
Abstract
In the present study, we aimed to evaluate temporal changes in heart-type fatty acid-binding protein (h-FABP) and myocardial performance index (Tei index) following administration of 5-fluorouracil (5-FU), a chemotherapeutic agent associated with myocardial ischemia induced by coronary vasospasm. Thirty-two patients with cancer receiving their first 5-FU-based chemotherapy were included in the study. Prior to chemotherapy and 24 hours after the initiation of chemotherapy, all patients underwent a comprehensive echocardiographic examination. Blood samples were taken for h-FABP and troponin I (TnI) measurements at different time points during the first 24 hours of 5-FU administration. Postinfusion echocardiography revealed worsening in Tei index (0.37 ± 0.08 vs 0.43 ± 0.07, P < .001). Clinically overt cardiotoxicity was evident in 4 (12.5%) of our patient population. Heart-type fatty acid binding protein and TnI levels were within normal ranges at all time points. Our results suggest that ischemia coronary vasospasm due to 5-FU cardiotoxicity should be reviewed. Furthermore, Tei index might be a sensitive indicator of occult 5-FU cardiotoxicity.
Introduction
5-Fluorouracil (5-FU) is a chemotherapeutic agent used in the treatment of various cancers. Cardiotoxicity induced by 5-FU is a serious side effect leading to myocardial ischemia, arrhythmia, or cardiomyopathy, which presents with various symptoms such as angina pectoris, hypotension, dyspnea, or sudden death. 1 5-Fluorouracil cardiotoxicity is the second most common cause of chemotherapy-induced cardiotoxicity, and the reported incidence ranges from 1.2% to 18%. 2 The exact mechanism of 5-FU cardiotoxicity is still an unresolved issue. Numerous mechanisms have been proposed in the pathophysiology of 5-FU cardiotoxicity. However, coronary vasospasm similar to that in Prinzmetal angina causing myocardial ischemia is the most commonly suspected mechanism. 3
Early detection of cardiotoxicity is very important to reduce the risk of cardiac sequelae in cancer survivors. 4 Myocardial performance index (MPI) also known as Tei index was defined as a Doppler index that can evaluate left ventricular (LV) systolic and diastolic functions together. 5 It can also detect subtle changes in cardiac function. Although it has been proposed as a sensitive indicator of anthracycline-induced cardiotoxicity in various studies, there are limited data regarding 5-FU-induced cardiotoxicity. 6,7 Moreover, few data are available on predictive biochemical markers of cardiac side effects of 5-FU. 8,9 Heart-type fatty acid-binding protein (h-FABP) is a small unbound cytoplasmic protein that is present in high concentration in myocardial cells and released into the circulation within minutes of ischemia. 10,11 Considering myocardial ischemia induced by coronary vasospasm as the main mechanism of 5-FU cardiotoxicity, we aimed to evaluate temporal changes in h-FABP and MPI (Tei index) following administration of 5-FU.
Methods
Study Population
Thirty-two patients receiving their first 5-FU-based chemotherapy at the Department of Oncology, Trabzon Numune Training and Research Hospital, were prospectively enrolled into this study. Patients with known or suspected coronary artery disease, hemodynamically significant valvular heart disease, and/or atrial fibrillation based on clinical history and previous laboratory examinations were excluded. Left ventricular ejection fraction (LVEF) <50% at baseline, serum creatinine > 1.5 mg/dL, and concomitant use of other chemotherapeutic agents that might induce cardiotoxicity such as anthracyclines, trastuzumab, cisplatin, and cyclophosphamide were other exclusion criteria. Diagnosis of hypertension was made if the patient was on an antihypertensive medication or if the blood pressure was >140 mm Hg systolic, >90 mm Hg diastolic, or both. Diabetes mellitus was defined as fasting plasma glucose levels > 126 mg/dL on multiple measurements or current use of antidiabetic medication. Hypercholesterolemia was defined as total cholesterol > 200 mg/dL. All patients gave their written informed consent for participation. The study conformed to the principles outlined in the Declaration of Helsinki and was approved by local ethics committee.
Prior to chemotherapy, all patients underwent a comprehensive echocardiographic examination. Echocardiographic examination was repeated 24 hours after the initiation of chemotherapy. Baseline electrocardiogram (ECG) and ECG following completion of drug administration were collected. Blood samples were taken for h-FABP measurements at 3 time points: before chemotherapy (T0) as well as at 6 hours (T1) and 12 hours (T2) after chemotherapy initiation. Likewise, blood samples were collected for troponin I (TnI) measurements before chemotherapy (T0) and at 24 hours (T3) after chemotherapy initiation (Figure 1).
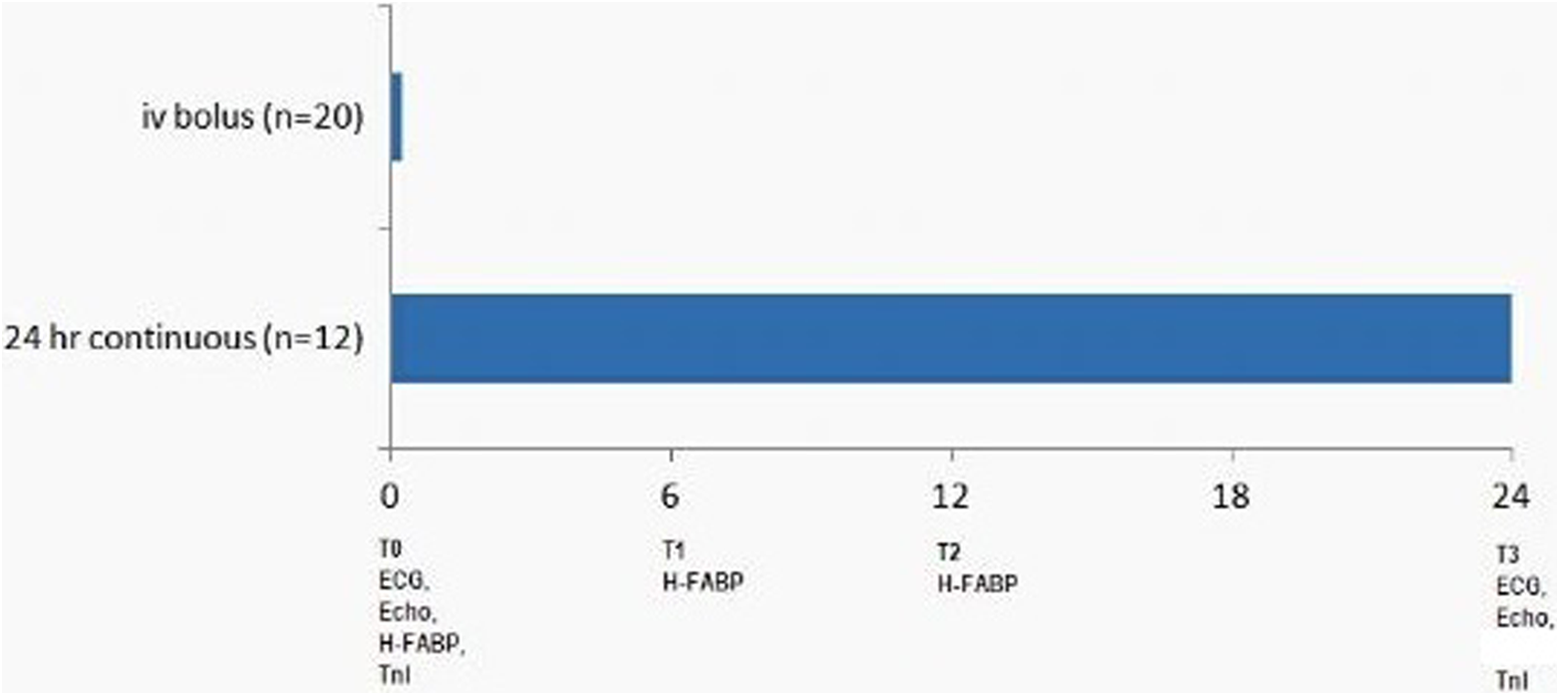
Study protocol. ECG indicates electrocardiogram; ECHO, echocardiography; 5-FU, 5-fluorouracil; h-FABP, heart-type fatty acid-binding protein; TnI, troponin I.
Echocardiographic Evaluation
Echocardiographic examination was performed with a commercially available cardiovascular ultrasound system (Vivid 3; GE Vingmed, Horten, Norway). Data acquisition was performed with a 1.5 to 2.6 MHz transducer in the parasternal and apical views (standard 2- and 4-chamber views). Two-dimensional and Doppler images were obtained during breath hold and stored in cine-loop format from 3 consecutive beats, and average values were reported and ECGs were simultaneously recorded. Left ventricular ejection fraction was derived by the apical biplane modified Simpson rule. Fractional shortening (FS) was calculated by dividing the difference between LV end-diastolic and end-systolic dimensions to LV end-diastolic dimension. Doppler measurements included peak early mitral filling velocity (E wave), peak late mitral filling velocity (A wave), and ratio of peak early and late mitral filling velocities (E/A). For myocardial tissue velocities, tissue Doppler imaging (TDI) sample volume was placed at the lateral mitral annulus, at the junction between the LV lateral wall and the mitral annulus, in apical 4-chamber view. For each circulatory situation, the duration was measured from the peak of the R wave of the ECG to the onset of the late diastolic A wave of the next cardiac cycle. The sum of isovolumetric contraction time (IVCT) and isovolumetric relaxation time (IVRT) was measured as the interval from the cessation to the onset of the mitral inflow. Tissue Doppler imaging included following parameters: early diastolic myocardial velocity (Em), late diastolic myocardial velocity (Am), systolic myocardial velocity (Sm), Em/Am, IVRT, IVCT, and ejection time (ET). Tei index was calculated by dividing the sum of isovolumic times to ET ([IVRT + IVCT]/ET). All echocardiograms were interpreted by 2 experienced cardiologists (M.T.A. and A.C.A.) who were blinded to patient chemotherapy status.
Biochemical Analysis
Blood samples were centrifuged at 2500 rpm for 20 minutes at 4°C and the sera frozen at −80°C until assayed. Heart-type fatty acid-binding protein was measured by quantitative enzyme-linked immunosorbent assay (BioCheck, Inc, Foster City, California). Normal range was 1.6 to 19 ng/mL. A value >19 ng/mL was considered to indicate myocardial injury. Troponin I was measured by a 2-site immunoenzymatic (sandwich) immunoassay (Access immunoassay; Beckman Coulter, Inc, Chaska, Minnesota). Normal range was 0.0 to 0.1 ng/mL.
Statistical Analysis
Data are expressed as means ± standard deviation for normally distributed continuous variables, as median for skew-distributed continuous variables, and as frequencies for categorical variables. Paired statistical comparisons were made using the paired samples t test and Wilcoxon signed rank test where appropriate. Categorical variables were compared using the χ2 test. The intraobserver and interobserver variabilities were assessed from echocardiographic data that were obtained in a subgroup of 11 patients. A 2-tailed P < .05 was considered significant. SPSS for Windows version 15.0 statistical package was used (SPSS Inc, Chicago, Illinois).
Results
The study population consisted of 22 male and 10 female patients (mean age: 57 ± 14 years). Diagnoses were colorectal adenocarcinoma (n = 22), gastric (n = 8), pancreatic (n = 1), and head and neck cancer (n = 1). Twenty patients received a 15-minute intravenous (IV) bolus infusion, whereas the remaining 12 patients received a 24-hour continuous IV infusion. The dose of 5-FU ranged between 425 and 1600 mg/m2/24 h. Baseline echocardiography was compared with the echocardiography at 24 hours. Although both values remained within normal ranges, a significant reduction in LV systolic function indices was observed. Left ventricular ejection fraction was reduced from 59% ± 6% to 57% ± 5% (P = .004). Fractional shortening was reduced from 32% ± 4% to 30% ± 3% following 5-FU administration (P = .003). There were no significant changes with regard to E, A, E–A ratio, ET, Em, and Am following 5-FU administration. However, there were significant prolongations in IVCT and IVRT (Figure 2). Tei index was significantly increased (0.37 ± 0.08 vs 0.43 ± 0.07, P < .001), whereas Em–Am ratio was significantly decreased following 5-FU administration (Tables 1 and 2; Figure 3). Furthermore, in 6 (18.7%) patients, various degrees of diastolic dysfunction were observed: stage 1 diastolic dysfunction was determined in 2 (33.3%) patients with no pretreatment diastolic dysfunction; stage 2 diastolic dysfunction was determined in 2 (33.3%) patients with no pretreatment diastolic dysfunction; and stage 2 diastolic dysfunction was determined in 2 (33.3%) patients with pretreatment stage 1 diastolic dysfunction. Three (50%) of the 6 patients who had diastolic dysfunction received infusion and the other 3 (50%) received bolus 5-FU treatment.
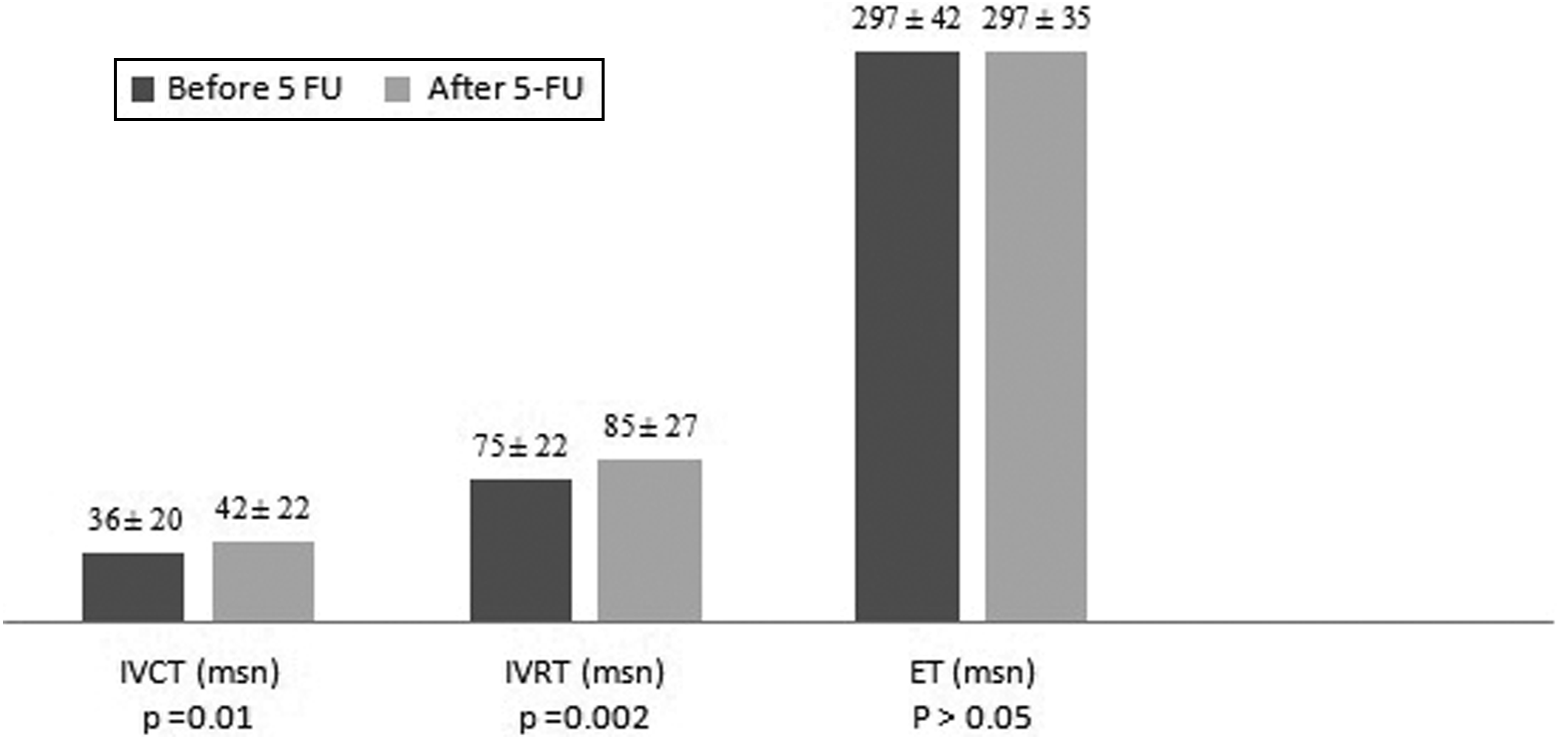
Temporal changes in tissue Doppler parameters following 5-FU administration. ET indicates ejection time; 5-FU, 5-fluorouracil; IVCT, isovolumic contraction time; IVRT, isovolumic relaxation time.
Changes in Conventional and Tissue Doppler Echocardiographic Parameters Following 5-FU Administration in Study Population.
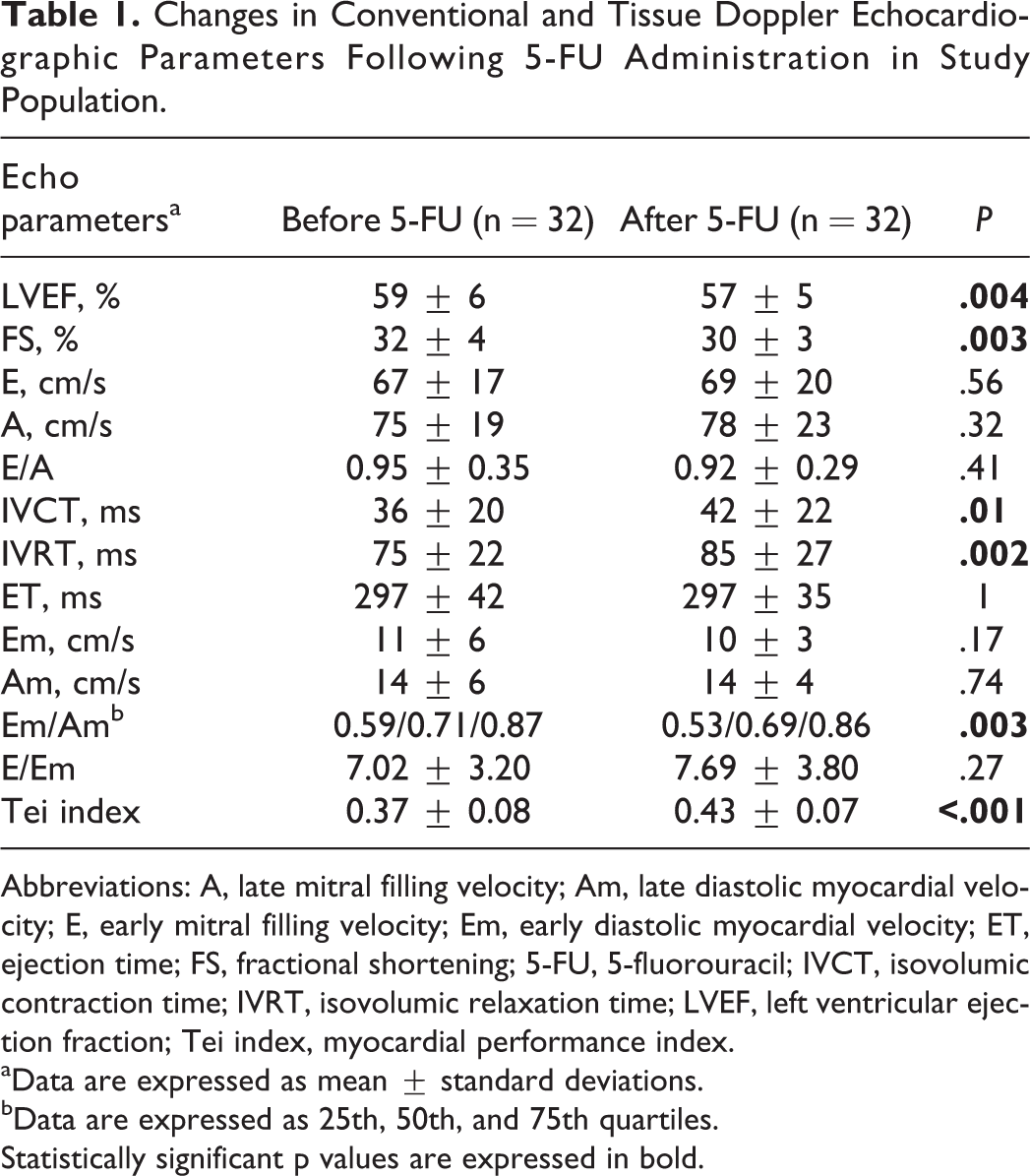
Abbreviations: A, late mitral filling velocity; Am, late diastolic myocardial velocity; E, early mitral filling velocity; Em, early diastolic myocardial velocity; ET, ejection time; FS, fractional shortening; 5-FU, 5-fluorouracil; IVCT, isovolumic contraction time; IVRT, isovolumic relaxation time; LVEF, left ventricular ejection fraction; Tei index, myocardial performance index.
aData are expressed as mean ± standard deviations.
bData are expressed as 25th, 50th, and 75th quartiles.
Statistically significant p values are expressed in bold.
Changes in Conventional and Tissue Doppler Echocardiographic Parameters Following 5-Fu Administration in Asymptomatic and Symptomatic Patients.
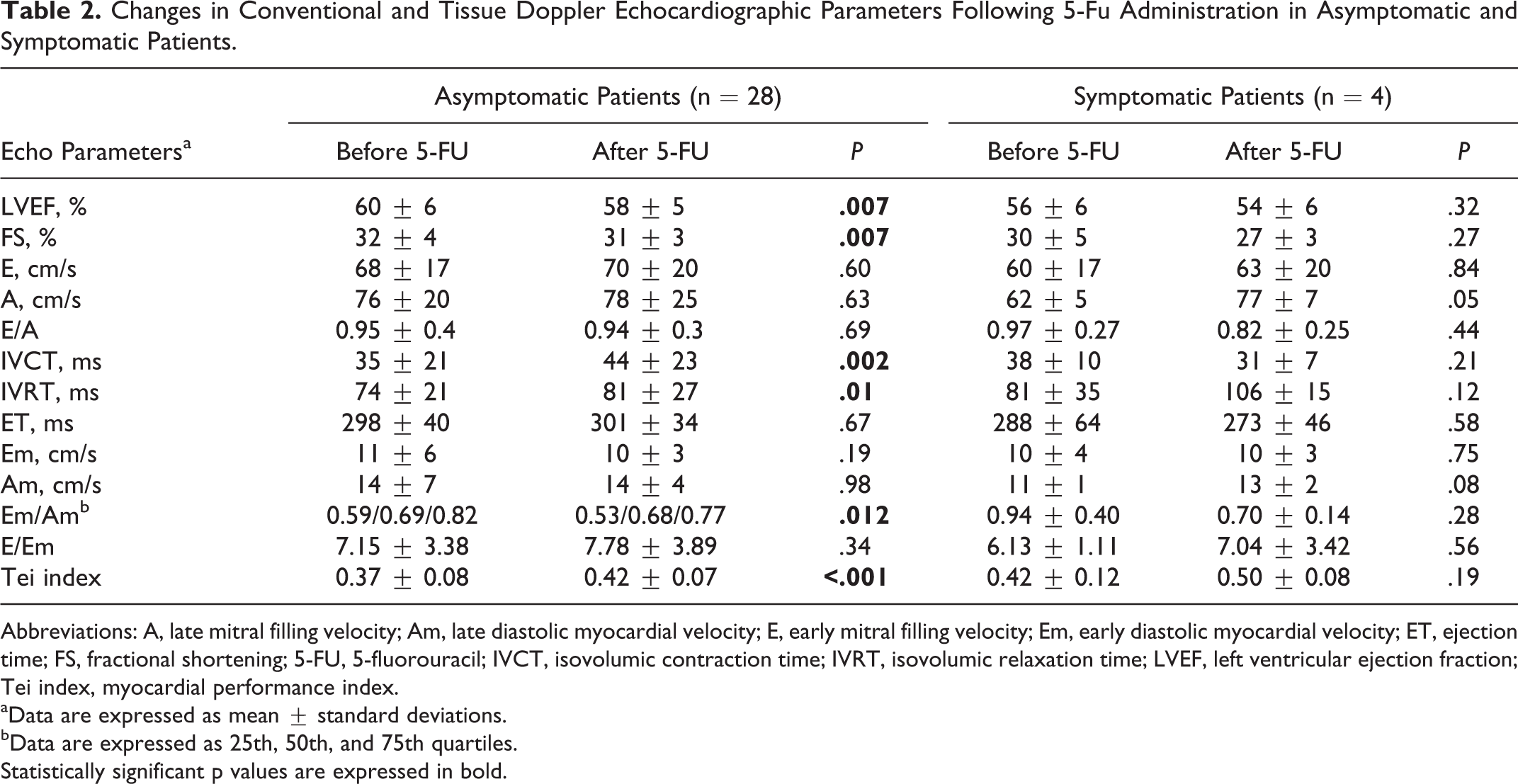
Abbreviations: A, late mitral filling velocity; Am, late diastolic myocardial velocity; E, early mitral filling velocity; Em, early diastolic myocardial velocity; ET, ejection time; FS, fractional shortening; 5-FU, 5-fluorouracil; IVCT, isovolumic contraction time; IVRT, isovolumic relaxation time; LVEF, left ventricular ejection fraction; Tei index, myocardial performance index.
aData are expressed as mean ± standard deviations.
bData are expressed as 25th, 50th, and 75th quartiles.
Statistically significant p values are expressed in bold.
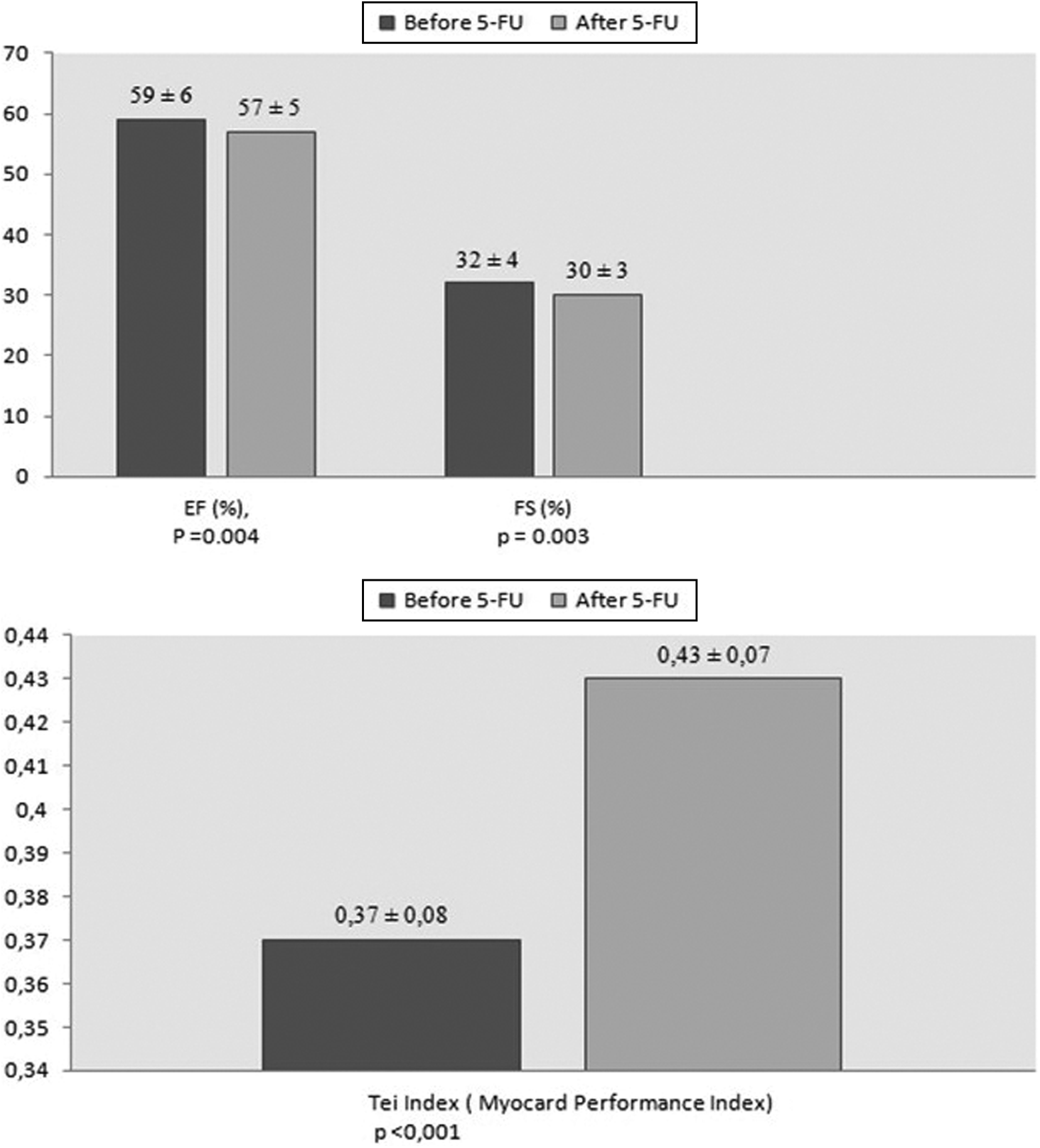
Changes in echocardiographic left ventricular systolic function indices following 5-FU administration. EF indicates ejection fraction; FS, fractional shortening; 5-FU, 5-fluorouracil.
Clinically overt cardiotoxicity was evident in 4 (12.5%) of our patient population. This patient group is defined as the symptomatic group. The remaining 28 patients constituted the asymptomatic group. In the symptomatic group, 3 (9.4%) patients complained of angina and two of them (6.25%) showed ECG change (1-mm ST-segment depression and biphasic T wave). In 1 patient, asymptomatic 1-mm ST-segment depression was observed. Two (67%) of the 3 patients who developed symptoms had received 1000 mg/m2 infusion therapy, whereas the other (33%) patient had received 620 mg/m2 bolus therapy. The symptoms and the ECG changes were developed during the first hours of infusion therapy in patients who received infusion therapy, and the symptoms and ECG changes occurred just a minute after the bolus administration of 5-FU.
Analyses of our data in 2 separate symptom group are presented in Table 2. Although the similar alteration trends were observed in symptomatic patients, they did not reach statistical significance due to the small number of symptomatic patients. Diastolic dysfunction was observed in 3 (75%) of the 4 patients with clinically overt cardiotoxicity but only in 3 (10.7%) of the 28 patients in the asymptomatic group.
The intraobserver and interobserver variabilities were assessed from echocardiographic data that were obtained in a subgroup of 11 patients. The intraobserver and interobserver variabilities for the measurement of LVEF were 6.5% and 8.2%, for Tei index 6.1% and 7.4%, for IVRT 6.9% and 7.3%, and for IVCT 7.9% and 5.6%. Biochemical markers collected at different time points were compared accordingly. Heart-type fatty acid-binding protein levels were within normal ranges at all time points, and no significant difference was observed in paired comparisons at any time points. Likewise, no significant increment was noted in TnI levels following 5-FU administration (Table 3).
Temporal Changes in TnI and h-FABP Levels Following 5-FU Administration.
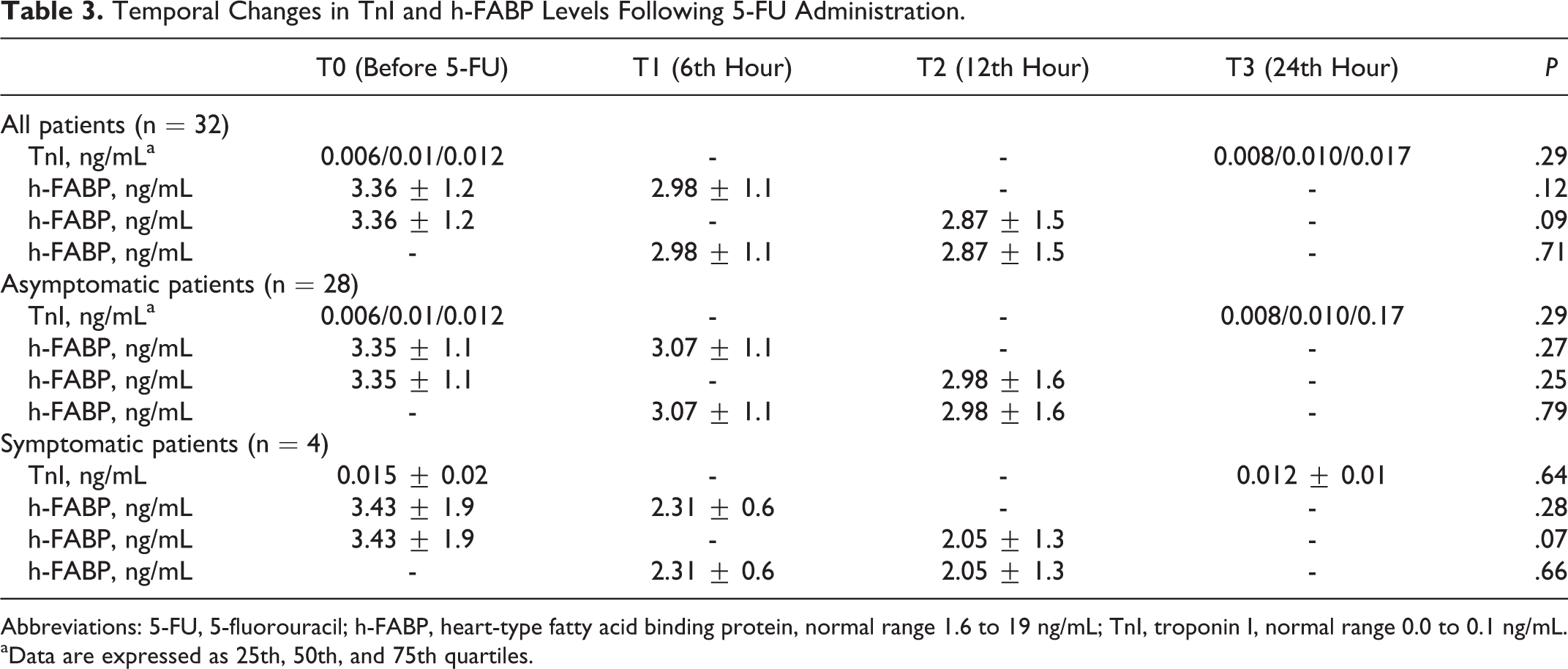
Abbreviations: 5-FU, 5-fluorouracil; h-FABP, heart-type fatty acid binding protein, normal range 1.6 to 19 ng/mL; TnI, troponin I, normal range 0.0 to 0.1 ng/mL.
aData are expressed as 25th, 50th, and 75th quartiles.
Discussion
In the present study, we failed to show any significant alteration in h-FABP and TnI levels at different time points in any of the patients including the patients who developed clinical signs and symptoms of 5-FU cardiotoxicity. However, postinfusion echocardiography revealed worsening in Tei index, significant deterioration in LVEF, and some degrees of diastolic dysfunction.
Echocardiography is the main imaging technique for the detection of chemotherapy-induced cardiotoxicity. Among the echocardiographic techniques, TDI appears to offer important advantages over traditional techniques in revealing the presence of early signs of cardiotoxicity. 12 Likewise, the Tei index may provide a valuable tool for early detection of chemotherapy-induced cardiotoxicity. In another study, 6 the Tei index was found to be increased in the majority of patients (78.8%) who received anthracycline chemotherapy indicating that myocardial alteration is more common than previously recognized. In another study, Senju et al 7 studied the Tei index in patients with hematologic malignancies. They reported that the echocardiographic Tei index reflects early myocardial damage induced by anthracyclines. Similar to these studies, the Tei index was significantly increased after 5-FU chemotherapy compared with pretherapy values in our patients.
Although the exact mechanism of 5-FU cardiotoxicity is not yet completely understood, the most emphasized scenario is vascular spasm caused by the drug or metabolites (fluoro-beta-alanine, fluoroacetate). 3 In an in vitro model, 5-FU was shown to cause vasoconstriction in smooth muscle rings that can be reversed with nitrates. 13
Evaluation of cardiac-specific biomarkers represents an alternative diagnostic tool for early detection of chemotherapeutic drug-induced cardiotoxicity. However, the role of cardiac troponins, for the early detection of cardiotoxicity due to nonanthracycline agents such as 5-FU, is quite obscure. Oztop et al 8 and the present study have failed to show any significant change in TnI following 5-FU administration. Another potential biomarker of cardiotoxicity that currently attracted attention is h-FABP. Due to its small size, h-FABP rapidly diffuses through the interstitial space and appears in the circulation as early as 90 minutes after myocardial ischemic damage. 10,11 Owing to its rapid release in response to ischemia, the present study evaluated its role in detecting 5-FU-induced cardiotoxicity. However, similar to our findings on TnI, we failed to show any significant alteration in serum h-FABP level during the course of 5-FU administration. Although coronary vasospasm causing myocardial ischemia is the most commonly suspected mechanism of 5-FU-induced cardiotoxicity, there is no evidence that calcium channel blockers or nitrates reduce the risk. 14,15 In addition, although vasoconstriction is observed immediately after 5-FU infusion, clinically overt cardiotoxicity often presents at the end of infusion or hours later. 16 Therefore, it remains to be elucidated in which circumstances 5-FU-induced vasoconstriction leads to clinical signs of cardiotoxicity. 17 The studies performed by Grandi et al 18 and Arellano et al 19 showed that some active 5-FU metabolites may alter myocardial energy metabolism and cause diffuse cellular hypoxia similar to ischemic heart disease. They suggested that these conditions could cause change in myocyte structure (mitochondria, nucleic acid metabolism, structural proteins, and ion channels) and lead to myocardial dysfunction without necrosis, a condition similar to postischemic myocardial stunning. Similar to these data, our results also suggest that the side effect mechanisms other than ischemia may be at the forefront in 5-FU-related cardiotoxicity.
Our study has some limitations. The sample size is the major limitation. Due to the small scale of our study population, the power of multivariate analysis was not adequate. Therefore, we did not perform multivariate analyses to determine independent predictors. Our study has a cross-sectional design that limits interpretation concerning the long-term effect or delayed cardiotoxicity due to 5-FU. Since it was not available in our hospital, we did not use a high-sensitivity TnI assay. Use of a more sensitive assay may detect subtle changes in TnI. Finally, more comprehensive echocardiography techniques were not used due to lack of available hardware.
According to these findings, the most emphasized thesis of coronary spasm as 5-FU cardiotoxicity mechanism must be reviewed. In addition, MPI might be a sensitive indicator of occult 5-FU cardiotoxicity.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.