
Abstract
Endothelial dysfunction is common in patients with type 2 diabetes mellitus (T2DM) and is associated with atherosclerotic disease. This study aimed to determine prognostic factors for endothelial dysfunction and identify relationships between reactive hyperemia index (RHI) score, clinically relevant coronary artery disease (>50% stenosis), and major adverse cardiovascular events (MACEs) in patients with T2DM. Endothelial function was assessed using peripheral arterial tonometry and correlated with patient characteristics and cardiovascular outcomes during a median follow-up of 22.8 months. Among 235 patients with a median duration of T2DM of 13 years, mean (standard deviation) RHI score was 2.00 (0.76). Serum low- and high-density lipoprotein cholesterol levels positively (P = .004) and negatively (P = .02) predicted RHI score, respectively. Median coronary artery calcium (CAC) score was 109 Agatston units, but no correlation between CAC and RHI scores was observed. The RHI score did not predict the number or severity of coronary plaques identified using computed tomography coronary angiography. Additionally, there was no association between RHI score and the risk of an MACE during follow-up. Overall, endothelial function was not predictive of CAC score, extent, and severity of coronary plaque or MACEs and did not demonstrate utility in cardiovascular risk stratifying patients with T2DM.
Keywords
Introduction
Vascular endothelial cells play a major role in maintaining homeostasis. The endothelium secretes a number of mediators that regulate platelet aggregation, coagulation, fibrinolysis, and vascular tone. 1 Endothelial dysfunction refers to a loss of the primary physiological function of the endothelium in promoting vasodilatation, fibrinolysis, and inhibiting platelet aggregation. 2,3 Several vasodilatory mediators, such as nitric oxide (NO), prostacyclin, and endothelium-derived hyperpolarizing factor, aid in maintaining this physiological homeostasis. 1,3,4 Additionally, under normal physiological conditions, insulin increases skeletal muscle blood flow via endothelium-mediated increases in NO production, 5 an effect that is attenuated in patients with type 2 diabetes mellitus (T2DM). 6 As such, significant endothelial dysfunction has been noted in these patients.
The pathophysiology of endothelial dysfunction in patients with T2DM is poorly understood, but is associated with a proatherogenic state, an increased risk of plaque activation and rupture, and decreased blood flow due to thrombosis and vasospasm. 7 Therefore, endothelial dysfunction can be considered the primary event in atherogenesis. 7
Accordingly, the present study investigated whether endothelial function in patients with T2DM correlates with coronary artery atherosclerosis and major adverse cardiovascular events (MACEs).
Methods
Patient Population
Patients were recruited from hospital diabetic clinics and a cardiovascular screening clinic in North-West London (Barnet Hospital, Central Middlesex Hospital, Royal Free Hospital, and North West London Cardiovascular Screening Community Clinic) as part of the Progression of Coronary Atherosclerosis in Asymptomatic Diabetic Subjects: Evaluation of the Role of CT Coronary Angiography and Markers of Endothelial Function and Vascular Inflammation (PROCEED) study. All patients aged ≥35 years attending these clinics who had been diagnosed with T2DM ≥1 year before enrollment were invited to participate in the study. Pregnant women, patients with established coronary artery disease (CAD), a severe allergy to iodinated contrast media, or an estimated glomerular filtration rate <45 mL/min/1.73 m2 were excluded from the study. Patients with known atrial fibrillation were also excluded due to the limited ability to obtain diagnostic computed tomography coronary angiography (CTCA) images.
All patients enrolled in the PROCEED study provided written informed consent before enrollment. This study was registered with ClinicalTrials.gov before the first patient was enrolled (Clinicaltrials.gov identifier: NCT02109835). Ethical approval was obtained from National Research Ethics Service, United Kingdom, and the study was performed in accordance with the principles of the Seventh Revision of the Declaration of Helsinki (2013).
Baseline demographic, clinical, and laboratory data were obtained from all patients and included age, gender, ethnicity, height, weight, waist and hip measurements, blood pressure, diabetes medication, duration of diabetes, presence of microvascular disease and type, hyperlipidemia, hypertension, history of smoking, family history of ischemic heart disease, glycated hemoglobin (HbA1c), serum creatinine, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides. Ethnicity was self-reported with Mediterranean ethnicity being designated as Caucasian. Patients with a coronary artery calcium (CAC) score of >1000 Agatston units (AU) were presumed to have significant coronary artery stenosis and did not undergo a CTCA.
Determination of Digital Pulse Amplitude
Digital pulse amplitude was measured in the fasting state with a peripheral artery tonometry (PAT) device (EndoPAT2000, Itamar Medical, Caesarea, Israel) comprising a pneumatic plethysmograph that applied homogenous pressure to the fingertip of the middle finger of both hands, allowing measurement of pulse volume changes in each finger. Baseline pulse amplitude for each fingertip was measured for 5 minutes. On completion of baseline recording, arterial occlusion was performed by inflating a blood pressure cuff to 20 mm Hg above the patient’s systolic blood pressure, or 200 mm Hg, whichever was higher. Following the test period, the arterial occlusion was released and pulse amplitude measured for a further 5 minutes. Pulse amplitude was recorded electronically and analyzed using a computerized, automated algorithm (Itamar Medical) to calculate average pulse amplitude and reactive hyperemia index (RHI). The RHI score represents the change in PAT signal ratio produced by occlusion of the brachial artery, relative to RHI score in the nonoccluded arm, and corrected for baseline endothelial tone. 8
CTCA Scan Protocol
All scans were acquired using a dual-source computed tomography scanner (Somatom Definition, Forchheim, Germany) with a maximum load capacity of 220 kg. The CTCA scan protocol consisted of (1) topogram; (2) prospectively gated, nonenhanced scan to calculate CAC score according to standard protocol 9 ; (3) test bolus scan to determine the circulation time; and (4) contrast-enhanced coronary angiogram.
Nitroglycerin (800 µg sublingual) was administered to each participant immediately prior to beginning CTCA scanning. Intravenous metoprolol (up to 15 mg) was administered to participants with a heart rate >70 beats/min (bpm), unless contraindicated. All images were acquired craniocaudally, in a supine position, during a single breathhold in inspiration. Images were acquired with a gantry rotation time of 330 milliseconds, detector collimation of 2 mm × 32 mm × 0.6 mm (with double sampling in the z-axis, using flying focal spot technology), pitch of 0.2 to 0.5 (adapted to heart rate) with retrospective electrocardiography (ECG) gating, and ECG-controlled tube current modulation. In participants scanned with 120 kV tube current of up to 450 mA was used. A triple phase-contrast protocol was used with a bolus of contrast (Iomeron 400, Bracco, Italy) followed by 30 mL of a 30:70 mixture of contrast and saline followed by a 70-mL saline flush, all at a rate of 5.5 to 6.0 mL/s. Volume of contrast bolus was calculated for each patient based on the scan time as follows: contrast volume (mL) = scan time (seconds) × flow rate + 10 mL (minimum volume 60 mL).
Image Reconstruction
The CTCA images were reconstructed in mid diastole in patients with a heart rate <70 bpm and in end systole in patients with a heart rate >70 bpm. If initial reconstructions were not satisfactory, additional reconstructions were made every 5% of the R-R interval and reviewed in an attempt to pick the best quality data set. Images were reconstructed with a slice thickness of 0.75 mm and increment of 0.50 mm using B26 heart view convolution kernel. Images were then transferred to a dedicated workstation (Leonardo, Siemens, Forchheim, Germany). Axial slices, multiplanar reconstructions, and maximum intensity projections were used to evaluate the patency of coronary arteries. 7
MACE Follow-Up
A MACE was defined as all-cause death, nonfatal myocardial infarction, or late coronary revascularization (a procedure undertaken more than 60 days after baseline investigations). Patients were routinely followed up for MACE by e-mail or telephone. All self-reported MACEs were confirmed by medical records.
Statistical Analysis
Baseline characteristics were described using frequencies and percentages for categorical variables. For continuous variables, mean and standard deviation (SD) were used if the variable was normally distributed and median and interquartile range (IQR) if not normally distributed. Independent Student's t test was used to examine the difference between 2 independent groups for a normally distributed variable. Categorical variables were compared using the χ2 test. Distribution of RHI scores between the groups was compared using a Kruskal-Wallis test. Regression analysis (binary logistic) was used to test the strength of association for various factors, alone at first and then in a multivariate model. Receiver–operator characteristic curve analysis was used to identify the coordinates of the variable in question at which optimal sensitivity and specificity were achieved. A 2-sided P <.05 was considered significant for all analyses. Any variable with >15% missing data was excluded from the final analysis. Data were analyzed using STATA (StataCorp LLC, College Station, Texas).
Results
Of the 258 patients who were investigated, 23 patients did not have an RHI score. Two patients had an upper limb amputation, while an accurate reading could not be obtained in another 2 patients. The RHI testing could not be performed in the remaining 19 patients due to technical difficulties. Therefore, 235 patients with a mean (SD) age of 62 (8.5) years were included in the final analysis. The majority of patients (59%) were male and 56% were of South Asian origin, reflecting the ethnic composition of the screening population and high prevalence of T2DM in this ethnic group. Microvascular disease was documented in 48% (123/235) of patients and mean (SD) RHI score was 1.99 (0.75), which was considered to be high for a diabetic population. Baseline characteristics of the entire study population are shown in Table 1. Patients were followed up for a median duration of 22.8 months. Nine patients were lost to follow-up after the index visit.
Baseline Clinical and Demographic Characteristics.
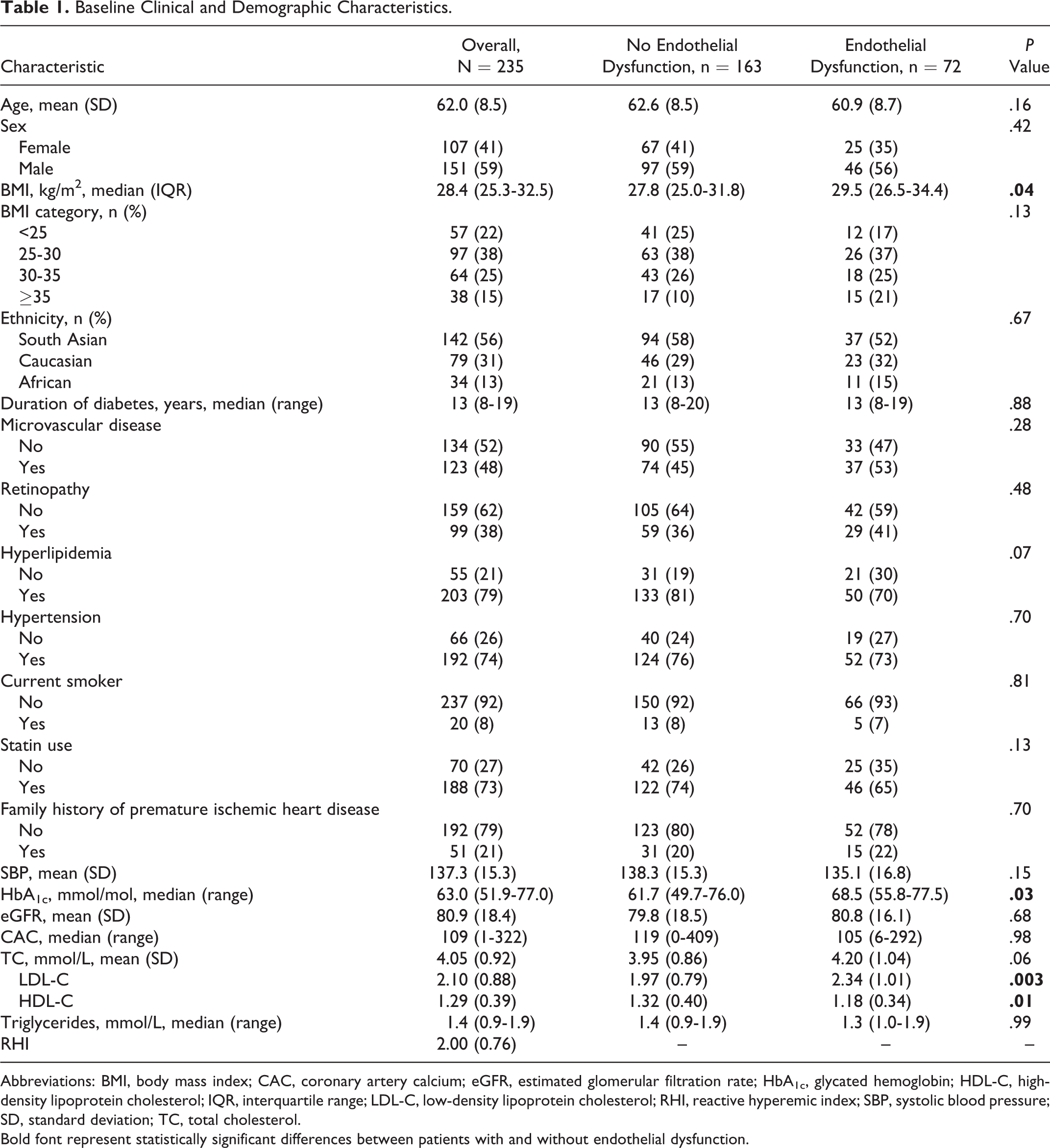
Abbreviations: BMI, body mass index; CAC, coronary artery calcium; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; RHI, reactive hyperemic index; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol.
Bold font represent statistically significant differences between patients with and without endothelial dysfunction.
Characteristics of Patients With Endothelial Dysfunction
Among patients with an RHI score available, 163 (69.4%) had normal endothelial function and 72 (30.6%) had endothelial dysfunction. Patients with endothelial dysfunction were more likely to be obese with a median body mass index (BMI) of 29.5 compared with 27.8 in those with preserved endothelial function. Patients with endothelial dysfunction also had poorer glycemic control and a higher prevalence of dyslipidemia, characterized by higher serum LDL-C concentrations and lower serum HDL-C concentrations (Table 1). No significant difference was observed between patients administered statins and those who were statin-naive. There was also no significant difference in triglyceride or TC:HDL-C ratios (Table 1).
Endothelial Function and BMI
Endothelial function was significantly negatively correlated with BMI (P = .032; Figure 1). Patients with higher BMI had lower RHI scores, although the size of the effect was small.
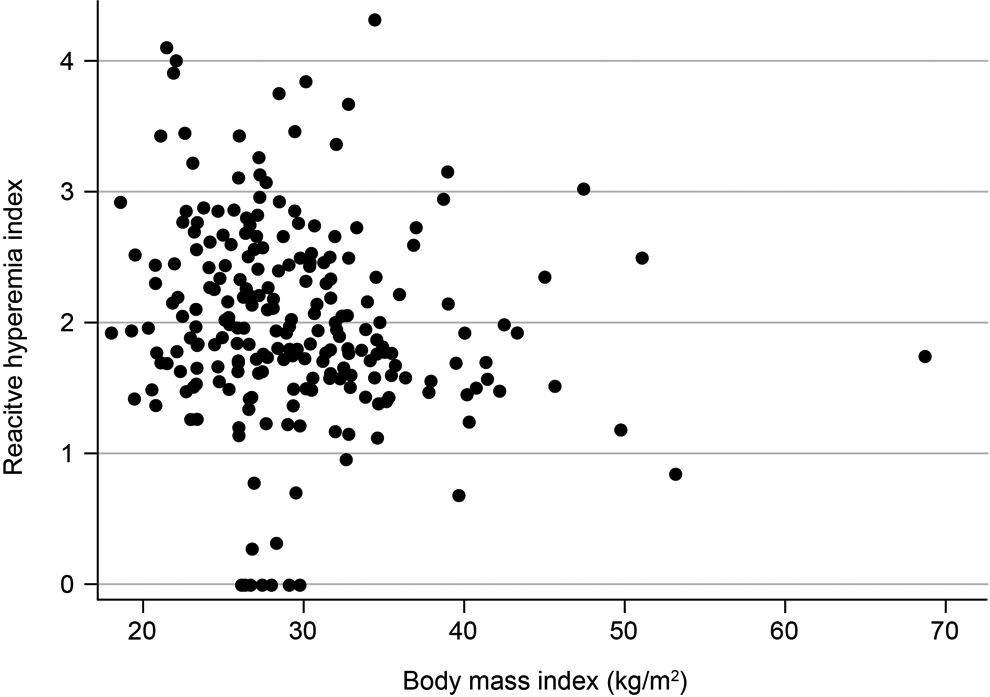
Scatter plot illustrating the relationship between body mass index and reactive hyperemia index scores.
Patients were segregated into 4 groups based on BMI (group 1: <25 kg/m2; group 2: 25-30 kg/m2; group 3: 30-35 kg/m2; group 4: >35 kg/m2). Median (IQR) RHI scores for groups 1 to 4 were 2.10 (0.98), 1.98 (1.01), 1.87 (0.62), and 1.68 (0.72), respectively, and a significant difference in the distribution of RHI scores was identified between the groups (Kruskal-Wallis test, P = .047; Figure 2). There was also a negative, but statistically nonsignificant, trend noted in the relationship between waist-to-hip ratio and the RHI scores (P = .07).
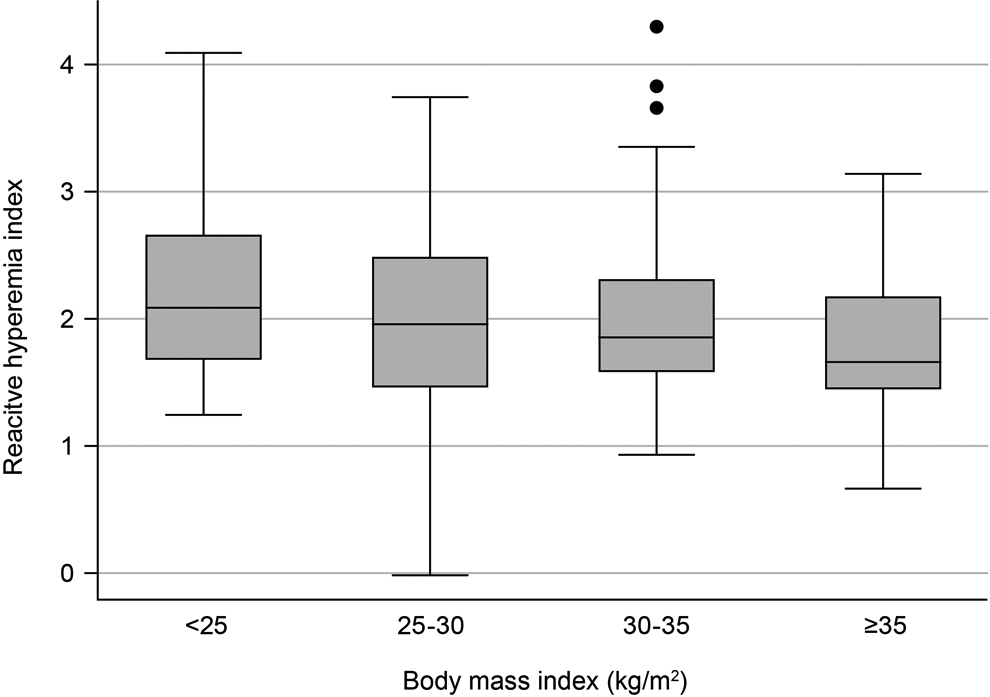
Median and distribution of reactive hyperemia index scores in different body mass index categories.
Determinants of Endothelial Dysfunction
Following univariate and multivariate regression analyses, only serum LDL-C (P = .004) and HDL-C (P = .02) levels were significant predictors of endothelial dysfunction. Identical results were observed in both analyses: Every 1 mmol/L increase in LDL-C was associated with a 59% increase in the probability of endothelial dysfunction (odds ratio [OR], 1.59; 95% confidence interval [CI], 1.16-2.19), whereas each 1 mmol/L increase in serum HDL-C reduced the odds of endothelial dysfunction by approximately two-thirds (OR, 0.37; 95% CI, 0.16-0.82). In the univariate analysis, trends toward increased endothelial dysfunction being associated with total serum cholesterol levels (OR, 1.33; 95% CI, 0.99-1.79; P = .06) and BMI (OR, 1.22; 95% CI, 0.99-1.51; P = .06) were identified but were not statistically significant following multivariate analysis.
RHI and CAC Scores
Both RHI and CAC scores were not significantly correlated (r = −0.04; P = .56) nor were CAC scores predictive of the presence of endothelial dysfunction. Patients with endothelial function had a median CAC score of 119 (IQR, 0-408) compared to a median of 105 (IQR, 6-292) in patients with endothelial dysfunction (P = .98). No statistically significant difference in mean RHI scores was observed between the levels of CAC (P = .30; Table 2).
Relationship Between Reactive Hyperemia Index and Endothelial Dysfunction in Patients by CAC Score and Presence of Coronary Artery Plaque.
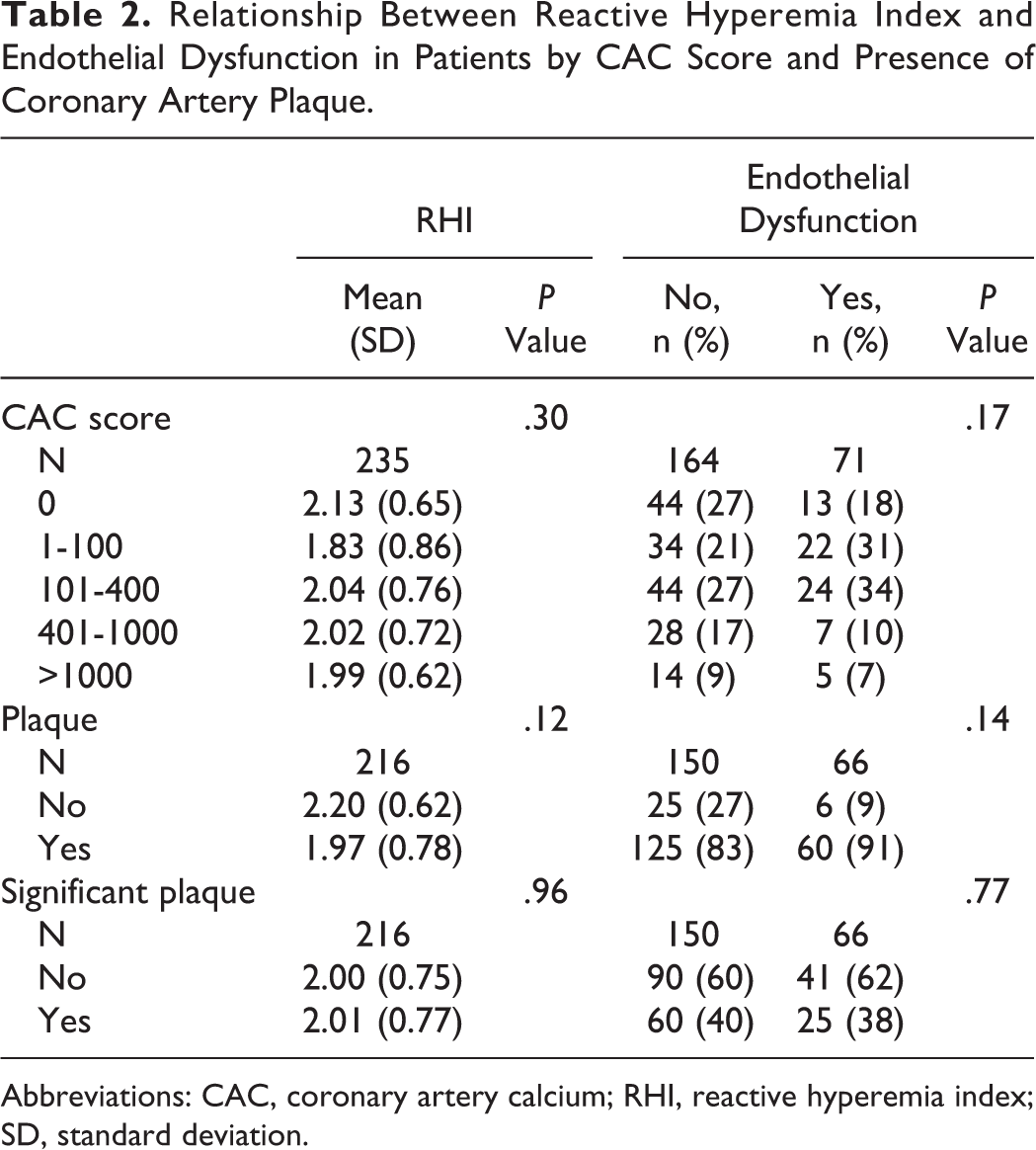
Abbreviations: CAC, coronary artery calcium; RHI, reactive hyperemia index; SD, standard deviation.
RHI Score and Prevalence and Severity of CAD
There was no significant association between RHI score and the presence or number of coronary plaques in this cohort (P = .12 and .58, respectively; Table 2). Similarly, there was no difference in plaque prevalence in patients with or without endothelial dysfunction (P = .14). The median number of coronary plaques in those with or without endothelial dysfunction was also not significantly different (6 [IQR, 1-10] vs 6 [IQR, 3-9], respectively). We also examined the relationship between clinically relevant CAD (>50% stenosis), RHI score, and endothelial dysfunction and found no statistically significant association (P = .96 and .77, respectively).
Endothelial Dysfunction and MACEs
A total of 18 MACEs were noted during the study period, including 6 deaths, 1 ischemic stroke, and 11 late revascularizations (7 percutaneous coronary interventions and 4 coronary artery bypass graft surgeries). No significant association between the presence/absence of endothelial dysfunction or continuous or categorical measures of RHI was demonstrated (Table 3).
Relationship Between Measures of Endothelial Function and Major Adverse Cardiovascular Events.
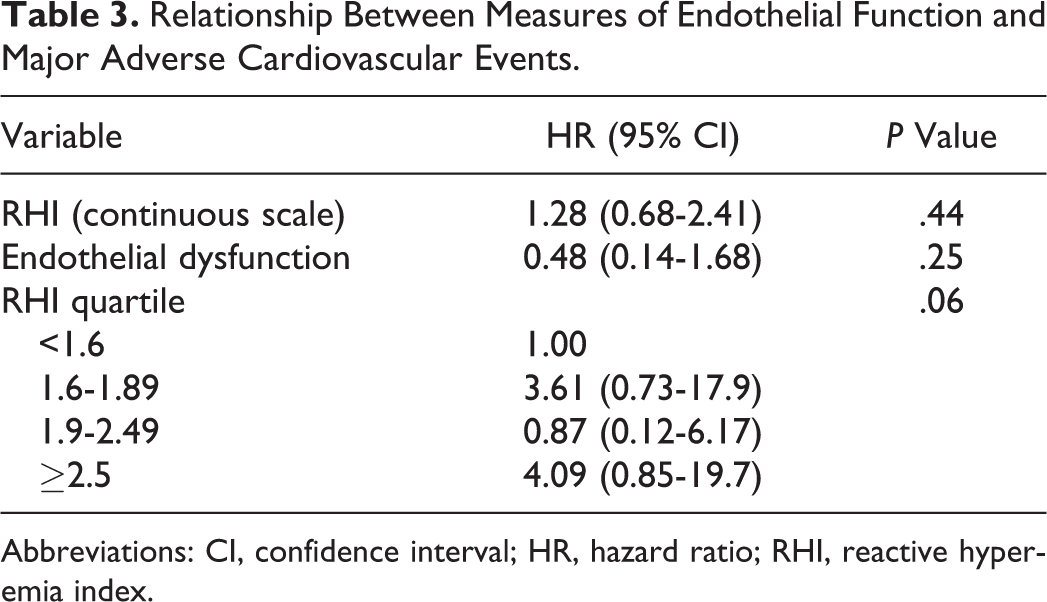
Abbreviations: CI, confidence interval; HR, hazard ratio; RHI, reactive hyperemia index.
Discussion
Endothelial dysfunction was observed in approximately 30% of patients with T2DM and was associated with higher BMI, poorer glycemic control, and a higher prevalence of dyslipidemia, characterized by higher serum LDL-C concentrations and lower serum HDL-C concentrations. The LDL-C and HDL-C were the only independent predictors of endothelial dysfunction. Furthermore, no significant association between endothelial function, measured by RHI, and measures of CAD was identified in patients with T2DM.
Our data do not support the use of endoPAT as a surrogate marker of epicardial coronary disease, which contrasts with an earlier study where a moderate association between coronary and peripheral endothelial function has been demonstrated using flow-mediated dilation (FMD) of the brachial artery. 10,11 However, the use FMD is limited due to disparate, nonstandardized protocols and interobserver variability when comparable protocols are applied. 11 –13 By comparison, PAT using the EndoPAT2000 uses an automated computer algorithm to ensure reproducible measurements with a low risk of interobserver variability, offering a rapid, noninvasive endothelial dysfunction-based screening option for asymptomatic CAD in patients with T2DM with increased accuracy across time and different clinical settings. Notably, the 2 techniques also differ in their physiological assessments: FMD assesses endothelial function in the larger conduit vessels, whereas PAT assesses endothelial function in the microvasculature, so differences in endothelial function in the microvasculature may not physiologically reflect those in the epicardial coronary arterial tree. 14
While direct assessment of endothelial function using invasive procedures may be investigated to confirm any relationship between endothelial dysfunction and CAD, these procedures are time-consuming and challenging to perform and not suitable for use as a routine screening option in clinical practice. 15
In this study, RHI scores were not associated with MACE rates, despite previous studies indicating that assessments of endothelial function may have utility as a prognostic tool for MACEs, especially in studies of a longer duration than the current study. 10,16,17 However, most of these studies used FMD of the brachial artery as a marker of endothelial function. 10,16 Furthermore, the cohort of patients in this study also had a very high rate of statin and angiotensin-converting enzyme inhibitor (ACEi) use and, as a result, presented with favorable blood pressure and lipid profiles. 10,16 While very few studies have investigated the prognostic value of endothelial function measured using PAT, a low RHI score has been found to independently predict subsequent cardiovascular events and was associated with a significantly higher rate of cardiovascular hospitalization. 17 However, these findings were observed in patients with symptomatic cardiovascular disease and during a 7-year follow-up. 17 Furthermore, only 12% (n = 32) of the patient cohort had diabetes mellitus. 17 Therefore, to our knowledge, this is the first study to assess the association of RHI scores with MACEs in a cohort of patients with T2DM and asymptomatic CAD.
Endothelial dysfunction was more likely to be observed in patients who were obese and exhibiting poorer glycemic control as shown by correlation between higher HbA1c and serum LDL-C (and lower HDL-C) levels in the serum of patients with RHI scores. Accordingly, the failure of EndoPAT2000-assessed RHI to predict asymptomatic CAD in patients with T2DM may be linked to the well-established correlation between higher serum HbA1c levels and microvascular disease. 18,19 However, the relationship between macrovascular disease is more nuanced, with epidemiological studies suggesting a link between HbA1c levels and CAD in patients with T2DM, but improved glycemic control not translating into a reduction in macrovascular end points in randomized controlled trials. 18 –20 We have previously established the role of CAC in a similar asymptomatic T2DM population and shown the prognostic value of CAC and compared CAC with more established markers of prognosis using myocardial perfusion imaging. 21,22 However, optimal glycemic control has been shown to reduce CAC progression in patients with T2DM and asymptomatic CAD. 22,23
The mechanisms underlying the pathogenesis of endothelial dysfunction and subsequent coronary atherosclerosis in patients with T2DM are not yet fully understood. However, several main pathways have been implicated. 24,25 For example, the direct effects of accumulation of advanced glycation end products (AGE) within the vascular wall and upregulation of the AGE receptor (RAGE) have been reported in patients with endothelial dysfunction. 24,25 The RAGE is found on the surface of endothelial cells, as well as monocytes and macrophages, and upregulation leads to downstream activation of proinflammatory factors. 24
Another potential pathway toward endothelial dysfunction in patients with T2DM involves T2DM-related activation of the renin–angiotensin system (RAS) significantly altering endothelial cell function, reducing endogenous NO production, and increasing levels of vasoconstrictors, such as angiotensin-II. 25,26 Moreover, activation of the endothelin pathway results in endothelial dysfunction with decreased production of NO and increased plasma endothelin-1 (ET-1), which is a potent vasoconstrictor. 25,26 The ET-1 also upregulates the production and release of inflammatory cytokines from monocytes. 25,26
The effects of RAS activation, and to some extent the ET-1 pathway, can be attenuated by the use of ACEis and angiotensin receptor blockers. In addition, treatment with statins has also been shown to have pleiotropic effects, particularly on endothelial function, as well as upregulating endothelial NO synthase activity. 27 The resulting increase in NO production, and inhibition of ET-1 expression, by statins may improve overall endothelial cell function. 27 Accordingly, the physiological effects of statin and ACEi therapy in this cohort of patients may have additionally contributed to the observed prevalence of CAD and MACE in this population, above and beyond controlling dyslipidemia and hypertension. 27
Similarly, antihyperglycemic treatment with sodium-glucose cotransporter type 2 (SGLT-2) inhibitors has been shown to significantly improve endothelial function in patients with type 1 diabetes mellitus after 12 weeks of treatment. 28 Specifically, RHI scores were increased by 1.3-fold following empagliflozin therapy. 28 While such findings may be important when considering the results of large studies of endothelial function and cardiovascular outcomes in patients with T2DM, <2% of patients enrolled in this study were being treated with an SGLT-2 inhibitor, suggesting that the impact on the overall study outcomes was likely to be negligible.
The generalizability of this study is limited by its observational nature and reliance on a relatively small sample derived from patients attending specialist secondary clinics for managing T2DM within a restricted geographical area. Additionally, the relatively short follow-up duration of <2 years resulted in a low number of MACEs being observed, restricting the ability to detect any association between RHI and MACEs. Furthermore, the duration of diabetes was calculated from the time of diagnosis, as documented in clinical notes, and did not account for the influence of any period of impaired glucose tolerance prior to diagnosis and treatment. Similarly, cross-sectional assessments do not account for the influence of long-term glycemic and blood pressure control on CAD risk and progression. It is also possible that the high use of ACEi and statin therapy in this cohort, and corresponding control of hypertension, masked a relationship between RHI score and CAD.
Conclusions
Endothelial dysfunction, measured by EndoPAT2000, can be predicted by LDL-C and HDL-C levels in patients with T2DM. However, RHI scores are not predictive of asymptomatic CAD or the risk of a future MACE in this population.
Footnotes
Authors’ Note
Acknowledgments
The authors thank the patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the British Cardiac Research Trust (grant number: BCRT/3277/PROCEED), The Tabor Foundation, The Derrick Smith Trust Social Research Council, The Easa Saleh Al-Gurg Charity Foundation, The Charles Wolfson Charitable Trust, and The Wellington Hospital. Medical writing support to subedit this manuscript was provided by Dr Blair Hesp CMPP of Kainic Medical Communications Ltd (Dunedin, New Zealand) and funded by the British Cardiac Research Trust.