
Abstract
Since the first cardiac catheterization in 1929, this procedure has evolved considerably. Historically performed via the transfemoral access, in the last years, the transradial access has been spreading gradually due to its many advantages. We have conducted a review of published literature concerning efficacy, safety, and cost-effectiveness, and we analyzed our patients’ data, including the results of the recently published Minimizing Adverse hemorrhagic events by TRansradial access site and systemic implementation of angioX (MATRIX) study. This review confirmed the superiority of the transradial access compared to the femoral access, especially regarding complications related to the access site, duration of hospitalization, and comfort for the patient. The transradial approach is an excellent option for coronary angiography, and the procedure’s risks are reduced by increased operator experience.
Introduction
The history of cardiac catheterization and angioplasty began in 1711 when Hales performed the first equine biventricular catheterization 1 and progressed through the centuries till 1929 when German physician Forssman performed a dramatic right-heart self-catheterization through the antecubital vein. 1
During the following years, many other accesses were tried, such as the femoral, the radial, and the brachial artery. The latter is usually unused due to its high susceptibility to damage either at the time of puncture or during the hemostasis, and as the only artery that supplies blood to the upper limb, its damage would result in a significant ischemia with serious implications for function. Kiemeneij et al confronted the 3 accesses in the ACCESS study, which highlighted that, with equal procedural immediate result (about 91% in the 3 groups), the percentage of complications is lower with the radial route (0%), compared to the femoral (2%) or the brachial (2.3%). 2
The first publication relating to the transradial approach dates back to 1989 with Campeau, 3 which set forth the considerable advantages in terms of safety and ready mobilization of the patient. Before long, many specialists were trained on transradial access, forming a core team of “radialists,” with the goal of enabling the international spread of this innovative technique.
Despite the clear advantages, the transradial approach has taken more than 10 years to be widely shared; the main reason is that the coronary angioplasty by transradial is technically more challenging than the traditional transfemoral technique, since it involves the use of smaller guiding catheters and devices, requiring greater caution in their handling; cannulation of the right arm, bearing in mind that the arterial anatomy of the arm and the subclavian arteries is less well known, can reserve some unexpected surprise. 4,5
Today, more than 20 years after the first procedure, the transradial approach has established itself as one of the more conventional routes, it has spread around the world, and more young interventional cardiologists seem to be interested in this technique. 6 The transradial approach, notwithstanding the undoubted advantages, cannot be applied indiscriminately. The major drawback is the absence of adequate collateral circulation between the ulnar and the radial arteries; although radial occlusion is a rare complication (3%-5% of patients 6 ), it could have serious consequences. Other contraindications to the radial approach are patients with chronic renal failure, in which the artery may be necessary for the creation of an arteriovenous fistula (AVF). Yan et al evaluate the impact of radial catheterization for coronary angiography and percutaneous coronary intervention (PCI) measuring the radial artery diameter and intima–media thickness (IMT) 7 before, 1 day, and 1 month after the procedures. They observed an increased IMT from 0.25 ± 0.12 mm before the procedure to 0.69 ± 0.31 mm the day after it (P < .01 compared to baseline) and a decrease to 0.38 ± 0.17 mm after a month (P < .05 compared to baseline); the radial artery diameter followed a similar pattern. Perhaps not surprisingly, a study investigating the impact of increased radial artery IMT on the patency of radiocephalic AVF in hemodialysis patient showed an early failure of the AVF. 8 Even if transradial PCI improves the safety and the efficacy of outcome in both sexes, 9 it is not always feasible, especially in women of short stature who tend to have smaller hardly palpable radial arteries and patients with known pathologies of the subclavian or innominate artery.
The main complication observed with the transradial approach,
10
–15
directly correlated with the excessive manipulation of the catheters and with the preprocedure anxiety level,
16
–18
is spasm: In most cases, it can be easily treated with medical therapy (nitroglycerin; verapamil, or nitroprusside); sometimes, however, it is a refractory spasm that requires conversion to a femoral approach. Other rare complications may be: hematoma of the vascular access site or in the forearm for perforation of a small capillary; AVF; pseudoaneurysm; causalgia, a rare nerve injury during the puncture; pain from refractory spasm during and after the procedure; eversion or artery rupture during removal of the introducer; ischemia of the hand in case of occlusion of the radial artery in the absence of collateral circulation; and delayed bleeding a few days later.
The femoral artery has a size that allows easier cannulation of the artery and manipulation of the catheters; therefore, so far, the femoral artery has been the most suitable approach for PCI. The femoral artery access, however, is not without limitations; it is a relatively deep artery, particularly in patients with obese, which is difficult to reach. It is located in close contact with the vein and the femoral nerve, so it can potentially lead to iatrogenic injuries. Finally, this approach necessarily requires a period of immobilization in bed. In addition, the most feared complication associated with femoral access is retroperitoneal hematoma, a rare but potentially fatal complication (0.1%-0.5%
The radial artery has considerable advantages such as the already mentioned easier hemostasis, without considering that the patient himself can recognize more easily and promptly any bleeding and control it with a compression waiting for medical help, although severe bleeding is unusual and the ability to mobilize patients immediately after the procedure, no additional bleeding risks, which is clearly demonstrated in the large randomized clinical trial: Radial Versus Femoral Access for Coronary Angiography and Intervention in patients with acute coronary syndromes (RIVAL). 6
Unlike the femoral artery, the median nerve is not located in proximity of the artery, reducing the risk of nerve damage during the puncture or in case of hematoma; besides, the risk of AVFs is rare because venous return is ensured by a deep vein network and a superficial and not by a single main vein that runs near the radial artery.
Finally, we need to consider the low total cost and reduction in waiting lists, thanks to the increased turnover in cardiology departments; the benefits for the nursing staff in terms of patient care; and the satisfaction of the cardiologist to perform a less invasive and more comfortable procedure for the patient, despite the initial greater complexity of the technique.
Single-Center Experience and Review of the Literature
In our department, we retrospectively analyzed our patient data from 2008 to 2013. During the first 3 years, 2008 to 2010, we carried out a total of 1196 procedures, including 49 by the radial route and 1147 by the femoral route; in particular, in 2008, only 7 procedures by the radial route and 405 by the femoral route among over 412 procedures were performed; in 2009, the corresponding numbers were 14 radial and 382 femoral in over 396 total procedures performed; and in 2010, 28 radial artery and 360 femoral in over 388 procedures.
In the second 3-year period, 2011 to 2013, considering the obvious advantages of radial access as demonstrated in the international literature, 10,11,12,13 we decided to switch to the radial approach, with a total number of procedures amounted to 2622, of which 1945 were by the radial approach and 677 were by the femoral artery route.
In 2011 to 2013, we observed a marked increase in procedures performed both overall and specifically the transradials, in particular, in 2011, 384 via the radial route among over 488 total procedures; in 2012, 737 via the radial route among over 1036 and in 2013, 824 via the radial route among over 1098 procedures performed (Figure 1).
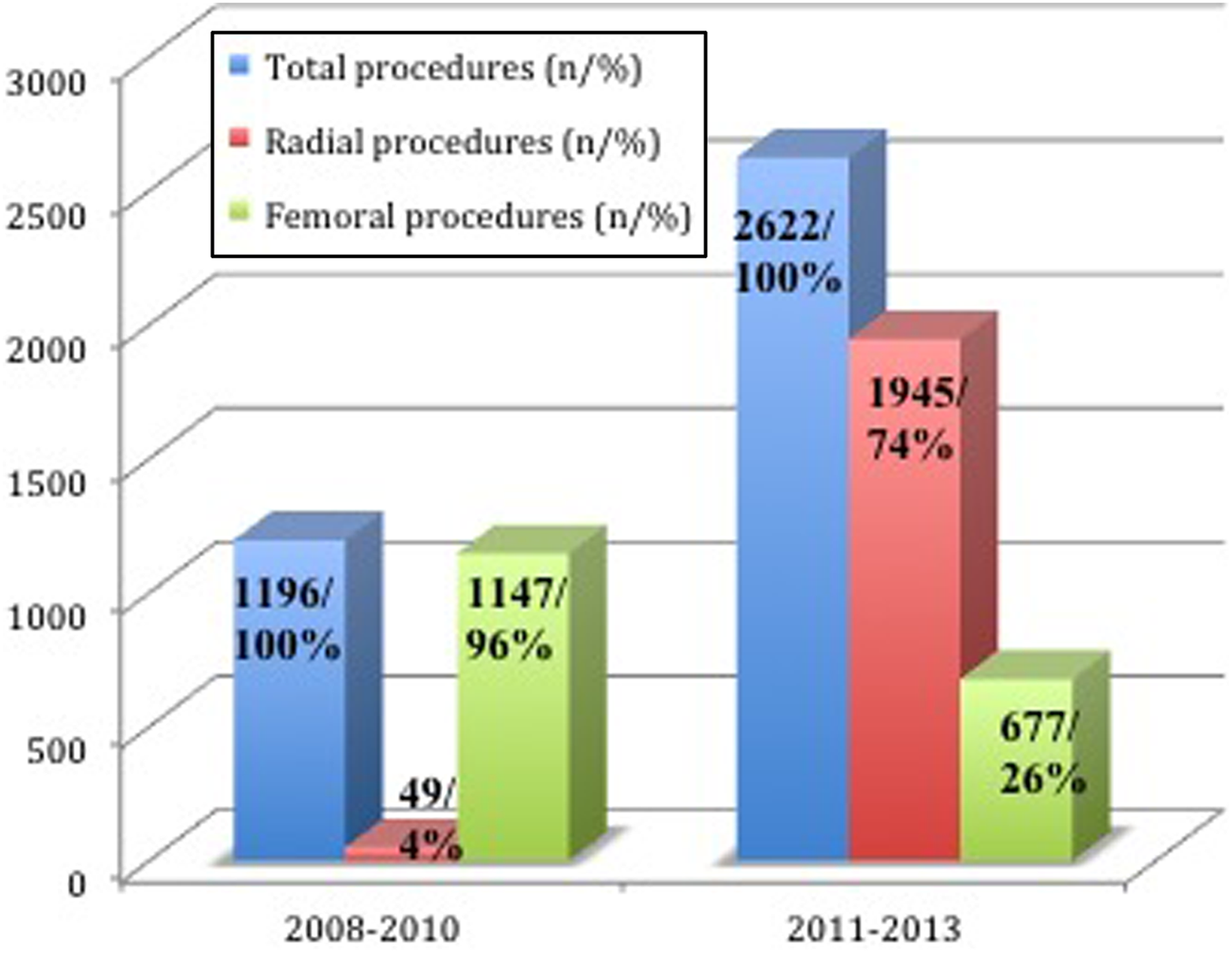
Graph showing analysis of access route (femoral vs radial) in our center from 2008 to 2013. We observed a marked increase in procedures performed both overall and specifically by the transradial compared to transfemoral routes.
The comparison of the prevalence for each year is impressive: we have gone from an average of 3.6% transradial approaches in 2008 to 2011 to an average of 74.6% transradial procedures in the second 3-year period (Figure 2).
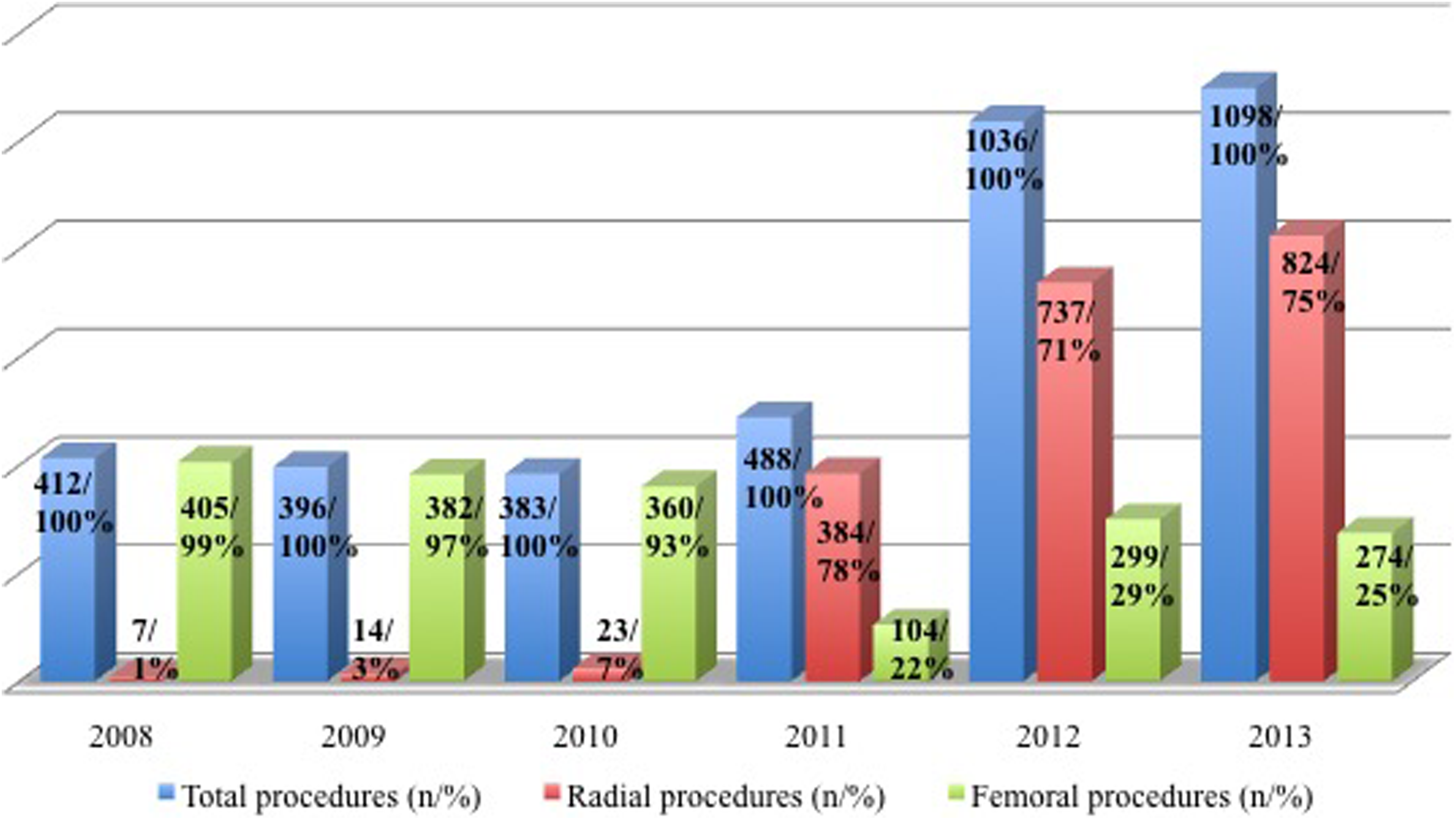
Graph showing analysis of access route (femoral vs radial) in our center for each year.
Looking at the available data, it is possible to appreciate how in 2011 there has been a rising trend of transradial procedures; this occurred in the first place for a critical and conscious choice about the risks and benefits of procedures via the radial and femoral artery, with the aim of always ensuring greater patient comfort and less risk and second to participation in the Minimizing Adverse hemorrhagic events by TRansradial access site and systemic implementation of angioX (MATRIX) study, 19 –21 which included a double randomization: the first one for the vascular access and the second one for pharmacological treatment.
It is obvious that the randomization influenced the distribution of patients in the 2 arms, slightly altering the prevalence in each individual year. Patients were randomly placed with a 1:1 in radial or femoral access by a computer system, with an operating sequence stratified by use of ticagrelor or prasugrel, type of acute coronary syndrome (ACS; ST elevation myocardial infarction, non-ST elevation myocardial infarction, or unstable angina), and immediate execution angiography.
The coprimary results at 30 days were major adverse cardiovascular events, defined as death, myocardial infarction, or stroke, and adverse clinical events, defined as major adverse cardiovascular events or Bleeding Academic Research Consortium (BARC) major bleeding unrelated to coronary bypass. 19 A total of 8404 patients were randomized with ACS with or without ST-segment elevation, of which 4197 were assigned to the radial access and 4207 to the femoral artery route. Of those assigned to radial access, 369 (8.8%) had major cardiovascular events compared to 429 (10.3%) of those assigned with femoral access (rate ratio [RR] 0.85, 95% CI 0.74-0.99; P = .0307); 410 (9.8%) patients with radial access had reduced incidence of clinical events compared to 486 (11.7%) patients with femoral access (P < .05). The difference was driven by the higher incidence of major bleeding according to the BARC criteria unrelated to bypass (1.6% vs 2.3%, RR 0.67, 95% CI 0.49-0.92; P = .013) and mortality from all causes (1.6% vs 2.2%, RR 0.72, 95% CI 0.53-0.99; P = .045). These data have shown that the treatment by radial, compared to the femoral, reduces the incidence of adverse clinical events, mainly due to a reduction in major bleeding and mortality.
About stroke risk with radial access, Jurga 22 compared the incidence of cerebral microembolism during PCI via the radial and femoral artery. They observed that the median (minimum–maximum range) numbers of particulate emboli were significantly higher with radial 10 (1-120) than with femoral 6 (1-19). More microemboli passed the right middle cerebral artery with the radial access and thus may influence the occurrence of silent cerebral injuries. Otherwise Ratib et al 23 performed a retrospective analysis of the British Cardiovascular Intervention Society database between January 2006 and December 2010, and the data were split into 2 cohorts based on the access site. They observed a neurologic complication (NC) rate of 0.11% in each cohort over a total of 124 616 radial procedures and 223 476 femoral procedures. In univariate (P = .93) and multivariate analyses (P = .91), there was no significant association between the use of radial access and the occurrence of NCs.
The MATRIX study is the starting point of other important substudies still in progress, such as the RAD-MATRIX—Radiation Dose study-Minimizing Adverse hemorrhagic events by TRansradial access site and systemic implementation of angioX— 24 which compares operator exposure to the radiation with the 2 different vascular accesses, and the AKI-MATRIX—Acute Kidney Injury-Minimizing Adverse hemorrhagic events by TRansradial access site and systemic implementation of angioX— 25 which studies the correlation between AKI and PCI.
In the literature a frequent topic of debate is the increased radiation exposure potentially associated with transradial access, which is a possible drawback of this method. Whether transradial access is associated with a clinically significant increase in radiation exposure that outweighs its benefits however is unclear. Plourde et al 26 compared radiation exposure between transradial access and transfemoral access for diagnostic coronary angiograms and PCIs with a systematic meta-analysis focused on the primary radiation outcomes of fluoroscopy time and operator radiation exposure. The analyses showed that the transradial access was associated with a small but significant increase in fluoroscopy time for diagnostic coronary angiograms and PCI compared to the transfemoral access. Mean operator radiation doses for PCI with basic protection were higher with the transradial access compared to the transfemoral access. The authors concluded that the transradial access was associated with a small but significant increase in radiation exposure in both diagnostic and interventional procedures compared to the transfemoral access. Since differences in radiation exposure narrow over time and experience of the operators, the clinical significance of this small increase is uncertain and is unlikely to outweigh the clinical benefits of the transradial access.
Related to the risk of AKI, a recent report from the large retrospective Blue Cross Blue Shield of Michigan Cardiovascular Consortium database 27 and exploring the risks of AKI and nephropathy requiring dialysis in patients treated with transradial intervention (TRI), when compared to transfemoral intervention (TFI), demonstrates that TRI is associated with a significantly reduced risk of AKI. Moreover, observational data suggest an advantage of TRI over TFI in terms of reduction in the risk of AKI, although they are only hypothesis generating. 28 Actually, it may be argued that the supposed benefits of TRI might be due to the selection bias, which is inherent in registries. Else, they might be mediated by lower bleeding complications, lower cholesterol embolization syndrome, or a combination of both. Importantly, no prospective comparison on renal outcomes has been carried out in randomized trials of TRI versus TFI.
Finally, in the subset of patients with previous coronary artery bypass grafting (CABG), an optimal vascular access site for coronary angiography and intervention is still a matter of debate. In a systematic review and meta-analysis of available studies comparing Radial Approach (RA) with Femoral Approach (FA) in patients with previous CABG, Rigattieri et al 29 found that compared to FA, RA required similar procedural time, fluoroscopy time, and contrast volume and was associated with similar rate of procedural failure, higher rate of crossover to another vascular access, and lower risk of access site complications.
After looking at the change in the incidence of transradial procedures in these 6 years, it is also important to evaluate how the incidence of postprocedural complications changed, including radial access artery occlusion and, for the femoral access, the incidence of hematoma, pseudoaneurysm, and/or AVFs.
Regarding the first 3 years, over 1196 procedures—49 by radial and 1147 by femoral artery—48 complications were registered (4.01%)—1 by radial and 47 by femoral. A retrospective analysis of femoral access complications showed that in 2008, there were 18, corresponding to 4.44% of the procedures performed by femoral access; in 2009, there were 15, corresponding to 3.92% of femoral procedures, and in 2010, there were 14, corresponding to 3.88%.
Otherwise over 49 transradial procedures performed, only 1 complication occurred in 2010 corresponding to 3.57% of the transradial procedures.
As for the second 3 years, 125 complications occurred over 2622 (4.95%) procedures—104 by radial and 21 by femoral. In particular, about 677 transfemoral procedures, 21 complications occurred: 5 in 2011, corresponding to 4.8% of procedures by femoral access; 9 in 2012, corresponding to 3% of the femoral procedures; and 7 in 2013, 2.5% of the femoral procedures. Instead, for what concerns transradial procedures, over 1845 procedures, 104 complications occurred: 33 in 2011, corresponding to 11.7% of the radial procedures; 47 in 2012, 6.47% of the procedures; and 24 in 2013, 2.9% of the transradial procedures.
It seems clear that there has been a progressive reduction in complications both in the femoral vascular access site, as can be seen from Figure 3, and also in the transradial, as a matter of fact, we noted a progressive but net percentage of reduction in the complications of the vascular access site, as shown in Figure 4.
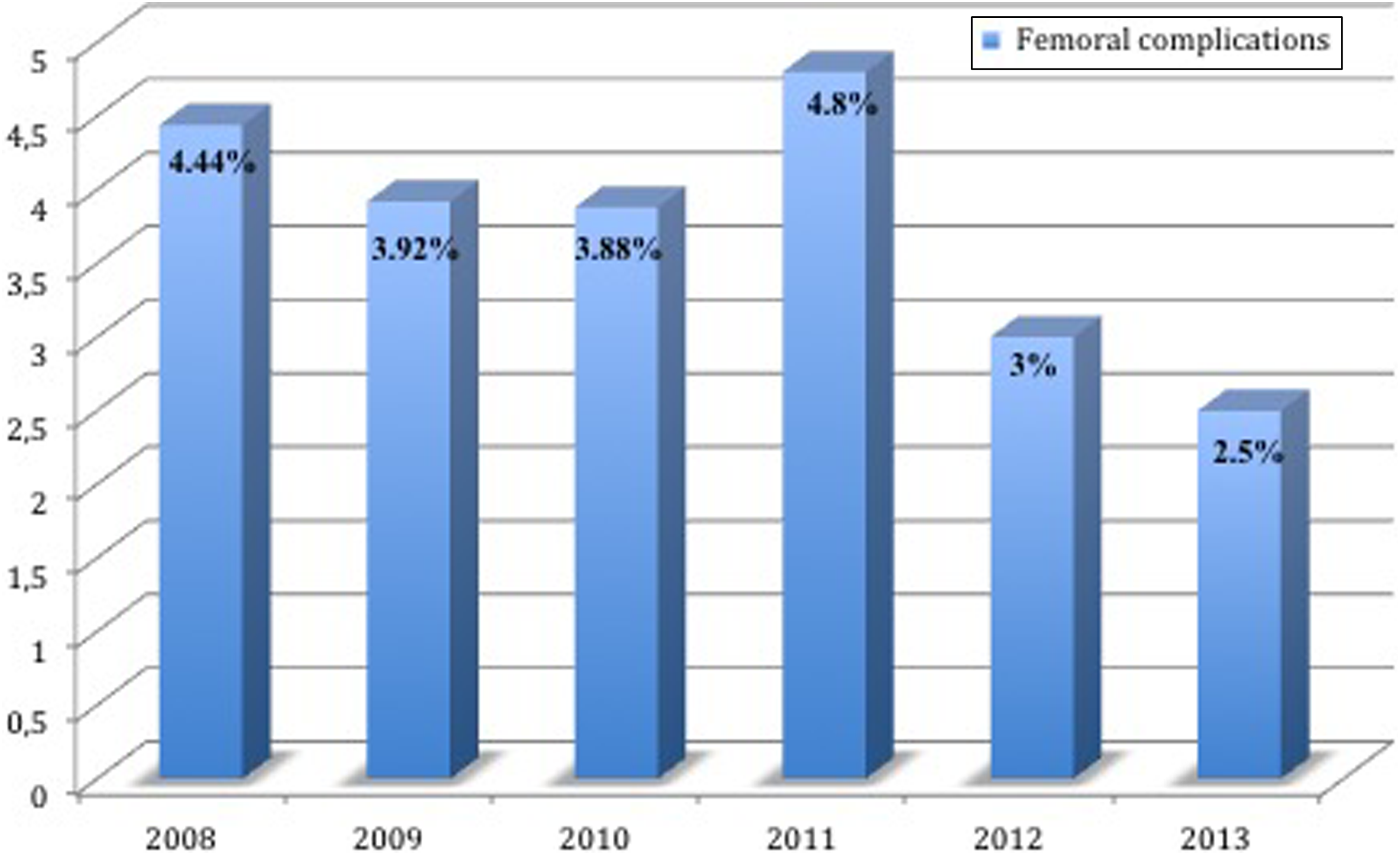
Graph showing rate of complications in the femoral vascular access site from 2008 to 2013. There has been a progressive reduction in complications in the femoral vascular access site, especially when compared to the number of overall procedures.
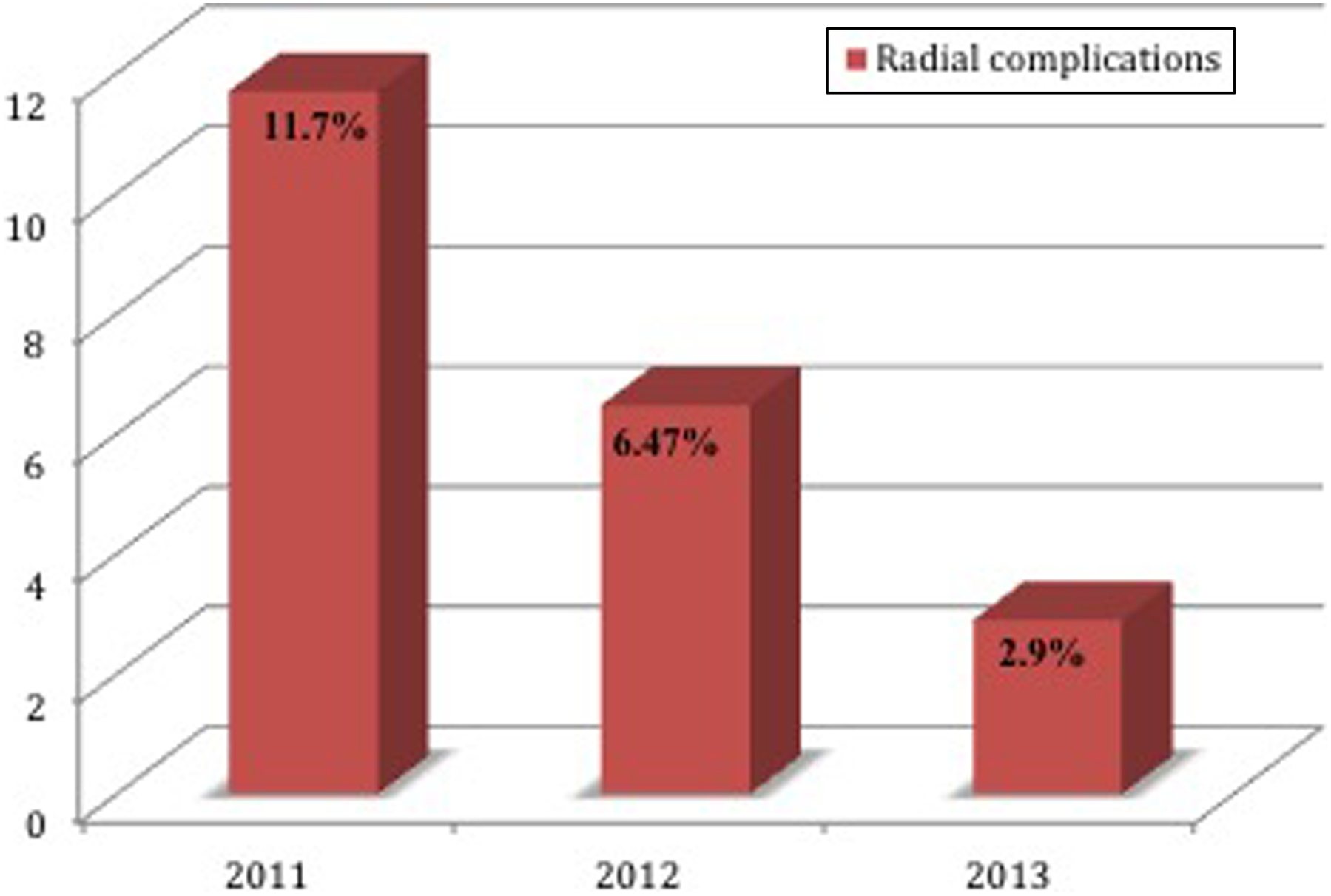
Graph showing rate of complications in the radial vascular access site from 2010 to 2013. We noted a progressive net percentage of reduction in the complications of this vascular access site.
Conclusion
More and more evidence shows that the benefits associated with the execution of invasive coronary procedures by the radial approach if performed at high-volume centers. As the consensus document 30 on the radial approach in PCI stated, the risks related to transradial approach are minimized by operator experience. An operator’s annual procedure volume >80 transradial cases correlates with a significant reduction in access failure, sheath insertion time, and procedure time. In our experience, we observed a significant increase in total complications in the first year switching from femoral to radial probably due to the learning curve. Although this is inconvenient, we registered a progressive reduction in total complication using the radial approach from 2011 to 2013, lower than the incidence of total complication registered in first 3-year period (2008-2010) as shown in Figure 5. These advantages are not limited to within the medical (reduction in complications) but also extend to the fields of personnel management (reduction in the workload), patient satisfaction (reduction in median length of stay in hospital 3.6 vs 10.4 hours, P < .0001 31 ), and economic resources (reduction in costs by procedure, increase in total procedures). In addition, the radial access opens new perspectives, not otherwise practicable, by accessing the femoral (execution of outpatient procedures), and it allows reaching many patients, previously untreated for many reasons (clinical and/or emotional). Recent trials, such as the MATRIX, 19 have shown how the radial access reduces mortality and major bleeding in patient with ACS. In our view, the radial approach should not be seen as a simple alternative to the femoral artery (in which case most of its advantages would not be obvious) but definitely as an innovation to be introduced in the daily practice of invasive cardiology.
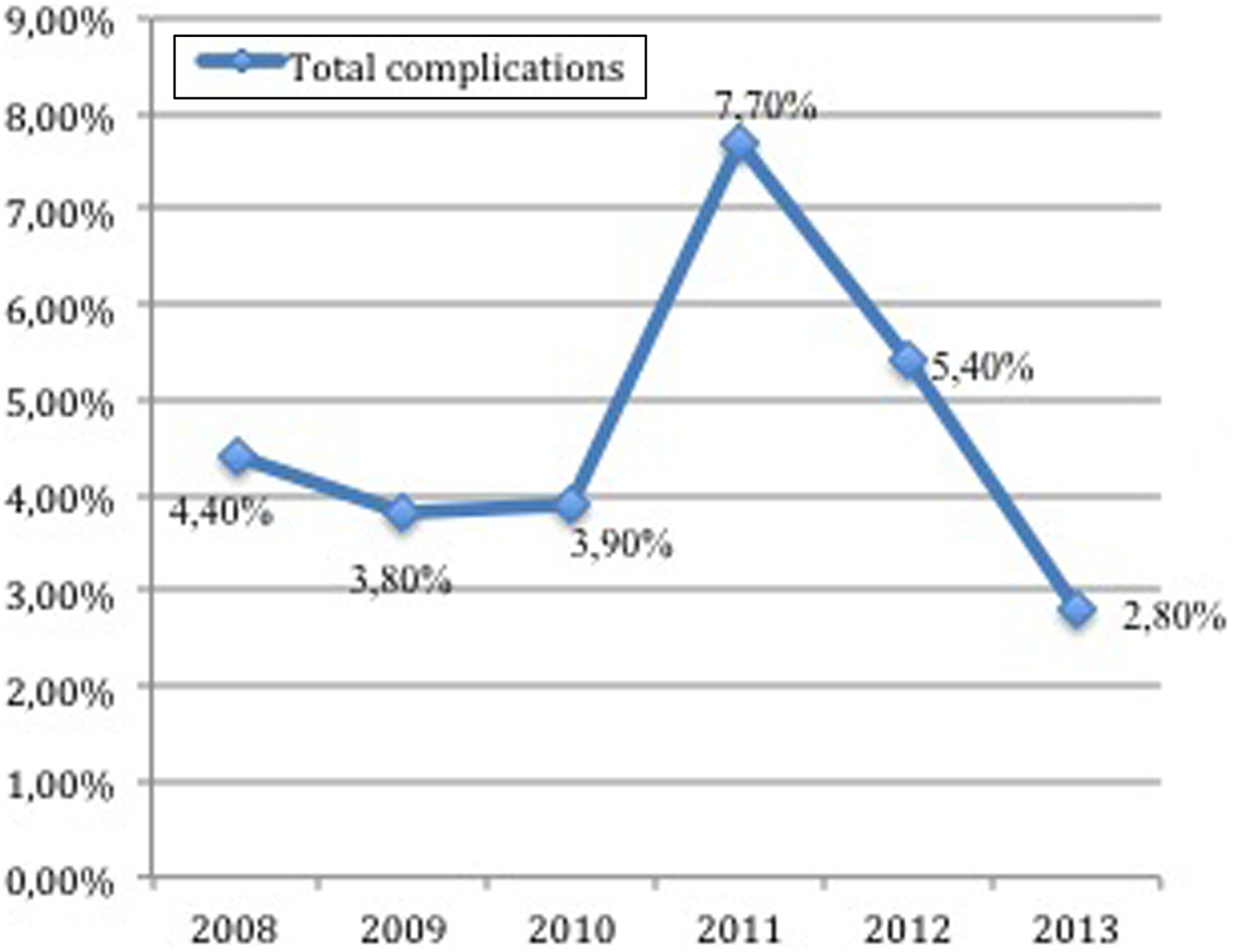
Graph showing how, for an operator’s annual procedure >80 transradial cases, we registered a progressive reduction in total complications with radial approach from 2011 to 2013, lower than the incidence of total complication registered in the first 3-year period (2008-2010).
Footnotes
Authors’ Note
All authors contributed to (1) conception and design or acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.