
Abstract
We compared the efficacy and safety of the transradial approach percutaneous coronary intervention (TRA-PCI) and transfemoral approach percutaneous coronary intervention (TFA-PCI) for bypass grafts lesions. Patients (n = 184) were retrospectively enrolled. Less contrast was used during the procedure in the TRA group than in the TFA group, 201.5 (45.5) mL versus 221.5 (49.1) mL, P = .004, although fluoroscopy time was longer in the TRA group, 22.5 (6.3) minutes versus 20.3 (6.1) minutes; P = .017. The incidence of net adverse clinical events (NACEs) was lower in the TRA group than in the TFA group (3.1% vs 8.8%, respectively, P = .111). The incidence of Bleeding Academic Research Consortium type 3 and 5 bleeding (0% vs 5.5%, respectively, P = .022) was significantly lower in the TRA group than in the TFA group. For 1-year outcomes, there was no difference in the incidence of major adverse cardiovascular events (7.5% vs 9.9%, respectively, P = .569). In conclusion, TRA-PCI was associated with a lower rate of in-hospital NACEs mainly attributed to lower rates of major bleeding. The TRA-PCI showed comparable feasibility and efficacy in bypass grafts as compared with TFA-PCI when carried out by experienced operators.
Introduction
Since Campeau first reported percutaneous radial artery approach for coronary angiography in 1989, 1 many clinical trials and registries have shown that, compared to the transfemoral approach (TFA), the transradial approach (TRA) for coronary angiography and intervention significantly reduces all-cause mortality, major adverse cardiovascular events (MACE), access site bleeding, major vascular complications, and duration of hospital stay. 2 –10 Notably, as operators become familiar with and skilled at transradial interventional techniques, procedural outcomes of transradial coronary intervention have been substantially improved. 11
The literature demonstrated that the procedure time, fluoroscopy time, and radiation exposure were dramatically reduced in TRA-percutaneous coronary intervention (PCI) and were comparable with TFA-PCI if the transradial interventional procedures were performed by experienced operators. 6,11,12 Consequently, TRA has been widely accepted by interventional cardiologists and has gradually replaced TFA in the past 2 decades as an optimal choice for diagnostic and therapeutic coronary intervention in a broad spectrum of patients. 2,4 However, angiography and interventions through radial artery access in bypass grafts remain a challenge because of the complexity of anatomical issues. 13,14
To date, the procedural and clinical outcomes of PCI via TRA versus TFA in patients with bypass grafts lesions after coronary artery bypass graft (CABG) surgery are less studied. 15 –19 Therefore, we compared the efficacy and safety of TRA-PCI with TFA-PCI in bypass grafts.
Methods
Study Design and Patient Population
This is a single-center retrospective study that compared the procedural and clinical outcomes of TRA-PCI with TFA-PCI in bypass grafts. From January 2006 to December 2015, a total of 184 patients who had previously undergone CABG surgery and received interventional cardiac catheterization in bypass grafts in our interventional center were included in the present study. All of the procedures were performed by experienced operators who have more than 10 years’ experience of coronary intervention and have performed more than 1000 PCIs per year with a success rate of >95% using both the TFA-PCI and TRA-PCI approach. According to the access site used during interventional procedures, patients included in the study were initially categorized into a TRA group (n = 93) and a TFA group (n = 91). Patients whose procedural information was incomplete, who simultaneously received PCI for original coronary lesions, or who lost at 1-year follow-up were excluded (Figure 1).
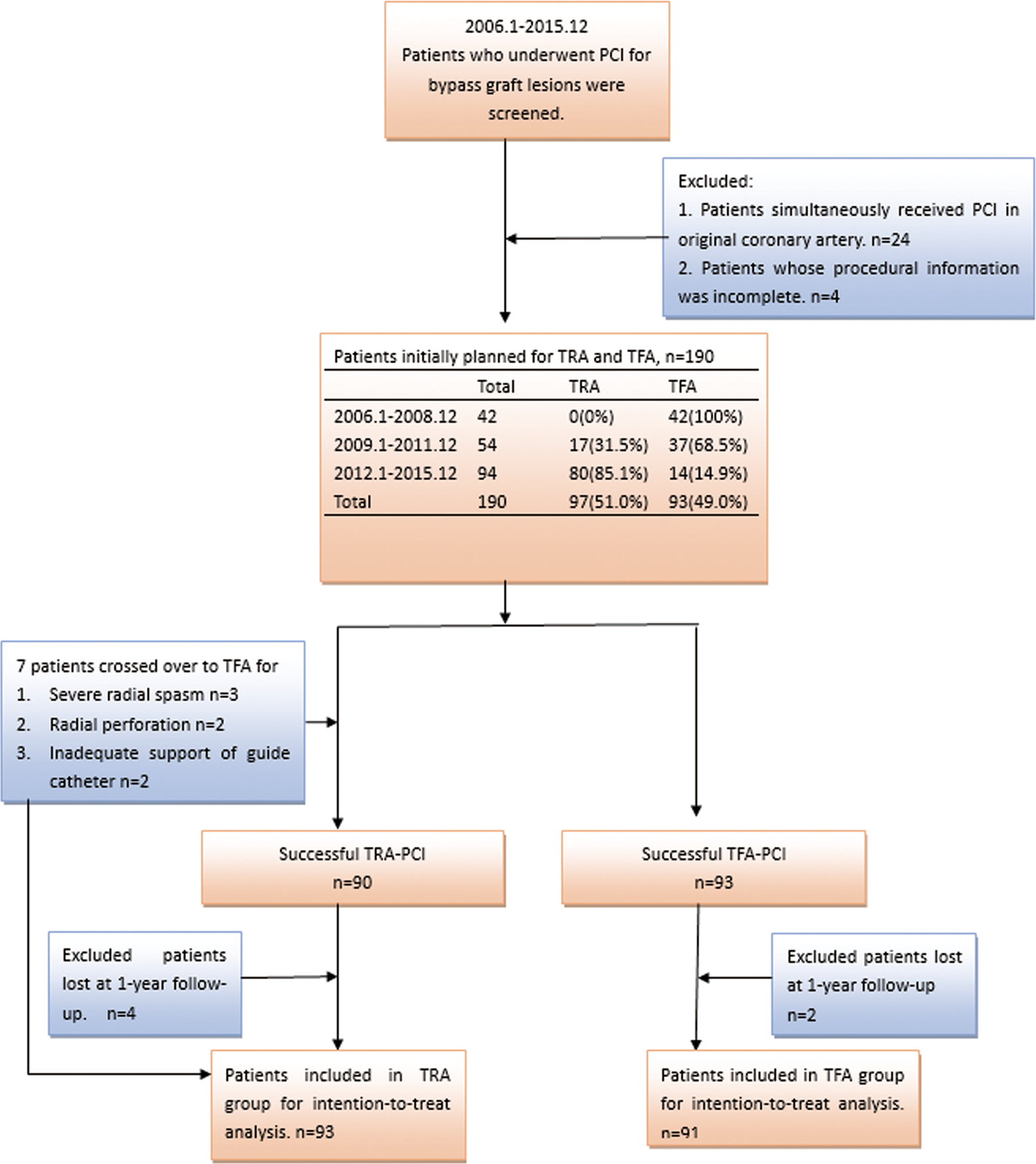
Flowchart of patients who underwent PCI in bypass graft lesions in this study. PCI indicates percutaneous coronary intervention.
Patient data including baseline characteristics, procedural documents, and in-hospital clinical outcomes were extracted from the electronic medical record system and cardiac characterization reports. As most patients undergoing coronary interventions in our center are followed up with regular clinic visit, we managed to collect 1-year clinical outcomes. This study was approved by the institutional review board of Zhongshan Hospital, Fudan University.
Procedure Description
All procedures were performed in accordance with the American College of Cardiology/American Heart Association PCI guidelines. A preprocedural loading dose of 0.3 g aspirin and 300 mg clopidogrel or 90 mg ticagrelor was prescribed for all patients. All patients received statins routinely after admission (atorvastatin 20 mg/d, rosuvastatin 10 mg/d, pravastatin 40 mg/d, or simvastatin 20 mg/d). Statin loading was not used before PCI. Patients with estimated glomerular filtration rate <60 mL/min/1.73 m2 (using Chronic Kidney Disease Epidemiology Collaboration equation 20 ) received hydration therapy (0.5-1 mL/kg/h 0.9% normal saline, according to cardiac function) 12 hours before and 24 hours after intervention. The selection of the access sites was at the operator’s discretion. Patients planned for TRA underwent Allen test to assess ulnar artery patency prior to the procedures. The TFA catheterization was performed via the right or left common femoral artery if the former was not appropriate. Hemostasis was achieved through manual compression or using an Angio-Seal vascular closure device (St Jude Medical, Inc, Saint Paul, Minnesota) according to the operator’s decision. After procedures, patients were mandatorily immobilized in bed for 24 hours. Catheterization was performed via the left radial artery to facilitate angiography of the left internal mammary artery graft. In all cases, the operators were standing on the right side of the patients. A “cocktail” of nitroglycerin and lidocaine was administered via the radial sheath to prevent arterial spasm. Hemostasis was achieved using a TR Band (Terumo, Inc, Somerset, New Jersey) for 6 to 8 hours. Dual antiplatelet therapy (DAPT) with clopidogrel 75 mg/d and aspirin 100 mg/d was required to last for at least 12 months for all patients, and aspirin was required indefinitely after the end of DAPT.
Variables of Interest
The primary variables of interest were procedure related, including procedural time, fluoroscopy time, radiation exposure, and contrast volume. The secondary variables of interest were clinical outcomes, including in-hospital net adverse clinical events (NACEs) and 1-year MACEs. The NACE was a composite of all-cause mortality, myocardial infarction (MI), stroke, target vessel revascularization (TVR), Bleeding Academic Research Consortium 21 (BARC) type 3 and 5 bleeding, and major vascular complications. The MACE was a composite of all-cause mortality, MI, stroke, and TVR. Major vascular complications included retroperitoneal hematoma, limb ischemia, dissection, perforation, pseudoaneurysm, and arteriovenous fistula. Myocardial infarction was defined as new onset of chest pain accompanied with an elevation in troponin T more than 3 times the 99th percentile upper reference limit. 22 The TVR was defined as any clinically driven repeat PCI of the target vessel.
Statistical Analysis
Continuous variables were presented as mean (standard deviation) and compared using independent sample t test. Categorical variables were expressed as percentages (%) and compared using χ2 test or Fisher exact test. Intention-to-treat analysis was performed in the present study. All statistical analyses were performed by SPSS 18.0 (SPSS Inc, Chicago, Illinois). A 2-tailed P <.05 was considered significant.
Results
Patient Characteristics
A total of 184 patients were finally included into the present study, with 93 patients initially planned for TRA-PCI and 91 patients for TFA-PCI. As shown in Table 1, the mean age of the patients was 62.8 (8.7) and 61.2 (7.6) years in the TRA and TFA groups, respectively. Clinical presentations such as stable angina (48.4% vs 38.5%; P = .174), non-ST-segment elevation acute coronary syndrome (48.4% vs 57.1%; P = .234), and ST-segment MI (3.2% vs 4.4%; P = .678) were not significantly different between the 2 groups. In addition, cardiovascular risk factors such as current smoking (31.2% vs 28.6%; P = .699), hypertension (79.6% vs 76.9%; P = .663), diabetes mellitus (45.2% vs 48.4%; P = .665), hypercholesterolemia (67.7% vs 65.9%; P = .795), and peripheral arterial disease (46.2% vs 54.9%; P = .237) were not significantly different between the 2 groups. Meanwhile, no difference was observed regarding the age of CABG, 4.1 (2.5) versus 3.7 (2.3) years; P = .261, between the 2 groups. Therefore, there were no differences in demographic and baseline characteristics of patients between the TRA and TFA groups, as well as clinical presentation, patient history, and graft anatomy information.
Baseline Characteristics of Patients in the TRA and TFA Groups.
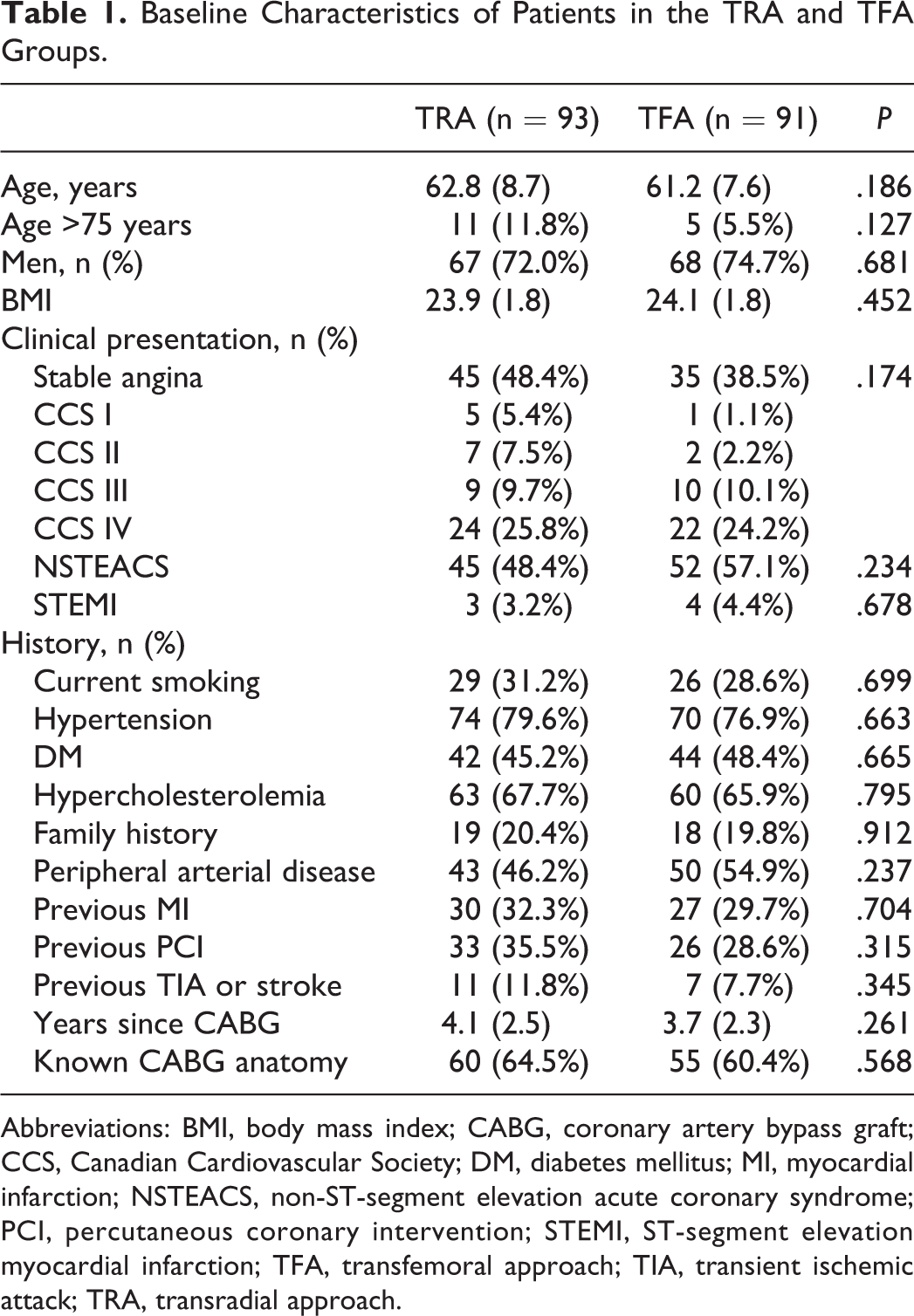
Abbreviations: BMI, body mass index; CABG, coronary artery bypass graft; CCS, Canadian Cardiovascular Society; DM, diabetes mellitus; MI, myocardial infarction; NSTEACS, non-ST-segment elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; TFA, transfemoral approach; TIA, transient ischemic attack; TRA, transradial approach.
Procedural Outcomes
All patients included in the present study received PCI in only 1 bypass graft (saphenous venous graft or left internal mammary artery graft). Seven patients (crossover rate 7.5%) initially planned for radial approach crossed over to the TFA group because of severe radial spasm (n = 3), radial perforation (n = 2), and inadequate support of guide catheter (n = 2). No patients in the TFA group crossed over to the TRA group in the present study. All patients in the TRA group used 6F arterial sheath and 6F guide catheter, while 32 (35.2%) patients in the TFA group used 7F arterial sheath and 7F guide catheter. There were no differences in the distribution of target grafts undergoing intervention, the number of diagnostic catheters used, the number of guide catheters used, the number of lesions treated, the number of balloons used, the number of stents implanted, and the average stent length between the 2 groups. The volume of contrast used during the procedure was greater in the TFA group than in the TRA group, 221.5 (49.1) mL versus 201.5 (45.5) mL; P = .004, while the fluoroscopy time was longer in the TRA group than in the TFA group, 22.5 (6.3) minutes versus 20.3 (6.1) minutes; P = .017. No differences were observed in procedure time and radiation dose between the 2 groups (Table 2, Figure 2). Additionally, there was no difference in the use of periprocedural antiplatelet and anticoagulant medications between the 2 groups, including aspirin, clopidogrel, ticagrelor, heparin, bivalirudin, and glycoprotein IIb/IIIa inhibitors (Table 2, Figure 3).
Procedural Characteristics and Periprocedural Medications of TRA-PCI and TFA-PCI for Bypass Grafts Lesions.a
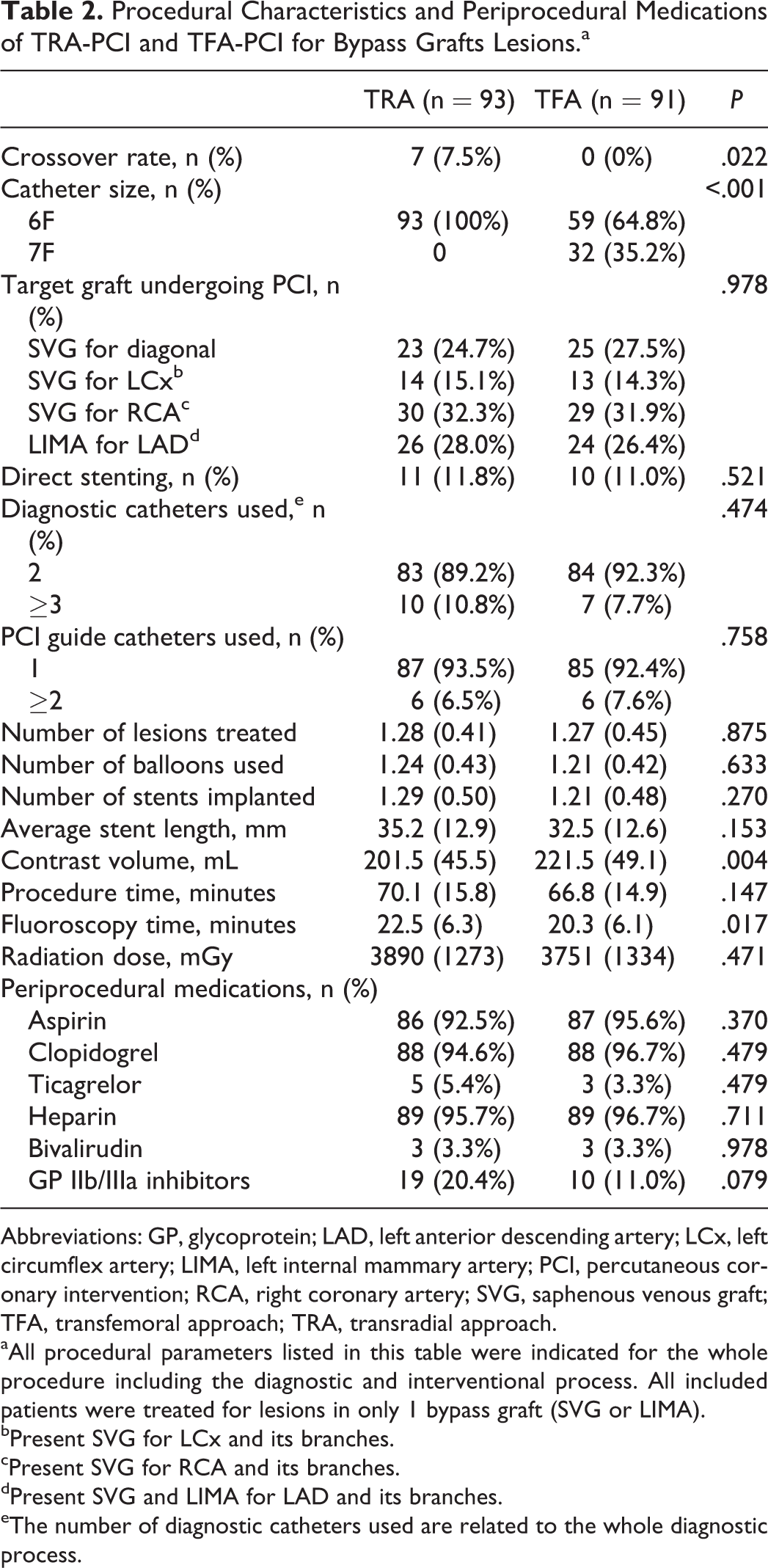
Abbreviations: GP, glycoprotein; LAD, left anterior descending artery; LCx, left circumflex artery; LIMA, left internal mammary artery; PCI, percutaneous coronary intervention; RCA, right coronary artery; SVG, saphenous venous graft; TFA, transfemoral approach; TRA, transradial approach.
aAll procedural parameters listed in this table were indicated for the whole procedure including the diagnostic and interventional process. All included patients were treated for lesions in only 1 bypass graft (SVG or LIMA).
bPresent SVG for LCx and its branches.
cPresent SVG for RCA and its branches.
dPresent SVG and LIMA for LAD and its branches.
eThe number of diagnostic catheters used are related to the whole diagnostic process.
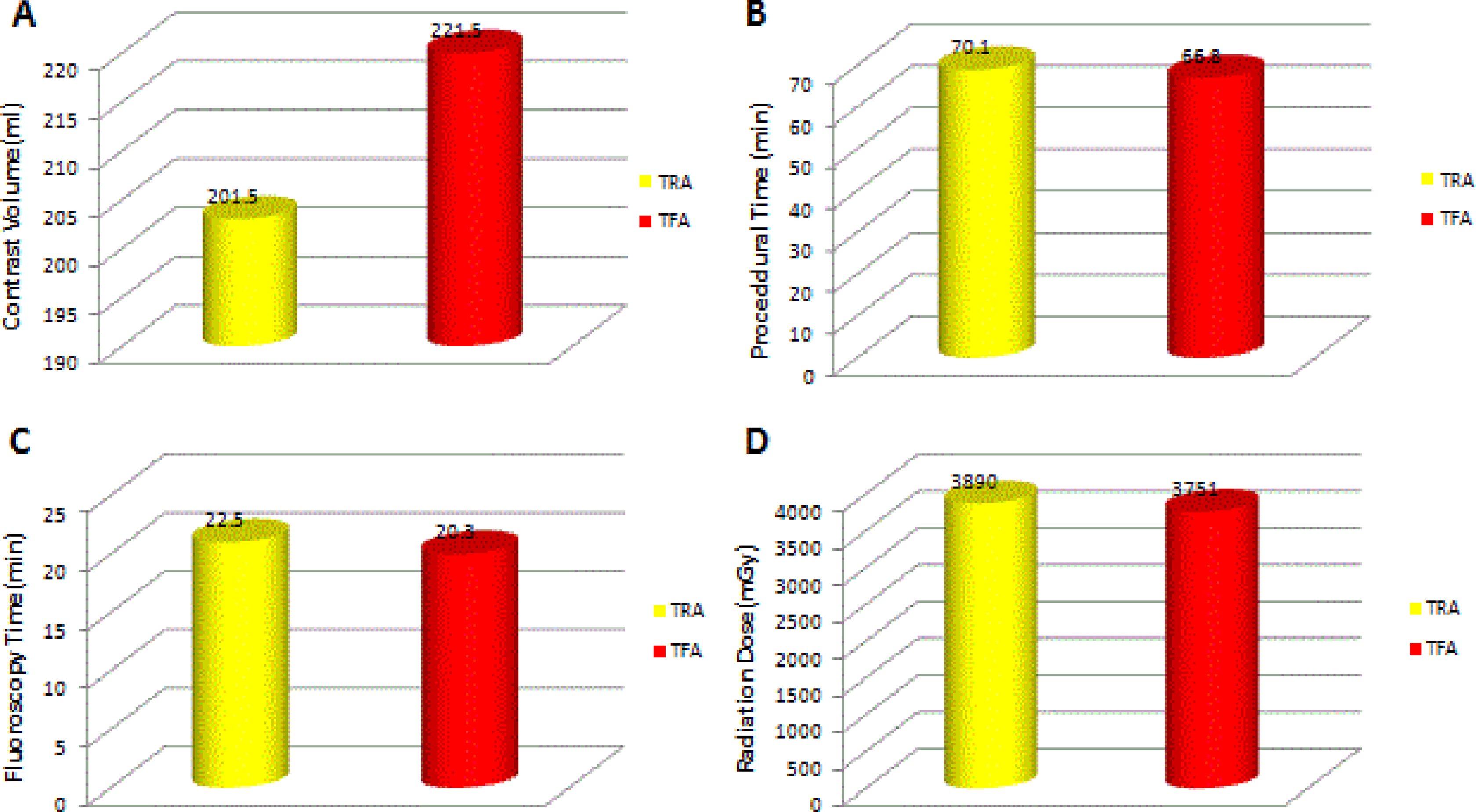
Procedural outcomes: (A) contrast volume, (B) procedural time, (C) fluoroscopy time, and (D) radiation time.
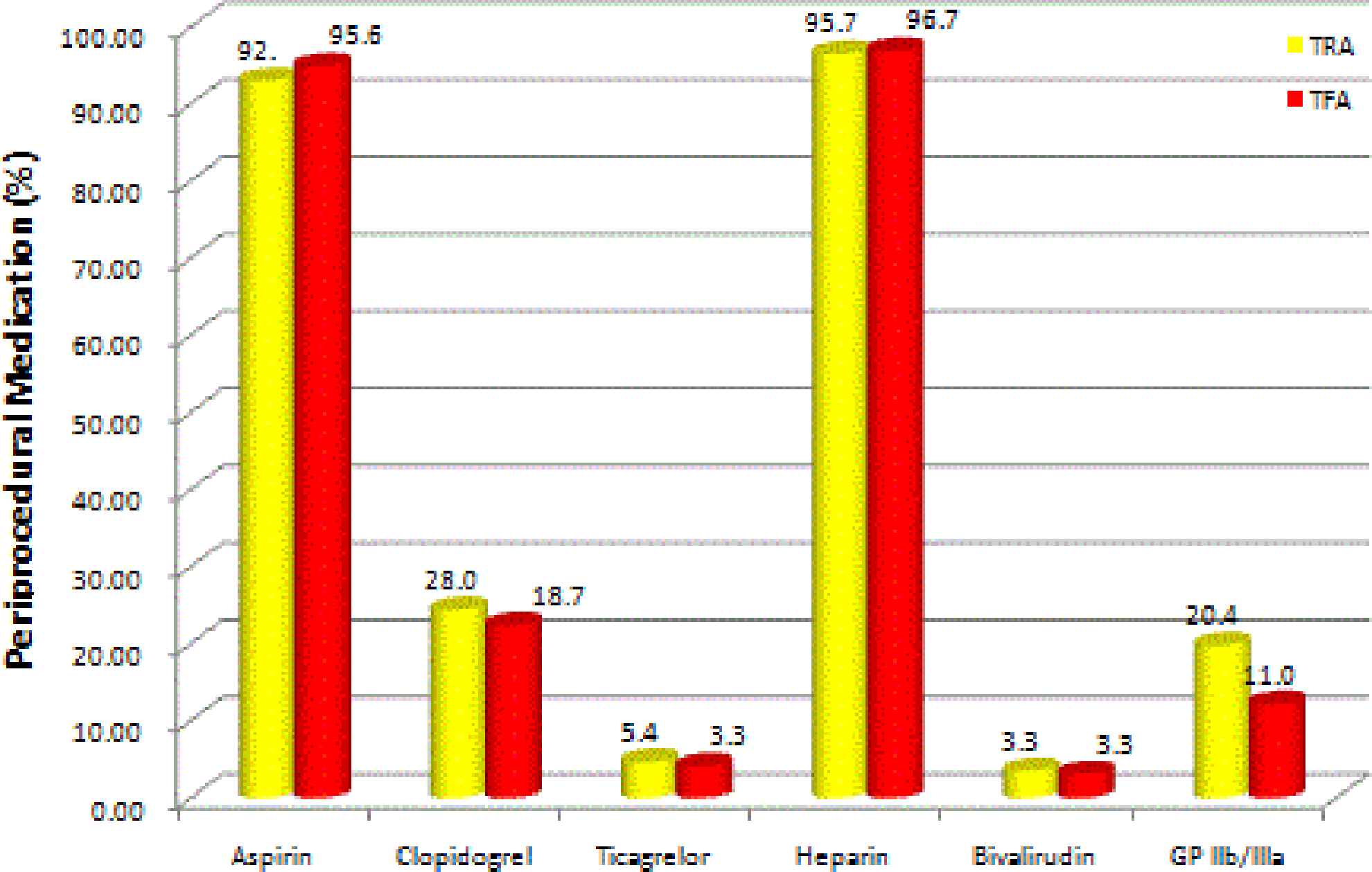
Periprocedural medication.
Clinical Outcomes
As demonstrated in Table 3, the rate of in-hospital NACEs was not significantly different in the TFA group than in the TRA group but numerically higher in the TFA group (8.8% vs 3.3%; P = .111). Notably, no bleeding event was observed in the TRA group, while BARC type 3 and 5 bleeding happened in 5 patients in the TFA group (0% vs 5.5%; P = .022). Vascular complications were not significantly different between groups. No differences were observed regarding other components of NACEs (Table 3, Figure 4). For 1-year clinical outcomes, there was no difference in the incidence of MACEs, all-cause mortality, MI, stroke, and TVR (Table 3).
In-hospital and 1-Year Clinical Outcomes of Patients in the TRA and TFA Groups.
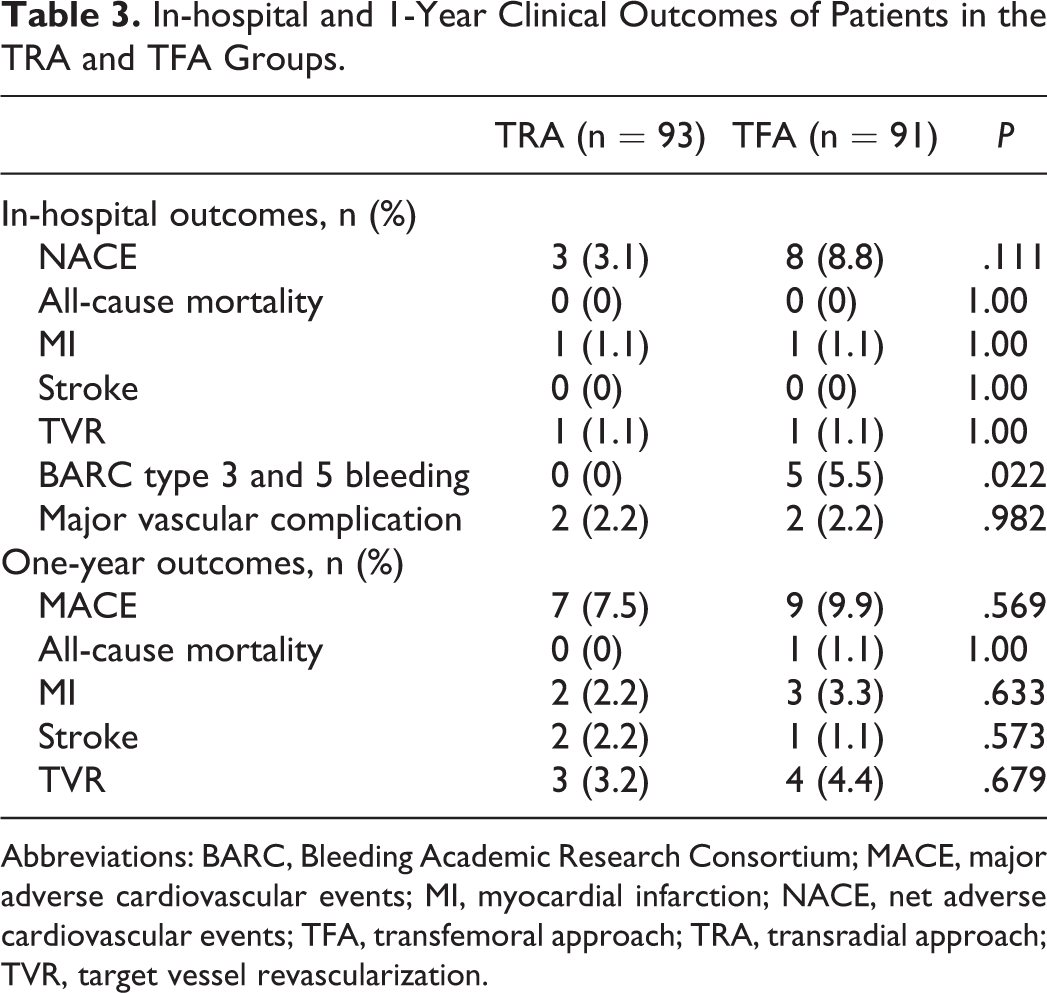
Abbreviations: BARC, Bleeding Academic Research Consortium; MACE, major adverse cardiovascular events; MI, myocardial infarction; NACE, net adverse cardiovascular events; TFA, transfemoral approach; TRA, transradial approach; TVR, target vessel revascularization.
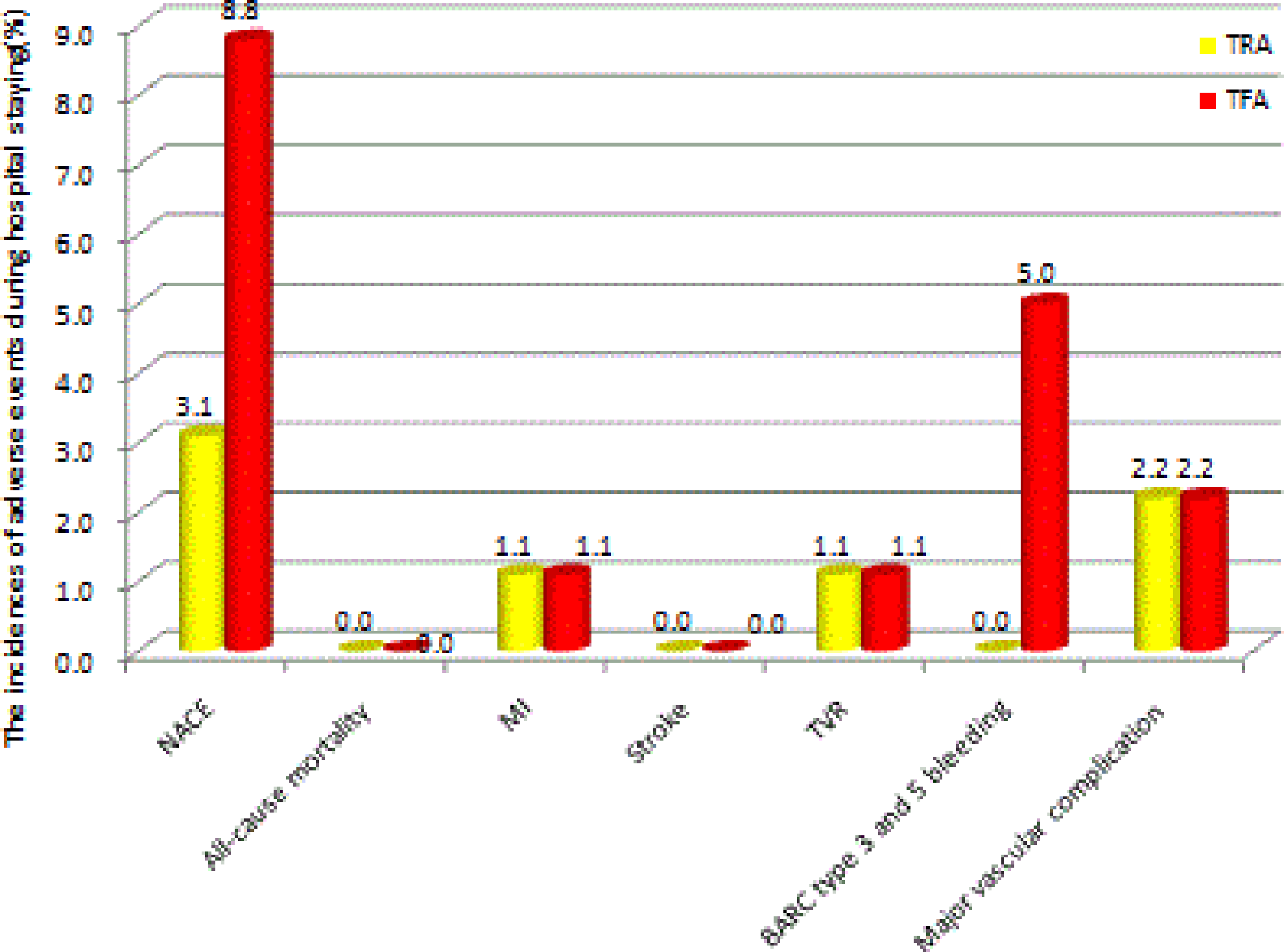
In-hospital clinical outcomes between the TRA and TFA groups. NACE indicates net adverse clinical events; MI, myocardial infarction; TFA, transfemoral approach; TRA, transradial approach; TVR, target vessel revascularization.
Discussion
This is a retrospective study that investigated the efficacy and safety of TRA-PCI compared with TFA-PCI for bypass graft lesions; the procedures were performed by experienced operators. The major findings are (1) Except for the contrast volume, which is significantly lower in the TRA group, there was no significant difference between groups regarding procedural outcomes such as procedural time and radiation dose, (2) The in-hospital NACE was numerically lower in the TRA group but not significantly different between the 2 groups. However, BARC type 3 and 5 bleeding was significantly higher in the TFA group, and (3) Both groups had comparable 1-year clinical outcomes.
Degeneration and occlusion of bypass grafts remain the main problems in maintaining long-term benefit in patients who have undergone CABG surgery. 23 Coronary angiography is an important diagnostic tool for the evaluation of bypass graft patency in patients after CABG presenting with angina or ischemia, and coronary interventions are common practice for bypass graft lesions. 15,18 Periprocedural bleeding has become the most common in-hospital complications associated with PCI and is independently and strongly associated with increased rates of morbidity and mortality. 5,6 Recently, the adoption of TRA for PCI has reduced vascular access site complications and bleeding, especially in the elderly patients, obese, patients with ST-segment elevation MI, and patients receiving glycoprotein IIb/IIIa inhibitors. 24,25 Thus, the popularity of TRA in PCI increased in recent years. However, angiography and intervention of bypass grafts via TRA are technically more complex and challenging even for experienced operators. 17
In the present study, we found that procedure time and radiation dose in the TRA group were comparative with those in the TFA group, except for contrast volume, which is higher in the TRA group, and fluoroscopy time, which is higher in the TFA group. More use of 7F guiding catheter may be the potential reason for more contrast volume used in the TFA group. Previous studies had concerns regarding the prolonged procedure in PCI via TRA, 26,27 which could be explained by a significant learning curve of TRA, 11,28 especially in bypass grafts. However, in the present study, all operators were highly experienced, which indicates that this factor might contribute to shorter procedure time and fluoroscopy time and reduction in radiation dose in PCI of bypass grafts via TRA.
Previous studies have demonstrated that a lower rate of major bleeding and major vascular complications were the major advantages of TRA versus TFA. 6,12,29,30 In the present study, the incidence of BARC type 3 and 5 bleeding (5.5% vs 0%; P = .022) was significantly higher in the TFA group. This contributed mainly to the higher incidence of NACEs in the TFA group. However, the incidence of major vascular complications was not significantly different between the 2 groups. Specifically, 2 patients with radial artery perforation in the TRA group finally crossed over to the TFA group but were still included in the TRA group for the intention-to-treat analysis (see Figure 1), which may explain the insignificance of major vascular complications between the 2 groups. Other reasons that may help explain the insignificance included the relatively small sample size and an overall low incidence of adverse events. Notably, crossover rate was significantly higher in the TRA group (7.5% vs 0%; P = .022), and this was the major reason of the higher procedural failure rate for TRA-PCI. However, with the innovation of intervention technology and the increased experience of interventional cardiologists, this limitation is likely to be overcome by the benefits of a lower rate of bleeding and major vascular events.
Stroke is another controversial variable of interest in terms of the safety of TRA-PCI versus TFA-PCI. Recently, a meta-analysis conducted to determine the safety and efficacy of TRA in the elderly population showed that TRA-PCI for elderly patients is associated with a lower risk of stroke. 31 However, the ACCOAST (from the A Comparison of Prasugrel at PCI or Time of Diagnosis of Non -ST-Elevation Myocardial Infarction study) access substudy published recently suggested an association between TFA-PCI with a reduced risk of procedure-related stroke. 32 In the present study, the incidence of stroke at 1-year follow-up is very low and not significantly different between the TRA and TFA groups. This may be attributed to the small sample size. Large-scale randomized clinical trials are warranted to determine the association of access sites with the risk of stroke.
This study has several limitations. First, it was not a randomized comparison of TRA-PCI and TFA-PCI; all data were retrospectively collected. Second, bypass graft lesions are relatively rare in daily clinical practice, so the small sample size of the present study might be a major reason to cause insignificance between the groups. Notably, as radial occlusion was commonly not assessed after PCI, the vascular complications in the TRA group may be underestimated.
In conclusion, this study demonstrated that PCI via TRA showed comparative feasibility and efficacy in bypass grafts compared with TFA in the hands of experienced operators. The TRA was associated with a lower rate of in-hospital NACE mainly because of lower rates of major bleeding and major vascular complication.
Footnotes
Authors’ Note
Yuxiang Dai and Chenguang Li contributed equally to this manuscript.
Acknowledgments
The authors gratefully acknowledge financial support from the National Natural Science Foundation of China (Grant no 81300095).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant no 81300095).