
Abstract
Fatty acid–binding protein 4 (FABP4) is a possible biomarker of atherosclerosis. We evaluated FABP4 levels, for the first time, in patients with peripheral artery disease (PAD) and the possible association between baseline FABP4 levels and cardiovascular events over time. Patients (n = 327; mean age 69 ± 10 years) with stable PAD were enrolled in this study. Serum FABP4 was measured by bead-based multiplex assay. Cardiovascular events were analyzed by FABP4 tertiles using Kaplan-Meier and Cox regression analyses after 5 years. Serum FABP4 levels showed a significant association with the classical 3-point major adverse cardiovascular event (MACE) end point (including death, nonlethal myocardial infarction, or nonfatal stroke) in patients with PAD (P = .038). A standard deviation increase of FABP4 resulted in a hazard ratio (HR) of 1.33 (95% confidence interval [95% CI]: 1.03-1.71) for MACE. This association increased (HR: 1.47, 95% CI: 1.03-1.71) after multivariable adjustment (P = .020). Additionally, in multivariable linear regression analysis, FABP4 was linked to estimated glomerular filtration rate (P < .001), gender (P = .005), fasting triglycerides (P = .048), and body mass index (P < .001). Circulating FABP4 may be a useful additional biomarker to evaluate patients with stable PAD at risk of major cardiovascular complications.
Keywords
Introduction
Inflammation is a key component of atherosclerosis development. 1 Atherosclerosis is a complex process also involving endothelial dysfunction, changes in matrix metabolism, platelet activation, oxidative stress, vascular smooth muscle cell activation, and lipid disturbances. 1,2 White adipose tissue (WAT) itself is metabolically active, showing upregulated inflammatory pathways in obesity. 3 A cascade of events precedes the clinical onset of atherosclerosis: lesion initiation by endothelial dysfunction; fatty streak formation in the intima of the artery; fibroproliferative atheroma including smooth muscle cells; and advanced lesions including endothelial and smooth muscle cells, inflammatory cells, a lipid core, and a fibrous cap. 4
Peripheral artery disease (PAD) defined as an ankle–brachial index (ABI) <0.9 reflects the clinical onset of PAD, but not early stages of atherosclerosis development. 5 Well-established risk factors for the development for PAD include smoking, diabetes mellitus (DM), hypertension, and dyslipidemia. 5 The current management guideline of dyslipidemia with a strict low-density lipoprotein cholesterol (LDL-C) target reflects the continuous process of risk reduction in atherosclerotic diseases. 6 –8 Inflammation measured by C-reactive protein (CRP) as a risk marker for PAD development has been described in the Inter-Society Consensus for the Management of Peripheral Arterial Disease. 5
Adipokines released from WAT induce a state of chronic low-grade inflammation in obese people. 9 Fatty acid–binding proteins are intracellular lipid chaperons that are also released into the bloodstream by adipocytes and expressed in activated macrophages. 10,11 Fatty acid–binding protein 4 (FABP4), also termed adipocyte FABP or adipocyte protein 2, is preferentially produced in adipocytes and macrophages. 12 In animal models, FABP4 double knockout reduced atherosclerosis. 13 Additionally, FABP4 deficiency limited to macrophages showed a comparable reduction in atherosclerotic lesion area compared with whole-body deficiency. 13 The administration of a small-molecule inhibitor targeting FABP4 in mice was able to reduce atherosclerotic lesions. 14 Fatty acid–binding protein 4 in animal models promotes atherosclerosis, an effect mediated via macrophages. 13 Human studies showed an association of FABP4 with coronary artery disease (CAD). 15,16 In these patients with CAD, FABP4 was linked to increased atherosclerotic plaque burden as assessed by intravascular ultrasound. 15 Ultrasound assessment of the carotid artery showed a connection between FABP4 and intima–media thickness in Chinese people. 17 Recent data in patients with CAD propose FABP4 as a biomarker for adverse events in patients with acute coronary syndrome. 18 To the best of our knowledge, data on FABP4 and PAD are lacking. Therefore, we evaluated FABP4 levels in patients with PAD and the possible influence on cardiovascular outcome.
Materials and Methods
Study Population and Definitions
This is a substudy of the vascular medicine center cohort (VMC Vienna). 19 All patients with available frozen blood samples were included in this substudy. The study was approved by the institutional ethics committee and complies with the Declaration of Helsinki including current revisions and the Good Clinical Practice guidelines. 20,21 The procedures followed were in accordance with institutional guidelines, and all patients gave their written informed consent before entering the study.
Patients with PAD were consecutively recruited between 2006 and 2011 at the outpatient VMC of the Vienna General Hospital, a tertiary care center in Austria, for the VMC Vienna cohort. Detailed description of the cohort has been published. 19 Briefly, key inclusion criteria were stable PAD (ABI < 0.9, Fontaine stages I-II, and Rutherford stages I-III) and age between 40 and 90 years. Exclusion criteria were serum creatinine >229 μmol/L, connective tissue disease, hormone replacement therapy, critical illness within the last 6 months, type 1 DM, rest pain, ulcers, gangrene, or known cancer. Patients were assessed at the VMC for up to 60 months, every 6 to 12 months as medically needed. Unscheduled visits were performed in the VMC group at the patients’ request (eg, PAD worsening, cardiac/pulmonary symptoms).
Medical Investigation
A vascular assessment was performed at every visit including sphygmanometric oscillography (VL5000; ELCAT, Wolfratshausen, Germany) and ABI assessment by specialized technicians. The occurrence of cardiovascular events was assessed at every study visit. Fasting blood was drawn at each visit for glycated hemoglobin (HbA1c), cholesterol, and liver and renal function monitoring. Serum blood samples were drawn after an overnight fast and subsequently centrifuged at 3000 revolutions/minute for 15 minutes before storage at −80°C (at baseline and selected follow-up visits). A spot urinary sample was obtained to evaluate urinary albumin secretion measured as albumin to creatinine ratio >30 mg/g. Hyperlipidemia was defined as LDL-C ≥2.6 mmol/L or ≥1.8 mmol/L in diabetic patients and hypertension as sphygmanometric blood pressure readings exceeding 140/90 mm Hg or 140/85 mm Hg in diabetic patients according to the 2013 European Society of Cardiology arterial hypertension guideline 22 or by the administration of blood pressure medication.
Additionally, a standardized oral glucose tolerance test (oGTT, 75 g glucose) was performed in VMC patients, and glucose tolerance status was defined according the Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. 23 Glucose, insulin, and C-peptide levels were obtained in a fasting state (pretest) and at 2 hours during an oGTT. Prediabetes was defined by either a fasting glucose of 5.5 to 6.9 mmol/L, a 2-hour glucose level of 7.8 to 11.0 mmol/L, or an HbA1c of 39 to 46 mmol/mol. If either of these measures of glucose metabolism exceeded the aforementioned ranges, type 2 DM (T2DM) was diagnosed.
Measurement of Standard Laboratory Parameters and FABP4
Blood glucose, cholesterol, high-density lipoprotein cholesterol (HDL-C), and triglycerides were measured by enzymatic in vitro tests (Roche Diagnostics GmbH, Graz, Austria); the intra-assay and interassay coefficients of variation were 1.1% and 2.9%, 0.8% and 1.7%, 1.3% and 2.6%, 1.5% and 1.8%, respectively. Glycated hemoglobin was measured by high-performance liquid chromatography (Diamat; Bio-Rad, Hercules, California). Low-density lipoprotein cholesterol levels were estimated by the Friedewald equation. C-peptide and insulin were assessed by chemiluminescent immunoassay with a coefficient of variation between 3% to 4% and 4% to 7%, respectively. Serum creatinine was measured by Jaffe reaction with a coefficient of variation of 7.7%. Estimated glomerular filtration rate (eGFR) was calculated by the Chronic Kidney Disease Epidemiology (CKD-EPI) equation. 24 Creatinine clearance was calculated by Cockcroft-Gault formula. 25 Serum samples frozen (−80°C) at baseline and last available serum blood sample were thawed overnight at 4°C for FABP4 measurement. Fatty acid–binding protein 4 was measured at baseline visit and with the last available serum sample of the patient. Fatty acid–binding protein 4 levels were measured using bead-based multiplex assay for the Luminex platform with a sensitivity of 95.7 pg/mL (R&D Systems, Minneapolis, Minnesota). The intra-assay and interassay coefficients of variation for FABP4 levels were 6.16% and 6.25%, respectively.
Assessment of Survival
Survival of all patients was verified by central death registry database queries (Statistik Austria). In case of survival, additionally, hospital records were reviewed or the patient was contacted by phone to ensure data quality. International Classification of Diseases, Tenth Revision codes were obtained from the central death registry.
Statistics
Data are presented as mean (standard deviation [SD]) or median (25; 75th percentile). Student unpaired t test and χ2 test were used as appropriate. Fatty acid–binding protein 4 levels were log-transformed when the Kolmogorov-Smirnov test showed significant deviation from normal distribution. Survival curves were calculated by the Kaplan-Meier method. Between-group differences were tested by log-rank tests. Cox regression analysis was performed to estimate effect size and to allow for multivariable adjustment. Effect size for continuous parameters is given as hazard ratio (HR) per 1 SD. A 2-sided P < .05 was considered significant. All statistical analyses were performed with the statistical software package SPSS 24 (IBM, Chicago, Illinois). Figures were generated by GraphPad Prism 6.0h (GraphPad Software Inc, La Jolla, California).
Results
This study included 327 patients with PAD from the VMC Vienna cohort. This cohort was followed for up to 5 years. Typical cardiovascular risk factors and atherosclerotic comorbidities were highly prevalent in this PAD study. Patients with PAD are shown in Table 1 according to FABP4 tertiles at baseline to characterize the study cohort. Fatty acid–binding protein 4 levels were higher in female (P < .001) and older (P < .001) patients. Total cholesterol, LDL-C, HDL-C, or CRP was not associated with FABP4. Body mass index (BMI) was linked to FABP4 levels (P = .001), and declining renal function was associated with increased FABP4 levels (eGFR; P < .001).
Baseline Characteristics.a
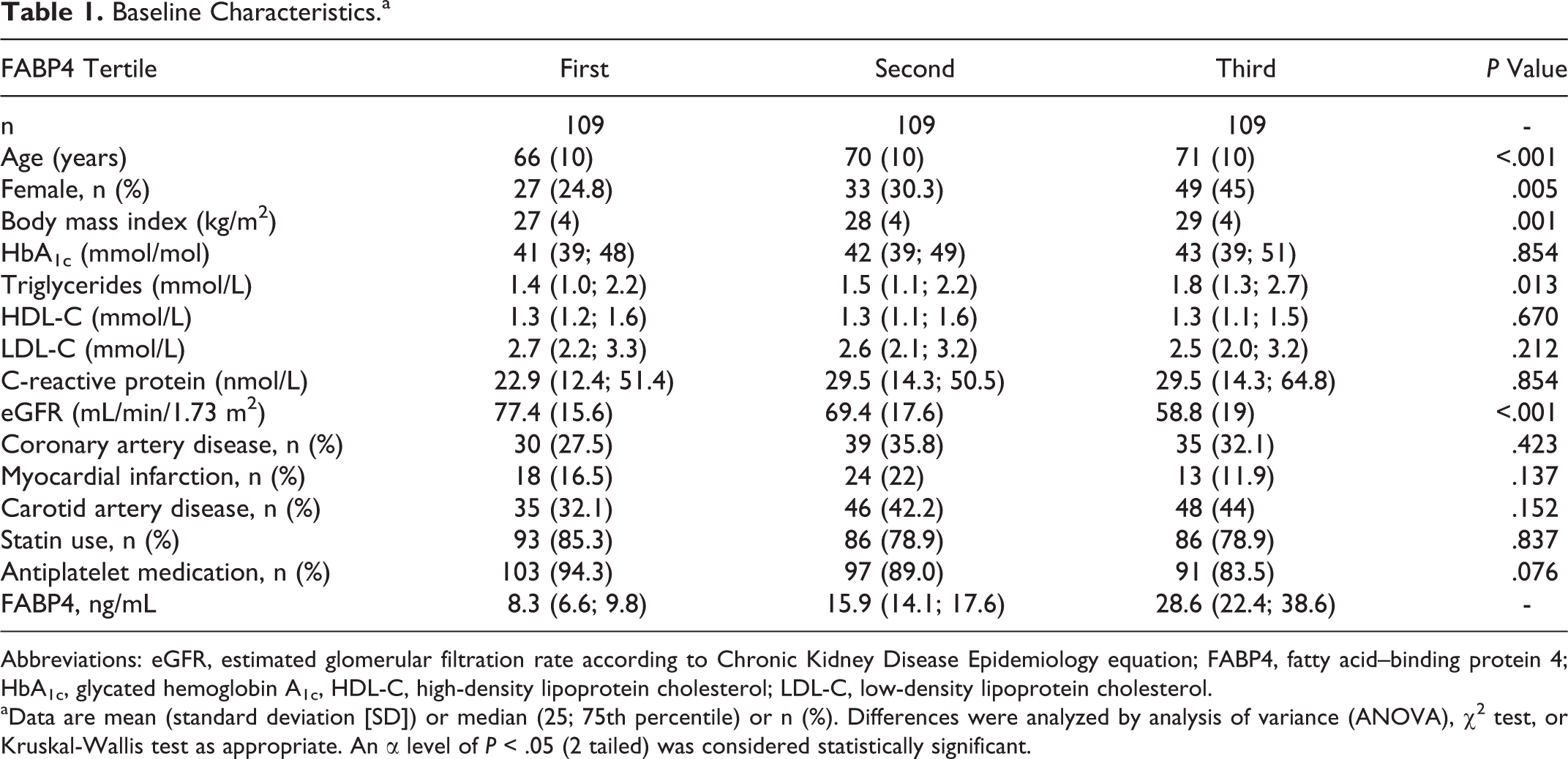
Abbreviations: eGFR, estimated glomerular filtration rate according to Chronic Kidney Disease Epidemiology equation; FABP4, fatty acid–binding protein 4; HbA1c, glycated hemoglobin A1c, HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
aData are mean (standard deviation [SD]) or median (25; 75th percentile) or n (%). Differences were analyzed by analysis of variance (ANOVA), χ2 test, or Kruskal-Wallis test as appropriate. An α level of P < .05 (2 tailed) was considered statistically significant.
Interrelation of FABP4 With Anthropometric and Laboratory Parameters
In univariate correlation analysis, FABP4 was significantly linked to patient age (R = .225, P < .001) and gender (female R = .194, P = .012). Furthermore, anthropometric markers such as waist circumference (R = .181, P = .001), hip circumference (R = .234, P < .001), inversely patient height (R = −.132, P = .018), and BMI (R = .223, P < .001) were related to FABP4 levels. Additionally, serum creatinine (R = .378, P < .001) as renal function parameters and inversely the calculated creatinine clearance (R = −.267, P < .001) and eGFR (R = −.467, P < .001) were significantly associated with FABP4. Rather weak ties to CRP (R = .127, P = .022) and triglyceride levels (R = .128, P = .020) were also observed.
Interrelation of FABP4 With Glucose Metabolism
Fatty acid–binding protein 4 was significantly linked with fasting insulin (R = .202, P < .001) and fasting C-peptide (R = .405, P < .001) levels. Additionally, fasting FABP4 was significantly associated with 2-hour oGTT insulin (R = .190, P = .001), 2-hour oGTT C-peptide (R = .266, P < .001), and 2-hour oGTT glucose (R = .120, P = .033).
Interrelation of FABP4 With Renal Function Parameters
Fatty acid–binding protein 4 was significantly associated with serum creatinine (R = .378, P < .001), eGFR (R = −.467, P < .001), and creatinine clearance (R = −.267, P < .001). These associations (creatinine, eGFR, and creatinine clearance) extend to patients with PAD with normal glucose metabolism (R = .334, P = .001; R = −.495, P < .001; R = −.299, P = .004), prediabetes (R = .438, P < .001; R = −.484, P < .001; R = −.280, P = .003), and overt T2DM (R = .327, P < .001; R = −.406, P < .001; R = −.225; P = .013), classified by oGTT.
Multivariable Regression Analyses
In multivariable linear regression analyses, only eGFR (P < .001), patient gender (P = .005), fasting triglycerides (P = .048), and BMI (P < .001) were significantly linked to serum FABP4 levels. Univariate-associated variables such as patient age, fasting insulin levels, serum CRP, waist circumference, hip circumference, and patient height did not remain associated with FABP4 serum levels.
Cardiovascular Outcome Analysis
Serum FABP4 levels showed a significant association with the classical 3-point major adverse cardiovascular event (MACE) end point (including death [n = 38], nonlethal myocardial infarction [n = 11], nonlethal stroke [n = 9]; P = .038). Figure 1 depicts the relation of FABP4 and MACE, showing a significant difference in event-free survival between the first tertile and the third FABP4 tertile (P = .046). In detail, MACE events by FABP4 tertile were 10/11/17 deaths, 3/6/2 nonlethal myocardial infarctions, and 1/3/5 nonlethal strokes in the first, second, and third tertiles, respectively. In unadjusted Cox regression analysis for MACE, 1 SD increase in FABP4 on the log scale resulted in an HR of 1.33 (95% confidence interval [95% CI]: 1.03-1.71). The association of FABP4 and MACE increased slightly (HR: 1.47, 95% CI: 1.06-2.03), after adjustment for gender, patient age, serum creatinine, serum triglycerides, serum cholesterol, HbA1c, and CRP (P = .020), as depicted in Table 2.
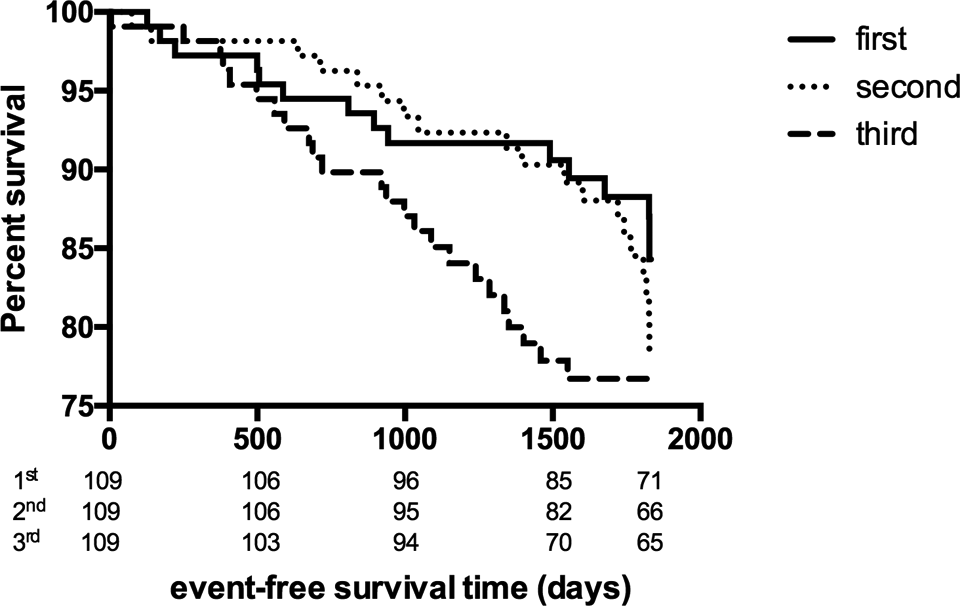
Major adverse cardiovascular event (MACE) including nonfatal myocardial infarction, nonfatal stroke, and all-cause mortality events are shown according to fatty acid–binding protein 4 tertile over the study period.
MACE Events by SD of Log FABP4.a
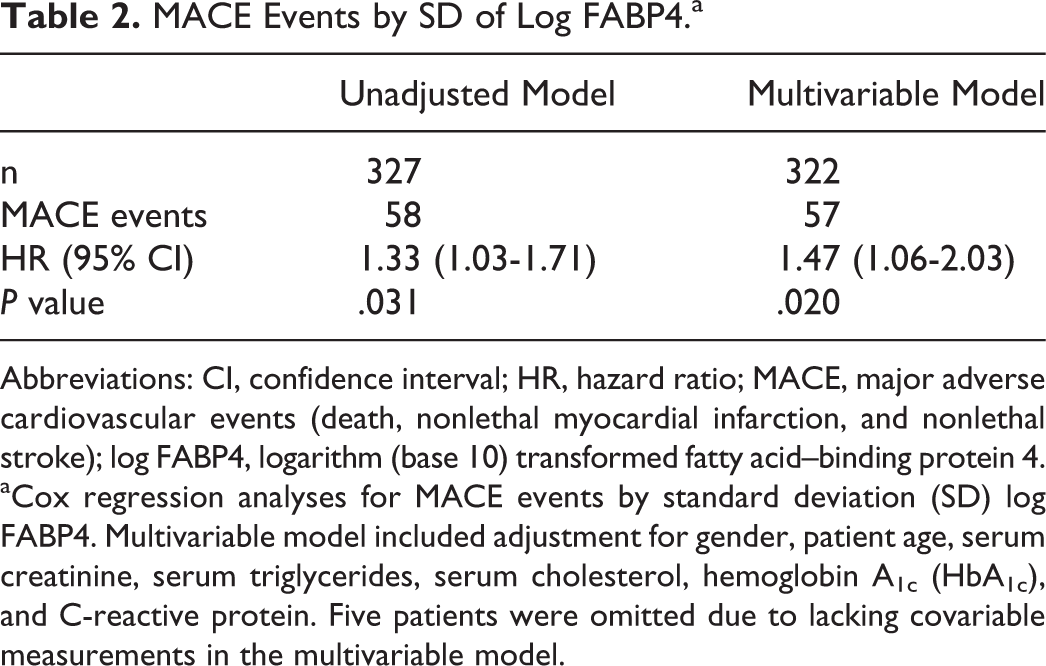
Abbreviations: CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiovascular events (death, nonlethal myocardial infarction, and nonlethal stroke); log FABP4, logarithm (base 10) transformed fatty acid–binding protein 4.
aCox regression analyses for MACE events by standard deviation (SD) log FABP4. Multivariable model included adjustment for gender, patient age, serum creatinine, serum triglycerides, serum cholesterol, hemoglobin A1c (HbA1c), and C-reactive protein. Five patients were omitted due to lacking covariable measurements in the multivariable model.
Overall Mortality
Higher FABP levels at baseline in patients with PAD resulted in a decreased survival, as shown in Figure 2. In detail, survival in the highest (third) FABP tertile was 81.7% compared to 90.8% in the lowest (first) FABP tertile (P = .023) and 89.9% in the middle (second) tertile (P = .036). In continuous analysis, baseline FABP4 showed a nonsignificant association with total mortality (P = .053). Survival was 94.5% in patients with PAD remaining in the first tertile at follow-up compared with 83.6% remaining in the third tertile at follow-up (P = .033; Figure 3A). In addition to those patients, increasing FABP4 levels to the third tertile at follow-up showed a nonsignificant trend for increased mortality compared to decreasing FABP4 levels to the first tertile (P = .096; Figure 3B).
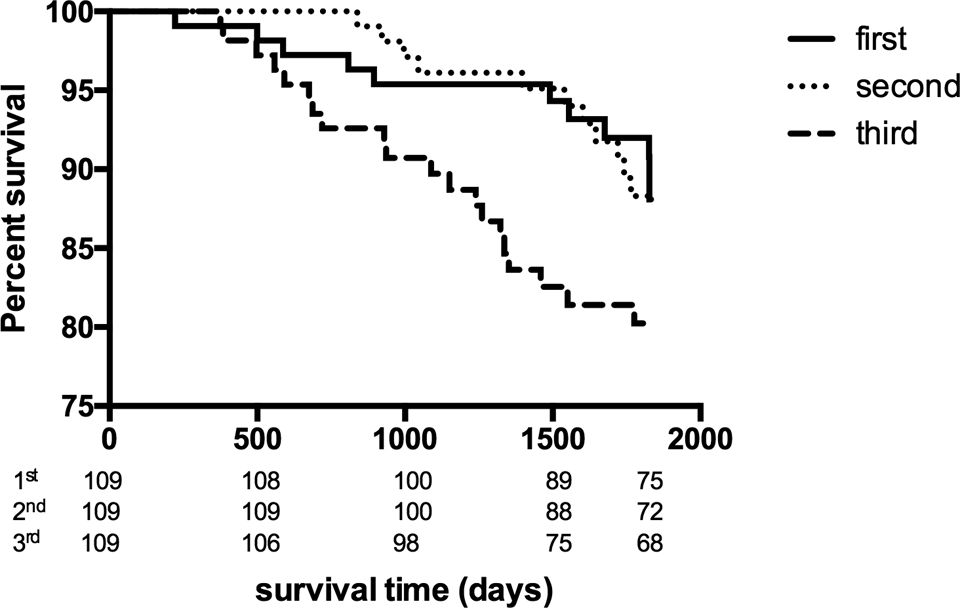
Survival of the patient cohort is shown according to fatty acid–binding protein 4 tertile over the study period.
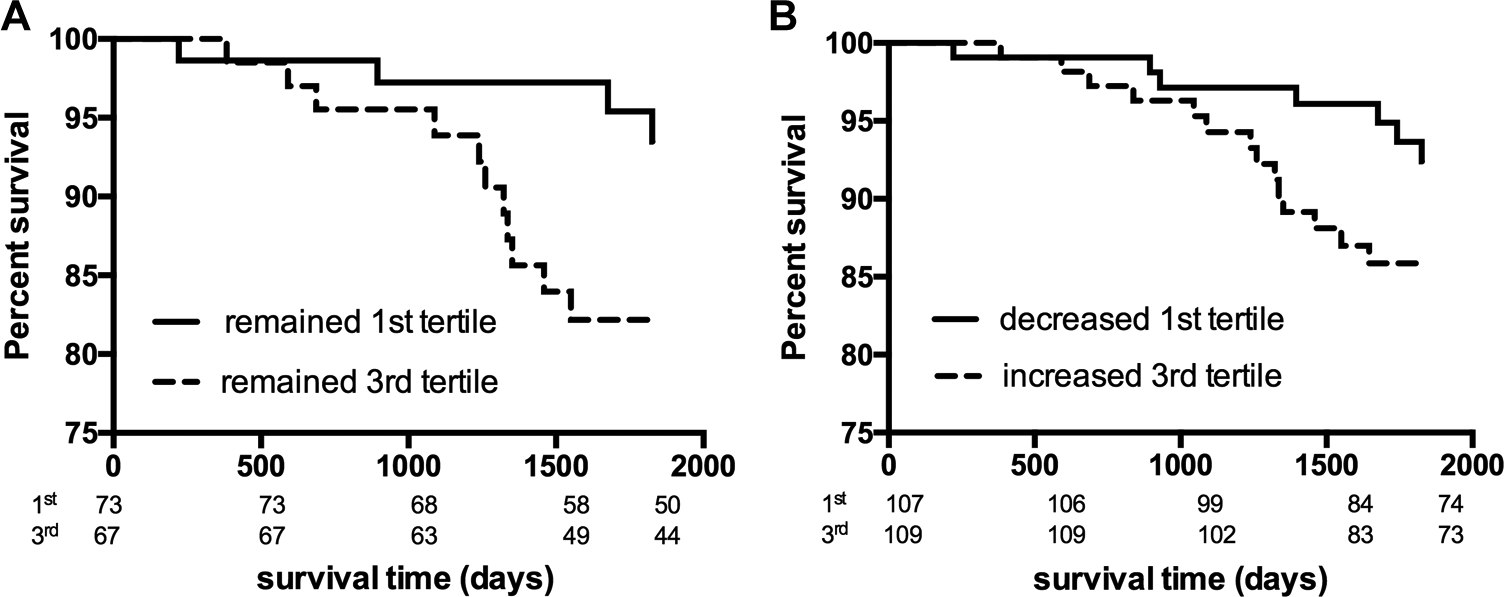
Subgroup analysis. A, Patients who remained in the first (lowest) fatty acid–binding protein 4 (FABP4) tertile in comparison to patients staying in the third (highest) FABP4 tertile over the study period. B, In addition, patients with decreasing (to the first tertile) or increasing (to the third tertile) FABP4 levels over the study period.
Discussion
To the best of our knowledge, this is the first description of the impact of circulating FABP4 levels on cardiovascular events in patients with PAD. This effect seems mainly mediated by increased all-cause mortality associated with higher FABP4 levels.
Recent publications reported an association between FABP4 and atherosclerotic diseases. 15 –18,26 Fatty acid–binding protein 4 has been proposed as a risk factor for cardiovascular disease development in Hong Kong Chinese people. 27 This population-based prospective study (n = 1847) assessing comprehensive cardiovascular risk factors showed that elevated baseline FABP4 levels were a predictor for developing cardiovascular disease (n = 182) within 12 years. 27 Increased carotid intima–media thickness (as an early marker of atherosclerosis) was linked to FABP4 in Chinese women, but not men. 17 In Japanese patients with CAD, FABP4 levels were higher compared with control patients without CAD. 15,26 Coronary plaque burden measured by intravascular ultrasound in these patients with CAD was linked to FABP4 levels. 15 In Korean adults, FABP4 levels seem to predict CAD severity measured by the number of affected coronary arteries (n = 234). In patients with CAD, elevated baseline FABP4 levels increased the risk of secondary cardiovascular disease events in a 10-year prospective study. 28 Elevated FABP4 in acute coronary syndrome predicted adverse events similar to the Global Registry of Acute Coronary Events score and was proposed as a possible biomarker. 18 In addition, in patients with end-stage renal disease and thus high cardiovascular risk, high FABP4 levels predicted increased mortality. 29 The current study highlights a similar association of elevated FABP4 levels and cardiovascular events in patients with PAD. Apart from atherosclerosis, FABP4 plays an important role in the development of insulin resistance and DM and was considered as a possible target for the prevention of cardiovascular disease. 30
In Caucasian people (Czech Republic, n = 138), FABP4 increases with the development of metabolic syndrome and correlates with fasting insulin, fasting glucose, triglycerides, and the anthropomorphic parameters such as BMI and waist circumference in healthy patients. 31 In line with these findings, this study found the same univariate association pattern in a cohort of patients with PAD. Fatty acid–binding protein 4 has been linked to the development of insulin resistance and was a predictor of T2DM development in Chinese people over 10 years (n = 544, 96 T2DM). 32
In Spanish patients with T2DM having renal dysfunction, FABP4 was associated with high plasma creatinine and low eGFR by Modification of Diet in Renal Disease estimation (n = 161). 33 In this study (n = 327), similar significant associations with serum creatinine, eGFR (CKD-EPI equation), and creatinine clearance were found in a cohort without significant renal dysfunction.
The interrelation of FABP4 with atherosclerosis, metabolic syndrome, T2DM, and renal function makes FABP4 a potential biomarker for cardiovascular risk, especially in patients with overt atherosclerosis. This marker might summarize the various disease components of a person and highlight those who need treatment to prevent cardiovascular events. However, it has to be taken into account that women with overt atherosclerosis show higher FABP4 levels (patients with CAD 18 or PAD in this study).
Several limitations of our study have to be considered. First, patients were included in a consecutive fashion, selecting patients motivated to take an active part in their treatment and patients with positive attitude toward cardiovascular risk modification. Second, we included older (69 ± 10 years), but not frail, patients with PAD with a high cardiovascular risk burden at baseline and thus high risk of cardiovascular events and natural increased mortality rate. Third, all patients were treated in a single center, and thus, our data need to be confirmed in large multicenter trials.
In Summary, FABP4 has been associated with atherosclerosis development and manifest atherosclerosis (carotid artery disease and CAD). Data on FABP4 in PAD have been scarce. Our data in patients with PAD demonstrate a clear association of FABP4 and PAD cardiovascular event risk.
Footnotes
Authors’ Note
C.H. performed the literature search, contributed to study design, performed FABP4 measurements and statistical analyses, contributed to interpretation of the results, and drafted the manuscript. C.T.H. conducted the statistical analyses, contributed to interpretation of the results, and drafted the manuscript. G.P. contributed to data collection in the VMC cohort and performed the FABP4 measurements. T.W. contributed to data collection, data coordination, and data management. R.K. participated in the interpretation of the results and revised the manuscript. G-H.S. designed the VMC study cohort, directed and performed the statistical analyses, contributed to interpretation of the results, and revised the manuscript. All authors read and approved the final manuscript.
Acknowledgments
The authors thank Daniela Seidinger, laboratory technician, for her support during this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Medical University Vienna, Vienna, Austria.