important role in the etiology. 32 In patients with MVA, the presence of the higher carotid intima–media thickness and increased arterial stiffness and elastic modulus is reported. 33 This finding points that MVA is a precursor of atherosclerotic CV disease. Besides this, the rate of the CV events is increased in this patient group. 34 Regarding the results of the present study, the hs-CRP and endocan levels in the MVA patients are comparable with the levels in the patients with CAD. We believe that this finding may reflect endothelial activation and endothelial dysfunction in the MVA patients similar to the patients with obstructive CAD.
Previous studies reported that endocan may be an independent indicator of subclinical and overt atherosclerosis in patients with HT. 8,35 It is believed that endocan levels correlate with several risk factors besides HT. It is reported that the endocan levels are increased in diabetic patients with the proliferative retinopathy. 36 Moreover, there are some studies showing that endocan levels are increased in the diabetic patients and that it decreases with improved glycemic regulation. 37,38 Yılmaz et al reported that endocan was correlating with the survival and the fatal/nonfatal CV events in patients with chronic renal disease. 39 In our study, in addition to other studies, endocan levels predicted the presence of the CAD also in the nonhypertensive patients similar to the patients with HT. This finding may point to a correlation between endocan and the atherosclerotic lesion formation. Menon et al detected increased endocan expression in atherosclerotic plaques. 40 They hypothesized that endocan plays a role in atherosclerosis through the stimulation of the smooth muscle cell proliferation and migration. In the present study, the independent predictability of the burden and the severity of the CAD by endocan levels is an additional important finding. Even if there is only a moderate correlation, we assume that endocan can be useful in the quantification of vascular inflammation and endothelial activation. Previous studies have shown that the regulation of HT and diabetes leads to a decrease in endocan levels. 24,37 These findings provide some clues about the dynamic character of endocan blood levels. In our study, the presence of increased hs-CRP levels in the patients with suspected endothelial activation concomitant to the increased endocan levels provides hope for a prognostic role of endocan in the future.
Endocan is a candidate to become a reliable indicator of endothelial dysfunction developing before the presentation of the apparent CV diseases. Therefore, this molecule has the potential to shape the therapies regarding the primary prevention of the CV diseases. Further studies are needed to confirm this concept.
The main limitation of our study is the small sample size. Control groups with greater number of participants may produce more reliable and significant results. Thus, our study may be considered as a pilot study. The compulsory nonexclusion of the other confounders, which may influence endocan levels, is another limitation of our study. The quantification of endothelial dysfunction levels may provide additional information. Besides this, we note that the absence of the microcirculation function tests and ergonovine administration in the diagnosis of MVA is another limitation of our study.
In conclusion, we observed that the circulating endocan levels in MVA patients were higher than for the control group and comparable with patients having obstructive CAD. Besides this, the endocan levels in the nonhypertensive patients—similarly to the patients with HT—displayed an independent correlation with the presence and severity of the obstructive CAD. These findings suggests that endocan could be a common predictor of the endothelium-dependent inflammatory processes, rather than related to specific risk factors. Finally, future studies are necessary to explore whether the endocan is a useful marker for identifying the patients at high risk of CV disease.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.