
Abstract
Many recent studies have suggested that psoriasis, a chronic, inflammatory, immune-mediated skin disease, is associated with increased risk of cardiovascular disease (CVD). We aimed to compare arterial stiffness in psoriasis and control patient groups using the cardio-ankle vascular index (CAVI) and to determine whether psoriasis is an independent risk factor for CVD. A total 103 patients with psoriasis and 103 age- and sex-matched controls were enrolled. Compared with controls, the patients showed a higher CAVI (P = .03), particularly patients older than 40 years. The duration of psoriasis exhibited a positive correlative tendency with CAVI (P = .066). Moreover, psoriasis is an independent predictor of arterial stiffness after adjusting for other factors (P = .011). We suggest that psoriasis can be a risk factor for CVD, and older patients with psoriasis of longer disease duration should be monitored carefully for cardiovascular risk.
Introduction
Psoriasis is a chronic, immune-mediated, inflammatory skin disease that affects 1% to 3% of the general population. 1 Psoriasis is considered a “systemic immune-mediated inflammatory disease” rather than simply a “skin disease”. 2,3 T-helper 1 and T-helper 17 cells play an important role in the pathogenesis of psoriasis, contributing to its understanding as a systemic inflammatory disease. 4,5 Previous studies suggested that psoriasis is an independent risk factor for cardiovascular disease (CVD) due to the nature of systemic inflammation, which can induce atherosclerosis. 6,7 Atherosclerosis is commonly assessed by measuring arterial stiffness, and arterial stiffness has been identified as an independent prognostic factor for patients with CVD. 8,9
There are various methods for the measurement of arterial stiffness. Although carotid–femoral pulse wave velocity (cfPWV) is generally recognized as the gold standard, in the present study, we used the cardio-ankle vascular index (CAVI) to overcome the blood pressure (BP) dependency of cfPWV. 10,11 The CAVI is a novel, BP-independent parameter that reflects overall wall stiffness of the aorta, femoral artery, and tibial artery. 12 It has been used to assess potential risk of CVD in a variety of specific patient populations and in the general population. 10 –13 Additionally, in our patient group with psoriasis, we measured the central augmentation index (cAIx), which is derived from the arterial wave reflection demonstrating central aortic pressure. 14
In Western countries, large-scale studies showed that psoriasis is an independent risk factor for CVD. 15,16 Generally, Asians are less obese than Western people and have a different cardiovascular risk factor profile. The aim of this study was to determine whether psoriasis is also an independent risk factor for CVD in an Asian population.
We evaluated arterial stiffness by measuring CAVI in Korean patients with psoriasis and in a healthy control group; cAIx was also measured in the patients with psoriasis. We compared the differences between the 2 groups and correlated the results with the clinical characteristics of the patients.
Materials and Methods
Study Population
A total 103 patients with psoriasis and 103 age- and sex-matched healthy controls were enrolled. Exclusion criteria included a history of diabetes, hypertension, renal failure, CVD, or cerebrovascular disease and the use of lipid-lowering or antihypertensive medications. The diagnosis of psoriasis was based on clinical or histopathological examination. Disease severity was evaluated using the Psoriasis Area and Severity Index (PASI), and disease duration was documented in the patient group. Blood pressure, heart rate (HR), body mass index (BMI), and smoking history were recorded in both groups.
This study was conducted in accordance with the Declaration of Helsinki and Korean Good Clinical Practice, and approval from the institutional review board was obtained. All participants provided informed consent before screening.
Laboratory Measurements
Fasting plasma glucose, total cholesterol, triglyceride, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and C-reactive protein (CRP) levels were recorded. The CRP was measured by a latex agglutination method, using an automated analyzer (TBA 200FR; Toshiba, Japan). In all, 7 of the 103 patients with psoriasis were not fasting at blood sampling.
Cardio-Ankle Vascular Index
Cardio-Ankle Vascular Index (CAVI) was recorded using a VeSera VS-1000 device (Fukuda Denshi, Tokyo, Japan). In order to assess CAVI, pulse transmission time and distance from the origin of the aorta to the tibial artery at the ankle, through the femoral artery, are measured. Pulse wave velocity (PWV) is then calculated as PWV = pulse transmission time/distance between the origin of the aorta and the ankle. 17 Finally, CAVI values are calculated to detect vascular elasticity, using the following equation: CAVI = aβ + b, where a and b are scale conversion constants, and stiffness parameter β = [2ρ/(Ps − Pd)] × ln(Ps/Pd) × PWV2 (ρ: blood density, Ps: systolic BP in mm Hg, Pd: diastolic BP in mm Hg; Figure. 1). Increasing BP exponentially increases the reciprocal of the percentage change in the radius, which the logarithmic pulse pressure exponentially decreases. Thus, stiffness parameter β is independent of BP. 11,12 After 15 minutes of supine rest, a single experienced operator performed CAVI measurement. The mean CAVI was used as each patient’s score.
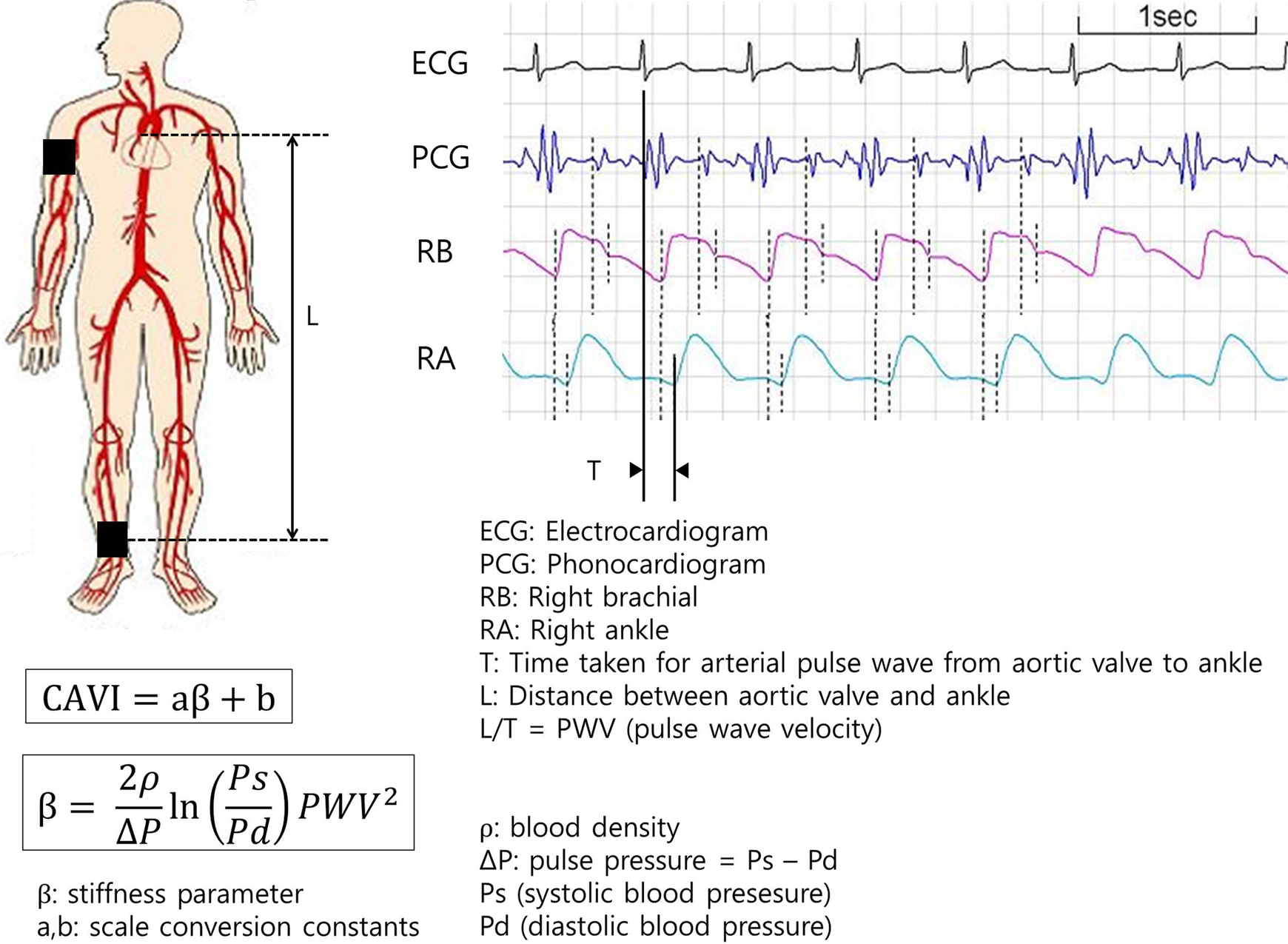
Schematic illustration of the acquisition of cardio-ankle vascular index (CAVI).
Central Augmentation Index
Blood pressure at the brachial artery (mean of 3 readings) was recorded using an automatic sphygmomanometer. For the assessment of Central Augmentation Index (cAIx), we used the commercially available SphygmoCor system (AtCor Medical, Sydney, Australia). Using a Millar applanation tonometer, the waveform of the radial artery at the wrist was recorded for 10 seconds of consistent waveform data. For quality control of the captured waveform, operator indices above 80 were included. The cAIx was derived from this via pulse wave analysis. 18 From the augmentation point (or the inflection point of the incident and reflected waves), augmentation pressure was calculated from the generated aortic pressure waveform. The cAIx was defined as the augmentation pressure divided by the pulse pressure. Owing to the influence of HR, an index normalized for a rate of 75 beats/min was used in this analysis. 19
Statistical Analysis
Analysis was performed using SPSS for Windows version 21.0 (SPSS, Chicago, Illinois). Descriptive statistics were used to describe demographics and anthropometric and laboratory measurements. Continuous data are expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]). The 2-sample t test, Mann-Whitney U test, and chi-square test were used for comparisons of the 2 groups. Pearson correlation analysis and simple and multiple linear regressions were used to evaluate the relationships between variables and arterial stiffness indexes, CAVI, and cAIx. For all statistical analyses, a P < .05 (2-tailed) was considered significant.
Results
Demographic Characteristics
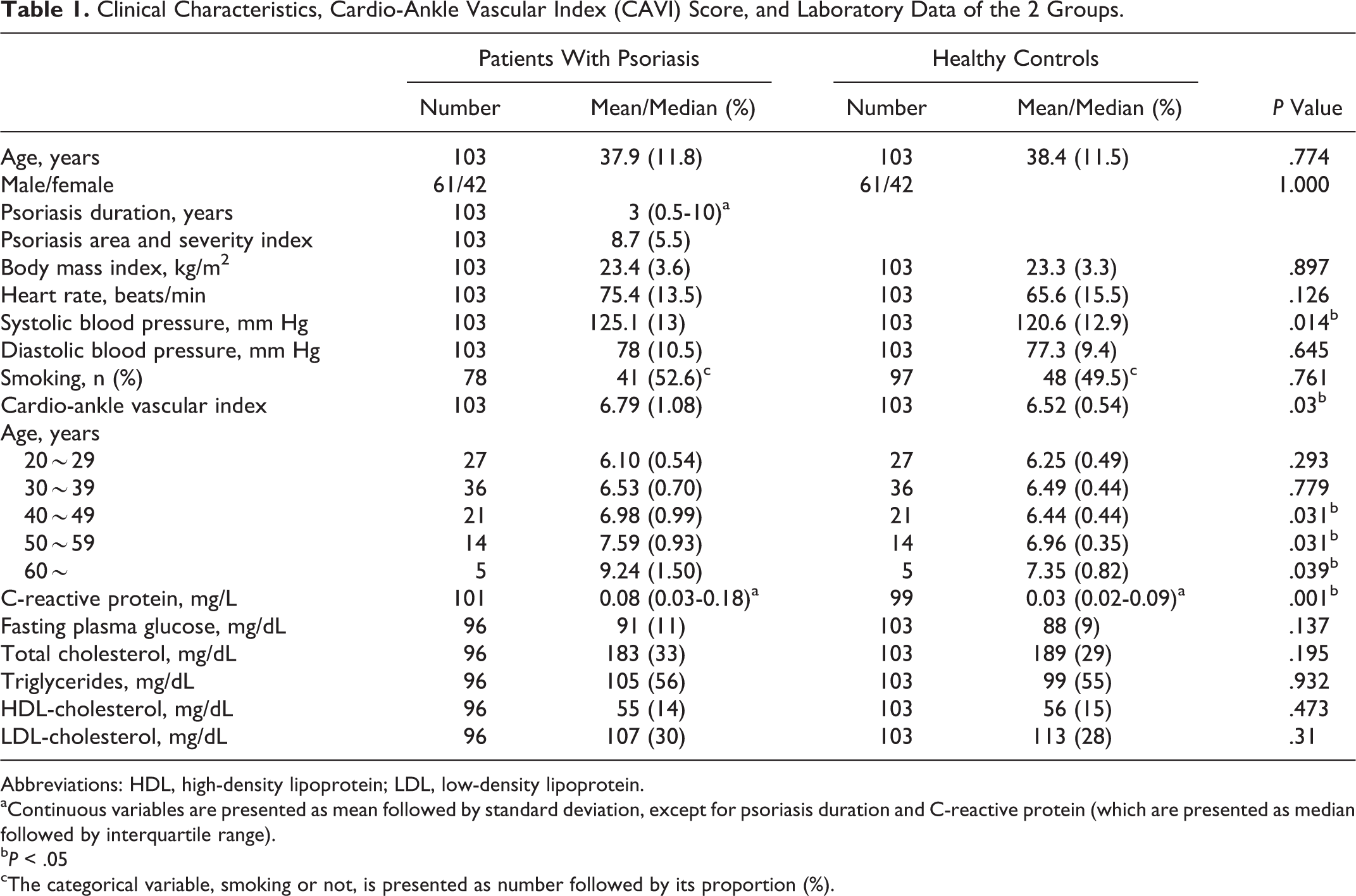
A total of 206 participants (103 patients and 103 controls) with an average age of 38.2 ± 11.6 years were included. The mean age did not differ significantly between the patient group with psoriasis (37.9 ± 11.8 years) and controls (38.4 ± 11.5 years; P = .77). Both groups were composed of 61 men and 42 women. Mean psoriasis duration was 3 years (IQR, 0.5-10 years), and mean PASI score was 8.7 ± 5.5 (Table 1).
Clinical Characteristics, Cardio-Ankle Vascular Index (CAVI) Score, and Laboratory Data of the 2 Groups.
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
aContinuous variables are presented as mean followed by standard deviation, except for psoriasis duration and C-reactive protein (which are presented as median followed by interquartile range).
bP < .05
cThe categorical variable, smoking or not, is presented as number followed by its proportion (%).
Cardio-Ankle Vascular Index
Mean CAVI was significantly higher in patients with psoriasis (6.79 ± 1.08) than in healthy controls (6.52 ± 0.54; P = .03), particularly in patients older than 40 years (Table 1). The CAVI tended to increase with age in both the groups. The differences in mean CAVI between the 2 groups also increased in patients older than 40 years. Differences were 0.54, 0.63, and 1.89 in the 41- to 50-year-old, 51- to 60-year-old, and older than 60-year-old age-groups, respectively. In all, 11 patients with psoriasis and only 1 control participant had a CAVI exceeding one standard deviation of the general population for that age group.
Traditional Cardiovascular Risk Factors and Laboratory Data
Mean systolic BP of the patients with psoriasis (125.1 ± 13 mm Hg) was higher than that of healthy controls (120.6 ± 12.9 mm Hg; P = .014). Other cardiovascular risk predictors, including diastolic BP, HR, BMI, smoking, fasting plasma glucose, total cholesterol, triglycerides, HDL cholesterol, and LDL cholesterol, were not significantly different between patients and controls (Table 1). The CRP was significantly increased in patients with psoriasis (0.08 mg/L; IQR, 0.03-0.18 mg/L) compared to controls (0.03 mg/L; IQR, 0.02-0.09 mg/L; P = .025; Table 1).
Correlations
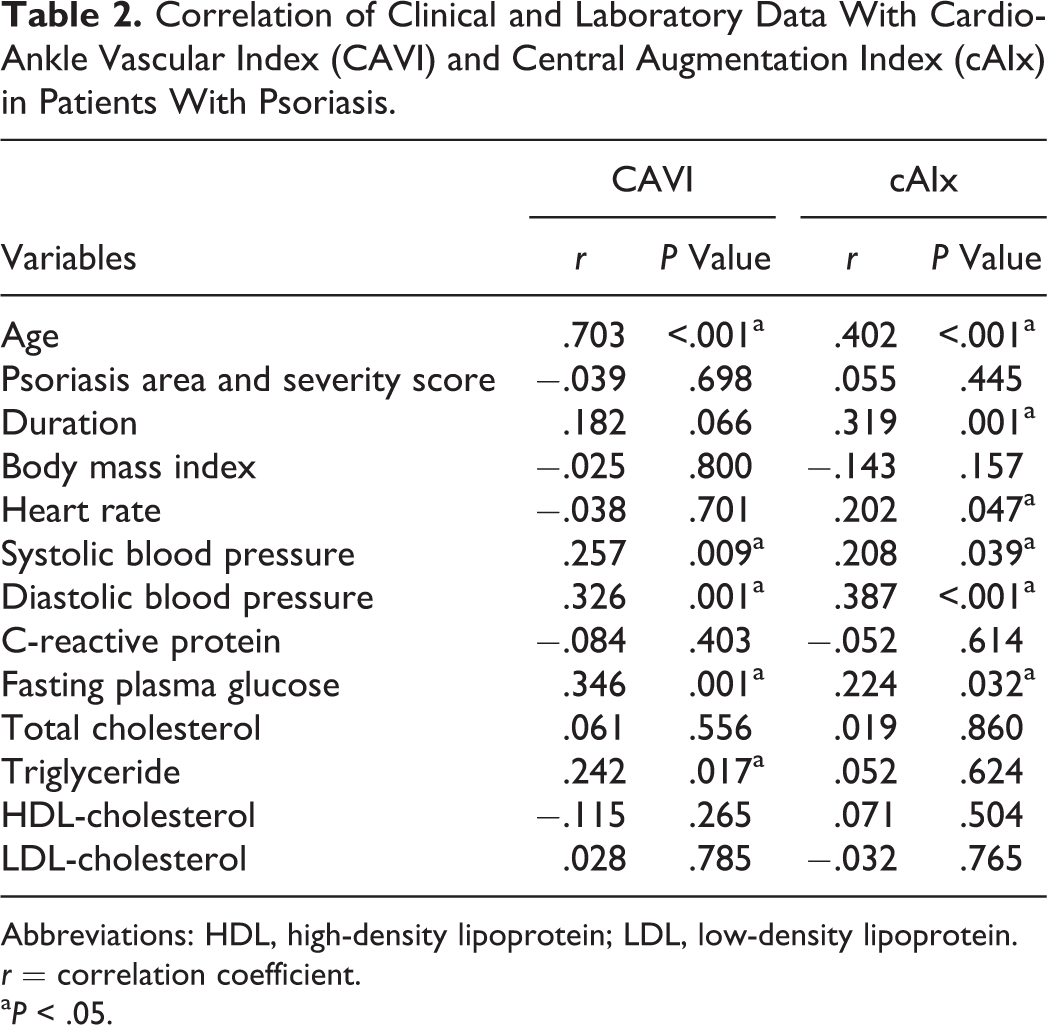
In patients with psoriasis, there was a strong positive correlation between both CAVI and cAIx versus age (r = .703, P < .001 and r = .402, P < .001, for CAVI and cAIx, respectively). Duration of psoriasis correlated significantly with cAIx (r = .319, P = .001). Psoriasis duration did not show a significant correlation with CAVI (r = .182, P = .066). Disease severity represented by PASI did not correlate with either CAVI or cAIx. Both systolic and diastolic BP and fasting plasma glucose showed a positive correlation with CAVI and cAIx. Heart rate positively correlated with cAIx (r = .202, P = .047), but considering the fact that BP is a confounding factor, the significance of this finding is uncertain. Triglycerides positively correlated with CAVI, but CRP, total cholesterol, HDL-cholesterol, and LDL-cholesterol showed no significant correlation (Table 2).
Correlation of Clinical and Laboratory Data With Cardio-Ankle Vascular Index (CAVI) and Central Augmentation Index (cAIx) in Patients With Psoriasis.
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
r = correlation coefficient.
aP < .05.
Multiple Linear Regression Analysis
Univariate and multivariate analyses were performed to determine independent predictors of arterial stiffness (Table 3). Psoriasis was an independent contributing factor to CAVI after adjusting for age and traditional cardiovascular risk factors (P = .011). Age (P < .001), BMI (P = .004), and triglycerides (P = .045) were also significant contributing factors to CAVI, but BMI had a negative coefficient of beta, −.179 (p = .004).
Multiple Linear Regression Analysis of Independent Predictors of Cardio-Ankle Vascular Index in Patients With Psoriasis and Controls.
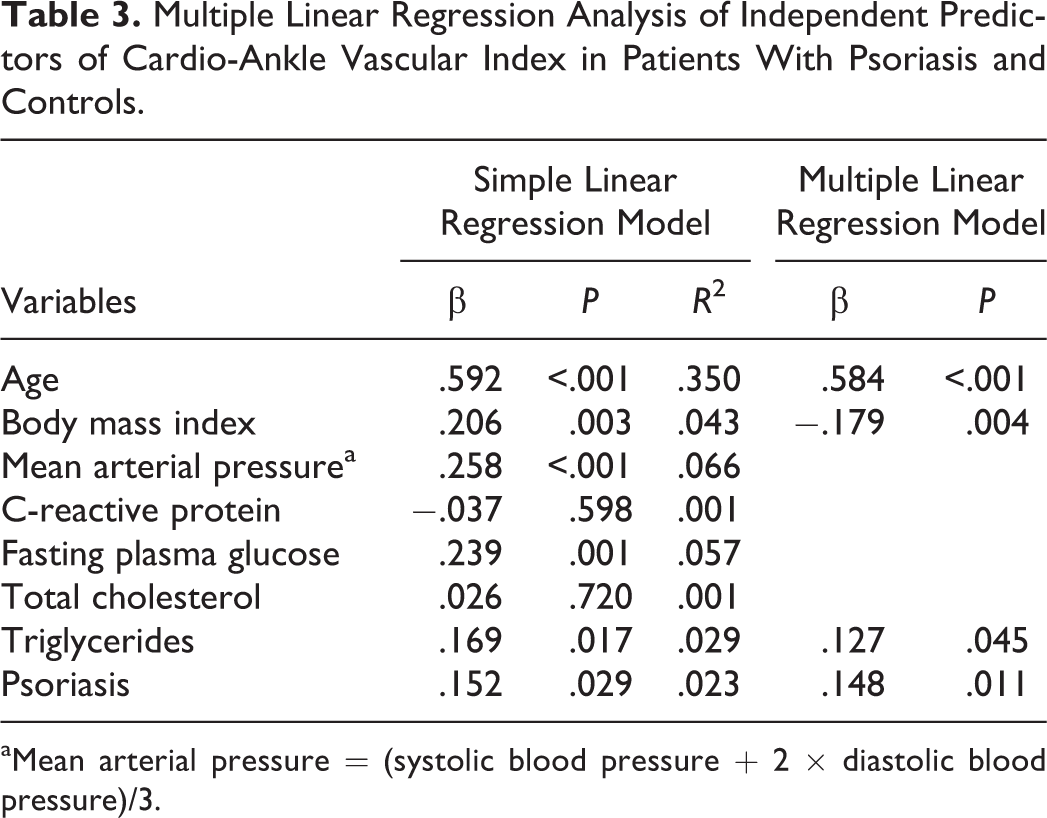
aMean arterial pressure = (systolic blood pressure + 2 × diastolic blood pressure)/3.
Discussion
Our findings suggest that psoriasis is a systemic inflammatory disease that is independently associated with arterial stiffness. The CRP levels and CAVI were significantly higher in patients with psoriasis than in age- and sex-matched controls, and CAVI was clearly higher in patients older than 40 years of age. The duration of psoriasis positively correlated with cAIx and showed a positive correlative tendency with CAVI. These findings suggest that psoriasis duration can affect arterial stiffness, and atherosclerosis caused by aging is more likely in patients with psoriasis than in healthy people.
The finding that CAVI showed a weaker correlation with disease duration than cAIx could suggest that CAVI is a less sensitive method and reflects arterial stiffness later than cAIx. McEniery et al 20 demonstrated that, in comparison with PWV, cAIx increased faster with aging and was more sensitive to decreased endothelial function. Because CAVI is a method based on PWV, AIx might represent a more sensitive technique for the measurement of arterial stiffness than CAVI. The cAIx reflects central BP and uses a tonometric sensor, which is more sensitive than the cuff sensor used in the CAVI method; this is a possible contributory factor to this finding.
Previous studies demonstrated that psoriasis is an independent risk factor for CVD, 15,16 and atherosclerotic change is obvious in patients with psoriasis. 21,22 Most of these investigations were conducted in Western populations, but some studies evaluated arterial stiffness in Asian patients with psoriasis. 22,23 In general, Asians are less obese than Westerners and have different cardiovascular profiles. Despite these differences, the present study shows that there is a significant increase in arterial stiffness, as measured by CAVI, in Korean patients with psoriasis.
Systemic inflammation can induce atherosclerosis, and the extent and duration of inflammation is associated with atherosclerosis progression. 24 In patients with psoriasis, it has been reported that the duration and severity of the disease are related to cardiovascular risk and the degree of atherosclerosis. 16,25 In this study, duration of psoriasis correlated positively with cAIx (r = .319, P = .001). Correlation between disease duration and CAVI was not significant (r = .182, P = .066), but a P value below .1 suggests a positive correlation tendency. However, the severity of psoriasis assessed by PASI did not affect arterial stiffness in this study. We believe that PASI at a specific point in time might not be a suitable representation of psoriasis severity over its entire course, as psoriasis is a dynamic disease.
The higher frequency of obesity and its correlation with psoriasis are well described in Western countries, but this remains controversial in Asia. 26 –29 In this study, there was no significant difference in BMI between the psoriasis and control groups (P = .897), and BMI showed a negative correlation with CAVI on multiple linear regression analysis (β = −.179, P = .004). Considering that the mean BMI is lower and severe obesity is uncommon in Asians, the correlation between obesity and psoriasis in Asians may differ from that in Western populations. In this study, we can say that patients with psoriasis are not more obese than healthy controls and that psoriasis plays an independent role in promoting atherosclerosis in a relatively nonobese Asian population, compared with a Western population.
This study has several limitations. First, most of our patients were referred from local clinics, and the majority of patients had moderate to severe disease. Second, although arterial stiffness may be affected by other cardiovascular risk factors, including family history of CVD and alcohol consumption, these factors were not assessed in this study.
In conclusion, psoriasis can be considered an independent risk factor for arterial stiffness in Koreans. Additionally, older patients with psoriasis with longer disease duration should be monitored carefully for cardiovascular risk.
Footnotes
Authors’ Note
Byung Gon Choi and Hyun Suk Yang had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design were done by Byung Gon Choi, Min Jung Kim, and Yong Beom Choe. Acquisition, analysis, and interpretation of data were done by Byung Gon Choi, Min Jung Kim, Hyun Suk Yang, and Yong Beom Choe. Drafting of the article was done by Byung Gon Choi, Min Jung Kim, Hyun Suk Yang, and Yong Beom Choe. Critical revision of the article for important intellectual content was done by Yang Won Lee, Yong Beom Choe, and Kyu Joong Ahn. Statistical analysis was carried out by Byung Gon Choi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Konkuk University Medical Center Research Grant 2015.