
Abstract
Cardiovascular disease (CVD) remains the major cause of death and disability worldwide, and residual risk after implementing all current therapies is still high. In this context, the latest (2016) European Cardiology Society/European Atherosclerosis Society guidelines recommend that triglyceride (TG)-lowering drugs should be used in high-risk patients with TGs levels >2.3 mmol/L (200 mg/dL), after lifestyle measures fail to lower them. After several neutral CVD outcome trials with n-3 fatty acids, the Reduction of Cardiovascular Events with EPA–Intervention Trial met its primary end point, that is, among patients with elevated TGs levels despite the use of statins, the risk of ischemic events, including cardiovascular death, was significantly lower in those who received 4 g of icosapent ethyl daily. In this review, we comment on the findings of previous and recently published randomized controlled CVD outcome trials assessing n-3 fatty acids supplementation. Both efficacy and safety, as well as future perspectives, are discussed.
Keywords
Introduction
Cardiovascular disease (CVD) remains a major health problem worldwide. 1 Even after implementing all current treatments, residual CVD risk remains high. During the past years, epidemiological, genetic, and biological data on the potential contributors to residual risk strongly suggested that elevated triglyceride (TG) levels (fasting and nonfasting) may represent causal risk factors for atherosclerotic CVD and all-cause mortality. 2,3 This led to a renewed clinical and scientific interest in hypertriglyceridemia and elevated non-high-density lipoprotein cholesterol (non-HDL-C) levels. In this context, the latest (2016) European Cardiology Society/European Atherosclerosis Society guidelines recommend that TG-lowering drugs should be used in high-risk patients with TG levels >2.3 mmol/L (200 mg/dL) when lifestyle measures fail to lower them. 4 Furthermore, non-HDL-C is regarded as a strong independent CVD risk factor, especially in the presence of hypertriglyceridemia, thus being a secondary (after low-density lipoprotein cholesterol [LDL-C]) treatment target. 4
Among lipid-lowering drugs, n-3 fatty acids (ie, eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) can be used at doses of 2 to 4 g/d to lower TG levels. 4 It has been shown that n-3 fatty acids affect serum lipids and lipoproteins, especially very-low-density lipoprotein concentrations. A recent scientific advisory from the American Heart Association (AHA) stated that n-3 (EPA plus DHA) supplementation may be reasonable in patients at high CVD risk, as well as in those with prevalent coronary heart disease (CHD), especially after a myocardial infarction (MI). 5 In the latter patient population, n-3 fatty acid supplementation was shown to significantly reduce CHD mortality, thus justifying this relative safe treatment option. 5 However, results of CVD outcome trials with long-chain n-3 fatty acids have been disappointing, failing to show further reductions in CVD morbidity when combined with statins. Furthermore, meta-analyses on the effects of n-3 fatty acid supplementation on CVD morbidity and mortality reported divergent results. 6,7 These discrepancies may be largely attributed to different formulations and dosages of n-3 fatty acid used as well as to differences in patient populations and duration of n-3 fatty acid administration.
In this narrative review, we comment on the findings of previous and recently published randomized controlled CVD outcome trials assessing n-3 fatty acids supplementation. Both efficacy and safety, as well as future perspectives, are discussed.
Reduction of Cardiovascular Events With EPA–Intervention Trial
In November 2018, the long-awaited results of the Reduction of Cardiovascular Events with EPA–Intervention Trial (REDUCE-IT) trial, a phase III multicenter, double-blind, placebo-controlled, randomized trial, were published. 8 This study met its primary end point demonstrating that among patients with elevated TG levels on a statin, the risk of a major CVD event (combined end point including CVD death, nonfatal MI, nonfatal stroke, unstable angina requiring hospitalization, or coronary revascularization) was significantly lower (by 25%) in patients receiving 2 g of icosapent ethyl (IPE), a highly purified EPA, twice daily (ie, total daily dose of 4 g), compared with those on placebo. 8 Briefly, patients enrolled (n = 8179; mean age = 64 years; 71.2% men) had baseline LDL-C between 41 and 100 mg/dL (median LDL-C = 75 mg/dL) and fasting TGs between 135 and 499 mg/dL (median TGs = 216 mg/dL) with either established CVD (70.7%, secondary prevention cohort) or diabetes mellitus (DM) and ≥1 other CVD risk factor (primary prevention cohort). Patients were followed up for a median of 4.9 years. 8
The risk of the primary composite end point assessed in a time-to-event analysis was significantly lower in patients taking IPE compared with placebo (22% vs 17.2%, hazard ratio [HR], 0.75; 95% confidence interval [CI], 0.68-0.83; P < 0.001), corresponding to an absolute between-group difference of 4.8% (number needed to treat = 21). This important benefit appeared to occur irrespective of (1) baseline TG concentrations (≥150 or <150 mg/dL, as well as ≥200 vs <200 mg/dL), (2) the attained TGs level at 1 year (≥150 or <150 mg/dL), or (3) the achieved LDL-C levels at 1 year (whether stable, increased, or decreased). 8 These findings suggest that the observed CVD reduction with IPE administration was not related to improvements in TG levels.
In the REDUCE-IT trial, the administration of n-3 fatty acids was generally safe, with similar rates of side effects in both groups. In this context, the overall rates of serious adverse bleeding events were 2.7% in the IPE group and 2.1% in the placebo group (P = 0.06), without any fatal bleeding events. 8 However, hospitalization for atrial fibrillation (AF) or flutter as well as peripheral edema were more frequently recorded in the IPE group than the placebo group (5.3% vs 3.9%, P = .003 and 6.5% vs 5.0%, P = .002). In contrast, the rates of anemia and gastrointestinal adverse events were significantly lower in the IPE group (4.7% vs 5.8%, P = .003 and 33.0% vs 35.1%, P = .04).
Other Randomized Controlled CVD Outcome Trials With n-3 Fatty Acids
Several questions arise following the publication of the REDUCE-IT trial. 8 Are the observed benefits mainly due to the high dose of n-3 fatty acids used (ie, 4 g/d), to the high-risk population studied, or possibly due to the specific n-3 fatty acid preparation used along with the specific high-risk population? A key question now is whether these favorable results reported with REDUCE-IT can be generalized to other n-3 fatty formulations and especially why or why not?
These questions are important since previous studies with n-3 fatty acids have tended to be negative in terms of lowering CVD risk. In this context, in the Risk and Prevention Study, 9 12 513 patients (mean age = 64.0 years; 61.5% men) with either atherosclerotic vascular disease (but not MI; 29.5% of the total population) or multiple CVD risk factors were randomly assigned to either n-3 fatty acids (1 g daily, n = 6244) or placebo (olive oil, n = 6269) and were followed up for a median of 5 years. No difference was observed in the rate of the primary combined end point (nonfatal stroke, nonfatal MI, or CVD death) between the 2 groups (HR, 0.97; 95% CI, 0.88-1.08; P = .58). 9 Of note, baseline fasting TGs were 150 mg/dL (ranging from 105 to 200 mg/dL in the n-3 fatty acids group and from 107 to 201 mg/dL in the placebo group) and the n-3 fatty acids administered were EPA and DHA (in a ratio ranging from 0.9:1 to 1.5:1). Furthermore, during the 5-year follow-up, TG levels had a more significant reduction in patients on n-3 fatty acids than in those on placebo (−28.2 ± 1.3 vs −20.1 ± 1.3 mg/dL; P < .001). On the other hand, HDL-C was slightly increased in patients taking n-3 fatty acids (+0.24 ± 0.2 vs −0.3 ± 0.2 mg/dL; P = .04). 9 Low-density lipoprotein cholesterol was similarly decreased in both groups (−21.9 ± 0.5 vs −21.5 ± 0.5 mg/dL; P = .63).
An analogous result was also reported in the Outcome Reduction with an Initial Glargine Intervention trial (n = 12 536 patients at high risk of CVD with impaired glucose metabolism who were treated with either 1 g n-3 fatty acids daily or placebo). The mean age of the patients was 63.5 years and approximately 35% of them were female. The administration of n-3 fatty during a median follow-up of 6.2 years did not affect the rates of major vascular events (9.1% vs 9.3%; HR, 0.98; 95% CI, 0.93-1.10; P = .81), total mortality (HR, 0.98; 95% CI, 0.89-1.07; P = .63), or death from arrhythmias (HR, 1.10; 95% CI, 0.93-1.30; P = .26). 10 Of note, 1 g of n-3 fatty acids contained 465 mg of EPA and 375 mg of DHA, whereas the placebo contained approximately 1 g of olive oil, 59% of the patients had a history of MI, stroke, or revascularization, and median TG levels at baseline were 142 (99-196) and 140 (97-195) mg/dL for the n-3 fatty acid and placebo groups, respectively. 10 In this trial, n-3 fatty acid supplementation reduced fasting TG levels significantly more than placebo (−23.5 ± 3.0 vs −9.0 ± 3.0 mg/dL; P < .001), whereas there were no other significant between-group differences in terms of lipids, glucose, glycated hemoglobin, blood pressure, or heart rate.
More recently, in the ASCEND (A Study of Cardiovascular Events in Diabetes) trial, n-3 fatty acid supplementation (1 g daily, containing 460 mg of EPA and 380 mg of DHA) did not reduce CVD events, total mortality, or CVD mortality, in comparison to olive oil alone. The ASCEND consisted of 15 480 patients (mean age = 63.3 years; 62.6% men) with DM free of CVD at baseline who were followed up in the study for a mean of 7.4 years. 11 Of note, the ASCEND trial measured nonfasting lipids. Similarly, the Vitamin D and Omega-3 Trial (VITAL) trial showed that supplementation of n-3 fatty acids (1 g daily; 840 mg EPA + DHA) did not affect CVD morbidity and mortality in 25 871 individuals without CVD at baseline (mean age: 67.1 years; 49.4% men) who were followed up for a median of 5.3 years. 12 However, subgroup analyses showed that n-3 fatty acids supplementation led to significant CVD benefits in those with lower dietary fish intake, in African Americans, and those with comorbidities. 12 Of note, there is no information regarding fasting status of lipid measurements in this trial. Why ASCEND and VITAL were negative is not clear. The presence/absence of CVD may be relevant as is the dose and type of n-3 formulation used.
In contrast, the GISSI (Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico)-Prevenzione trial 13 (n = 11 324 patients with a recent MI [≤3 months]; mean age = 59.4 years; approximately 85% men) showed that dietary supplementation with n-3 fatty acids (1 g daily; 850-882 mg EPA and DHA in an average ratio of 1:2) for 3.5 years led to significant reductions in the primary end point of all-cause death, nonfatal MI, and nonfatal stroke compared with controls (risk ratio [RR], 0.86; 95% CI, 0.74-0.99; P = .048). The benefit was attributed to decreases in the risk of CVD and all-cause mortality (by 30% and 20%, respectively) as well as of sudden death (by 45%). Of note, mean baseline TG levels (no information was given regarding fasting status) were 162 mg/dL and they were significantly decreased only in the n-3 fatty acid group (by approximately −3%; P = .0001 vs controls), whereas HDL-C increased in both groups (by approximately 9%). 13 Low-density lipoprotein cholesterol was increased by approximately 10% in the n-3 fatty acids group and by approximately 3% in the control group (P = .002). Similarly, in the Japan Eicosapentaenoic acid Lipid Intervention Study (JELIS) trial (n = 18 645 patients with total cholesterol ≥6. mmol/L [251 mg/dL]; mean age: 61 years; 31% men; mean follow-up: 4.6 years), supplementation of 1800 mg of EPA daily plus a statin was found to significantly reduce the primary combined end point (including fatal and nonfatal MI, sudden cardiac death, unstable angina pectoris, angioplasty, stenting, or coronary artery bypass grafting) compared with statin monotherapy alone (19% relative reduction in the primary end point). 14 Median baseline TG levels (no information available regarding fasting status) were 1.74 (1.25-2.49) mmol/L (154 [111-220] mg/dL) for the combined therapy group and 1.73 (1.23-2.48) mmol/L (153 [109-220] mg/dL) for the statin monotherapy group, and they were decreased by 9% and 4% in the EPA and control groups, respectively (P < .0001). In both groups, total cholesterol and LDL-C were also decreased (by 19% and 25%, respectively), whereas HDL-C was slightly increased. 14
Potential Explanations for Differences in CVD Outcome Trials With Different n-3 Fatty Acid Doses and Preparations
The reasons for the discrepancies in the results of the abovementioned CVD outcome trials remain to be elucidated, but several possible explanations can be hypothesized. For example, the dose of n-3 fatty acids supplements (1 g daily) used in the neutral studies was lower than those administered in the positive JELIS (1.8 g daily) 14 and REDUCE-IT (4 g daily) trials. 8 However, it should be noted that the same dose (ie, 1 g daily) of n-3 fatty acids was also used in the positive GISSI-Prevenzione trial 13 and that the daily supplementation of 1.8 g of n-3 fatty acids in the JELIS trial involved a Japanese population who are known to consume more fish than others and thus some would expect that such a low dose of “extra” n-3 fatty acid intake would not affect CVD risk. Furthermore, duration of follow-up ranged from a median of 3.5 (GISSI-Prevenzione trial) 13 to 7.4 years (ASCEND trial) 11 and primary end points varied across these trials (Table 1).
Summary of Randomized Controlled Cardiovascular Outcome Trials With n-3 Fatty Acid Supplementation.
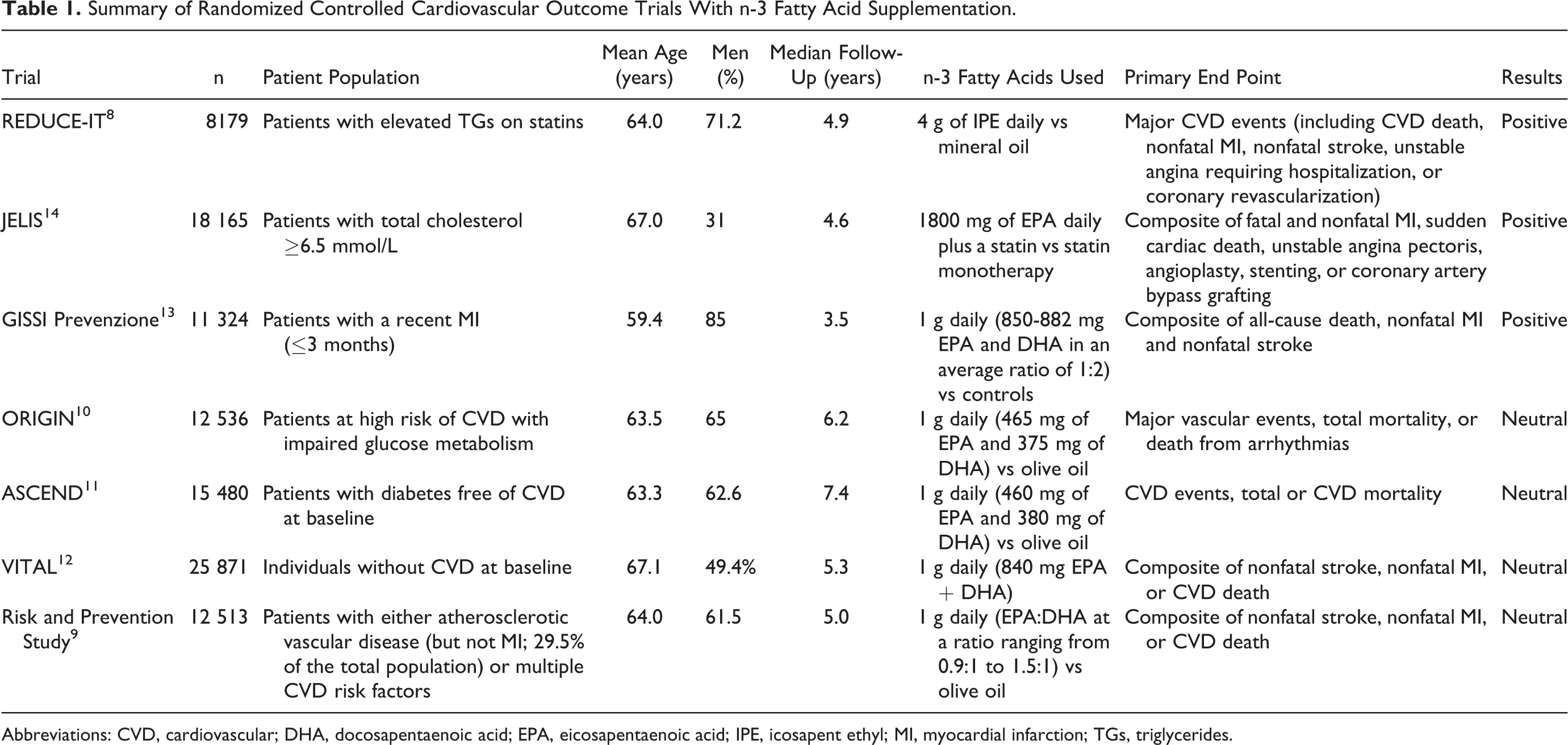
Abbreviations: CVD, cardiovascular; DHA, docosapentaenoic acid; EPA, eicosapentaenoic acid; IPE, icosapent ethyl; MI, myocardial infarction; TGs, triglycerides.
The exact type and amount of n-3 PUFAs administered were also slightly different. In this context, one must be cautious when generalizing the results of the REDUCE-IT trial, where only IPE, a high-purified form of EPA, was used compared with other n-3 fatty formulations and especially the combination of EPA and DHA which was administered in other trials. The results of the ongoing STRENGTH (Statin Residual Risk Patients With Hypertriglyceridemia) trial with supplementation of 4 g of Epanova daily will further elucidate the CVD effects of different n-3 fatty acids. 15 Furthermore, it has been suggested that statin use may diminish the beneficial impact of n-3 fatty acids on CVD events. 16 In this context, in post-MI patients participating in the Alpha Omega Trial, daily administration of 400 mg EPA + DHA plus 2 g α-linolenic acid was reported to significantly lower major adverse CV events (by 54%) only in statin nonusers (n = 413) and not in statin-treated patients (n = 3740). 16 Of note, TG levels were significantly reduced only in statin users. Furthermore, 71% of the patients in the GISSI-Prevenzione trial 13 did not take a statin (since there were no definitive data on their efficacy for CVD prevention when the trial was started), which could explain the observed positive results. These findings suggest that statins may inhibit the cardioprotective effects of n-3 fatty acids. Mechanisms potentially involved in this interaction include (1) statin-induced increase in arachidonic acid levels (ie, the main n-6 fatty acid), thus favoring n-6 fatty acids in the n-3/n-6 interplay, and (2) counteraction at the mitochondria level between statins and n-3 fatty acids. 17 Another suggestion is that n-3 fatty acids supplements could be protective in terms of CVD risk only in patients who are n-3 deficient. 17 These issues remain to be further elucidated in future trials. Of note, all patients were on a statin in the JELIS 14 and the REDUCE-IT trials. 8
The supplementation of EPA plus DHA has been previously approved for the treatment of adults with severe hypertriglyceridemia or for secondary prevention in patients with CVD or heart failure. 5 In this context, the Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction study, a randomized, double-blind, placebo-controlled trial, showed that supplementation of 4 g of n-3 fatty acids (containing 465 mg EPA plus 375 mg DHA) was a safe and effective treatment in improving cardiac remodeling in patients receiving current guideline-based post-MI therapies. 18 This finding was supported by the attenuation of concurrent fibrosis within the noninfarcted myocardium and the lower levels of systemic biomarkers of myocardial inflammation and cardiac fibrosis.
The ROMANTIC trial (Rosuvastatin-OMAcor iN residual hyperTrIglyCeridemia), a randomized, double-blind, placebo-controlled trial, the combination of rosuvastatin 20 mg plus 4 g of n-3 fatty acids (DHA + EPA) daily achieved a greater reduction in TG levels and non-HDL-C than rosuvastatin alone in patients with residual hypertriglyceridemia. 19 These additive TG-lowering effects were observed independent of age, gender, DM, and chronic kidney disease. Both EPA and DHA have been shown to reduce TG levels. However, they are known to have differing effects on LDL-C and HDL-C. 20 –22 In this context, compared with EPA, DHA can suppress LDL-receptor activity and thus consequently increase LDL-C levels. However, these effects are not accompanied by increased non-HDL-C, which is thought to provide a better indication of CVD risk in patients with elevated TG levels. 20,23 Furthermore, DHA may exert more potent antiaggregatory effects than EPA 24 and it has also been reported to lower blood pressure and heart rate. 25,26 On the other hand, EPA may promote improved endothelial function and plaque stability, 27,28 as well as a decrease in apolipoprotein C-III levels 29 and exert anti-thrombotic, antioxidant, and anti-inflammatory properties. 30,31 In this context, IPE administration significantly decreased C-reactive protein (CRP) levels in the REDUCE-IT trial. 8 This effect could provide a possible explanation for the observed CVD benefits that were independent of IPE TG-lowering properties. However, Kaplan-Meier curves in REDUCE-IT separated at 2 years, which appears less consistent with an anti-inflammatory or antithrombotic mechanism of action and more with a lipoprotein-mediated pathway, as mentioned in the accompanying editorial of the trial. 32 In the same editorial, the use of mineral oil as placebo was also commented on, highlighting the probability that the observed positive CVD effects with IPE supplementation could have been exaggerated due to the mineral oil–induced increases in lipoproteins and CRP levels in the placebo group. Statin absorption could also have been affected by mineral oil, thus increasing the CVD risk of the placebo group. However, it should be noted that the small differences in LDL-C concentrations cannot explain the 25% reduced CVD risk in the IPE group (as also supported by a post hoc analysis showing that the observed CVD benefits were independent of LDL-C changes). 8 It is also of note that mineral oil has not been reported to increase CVD risk in the medical literature.
Safety Issues With IPE Supplementation in the REDUCE-IT Trial
Icosapent ethyl was generally well tolerated in the REDUCE-IT trial. 8 The modest increase in major bleeding events with both IPE and placebo (2.7% vs 2.1%; P = .06) in this trial could be attributed to effects on platelet aggregation. Furthermore, since the majority of the patients had established CVD, one could speculate that they would be on antiplatelet therapy (although this was not reported in the trial). The interactions of IPE with antiplatelet drugs should be further investigated.
The rates of AF and peripheral edema were significantly higher in the IPE than the placebo group in the REDUCE-IT trial (5.3% vs 3.9% and 6.5% vs 5.0%, respectively). 8 In addition, hospitalization for AF or flutter was significantly more frequent in the IPE than in the placebo group (3.1% vs 2.1%). 8 Although the absolute increases in AF, peripheral edema, and hospitalizations for AF/flutter were only 1.4%, 1.5% and 1.0%, respectively, the numbers could become clinically significant if numerous patients worldwide were to start taking these supplements. Furthermore, on a long-term basis, such side effects could adversely affect individual CVD risk, cost of treatment, and quality of life. The underlying mechanisms for these side effects remain unknown. Whether they represent a dose- or product-related adverse event, increase with duration of treatment, or more frequently occur in certain patient populations who are prone to such arrhythmias (eg, the elderly patients) will have to be elucidated in future studies.
In our opinion, these side effects are substantial, should be taken into consideration in patient selection for IPE supplementation in clinical practice, and require clarification. In this context, we are surprised that they were not discussed more extensively in the REDUCE-IT trial publication, 8 as well as in the accompanying editorial. 32 In fact, the editorial adds a confounding declaration regarding the increased AF observed in the IPE group in the REDUCE-IT trial by stating that n-3 fatty acids may actually exert antiarrhythmic properties (which has been previously reported) 33 and then going on to state that such effects could not account for all the benefits seen in the REDUCE-IT trial. 8
Conclusions and Future Perspectives
After several neutral CVD outcome trials with n-3 fatty acids, the REDUCE-IT trial found a substantial clinical benefit in terms of major adverse CVD events with IPE administration at a dose of 4 g daily. Nevertheless, there is a need for further evidence to elucidate the role of n-3 fatty acids in reducing CVD risk, especially in patients with established CVD or hypertriglyceridemia (with or without obesity, diabetes, metabolic syndrome, nonalcoholic liver disease, etc).
The exact type, amount, and duration of n-3 fatty acid supplementation needed as well as the patient populations that will benefit more from this therapeutic strategy and the underlying mechanisms of any CVD benefits remain to be established. Ongoing studies, such as the Randomized trial for Evaluation in Secondary Prevention Efficacy of Combination Therapy–Statin and Eicosapentaenoic Acid (UMIN000012069), the Effect of Vascepa on Improving Coronary Atherosclerosis in People With High Triglycerides Taking Statin Therapy (NCT02926027), and STRENGTH (NCT02104817) trials, will provide more data in this field. Furthermore, postprandial hypertriglyceridemia has been linked to increased CVD risk. 34,35 There is evidence that some n-3 fatty acids formulations can reduce postprandial TG levels, 3,36 –38 but further research is needed in this field. Whether such effects will affect CVD risk remains to be established in the future.
From a clinical point of view and based on all available evidence, n-3 fatty acids may be an effective treatment option for patients with high-risk CVD to reduce the risk of major CVD events, as well as residual risk. However, if a significant benefit with this new n-3 fatty acid formulation is seen in a trial (ie, REDUCE-IT) lasting a median of 4.9 years, 8 will some adverse events (ie, AF/flutter and edema) reduce its longer-term efficacy and safety? In view of the unexpected incidence of AF/atrial flutter associated with this specific omega-3 formulation, further research is urgently needed to confirm these findings and especially assess them in the longer-term and in specific categories of patients. Finally, physicians should always consider other risk factors, such as smoking, diabetes, hypertension, obesity, and hypercoagulation (and not only TG levels) to minimize residual CVD risk. There is a need for more trial-based evidence before n-3 can be strongly recommended for CVD prevention. They remain useful agents to treat hypertriglyceridemia.
Footnotes
Authors’ Note
Pablo Perez-Martinez and Niki Katsiki are equal contributors. P.P.-M. has given talks and participated in trials sponsored by Astra Zeneca, Merck Sharp & Dohme, Boehringer Ingelheim, Eli Lilly, Novartis, Ferrer, Esteve, GlaxoSmithKline, Pfizer, Janssen-Cilag, Amgen and Sanofi. N.K. has given talks, attended conferences, and participated in trials sponsored by Amgen, Angelini, Astra Zeneca, Boehringer Ingelheim, MSD, Mylan, Novartis, Novo Nordisk, Sanofi, Servier and WinMedica. DPM has given talks and attended conferences sponsored by MSD, AstraZeneca, and Libytec.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.