
Abstract
Radial access for primary percutaneous coronary intervention (pPCI) in patients with ST-elevation acute myocardial infarction (STEMI) is recommended in high-volume experienced centers. This study investigated whether radial access for pPCI is safe even in a low-volume center. We performed radial access for pPCI in 171 patients. Major adverse cardiac events (total death, myocardial infarction, stroke) rate was 1.2%. The overall incidence of bleeding complications was 2.4%; there was no vascular complication at the access site. In patients with STEMI undergoing pPCI, the results of radial access in a low-volume center were acceptable. These findings support the safety of radial access in patients with STEMI.
Keywords
Introduction
Early reperfusion by percutaneous coronary intervention (PCI) in patients with ST-elevation acute myocardial infarction (STEMI) is the preferred therapy to optimize clinical outcome. 1 However, bleeding events following PCI remain a problem and are independently and strongly associated with adverse outcomes. 2 –4 In patients with STEMI, emergent PCI and aggressive antiplatelet and antithrombotic therapy are required; hence, bleeding complications remain an important issue.
Compared with femoral access, radial access reduces mortality and major adverse cardiac events (MACEs), with reductions in major bleeding and vascular complications across the entire spectrum of patients with coronary artery disease. 5 In patients with STEMI, a meta-analysis of randomized controlled trials suggested that radial access is associated with favorable outcomes and should be the preferred approach for experienced radial operators. 6 The current European Society of Cardiology and European Association for Cardio-Thoracic Surgery guidelines recommend the radial approach in patients with STEMI as the preferred method of access, as it has been shown to reduce the incidence of acute bleeding events, and was associated with lower mortality, depending upon the operators’ expertise. 7 However, these previous results were reported by experienced operators in high-volume centers. Owing to Japan’s geography and number of hospitals, many low-volume centers manage ≤200 PCI cases/year. During the study period, our hospital was a low-volume center, performing 150 to 200 PCI cases a year (approximately 50 emergency PCI cases a year for acute coronary syndrome). The physicians working in the cardiovascular department included 1 cardiologist (10 years of experience) and 2 residents (3-5 years of experience) during 2009 to 2014, and 3 cardiologists (1 with 16 years and 2 with 9 years of experience) and 2 residents (3-5 years of experience) since 2015. As our center did not have an intensive care or coronary care unit, mechanical support including respirator, intra-aortic balloon pump, and extracorporeal membranous oxygenation support were provided in a general ward.
In the present study, we evaluated primary percutaneous coronary intervention (pPCI) performed by radial access in our center for STEMI cases, aiming to investigate its safety in a low-volume center.
Method
From March 2009 through July 2016, a total of 217 patients with STEMI underwent pPCI within 24 hours of symptom onset. In order to evaluate the same items as the STEMI-RADIAL trial, 8 31 patients with Killip-4 were excluded. An additional 15 patients were excluded, in which femoral access was used, based on the operator’s determination that the radial artery was small or nonpalpable. Thus, the present study was conducted with 171 subjects who underwent pPCI for STEMI by radial access (Figure 1). Written informed consent was obtained from all patients in the emergency room immediately prior to the procedure.
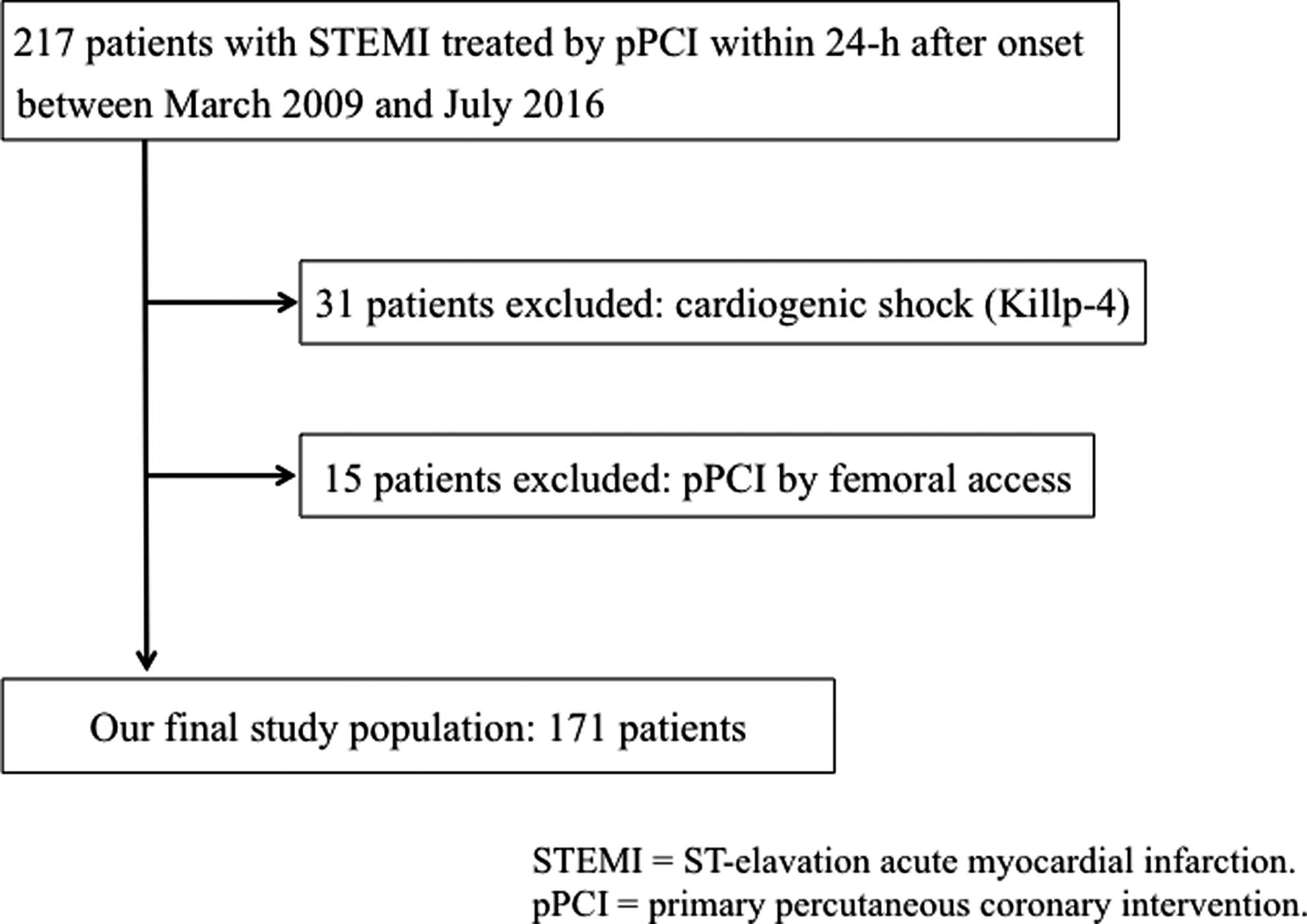
Entry flowchart.
The diagnosis of STEMI was made with (i) continuous chest pain lasting >30 minutes, (ii) ST elevation >1.0 mm in 2 or more contiguous precordial ECG leads, and (iii) elevation of cardiac biomarkers including creatine kinase, creatine kinase myocardial fraction, or troponin I. Patients were premedicated with aspirin (162 mg orally) and brought to the catheter laboratory. Unfractionated heparin (8000 IU) was administered intravenously during the procedure. The approach site and individual PCI strategy were at the operator’s discretion, although radial access is usually the first choice. As a rule, PCI is performed by a resident as the operator and a cardiologist as an assistant who directs the operator. Basic procedures were as follows: (i) the guide wire was advanced across the target lesion, (ii) thrombectomy was performed for thrombolysis in myocardial infarction (TIMI) flow grade 0 or 1, (iii) plain balloon angioplasty was performed with a 2.0-mm balloon, and (iv) a stent was implanted under intravascular ultrasonography guidance. After the procedure, clopidogrel 300 mg was administered orally at the earliest possible time, and unfractionated heparin (15 000 IU/day) was administered by a 48-hour continuous drip. The vascular sheath was removed at the end of the procedure, and hemostasis was achieved by a compressive device (BLEED SAFE; Medikit, Tokyo, Japan). Hemostasis was performed with 15 mL of air during the first 2 hours, the pressure was reduced 3 times, by 2 mL each time, at 2-hour intervals. Hemostasis was performed for a total of 8 to 10 hours.
We collected data for the following variables: MACEs (defined as a composite of death, myocardial infarction [MI], and stroke) at 30 days, major bleeding events, access site complications, technical success, procedural times including door-to-balloon time and artery puncture-to-balloon time, fluoroscopy time, and contrast volume. The definition of major bleeding was based on the HORIOZONS-AMI criteria, 9 and a hematoma >15 cm was defined as a major bleeding event according to the STEMI-RADIAL trial. 8 Access site complications were defined as pseudoaneurysms requiring closure, peri-procedural access site bleeding requiring anticoagulation reversal, arteriovenous fistulas, and radial artery occlusion requiring surgical or percutaneous intervention. Technical success was defined as the adequate dilatation of a culprit lesion (residual stenosis <50%), final TIMI flow grade 3, and no evidence of procedural complications.
Statistical Analysis
Our results are based on descriptive statistics, and the results from STEMI-RADIAL trial are shown as reference values in the figures. Data are expressed as mean (SD).
Results
Between March 2009 and July 2016, 171 patients with STEMI were treated by radial access pPCI in our hospital. Baseline characteristics of subjects are shown in Table 1. Average age was 71.0 (10.9) years (range: 44-92 years), and 73% of patients were male. Approximately 60% of patients were in Killip class 1, 56% had multivessel disease, 32% had diabetes, 9.9% had previous MI, and 11% had a history of stroke. Procedural characteristics are summarized in Table 2. The technical success rate was 98%. The rate of crossover to femoral from radial access was 0.6%. A 6-F guide catheter was used in 98% of patients. Final TIMI flow grade 3 was present in 98% of patients, and slow flow or no-reflow phenomenon occurred in 2%. Door-to-balloon time was 69.4 (25.6) minutes and puncture-to-balloon time was 20.1 (7.8) minutes. Contrast volume was 136.5 (43.7) ml. The rate of radial artery occlusion, evaluated by palpitation, was 0%.
Patient Characteristics.a
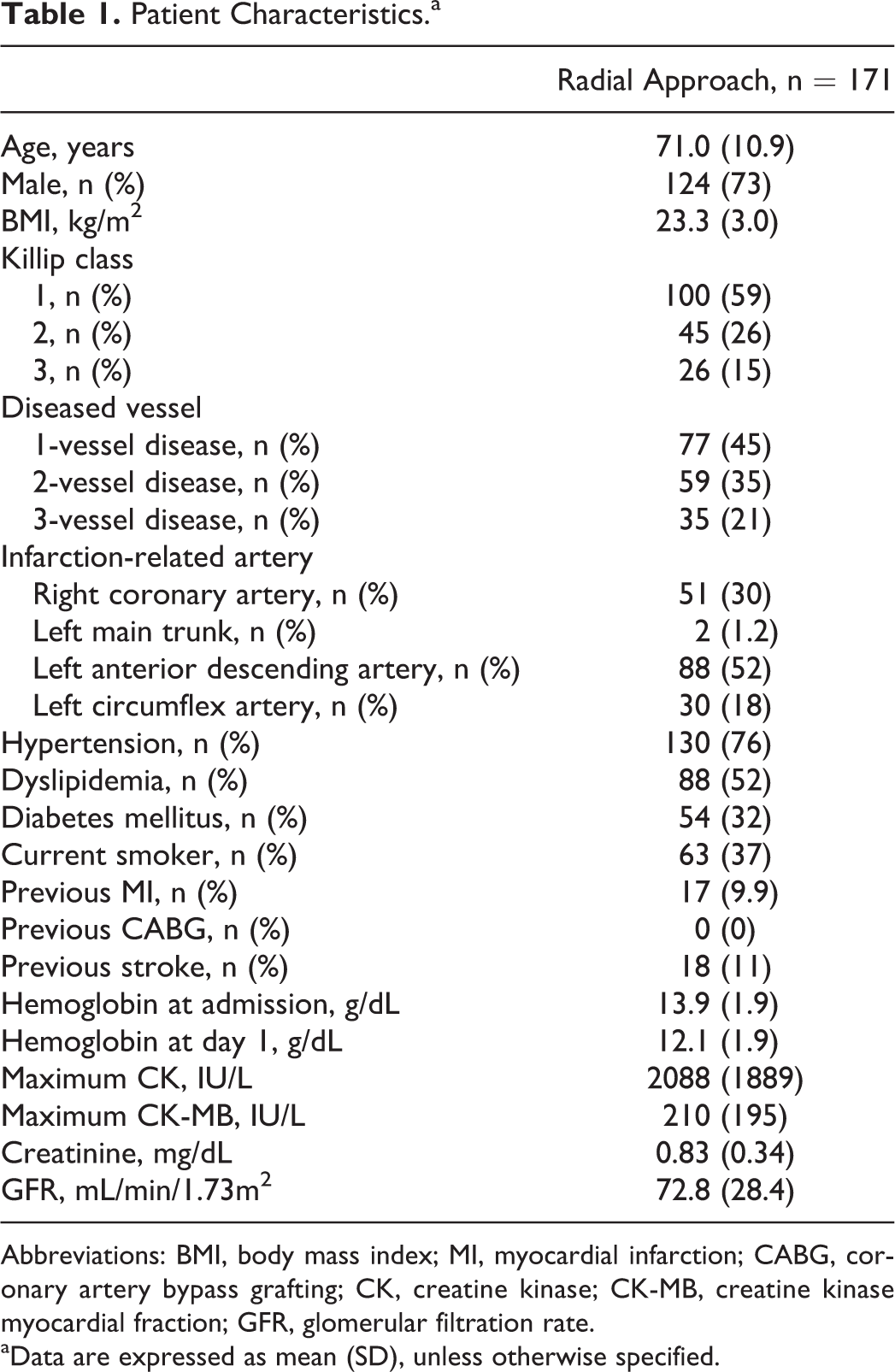
Abbreviations: BMI, body mass index; MI, myocardial infarction; CABG, coronary artery bypass grafting; CK, creatine kinase; CK-MB, creatine kinase myocardial fraction; GFR, glomerular filtration rate.
aData are expressed as mean (SD), unless otherwise specified.
Procedural Characteristics.a
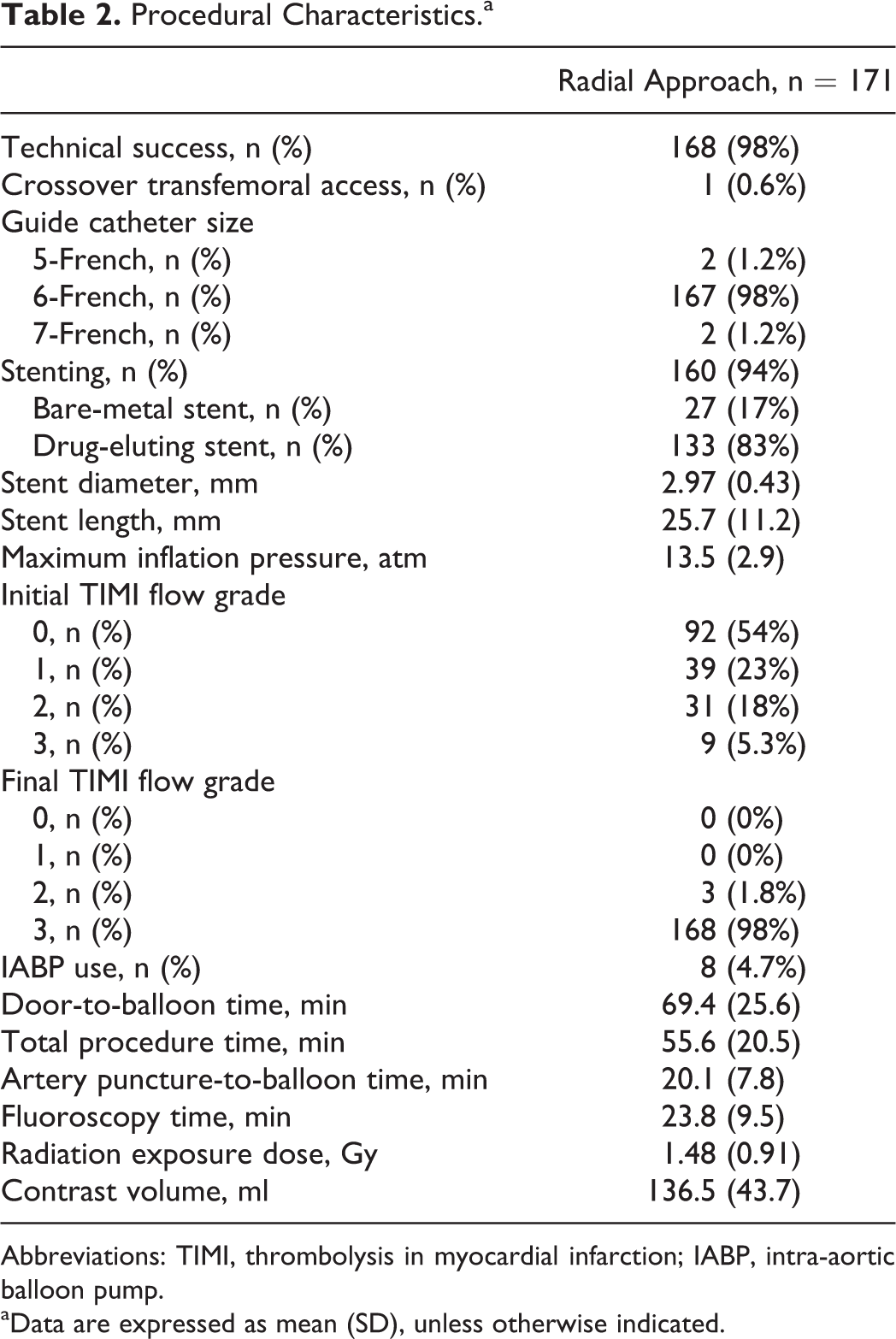
Abbreviations: TIMI, thrombolysis in myocardial infarction; IABP, intra-aortic balloon pump.
aData are expressed as mean (SD), unless otherwise indicated.
Clinical outcomes are shown in Figures 2 and 3, with results of the STEMI-RADIAL trial for reference. Total MACE at 30 days was 1.2% in our study: 2 patients, both were >75 years old, died suddenly because of rupture of left ventricular free wall on day 3 after pPCI. Major bleeding events occurred in 2.4%: 1 patient required blood transfusion due to gastrointestinal bleeding, and 3 had a decrease in hemoglobin level of >4 g/dL without an overt bleeding source (1 of 3 patients required blood transfusion). The rate of access site complications was 0% in our study.
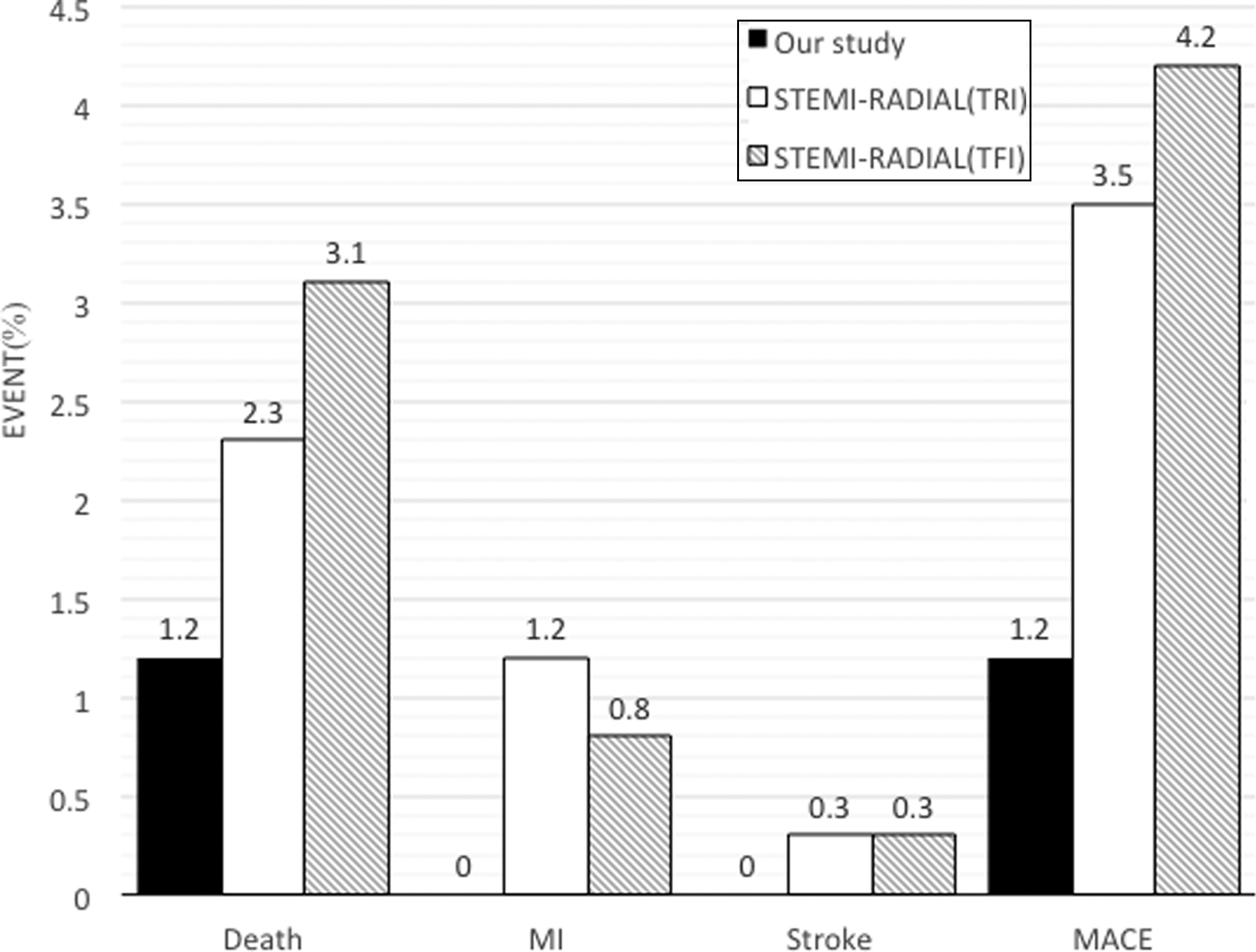
Clinical outcomes. MACE rate was 1.2% in our study; 2 patients died because of blow-out rupture. STEMI-RADIAL results are shown as reference values. MI indicates myocardial infarction; MACE, major adverse cardiovascular events; TRI, transradial intervention; TFI, transfemoral intervention.
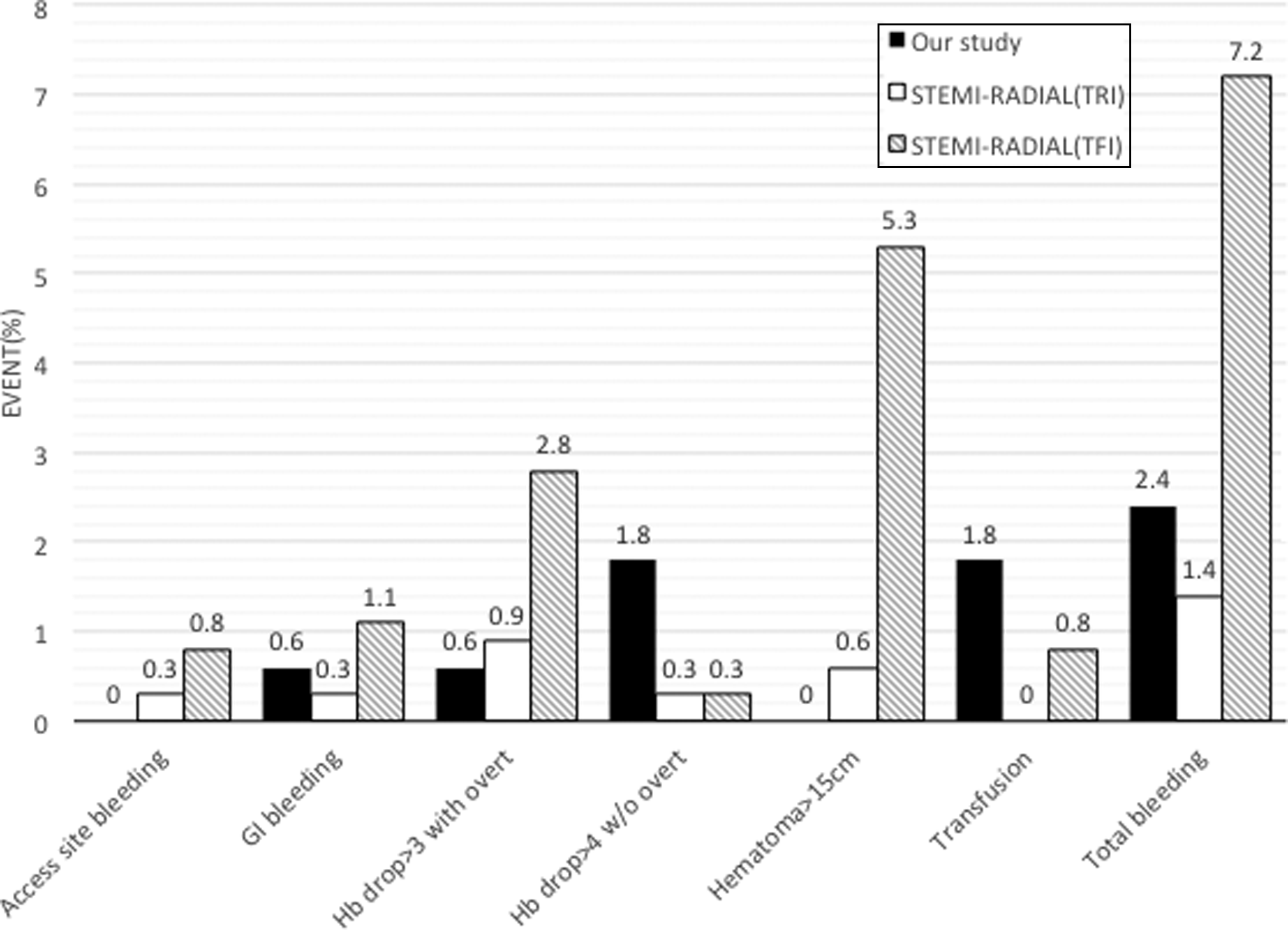
Bleeding events. Total bleeding event rate was 2.4% in our study; 1 patient had gastrointestinal bleeding and 3 patients had a decrease in hemoglobin level of >4 g/dL without an overt bleeding source. STEMI-RADIAL results are shown as reference values. GI indicates gastrointestinal tract; Hb, hemoglobin; TRI, transradial intervention; TFI, transfemoral intervention.
Discussion
We found that radial access for pPCI in patients with STEMI was acceptable in a low-volume center because the rate of MACE was 1.2% and the rate of bleeding events was 2.4%. Procedural results including technical success, door-to-balloon time, artery puncture-to-balloon time, fluoroscopy time, and contrast volume were also acceptable.
The effectiveness of radial access for pPCI has been reported in numerous randomized controlled trials for acute coronary syndrome. 8,10 –15 However, these reports gave the results for experienced operators in high-volume centers. The current European Society of Cardiology and European Association for Cardio-Thoracic Surgery guidelines recommend a radial access procedure by experienced operators. 7 Accordingly, the outcomes from our low-volume center with limited medical resources were examined in accordance with the end points of STEMI-RADIAL 8 and RIVAL. 10 In the STEMI-RADIAL trial, MACE occurred in 3.5% of the radial group and 4.2% of the femoral group, with bleeding events in 1.4% of the radial group and 7.2% of the femoral group. 8 In the RIVAL trial, MACE including death, MI, and stroke occurred in 3.2% of both the radial and femoral groups, and major bleeding (although the definition was not the same) occurred in 1.9% of the radial group and 4.5% of the femoral group. 10 Our results of 1.2% for MACE and 2.4% for overall bleeding events were almost comparable and within an acceptable range.
Peri-procedural bleeding is a strong independent predictor of early and late prognosis. 2 –4,16,17 Peri-procedural bleeding is categorized as access site- and nonaccess site related. Access site–related bleeding is associated with a 1.7-fold increase in mortality, compared with no bleeding; nonaccess site–related bleeding confers an even worse prognosis. 17 In patients with STEMI, access site–related bleeding represents 45% of total bleeding events. 18 Therefore, clinicians should minimize the risk of peri-procedural bleeding complications during PCI, especially in STEMI patients, by using bleeding avoidance strategies irrespective of the access site. The radial access procedure has been associated with >50% relative reduction in bleeding and access site complications compared with the femoral approach. 19,20 In a meta-analysis of randomized controlled trials comparing the radial and femoral approach, radial access was associated with reduction in relative risk of access site bleeding in patients with and without STEMI. 6,21 In the present study, the rate of access site bleeding was 0%, and our data support the effectiveness of radial access in preventing access site bleeding in patients with STEMI.
A concern with radial access is the high incidence of anatomic variability in size and course of the artery, 22 which can prolong the time for arterial puncture and cannulation of the coronary artery. This is a critical issue for pPCI in patients with STEMI, as the objective of the procedure is early reperfusion. Although PCI was initiated with femoral access due to a small or nonpalpable radial artery in 15 of 186 cases (8%) in the present study, there were no significant differences in baseline characteristics between the femoral access group and radial access group. In one case, catheter manipulation was difficult due to a tortuous subclavian artery, and crossover to femoral access was necessary. In previous trials, the rate of crossover from femoral to radial access was reported to be 4% to 10%, but was 0% in the TEMPURA trial. 8,10 –14 Although radial access was related to a significantly longer door-to-balloon time compared with that for femoral access, this had no influence on the incidence of MACE. 6,14 Considering these results, we could not support the strategy of femoral access as the first choice because of the complexity of radial access.
The PCI procedural volume has been associated with clinical outcomes in studies reporting primarily femoral access. 23 In addition, radial access is technically more challenging and may have a longer learning curve requiring higher volumes to achieve and maintain proficiency. 24 Therefore, the benefit of radial over femoral access depends upon the operator’s expertise in radial technique. 25 Jolly et al. defined a high-volume center as an institution with >146 radial PCIs/year/operator and reported that effectiveness of radial access in STEMI patients could only be accomplished in high-volume centers, not in low- or intermediate-volume centers. 26 Although our institution is a low-volume center with limited medical resources, the outcomes were acceptable when radial access was used as the first choice in pPCI for STEMI, suggesting that radial access would be safe and effective, even in a low-volume center.
Total MACE at 30 days in our study was only 1.2%, which was thought to be better compared with the results from previous trials. Although 2 elderly patients died suddenly because of free wall rupture, there was no event of MI and stroke in our study. Therefore, we could not conduct the prognostic factor of baseline characteristics including the preprocedure medications. Contrast-induced nephropathy (CIN) is also known to be a poor prognostic factor, 27 and prevention of CIN is an important issue especially in patients with STEMI requiring the emergent pPCI. Preventive therapies including preprocedure hydration, intravenous N-acetylcysteine administration, and statin use have been reported to reduce the risk of CIN. 28 –30 Although we did not perform these preprocedure measures, CIN occurred only in 8 (4.7%) patients, by minimizing contrast media volume. Further studies are needed in order to investigate the impact of radial access on CIN.
As the present study was a retrospective investigation in a single center, there are several limitations. First, the results summarized data on radial access in a single center, and the statistical power was low. While radial access should have been performed on all subjects, femoral access was actually used to initiate the procedure in 15 subjects, as radial access was difficult; these patients were removed from the analysis. Further, as the subjects were not randomized to radial or femoral groups, the superiority of radial access could not be demonstrated in the present study. Second, patients with Killip-4 were eliminated, and therefore, the effectiveness of radial access in shock remains unknown. Third, since the definitions of bleeding events and blood infusion were different from those of previous trials, direct comparison was not possible. In Japan, glycoprotein IIb/IIIa inhibitors that may have an effect on bleeding events are not approved, and therefore, it was difficult to make a comparison with previous results. Fourth, although the results of STEMI-RADIAL and RIVAL, both of which are large-scale clinical trials, are shown as reference clinical outcomes, we cannot directly compare the results with those of our study.
The clinical outcomes for pPCI with radial access in patients with STEMI in a low-volume center were acceptable. Our results indicate that radial access PCI is safe and may become the first choice, even in low-volume centers.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published. This study complied with the Declaration of Helsinki in regard to investigation in humans and was approved by the institutional ethics committees.
Acknowledgments
We extend our sincere appreciation to the late Dr Takako Kobori who provided medical care and performed PCI since our center was opened. Further, we would like to express our gratitude to the residents who worked with us: Dr Hiroko Hasegawa, Dr Masashi Hatori, Dr Yusuke Tamanaha, Dr Naoyuki Akashi, Dr Yusuke Adachi, Dr Shingo Yamamoto, Dr Jun Matsuda, Dr Takayuki Fujiwara, Dr Takunori Tsukui, Dr Tatsuro Ibe, Dr Daisuke Ono, Dr Hiroyuki Jinnouchi Dr. Keisuke Hirai, Dr Kohki Ishida, Dr Kei Yamamoto, Dr Mitsunari Matsumoto, Dr Yosuke Taniguchi, and Dr Yusuke Ugata.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.