
Abstract
Cardiac hematological malignancies (CHMs) are rare entities and comprise lymphoma, leukemic infiltration, and extramedullary manifestation of multiple myeloma. The aim of this work is to summarize typical growth patterns, imaging features, and outcome parameters of CHM. Overall, 12 cases from 4 centers were reviewed retrospectively together with 604 cases from the literature. Cardiac hematological malignancies were mainly represented by B-cell lymphoma (70.0%). Other entities were rarer. Almost half of the patients showed involvement of multiple cardiac structures. Most commonly right atrium, right ventricle, pericardium, left atrium, and left ventricle were affected in decreased order of frequency. Cardiac hematological malignancies manifested with 3 growth patterns: intracaval masses, heart wall infiltration, and pericardial effusion. Several subtypes of CHM tended to present with different patterns. Clinical presentation is unspecific—frequent signs were dyspnea (54.6%), arrhythmias (30.5%), and thoracic pain (18.5%). Outcome of CHM is poor with mean survival of 283.6 days for leukemias, 260.1 days for T-cell non-Hodgkin lymphoma (NHL), 217.9 days for B-cell NHL, and 155.5 days for multiple myeloma.
Introduction
Cardiac hematological malignancies (CHMs) are rare entities which comprise B- or T-cell lymphoma, leukemic infiltration, as well as extramedullary manifestations of multiple myeloma. 1,2 Their frequency is lower in comparison to other malignant cardiac tumors, such as metastases or sarcomas. 2
Cardiac hematological malignancies can be divided into primary and secondary meaning that primary cardiac lymphoma occurs without systemic manifestations. 3 Primary cardiac lymphoma is an extremely rare with a frequency of 1.3% of all primary cardiac tumors 4 and 0.5% of all lymphomas. 5 Compared with primary cardiac lymphoma, secondary cardiac involvement in malignant lymphoma is more common. 6 Histologically, most of cardiac lymphomas are B-cell manifestations. 3 –6 Additionally, it might be emphasized that immunodeficiency is an important risk factor, especially for primary cardiac lymphoma. 7,8
Echocardiography is frequently used for imaging of CHM. As in general for cardiac tumors, more complex tumor manifestations can be evaluated by further combination with computed tomography (CT) and/or magnetic resonance imaging (MRI). This combined imaging provides excellent anatomic orientation and is therefore useful in preoperative planning. 9 Publications on imaging features of CHM are rare so far consisting of only limited amount of patients.
The aim of this work is to assess typical growth patterns, imaging features, and clinical outcome parameters of CHM by: (1) reviewing our own cases of CHM and (2) reviewing published cases from the literature.
Methods
Data Acquisition and Patients
Figure 1 shows the data acquisition in this study. First, the databases of 4 radiological departments at university hospitals were screened for CHMs. Overall, 12 cases of CHM were identified. Second, PubMed database was screened for reports regarding CHM using the following search words: “heart lymphoma” (4158 articles), “cardiac lymphoma” (5159 articles), “heart leukemia” (3511 articles), “cardiac leukemia” (4488 articles), “heart plasmacytoma” (99 articles), and “cardiac plasmacytoma” (118 articles). Inclusion criteria were report of 2 and more features of CHM, such as diagnosis, localization, clinical signs, imaging findings, and survival. Furthermore, only publications in English language were included. Other cases were excluded from the analysis. Secondary references were also analyzed. After a thorough analysis of the data, 604 patients were identified. Therefore, our analysis comprised 616 cases of CHM.
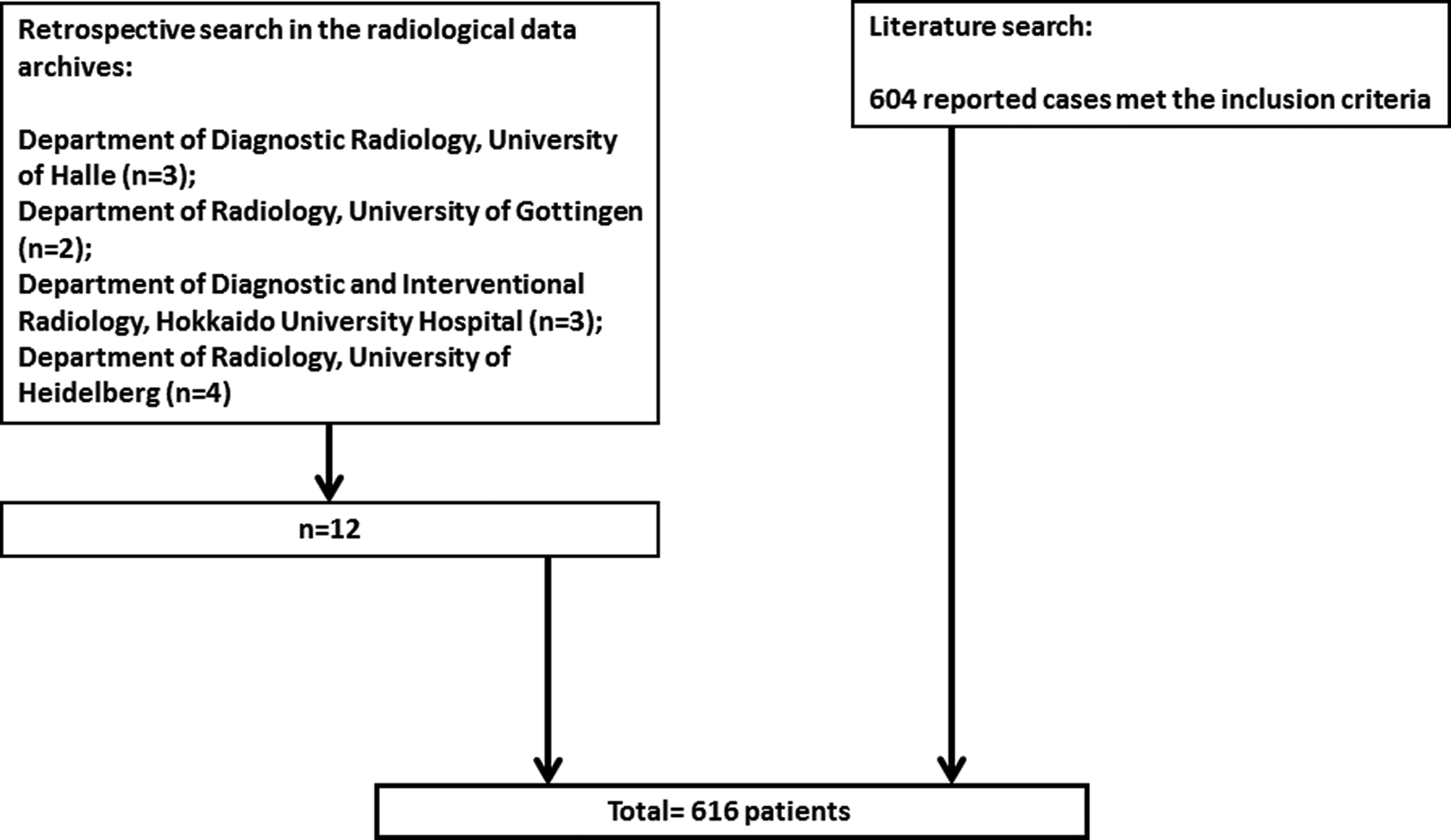
Patient acquisition and search strategy.
Statistical Analysis
Collected data were analyzed using descriptive statistics (absolute and relative frequencies). Continuous variables were expressed as mean (standard deviation) and categorical variables as percentages. Patterns and localizations of different CHM were analyzed by χ2 test. Significance level was P < .05 and was adjusted for multiple testing using the Bonferroni correction.
Results
Demographic Data and Hematological Malignancies Affecting the Heart
Table 1 shows demographic data of the patients. The majority of them were male (63.8%). The mean age of the patients was 55.7 ± 19.1 years, median age 59 years, range 1-90 years. Cardiac hematological malignancies occurred more often in age groups over 50 years (Table 1) and was rare in patients under 30 years.
Age and Gender Distribution of the Identified Patients With Cardiac Involvement in Hematological Malignancies.
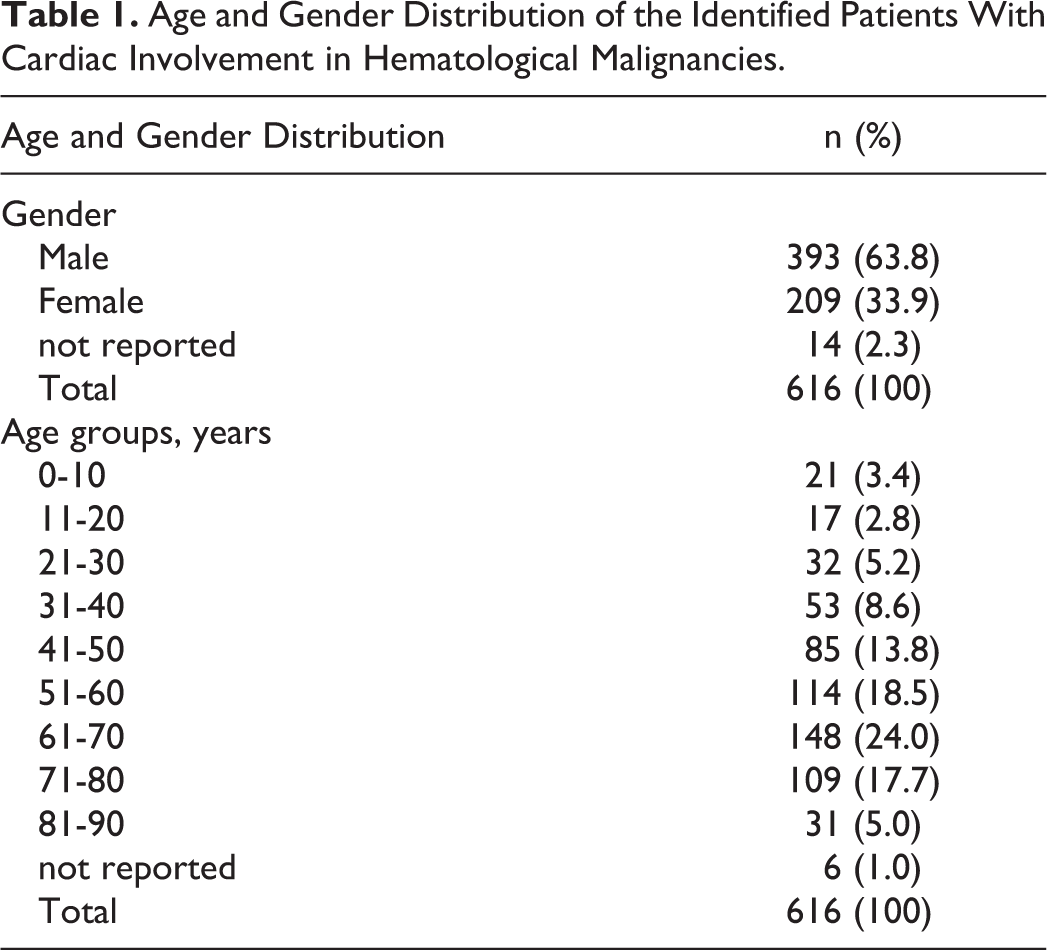
Table 2 summarizes the diagnoses of CHM in the patients. B-cell non-Hodgkin lymphoma (NHL) was diagnosed most frequently (70.0%). Other CHMs were rare (Table 2). Cardiac involvement in T-cell NHL occurred in 11.7%, in plasmacytoma or myeloma in 6.3%, and in different leukemias in 3.1%. There were no cases of Hodgkin disease affecting the heart. Of the cases with B-cell NHL, more often diffuse large B-cell lymphomas occurred.
Hematological Malignancies Affecting the Heart.
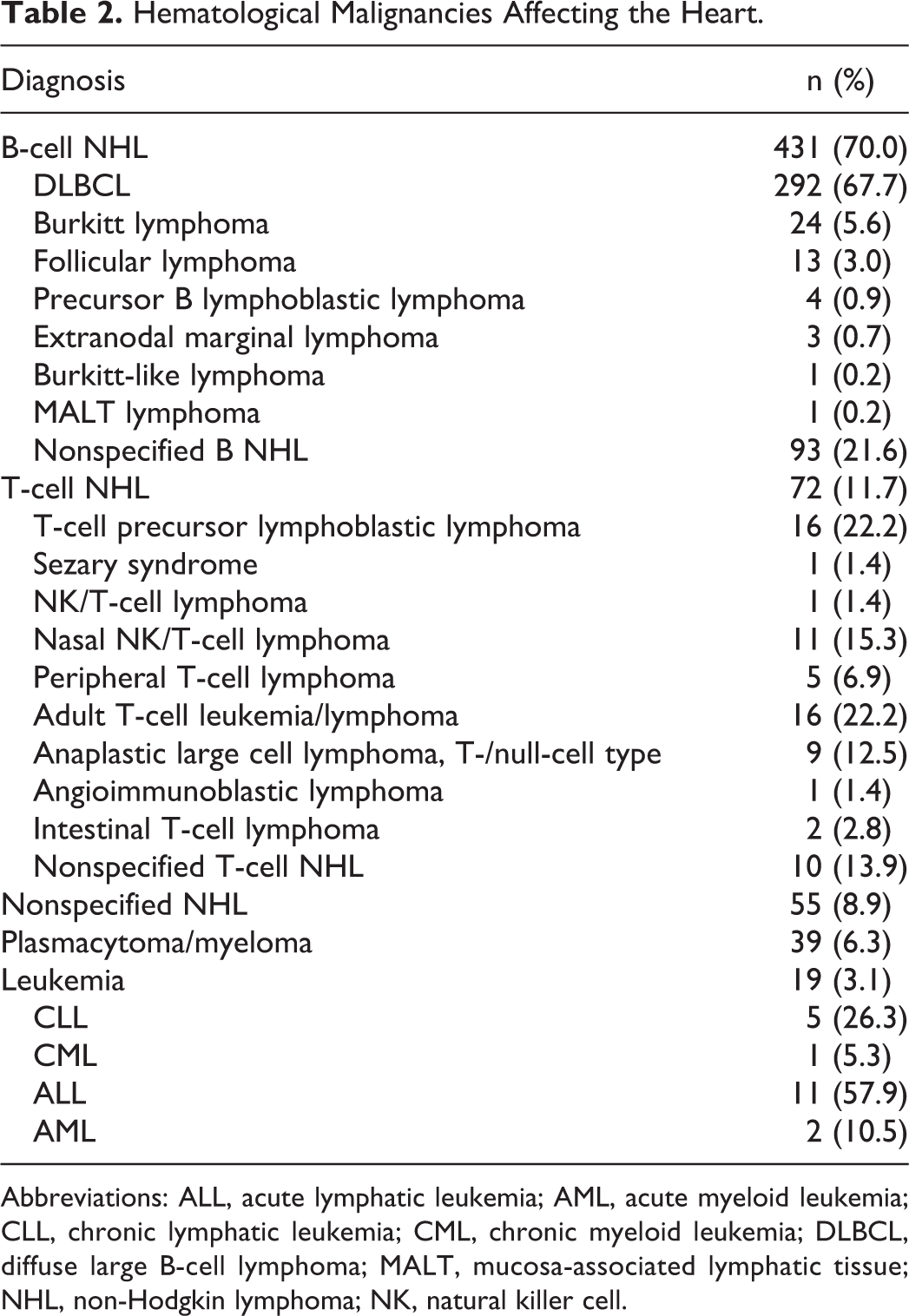
Abbreviations: ALL, acute lymphatic leukemia; AML, acute myeloid leukemia; CLL, chronic lymphatic leukemia; CML, chronic myeloid leukemia; DLBCL, diffuse large B-cell lymphoma; MALT, mucosa-associated lymphatic tissue; NHL, non-Hodgkin lymphoma; NK, natural killer cell.
Among the reported cases, primary CHM occurred in 417 (67.7%) and secondary heart involvement in generalized diseases in 134 (21.7%) cases. In 65 (10.5%) patients, the information regarding primary or secondary cardiac affection by hematological malignancies was not available.
Clinical Signs of CHM
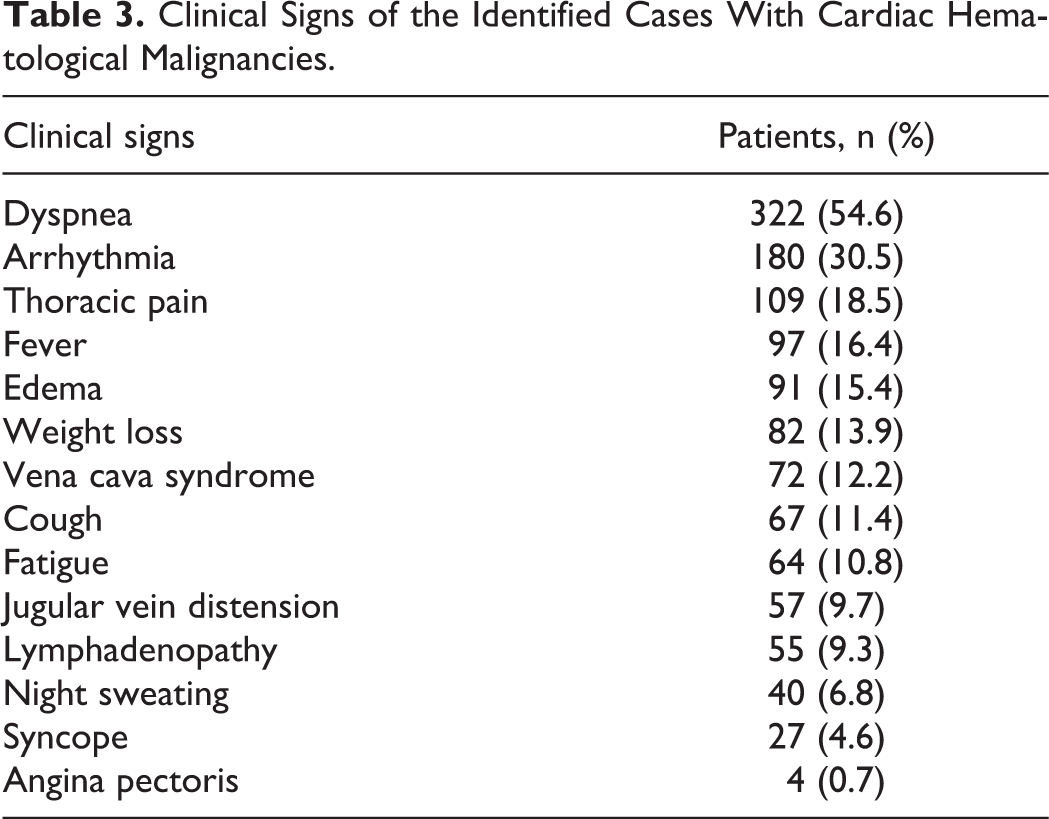
Clinical signs of CHM were available for 590 patients. Cardiac hematological malignancies presented with a broad spectrum of symptoms (Table 3). Most frequently, dyspnea (54.6%), followed by arrhythmias (30.5%), thoracic pain (18.5%), fever (16.4%), edema (15.4%), and other symptoms were rare.
Clinical Signs of the Identified Cases With Cardiac Hematological Malignancies.
Localization and Pattern of CHM
In 307 (49.8%) patients, 1 anatomical heart structure was affected by CHM, whereas in 268 (43.5%) patients, ≥2 structures were involved (Table 4). Localization of CHM was not available for 41 cases from the literature. In detail, more commonly the right atrium, right ventricle, pericardium, left atrium, and the left ventricle were affected in decreasing order of frequency.
Localization of Cardiac Hematological Malignancies.
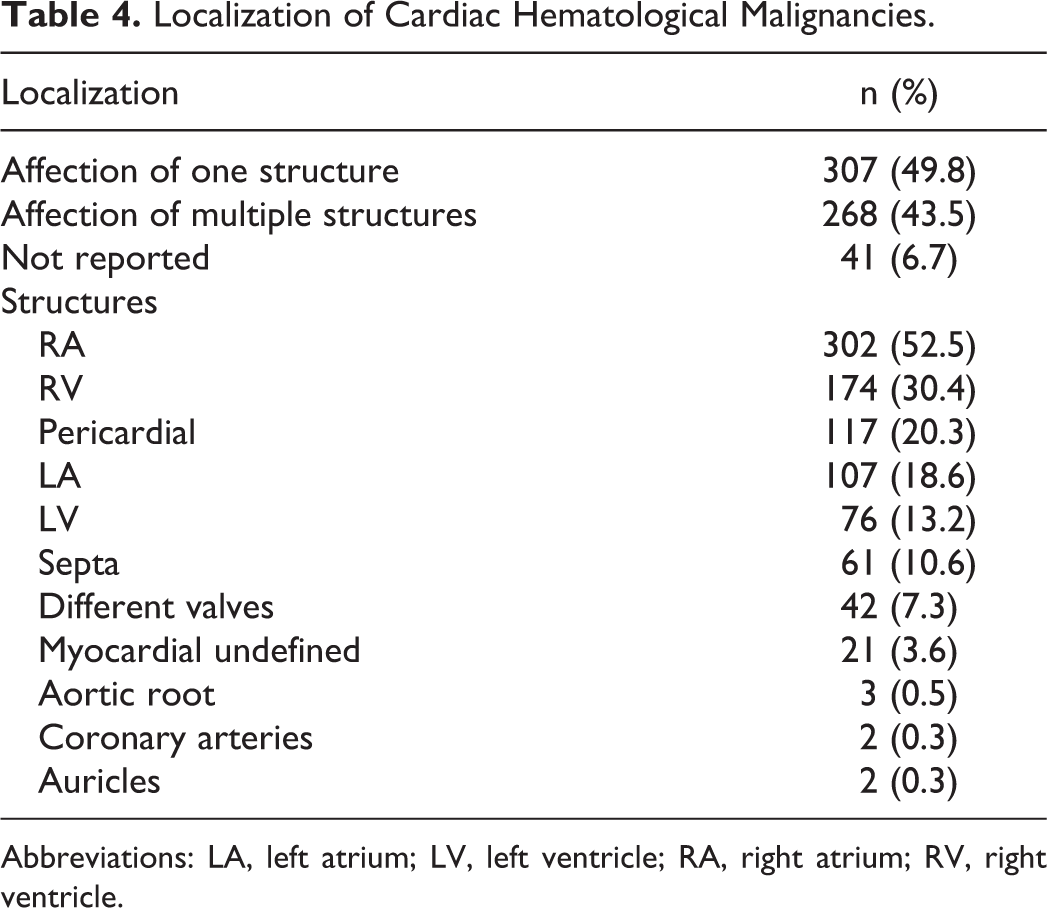
Abbreviations: LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
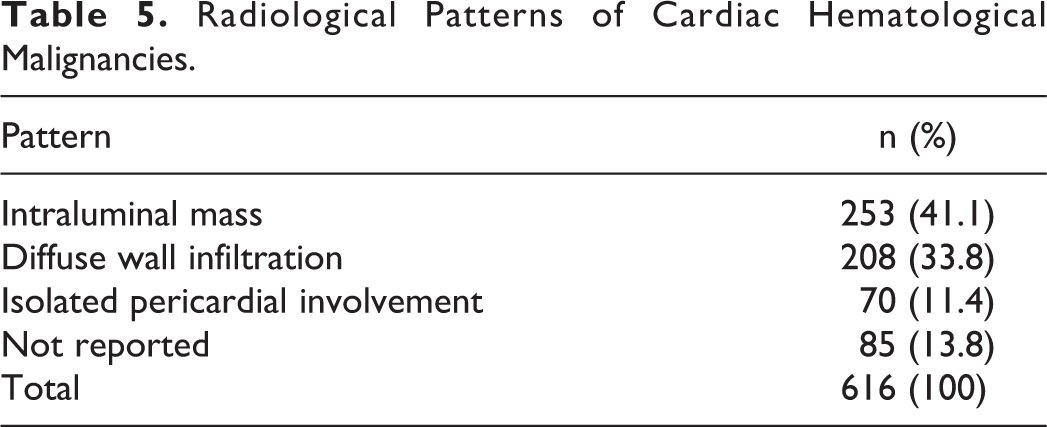
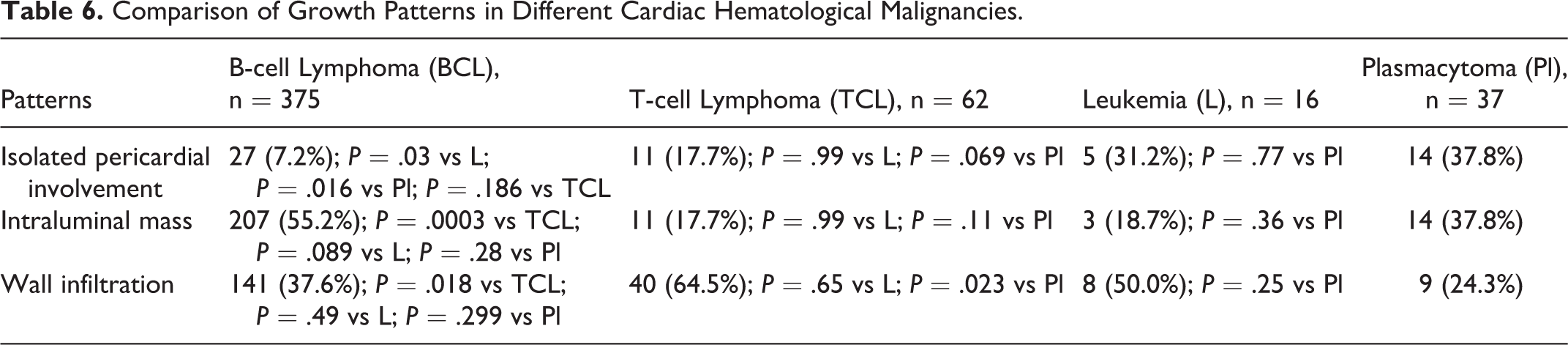
Patterns of heart involvement in hematological malignant diseases were categorized as follows: isolated affection of the pericardium, intracaval mass, and diffuse heart wall infiltration. More often, intracaval masses occurred (Table 5). Cardiac hematological malignancies subtypes presented with different patterns (Table 6). Isolated pericardial involvement was seen frequently in T-cell lymphomas and leukemias and rarely in B-cell lymphoma. Furthermore, B-cell NHL manifested more often as intracaval masses.
Radiological Patterns of Cardiac Hematological Malignancies.
Comparison of Growth Patterns in Different Cardiac Hematological Malignancies.
Imaging Features of CHM
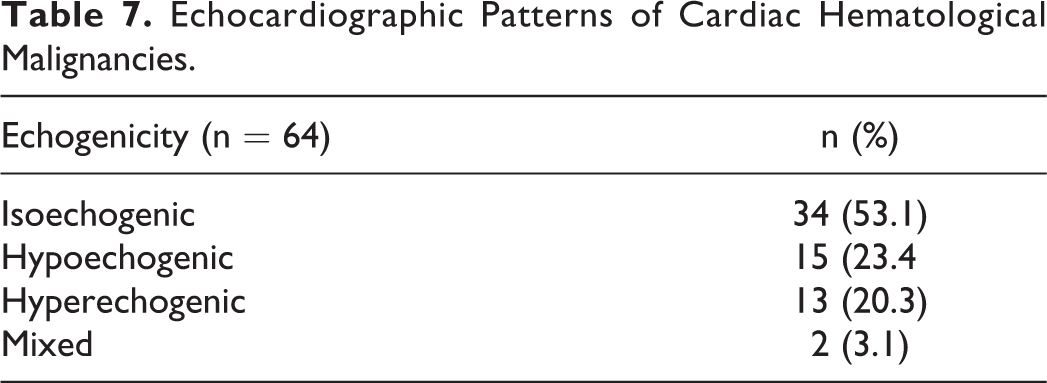
Imaging features were available for a small group of patients with CHM. On echocardiography, most CHM presented with an isoechogenic texture (Figure 2). Hypoechogenic and hyperechogenic patterns occurred rarely (Table 7).
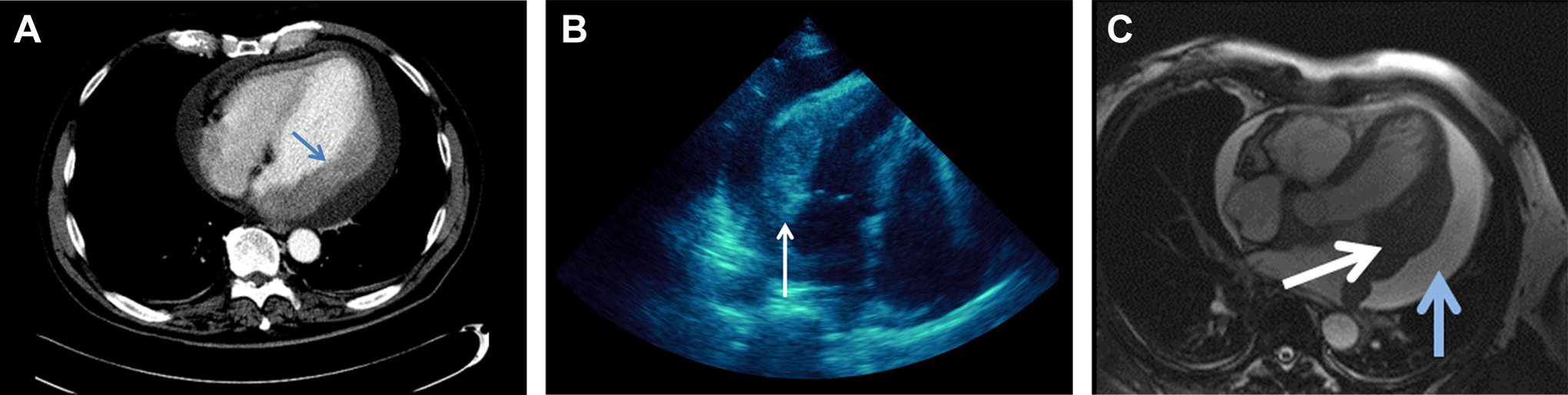
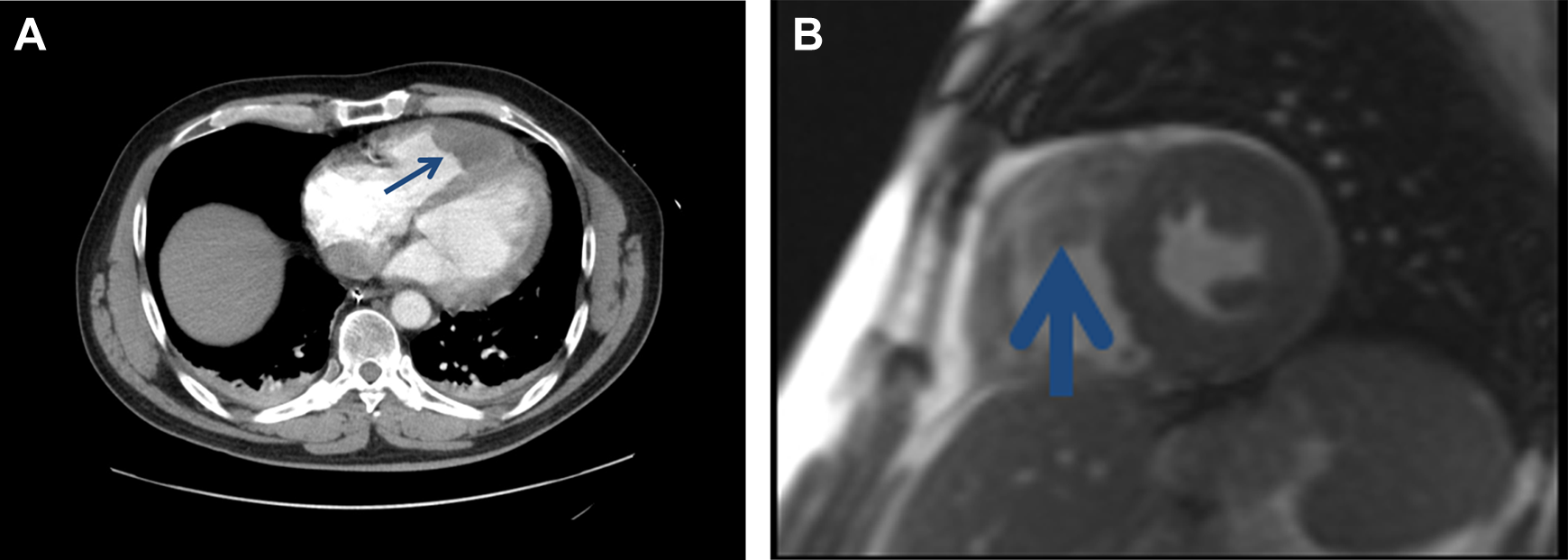
Imaging findings of a diffuse large B-cell lymphoma affecting the left ventricle. A, Contrast enhanced computed tomography of the chest shows an enlargement of the lateral wall (arrow) of the left atrium and ventricle. Additional pericardial effusion is also seen. B, On ultrasound the lesion is homogenous isoechoic in comparison with the myocardium. C, Same lesion on T2-weighted MRI with isointense signal (white arrow). Good delineation of the pericardial effusion (blue arrow). MRI indicates magnetic resonance imaging.
Echocardiographic Patterns of Cardiac Hematological Malignancies.
On CT without contrast medium, most CHM (72.92%) were hypodense (Table 8). After intravenous administration of contrast medium, they showed a moderate enhancement (Figures 2 –4).
Computer Tomographic Imaging Findings of Cardiac Hematological Malignancies.
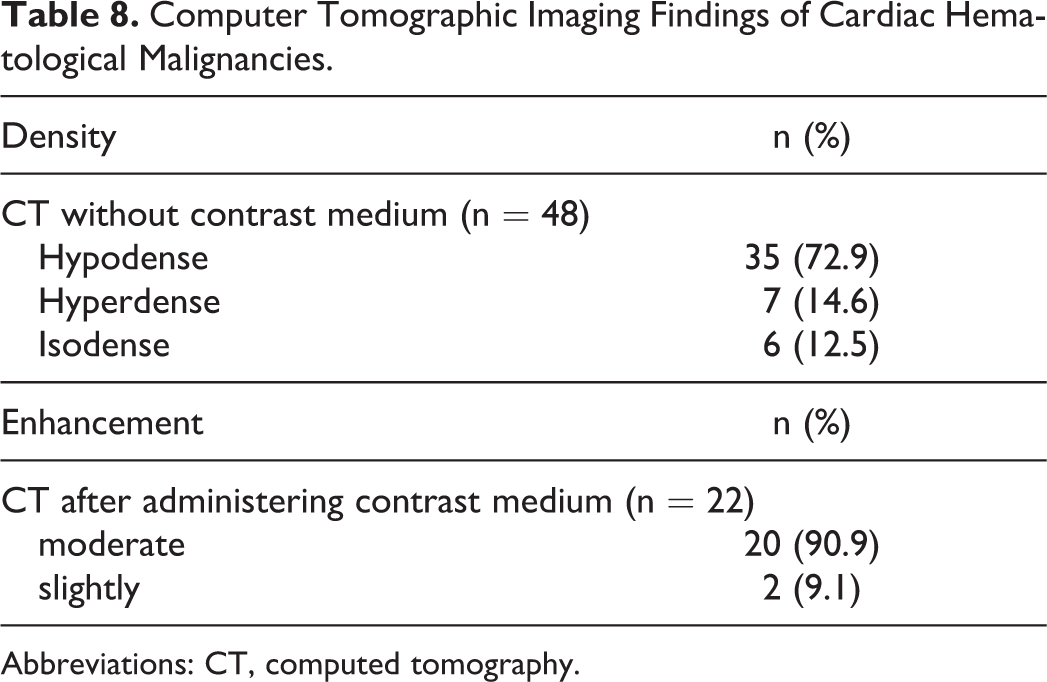
Abbreviations: CT, computed tomography.
Imaging findings of an intracardial lymphoma presenting as a caval mass. A, Contrast enhanced computed tomography of the chest documents a homogenous isodense mass within the right ventricle. B, Same lesion on contrast enhanced T1-weighted magnetic resonance imaging. Histopathological analysis (not shown) after a catheter-guided biopsy confirmed the diagnosis of a diffuse large B-cell lymphoma.
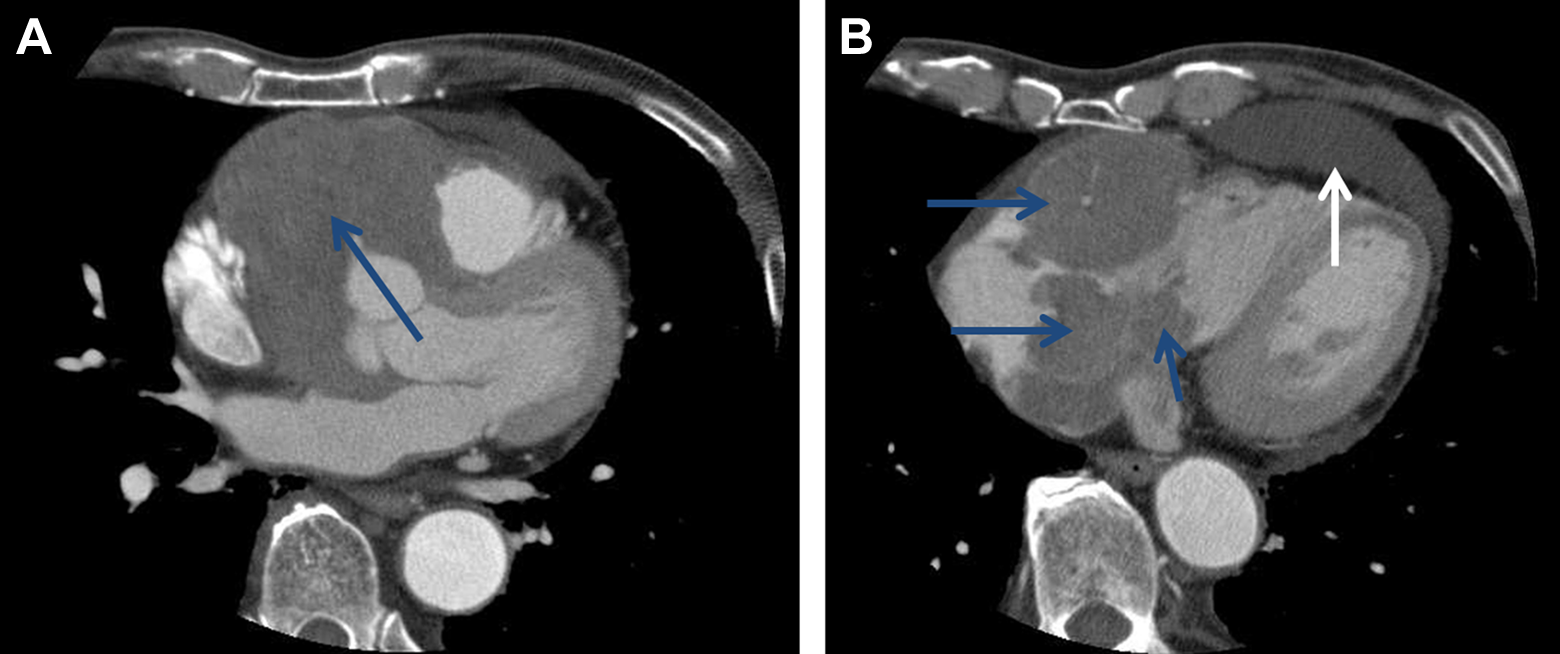
Intracardial lymphoma presenting as a caval mass. A, Contrast-enhanced computed tomography of the chest shows large inhomogeneous masses within the right atrium with infiltration of the adjacent walls (blue arrows). B, Additional slightly hyperdense pericardial effusion is also seen (white arrow).
On MRI, on T2-weighted (T2w) images, 75% of CHMs were hyperintense (Table 9). On T1-weighted (T1w) images, CHMs were predominantly hypointense or isointense and all tumors enhanced contrast medium after intravenous administration (Figure 2).
Magnetic Resonance Imaging Findings of Cardiac Hematological Malignancies.
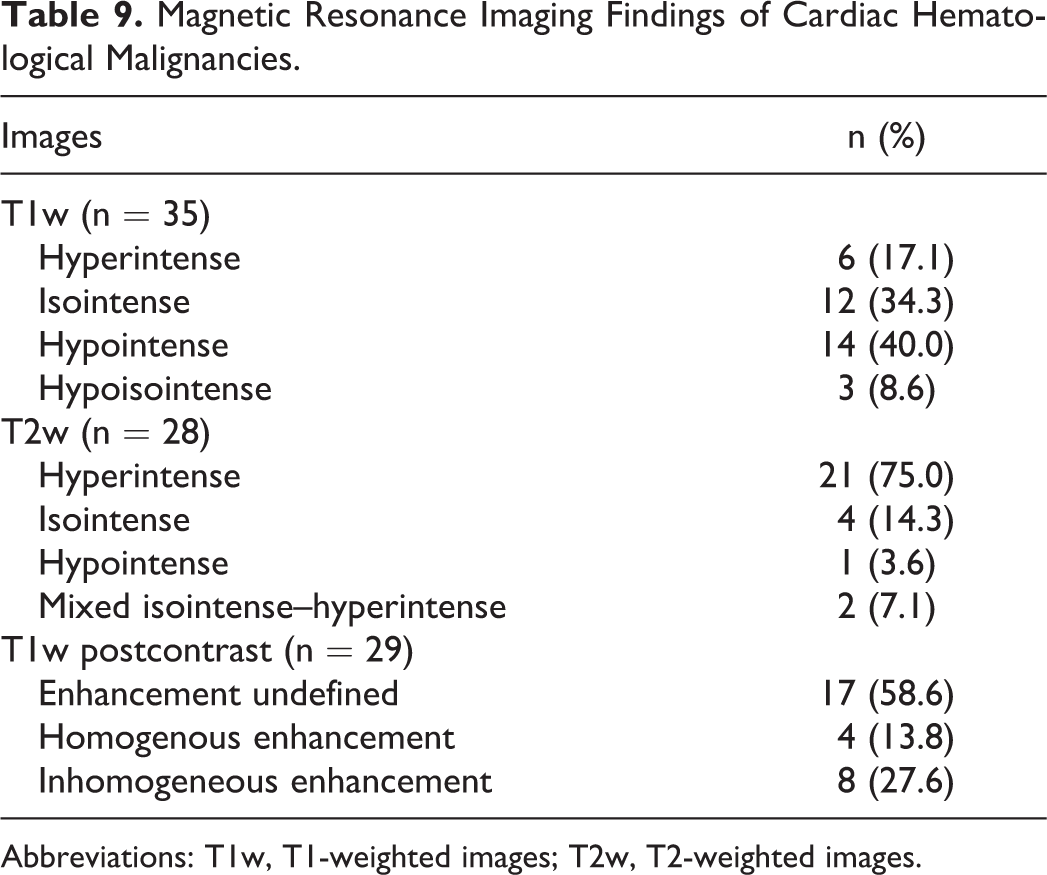
Abbreviations: T1w, T1-weighted images; T2w, T2-weighted images.
Therapy and Outcome of CHM
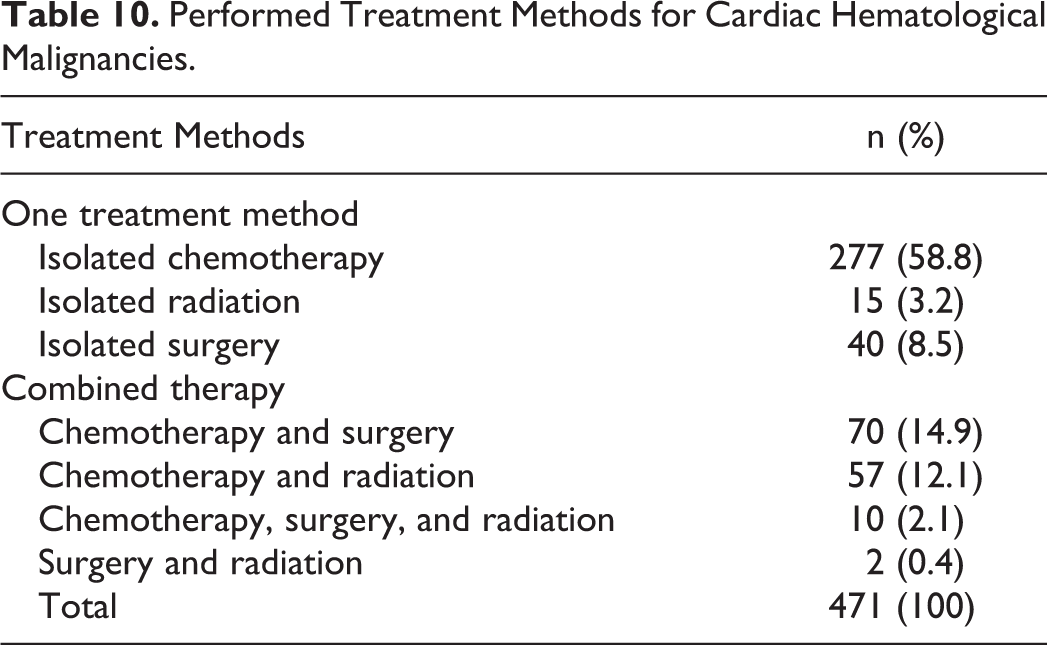
Treatment information was available for 471 cases. The identified patients underwent different therapies (Table 10). In most cases (n = 332, 70.5%), 1 treatment method, that is, isolated chemotherapy or surgery or radiation, was administered. Thereby, more often systemic chemotherapy (n = 277, 58.8%) was administered. In 139 (29.5%) patients, several treatment methods were combined. Most frequently, a combination of chemotherapy and surgery or chemotherapy and radiation was performed.
Performed Treatment Methods for Cardiac Hematological Malignancies.
Information regarding survival was available for 251 patients. Overall, the survival time was 215 days. In detail, the mean survival was 283.6 days for leukemias, 260.1 days for T-cell NHL, 217.9 days for B-cell NHL, and 155.5 days for plasmacytoma (Table 11). The survival time in relation to cardiac affection pattern is shown in Table 12.
Survival Time of Different Cardiac Hematological Malignancies.
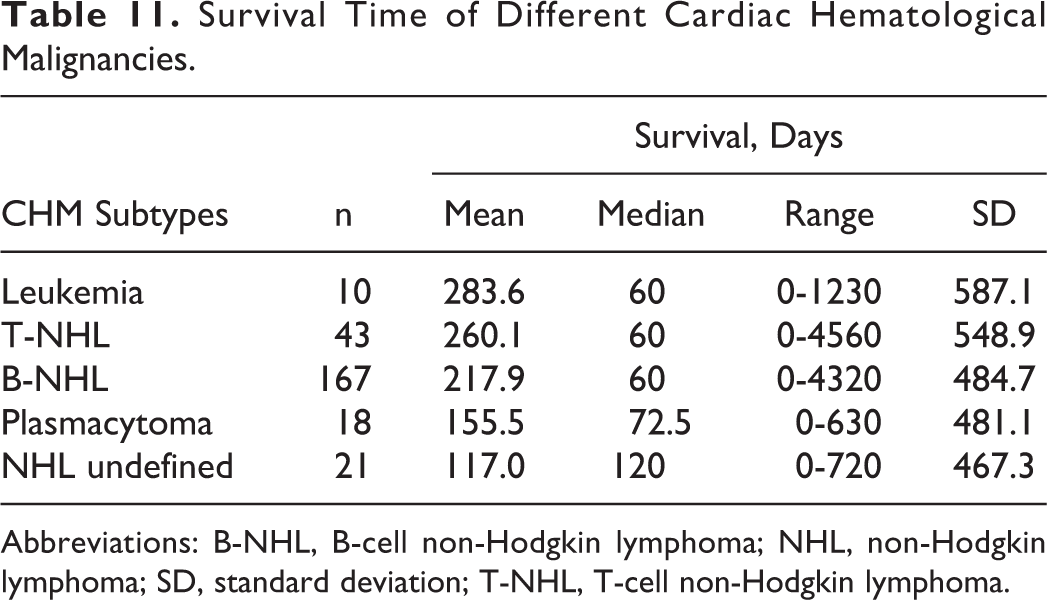
Abbreviations: B-NHL, B-cell non-Hodgkin lymphoma; NHL, non-Hodgkin lymphoma; SD, standard deviation; T-NHL, T-cell non-Hodgkin lymphoma.
Survival Time in Different Patterns of Cardiac Hematological Malignancies.
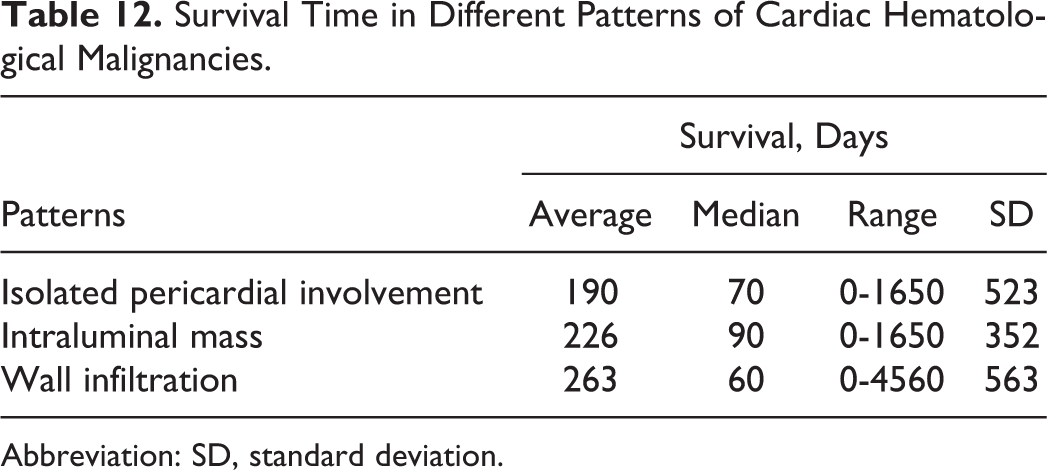
Abbreviation: SD, standard deviation.
Discussion
Most frequent cardiac malignancies are cardiac metastases and sarcomas. 2,10 Data on primary CHM are exceptionally rare so far and mainly comprise case reports and small case series on cardiac lymphoma. To the best of our knowledge, the current work is the largest summary of data on growth patterns, imaging features, clinical signs, and outcome of patients with CHM.
Our results revealed CHM to occur frequently in patients older than 50 years and rare in young patients. This is in accordance with data from previous literature; in the study of Miguel et al, 11 the average age of patient with CHM was 48 years, which is conclusive with an older autopsy series. 12 In contrast, patients with cardiac manifestation of multiple myeloma tend to be older with a mean age of 62 years. 13
Among the reviewed cases, we have a clear overrepresentation of primary cardiac lymphomas over secondary cardiac involvement in generalized disease. We assume this is due to selection bias as the epidemiologic literature on cardiac lymphoma concurrently describes secondary cardiac lymphoma to be much more frequent compared with primary cardiac lymphoma. 14,15 Up to 24% of patients with systemic lymphoma were suspected to have secondary cardiac involvement. 12 Undoubtedly, B-cell lymphoma was most frequent entity of CHM and represented approximately 70% of the reviewed cases. This fact has already been underlined in previous publications. 5,11 Other lymphoma subtypes, such as cardiac T-cell lymphoma, occurred rarely. 16 Our evaluation confirmed this finding. Even less frequent were leukemia and cardiac plasmacytoma.
As demonstrated within the results, CHM tended to involve pericardial structures. This explains the frequent observation of pericardial effusions in patients with CHM as described in previous publications. 7,11,14,17 They may occur in up to 17% of patients with cardiac lymphoma. 12 As a very rare cause of malignant (among others pericardial) effusion, the “primary effusion lymphoma” has been described in patients with human immunodeficiency virus and associated infections. 18,19 The frequent appearance of pericardial effusion may be of high relevance as it allows for confirmation of cardiac lymphoma by effusion cytology 5 which is diagnostic in roughly two-third of patients. 20 Some authors already advised to always consider cardiac lymphoma in case of unexplained pericardial effusions. 8,11
Furthermore, we demonstrated that CHM tended to occur in the right heart, especially the atrium. 8,14 Additionally, approximately 50% of the analyzed CHM infiltrated >1 cardiac structure. Referring to Shanmugam, this can be seen as a general aspect in the differentiation between malignant and benign cardiac tumors. 20,21 Roberts et al 12 mentioned that valve involvement was rare in CHM. Other tumors may be distinguished from CHM by different morphology and growth patterns. In contrast to CHM, common benign cardiac tumors, for example, myxoma, rhabdomyoma, and fibroma are more commonly found in the left heart. 22 Differentiation from other primary cardiac tumors can be more challenging. Given the infrequent valve infiltration of CHM, this might be seen as a criterion in the discrimination from rhabdomyosarcoma, which frequently involves valves. 20
Imaging is one of the basic instruments for the diagnosis of CHM. Due to availability, echocardiography is mostly the first step in imaging and allows the initial detection of cardiac masses. However, it may miss extracardiac tumor infiltration and is highly dependent on the experience of the operator. Therefore, modern electrocardiogram-gated cardiac CT offers imaging with excellent spatial resolution, exact evaluation of vascular involvement but requires radiation anyway. By its soft tissue contrast, MRI is able to exactly delineate the soft tissue extent of cardiac tumor masses. In synopsis of our own cases and the literature, CHM usually presented as ill-defined infiltrative hypodense to isodense masses with moderate enhancement on CT images. On MRI, they were most commonly isointense to hyperintense on T2w and hypointense to isointense on T1w with heterogeneous enhancement.
Our analysis showed that CHM presented with unspecific clinical signs. Moreover, they can be caused by radiochemotherapy. 23 Therefore, clinical manifestation of CHM can be underestimated and the diagnosis of heart affection can be delayed.
Overall survival time in patients with CHM was <1 year (215 days). In agreement with this observation, a couple of other publications have already emphasized the poor survival in patients with primary cardiac lymphomas. 24 This is most likely due to the unspecific clinical presentation of CHM and therefore difficult diagnosis. 16 Frequently the diagnosis of CHM is made at necropsy. 16 On the other hand, early diagnosis of CHM could probably enhance survival in affected patients.
Conclusions
Cardiac hematological malignancies are rare entities. Due to their preference of right heart structures, sparing of cardiac valves, and pericardial involvement, they can be distinguished from other cardiac tumors, such as cardiac sarcomas or metastases.
Cardiac hematological malignancies can manifest with 3 growth patterns: intracaval masses, heart wall infiltration, and isolated pericardial effusion. Combination of the patterns is also possible. Several subtypes of CHM tend to present with different patterns. As emphasized within previous publications, CHM should be considered in any cases of otherwise unexplained pericardial effusion. Due to unspecific clinical presentation, diagnosis of CHM is often late and therefore accounts for the poor prognosis.
Footnotes
Authors’ Note
All authors contributed to conception and design, acquisition of data, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.