
Abstract
The PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy (PRECISE-DAPT) score has been validated to predict bleeding complications in patients undergoing stent implantation and dual antiplatelet therapy. This score does not include the platelet count (PC), which has been shown to be an independent marker of mortality in patients with acute coronary syndrome (ACS). We assessed the role of the PRECISE-DAPT score calculated on admission for mortality risk prediction and evaluated whether the predictive accuracy of this score improved by adding the PC. In a retrospective cohort study of 1000 patients with ACS, after adjustment for relevant covariates, a PRECISE-DAPT score ≥25 was independently associated with mortality (hazard ratio [HR]: 7.91; 95% confidence interval [CI]: 4.37-14.30). When this score was combined with PC, compared to patients with PRECISE-DAPT <25 and PC ≥150 × 109/L, the adjusted HR was 7.2 (95% CI 2.4-21.6) for those with PRECISE-DAPT <25 and PC <150 × 109/L; 10.7 (95% CI: 5.2-21.9) for those with PRECISE-DAPT ≥25 and PC ≥150 × 109/L; and 17.9 (95% CI 7.0-45.4) for those with PRECISE-DAPT ≥25 and PC <150 × 109/L. Selecting thresholds for high-risk designation, the PRECISE-DAPT score integrated with PC had a higher prediction value, compared to the PRECISE-DAPT and Global Registry of Acute Coronary Events scores.
Introduction
Acute coronary syndromes (ACSs) represent one of the leading causes of overall mortality and subsequent major adverse cardiovascular events (MACEs). 1 Over the last 20 years, pharmacoinvasive strategies have been shown to reduce mortality and the risk of recurrent ischemic events. 2 –4 However, overall mortality remains high because of increasing patient age and comorbidities resulting in a frailty condition also affecting the mid- and long-term bleeding risk. 5 Since the most relevant predictors of bleeding risk might also affect the risk of mortality, recently released risk stratification tools have tried to address the complex trade-off between bleeding and ischemic events. 6 –8
The PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy (PRECISE-DAPT) score has been endorsed by the most recent European Society of Cardiology Guidelines on DAPT duration to inform on decision-making. 6 It includes 5 covariates that are associated with bleeding risk (age, leukocyte count, chronic kidney failure, previous bleeding, and hemoglobin level). Many of these covariates have been frequently associated with ischemic risk including mortality. This might explain why data from retrospective registries suggested that the PRECISE-DAPT score might also help risk-stratify patients for mortality; previous studies have also suggested a noninferior performance compared to the Thrombolysis in Myocardial Infarction risk score with regard to in-hospital mortality. 9,10
Platelets play a crucial role in several processes beyond hemostasis and thrombosis, such as inflammation, wound healing, angiogenesis, and maintenance of vascular integrity. 11 Through their interaction with other cellular effectors of both innate and adaptive immunity, platelets have emerged as modulators of progression of both atherosclerosis and atherothrombosis. 12 This explains why a decreased baseline platelet count (PC) has been associated with long-term bleeding events, MACE, and overall mortality. 13 –15 However, PC has not been included in the available risk assessment tools.
Therefore, the aim of this study was to test the role of the PRECISE-DAPT score calculated on admission for predicting long-term mortality and to evaluate whether the predictive accuracy of this score is improved by adding the PC.
Methods and Results
Methods
We conducted a cohort study of 1000 consecutive patients with ACS admitted to the Intensive Coronary Care Unit of ASST Grande Ospedale Metropolitano Niguarda in Milan between January 2014 and September 2017 and followed in a prospective database. No exclusion criteria were applied, and all patients had complete items for the PRECISE-DAPT score calculation.
Clinical, laboratory, procedural, pharmacological, and follow-up data of every enrolled patients were collected. Comorbidities were evaluated using the Charlson comorbidity index (CCI), an extensively adopted risk adjustment tool that measures the effect of multiple comorbidities on mortality using International Classification of Diseases, 9th Edition, diagnosis codes. 16,17
Assessment of left ventricular ejection fraction was performed according to the European Association of Cardiovascular Imaging and the American Society of Echocardiography recommendation. 18
Significant coronary stenosis was defined as any lumen diameter ≥50% in one of the major epicardial coronary arteries including left main coronary artery (LMCA), left anterior descending artery (LAD), left circumflex coronary artery (LCX), and right coronary artery. The involvement of LMCA was regarded as bivessel disease (concurrent stenosis of LAD and LCX).
The PRECISE-DAPT score was calculated on admission for all patients with available information, according to the definitions used in the developmental cohort. 6 In that cohort, the estimated glomerular filtration rate (eGFR) had been calculated using the Cockcroft-Gault formula in the PRODIGY, RESET, EXCELLENT, ZEUS, OPTIMIZE, and SECURITY trials (developmental cohort) and PLATO (validation cohort) trial, whereas the Modification of Diet in Renal Diseases (MDRD) formula had been used in the BIOSCIENCE and COMFORTABLE-AMI trials (developmental cohort) and in Bern PCI registry (validation cohort). 6
However, data from “real-world” registries indicate that the eGFR calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation 15 is able to reclassify patients into a different and more appropriate Kidney Disease Improving Global Outcomes stratum, being less biased than the MDRD equation and Cockcroft-Gault formula. 19 –21 Furthermore, the CKD-EPI equation has been shown to improve prognostic stratification in patients with established coronary artery disease. 22 Therefore, for the purpose of this study, the eGFR calculated using the CKD-EPI equation was included in the PRECISE-DAPT score. The PRECISE-DAPT score was dichotomized according to the original cut point (<25 vs ≥25).
Platelet count was categorized into 2 classes (<150 × 109/L; ≥150 × 109/L), considering the distribution of our sample (Figures 1 and 2) and population data. 23 Patients with thrombocytosis (ie, >450 × 109/L) were included in the ≥150 × 109/L group considering the rarity of this condition (15 patients, 1.5%). Chart review of these patients revealed that thrombocytosis was either reactive in nature or associated with the presence of underlying myeloproliferative neoplasm in a half of cases each.
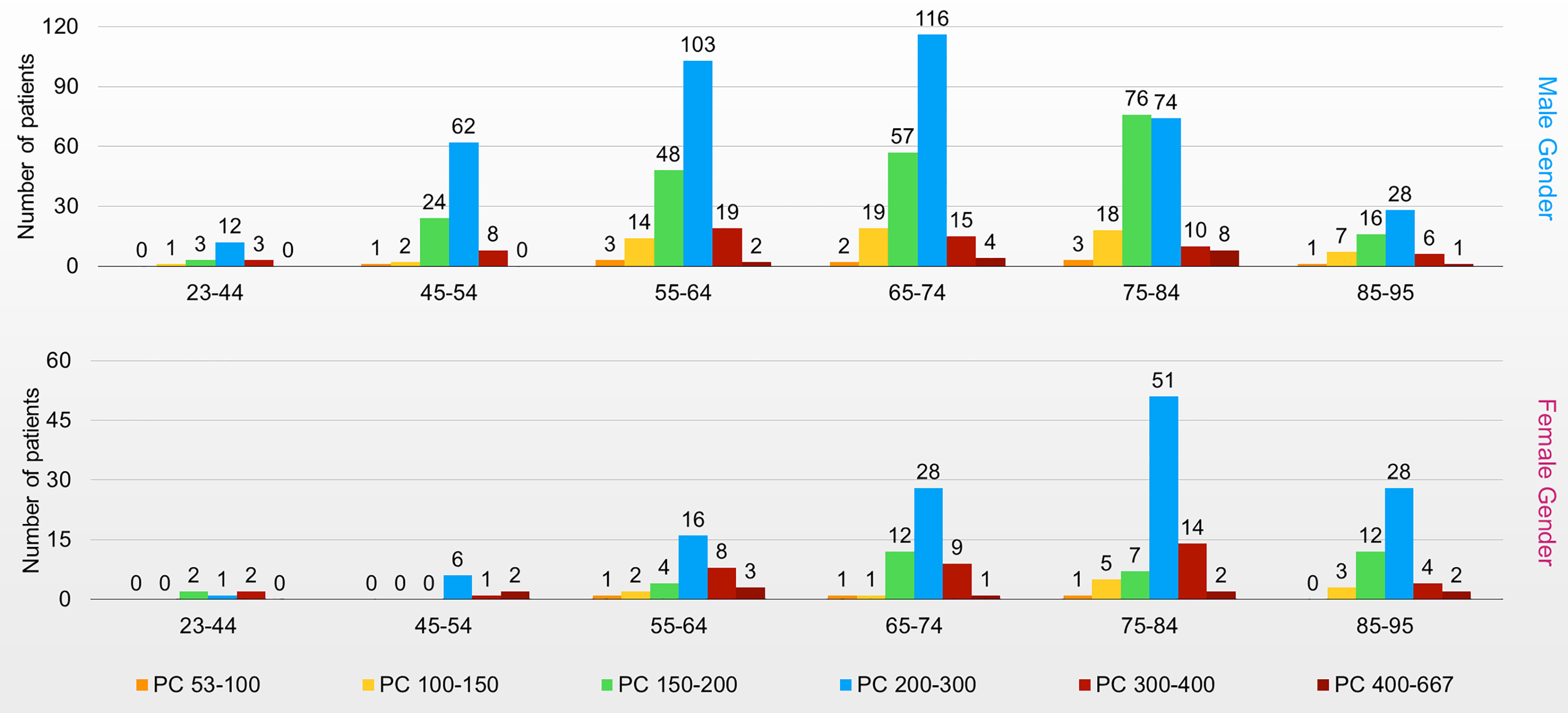
Platelet count (PC) distribution according to age classes and gender.
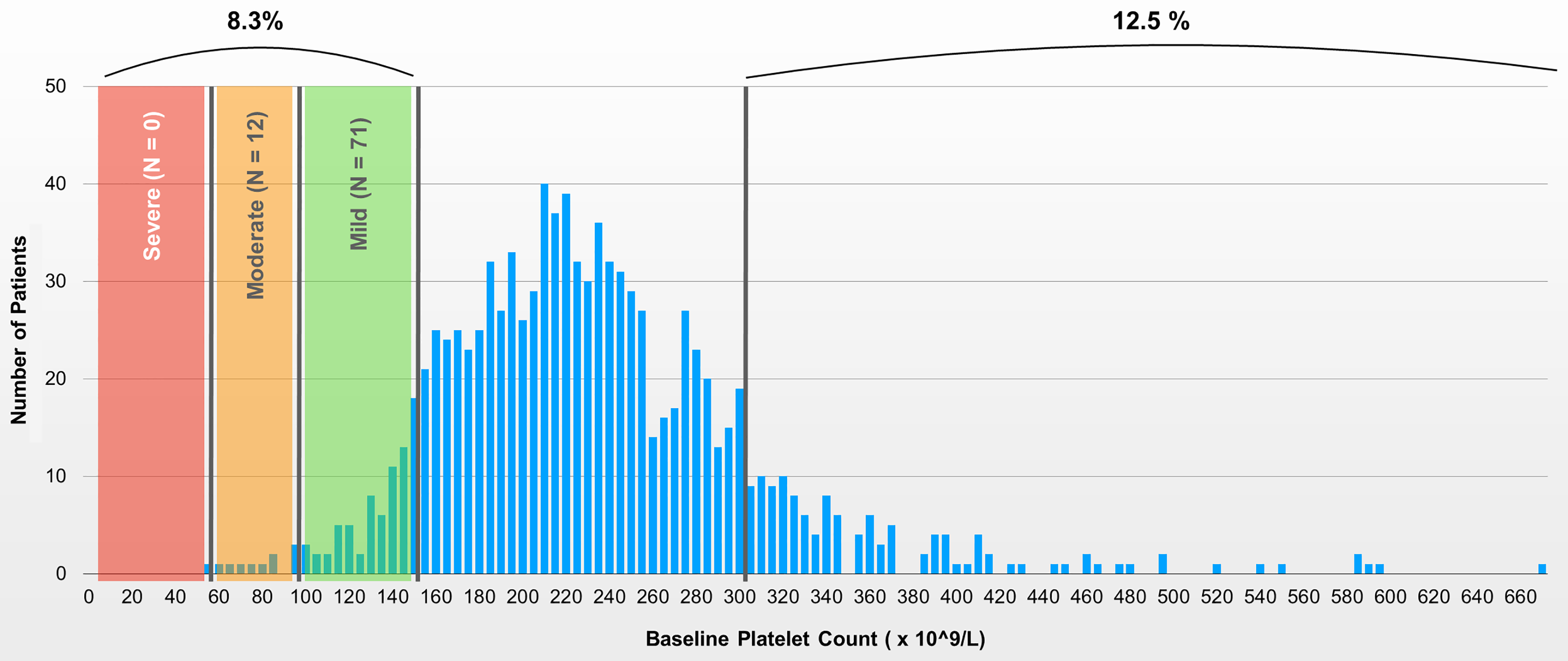
Distribution of platelet count at baseline.
The study was conducted in accordance with ethical principles based on Helsinki’s Declaration (current version: World Medical Association, 64th General Assembly, Fortaleza, Brazil, October 2013), International Conference on Harmonisation for Good Clinical Practice, and the current regulatory laws.
End Point Definition
The primary end point was overall mortality. As secondary end point, we considered the occurrence of bleeding events defined as Bleeding Academic Research Consortium score ≥2 and MACE defined as the composite of the following events: death from all causes, recurrent ACS, new cardiovascular hospitalization, and stroke.
Data Analysis
Sample size
One thousand patients with ACS with ≥12-month follow-up were present in the study database. Based on the available literature, 15,24 1-year survival rate was estimated to be 75% in patients with PC alterations and 85% in patients with close to median PC. Based on these assumptions, a log-rank assay would have had more than 97% potency in discriminating a 10% survival difference between 2 cohorts of 500 patients, with an α error of 5%.
Statistical Analysis
Continuous variables were tested for normality using the Shapiro-Wilk test and are reported as mean and standard deviation if normally distributed or medians and 25th and 75th percentiles if they did not satisfy the normal assumption. Categorical variables are shown as frequencies and percentages in each group. Median follow-up was calculated using the reverse Kaplan-Meier method. 25 To determine the potential effect of the PRECISE-DAPT score and PC (separately and combined) on overall mortality, bleeding events, and MACE, we fitted Cox proportional hazards models adjusted for gender, previous myocardial infarction (MI), and ST-segment elevation as admission diagnosis. Results were expressed as hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for patients with follow-up mortality versus patients who survived. Visual inspection of the Schoenfeld residual plot and the test proposed by Grambsch and Therneau 26 were used to assess the proportional hazard assumption. Using the linear predictor fitted by the Cox regression adjusted models, we performed the time-dependent receiver operating characteristic (ROC) curve analysis, 27 and the corresponding area under the curve (AUC), to evaluate the predictive accuracy for 1-year mortality of the PRECISE-DAPT score (adjusted for the confounders) or adding the PC (<150 × 109/L/≥150 × 109/L). We then computed the p value for testing the null hypothesis that 2 time-dependent AUCs of 2 markers from the same sample are equal. 28
Since the Global Registry of Acute Coronary Events (GRACE) score is the most commonly used risk score to estimate mortality in patients with ACS, 29 the predictive accuracy of the PRECISE-DAPT score (adjusted for confounders and adding the platelet levels) was compared to the AUC obtained for the GRACE risk tool.
According to the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis statement, 30 the change in net benefit was performed in order to quantify the incremental value of adding PC to the PRECISE-DAPT score. 31,32 The net benefit is used as an utility measure of risk prediction according to different thresholds. It has the peculiarity to account for costs and benefits of the clinical action following the classification in a population with a given prevalence, being defined on the ground of the joint distribution of the risk predictor and the disease outcome. Its clinical utility depends on the ability to determine the relationship between a chosen predicted probability threshold and the relative value of false-positive and false-negative results. In order to improve the interpretation, the net benefit can be multiplied by 100 or 1000.
The analyses were performed using SAS statistical software (SAS Institute, Cary, North Carolina), version 9.4, R Package “timeROC,” and Stata version 14 software (Stata Corporation, College Station, Texas).
Results
Baseline Characteristics
As shown in Figure 2, 83 (8.3%) patients had PC <150 × 109/L: 12 of 83 with PC between 50 and 100 × 109/L; none with PC <50 × 109/L. The distribution of demographic characteristics, risk factors, medical history, and other selected variables, according to platelet levels, is shown in Table 1. The median age of the population was 67 years (interquartile range [IQR]: 58-77). Patients with PC <150 × 109/L were older and had more frequently a history of coronary artery disease (previous MI, previous coronary artery bypass graft [CABG]) as well as a decreased ejection fraction on admission. They also had more comorbidities as expressed by a higher CCI.
Distribution of Demographic Characteristics, Risk Factors, Medical History, and Other Selected Variables According to Platelets Level in Patients With ACS.a
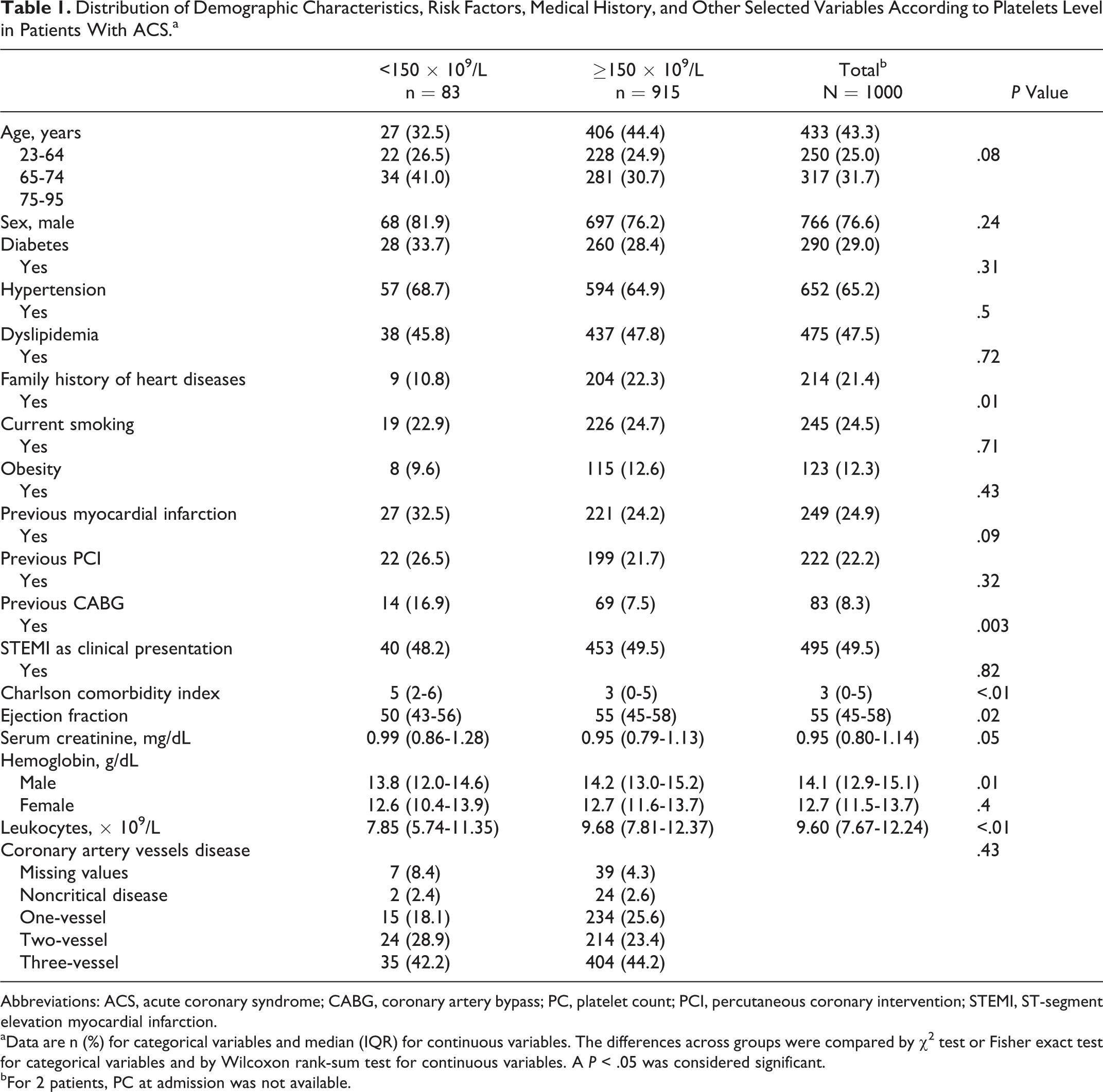
Abbreviations: ACS, acute coronary syndrome; CABG, coronary artery bypass; PC, platelet count; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
aData are n (%) for categorical variables and median (IQR) for continuous variables. The differences across groups were compared by χ2 test or Fisher exact test for categorical variables and by Wilcoxon rank-sum test for continuous variables. A P < .05 was considered significant.
bFor 2 patients, PC at admission was not available.
Patients on oral anticoagulant therapy represented only the 6.3% of the overall population: There were no patients on this treatment in the group with PRECISE-DAPT score <25 and PC <150 × 109/L, whereas in the other 3 groups, this population was almost equally represented.
Percutaneous coronary intervention was performed in 63 (76%) patients with PC <150 × 109/L and in 753 (82%) patients with PC ≥150 × 109/L (P = .149); drug-eluting stents (DESs) were implanted in 52 (63%) patients with PC <150 × 109/L and in 684 (75%) patients with PC ≥150 × 109/L (P = .016). The CABG was performed in 5 (6%) and 50 (5.5%) patients, respectively (P = .80).
Only a few patients discontinued DAPT before 12 (12.9%) months, without any significant difference across groups of PRECISE-DAPT score and PC. However, this information was not accurate for almost 50% of the patients because of recall bias. Clopidogrel was most frequently used in patients with low PC and higher PRECISE-DAPT score (up to 40%).
In-Hospital and Follow-Up Events
Over a median follow-up of 496 days (IQR: 359-760), 76 (7.6%) patients died (33 [3.3%] during index hospitalization), 72 had bleeding events (36 during index hospitalization), and 165 had MACE. The in-hospital and follow-up events, reported according to the categories of PC and PRECISE-DAPT, are detailed in Table 2. Patients with higher PRECISE-DAPT had an increased incidence of in-hospital and follow-up events (both ischemic and hemorrhagic). Bleeding events mostly occurred during index hospitalization, whereas MI and stroke were more frequent after discharge. Patients with PRECISE-DAPT <25 and PC ≥150 × 109/L had the lowest incidence of in-hospital and follow-up events.
Outcome According to PRECISE-DAPT Score and Platelet Count Categories.
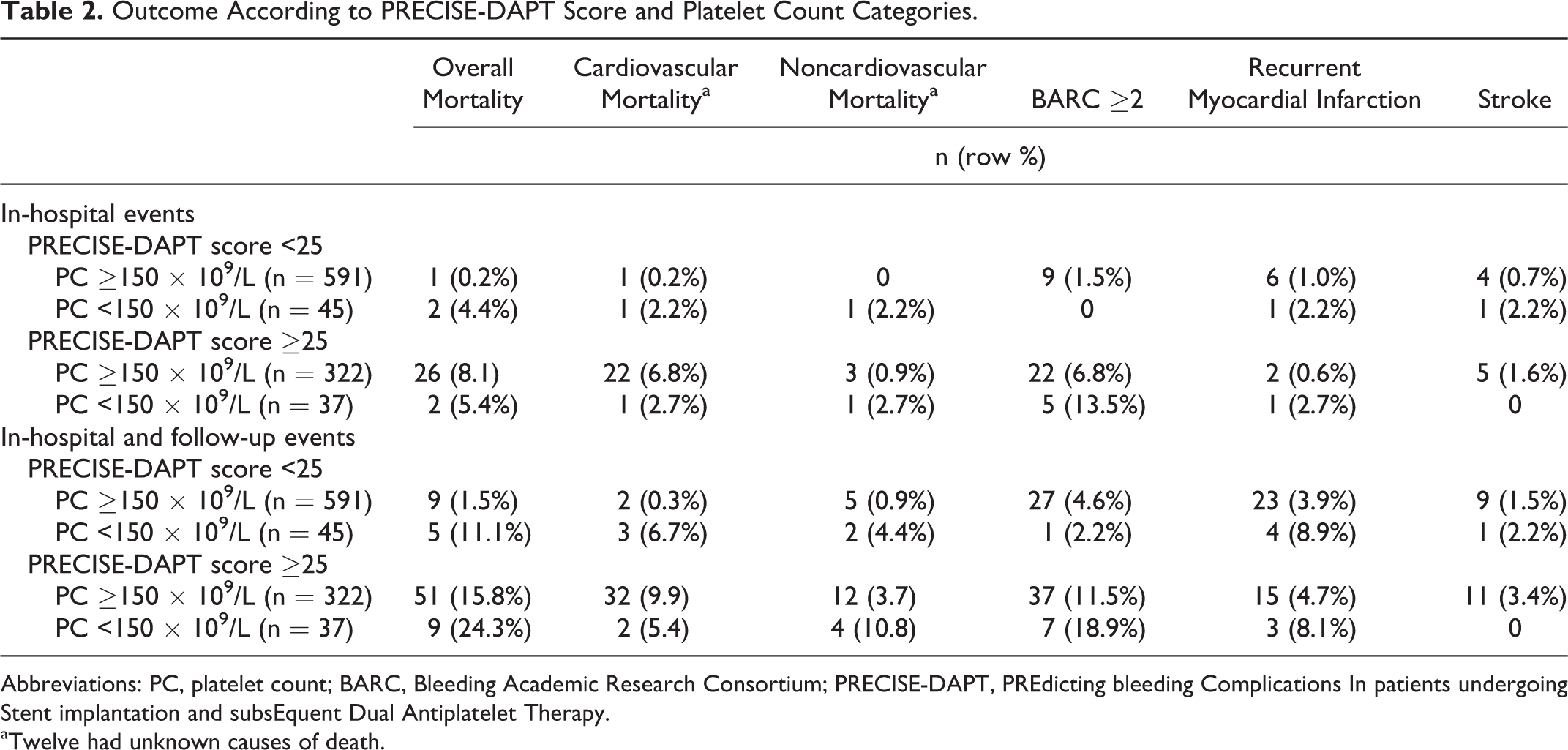
Abbreviations: PC, platelet count; BARC, Bleeding Academic Research Consortium; PRECISE-DAPT, PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy.
aTwelve had unknown causes of death.
Table 3 gives the HRs and corresponding 95% CIs of overall mortality, bleeding, and MACE according to PRECISE-DAPT score and PC categories. A PRECISE-DAPT score ≥25 was attributed to 359 (36%) of 995 evaluable patients. When PRECISE-DAPT score and PC were combined, 591 (59.4%) patients had PRECISE-DAPT score <25 and PC ≥150 × 109/L; 45 (4.5%) patients had PRECISE-DAPT score <25 and PC <150 × 109/L; 322 (32.4%) had PRECISE-DAPT score ≥25 and PC ≥150 × 109/L; and 37 (3.7%) had PRECISE-DAPT score ≥25 and PC <150 × 109/L.
Hazard Ratios (HRs) and Corresponding 95% Confidence Intervals (95% CIs) of Overall Mortality, Bleeding, and Major Adverse Cardiovascular Events (MACEs) According to PRECISE-DAPT Score and Platelet Count (PC) Categories.
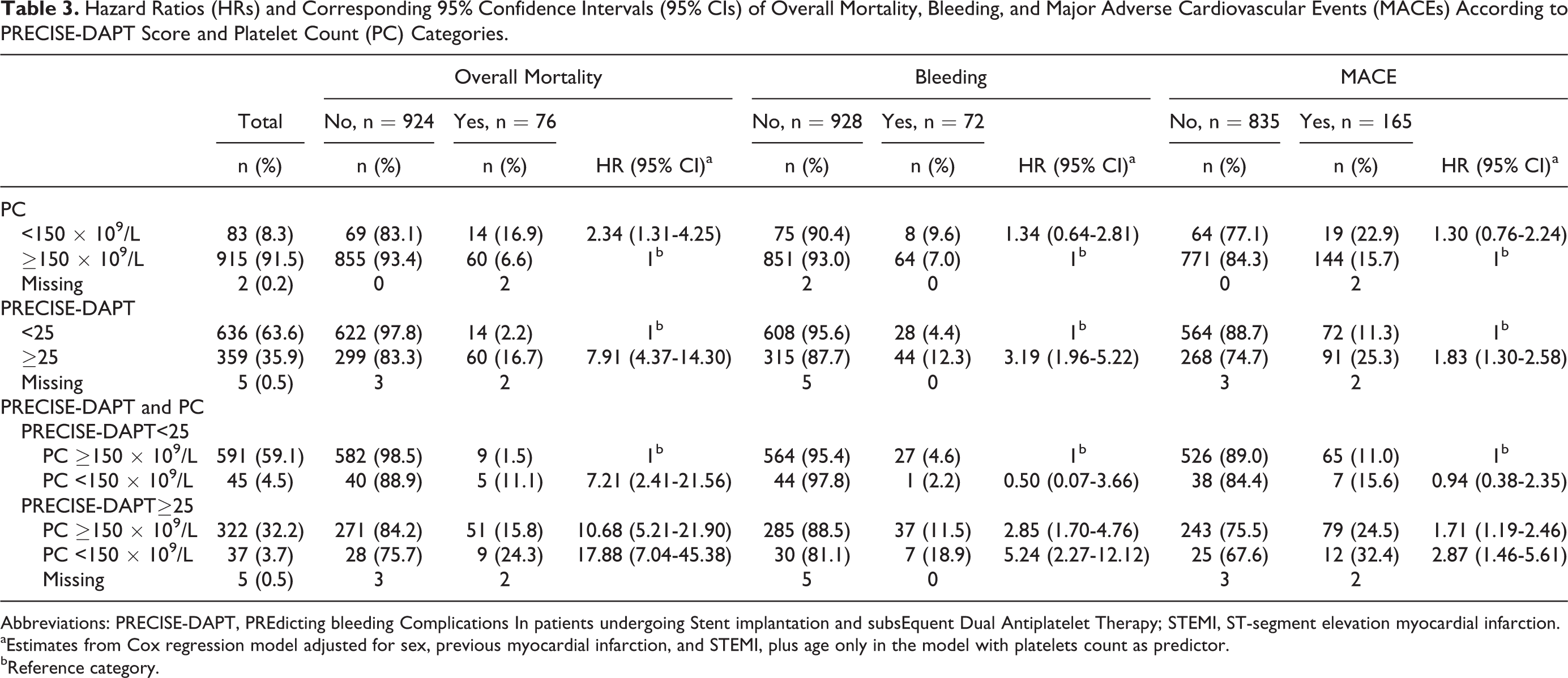
Abbreviations: PRECISE-DAPT, PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy; STEMI, ST-segment elevation myocardial infarction.
aEstimates from Cox regression model adjusted for sex, previous myocardial infarction, and STEMI, plus age only in the model with platelets count as predictor.
bReference category.
After adjustment for sex, previous MI, and ST-segment elevation at presentation, a PRECISE-DAPT score ≥25 was independently associated with mortality (HR: 7.9; 95% CI: 4.4-14.3), with the occurrence of bleeding events (HR: 3.2; 95% CI: 2.0-5.2) and MACE (HR: 1.8; 95% CI: 1.3-2.6). Platelet count <150 × 109/L was independently associated with mortality (HR: 2.3; 95% CI: 1.3-4.3), but not with bleeding events or MACE (HR: 1.3; 95% CI: 0.6-2.8 and HR: 1.3; 95% CI: 0.8-2.2, respectively).
When the PRECISE-DAPT score was combined with PC, compared to patients with PRECISE-DAPT <25 and PC ≥150 × 109/L, the adjusted HR for mortality was 7.2 (95% CI 2.4-21.6) for the group with PRECISE-DAPT <25 and PC <150 × 109/L; 10.7 (95% CI 5.2-21.9) for the group with PRECISE-DAPT ≥25 and PC ≥150 × 109/L; and 17.9 (95% CI 7.0-45.4) for the group with PRECISE-DAPT ≥25 and PC <150 × 109/L (Figure 3). As sensitivity analysis, a further model was performed adjusting for DES implantation. The entity of association between PRECISE-DAPT combined with PC and overall mortality remained substantially unchanged.
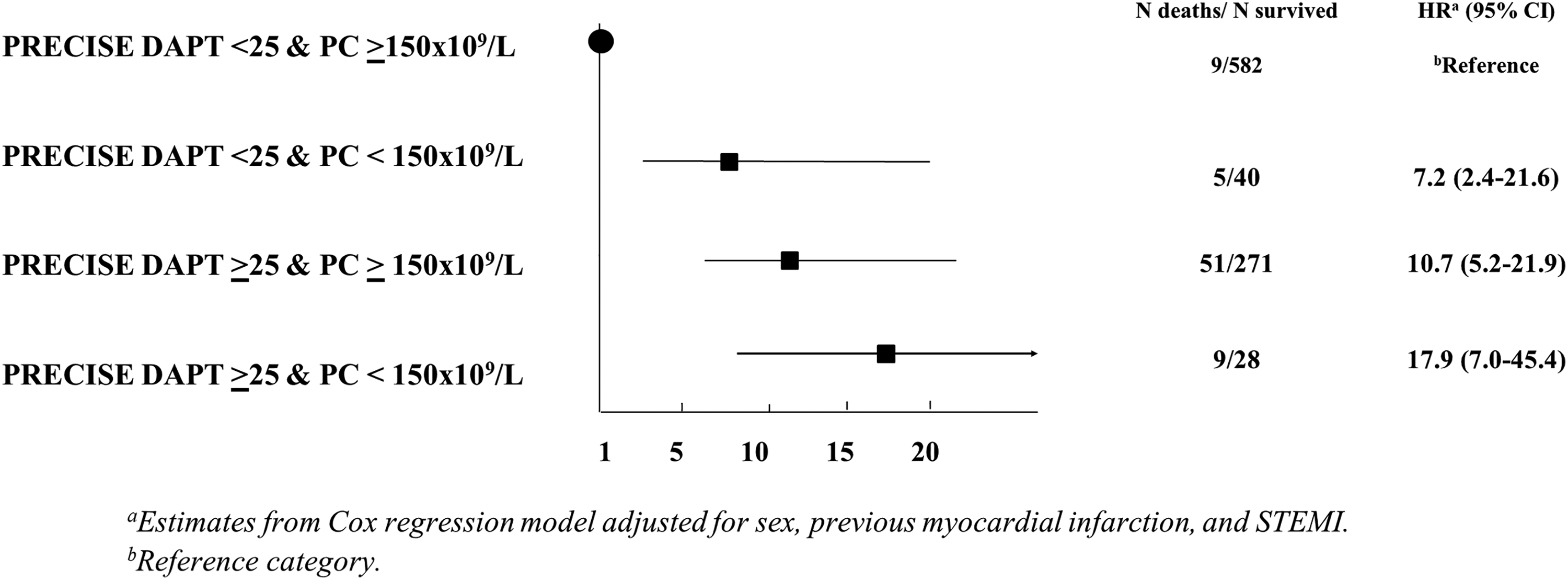
Hazard ratios (Hits) and corresponding 95% confidence intervals (95% CIs) of mortality according to PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy (PRECISE-DAPT) score and platelet count categories.
The proportions of cardiovascular and noncardiovascular mortality were almost equally distributed across all groups except that in those with PRECISE-DAPT ≥25 and PC ≥150 × 109/L, whose cardiovascular mortality was definitely more frequent compared with noncardiovascular mortality (9.9% vs 3.7%).
Risk Model Assessment
Figure 4 shows the time-dependent ROC curves to predict 12-month mortality for the risk model including the PRECISE-DAPT score alone and in combination with PC. The 2 curves were nearly identical and the AUCs around 0.8. Similarly, there were no statistically significant differences between the ROC curve for the PRECISE-DAPT score combined with PC and that for the GRACE score.
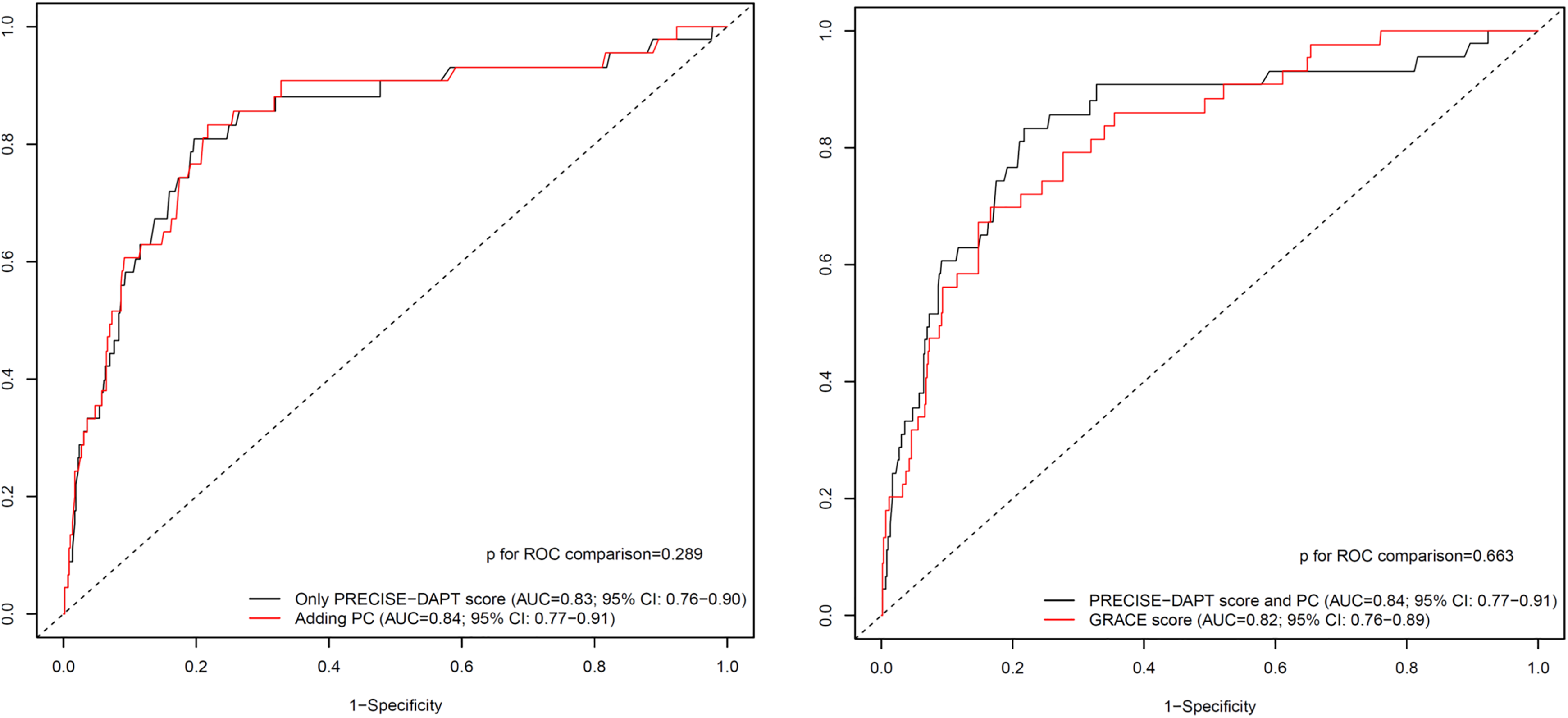
Survival receiver operating characteristic (ROC) curves of the PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy (PRECISE-DAPT) score (alone and extended by platelet count [PC]) and the Global Registry of Acute Coronary Events (GRACE) score for prediction of all-cause mortality after 1 year.
The proportion of true positives and that of false positives across the range of selected thresholds was computed according to the net benefit approach. Selecting thresholds for high-risk designation (≥5%) for 1000 patients who underwent risk prediction at 12-month follow-up, the PRECISE-DAPT score combined with PC was the model with the higher clinical value.
Discussion
The main findings of the present study in a cohort of patients with ACS mostly treated with PCI are the following: (1) the PRECISE-DAPT score on admission is strongly associated with overall mortality (both cardiovascular and non-cardiovascular) as well as with ischemic and bleeding events; (2) thrombocytopenia (TP) and thrombocytosis on admission are relatively rare; and (3) when present, TP is an important prognostic factor able to further improve the discriminatory power of the available stratification tools.
Several clinical prediction rules have been developed for patients with ACS in order to assist physicians in decision-making about invasive management and tailored antithrombotic therapy. 6 –8,33 Since target-lesion failure and target vessel–related MI have significantly dropped over time, thanks to the introduction of second-generation DES and progressive refinement of antithrombotic therapy, 1,3,34 a major issue for patients undergoing PCI has become the fine balance between advanced pharmacointerventional techniques and major bleeding. The PRECISE-DAPT score has been developed in order to improve bleeding risk assessment in patients treated with DAPT after PCI 6 and has been endorsed by the most recently published guidelines on DAPT duration. 4 However, data coming from retrospective registries have suggested that the PRECISE-DAPT score may also perform well as a stratification tool for in-hospital and long-term mortality. 9,10 This might partly be explained by the inclusion of variables that have been shown to be strongly associated with clinical thrombotic and bleeding events after short and long follow-up. 33,35 –49
Moreover, a recent retrospective registry has shown a significant association between the PRECISE DAPT score and the extension of coronary artery disease as evaluated by the Gensini score, 50 being able to discriminate patients at high risk of further ischemia. This was not considered a surprising finding, since each variable included in the PRECISE-DAPT score has been previously linked to coronary artery stenosis. 50
Age and creatinine clearance have been included in the GRACE score, 32 endorsed by the 2015 European Society of Cardiology 34 and 2014 American College of Cardiology/American Heart Association 35 guidelines on non-ST-segment elevation ACS for the quantitative assessment of ischemic risk on admission, considering their role in atherothrombotic burden.
Leukocytes may lead to a hypercoagulable state secondary to increased tissue factor expression. 41 –46 Since its first description by Friedman et al in 1974, 41 the association between white blood cell (WBC) count, as predictor of ACS episodes, and all-cause mortality has been repeatedly confirmed. 42 –46 Furthermore, WBC has been directly correlated with infarct size and high-risk features on presentation 46 and with atherosclerosis progression as well. 51
Low hemoglobin levels may increase myocardial oxygen demand by inducing a need for higher stroke volume and heart rate to maintain adequate systemic oxygen delivery. Conversely, very high hemoglobin levels increase blood viscosity. This underlying pathophysiology may explain the documented J-shaped association between hemoglobin levels and adverse clinical outcomes in patients with ACS. 47,48 Moreover, low hemoglobin levels could be a marker of multimorbidity. 50 Finally, even if the underlying mechanism is unknown, anemia has been associated with more severe coronary artery disease. 52
Platelet count has long been ignored as an event predictor in patients with ACS. Among the available scores for admission stratification in patients with ACS, only the SYNERGY risk score 53 has included low PC as predictor of adverse clinical events. However, data drawn from observational registries in patients with ACS 13,14,15 and from a population study in healthy individuals aged 65 years or more 24 suggest that PC might be a useful baseline clinical parameter to estimate both ischemic and hemorrhagic risk and overall mortality at both short- and long-term follow-up. In a recently published meta-analysis including 16 studies and 190 915 patients with ACS, preexisting TP was not significantly associated with mortality, whereas incident TP was associated with a greater risk of all-cause mortality, MACE, and major bleeding events. 54 The excess mortality risk of patients with abnormal PC is still controversial. 15 The mechanism could be related to occult disease processes affecting patients well-being or a direct role of abnormal PC in different pathways (eg, increasing bleeding events or via platelet involvement in atherosclerotic plaque formation). Indeed, it is well known that platelets are important coordinators of inflammation and both innate and adaptive immune responses, being involved in atherothrombosis and progression of atherosclerosis. 55
In our study population, patients with low PC were older and had a higher burden of previous cardiovascular events (ie, higher frequency of prior CABG and MI) as well as a slightly decreased baseline ejection fraction. However, even adjusting for the most relevant covariates, low PC remained an independent predictor of overall death, thus confirming that PC should be regarded as an “active” pathophysiological effector rather than a proxy of other disorders. Interestingly, patients with low PC were slightly undertreated, with PCI and DES implantation less frequently performed. Nevertheless, the strong association with overall mortality remained even adjusting for these covariates.
This study has several limitations. First, it is a single-center study and end points were self-reported (no adjudication). Second, cutoff values of PC to define TP were arbitrary, although based on the literature and the epidemiology of our study population. Third, as a retrospective study, we cannot exclude the role on unmeasured confounders. Fourth, we tested the PRECISE-DAPT score in a different population compared to that studied in the original manuscript by Costa et al which had included about 60% of patients with ACS and 40% of elective patients with PCI. 6 However, our results were consistent, and the predictive value of the score (alone and extended by PC) was excellent and increased compared to the derivation and validation cohort.
In conclusion, the PRECISE-DAPT score evaluated on admission in patients with ACS is a useful tool to improve bleeding and mortality prediction at 1-year follow-up. Although addition of PC only slightly improves the clinical value of this score, within each PRECISE-DAPT category, patients with lower PC count have a markedly increased HR of death.
Footnotes
Authors’ Note
Presented at Acute Cardiovascular Care Association (ACCA) Meeting 2019, Malaga, Spain. Morici, Cantoni, Cattaneo, and Savonitto made substantial contributions to conception and design Tavecchia, Caporale, Segreto, Viola, Meani, and Brunelli contributed to acquisition of data. Antolini, Bertuccio, Morici, and La Vecchia contributed to analysis and interpretation of data. Morici, Savonitto, Valgimigli, Sacco, Oreglia, Lombardi, and Oliva contributed to drafting the article or revising it critically for important intellectual content. All authors contributed to final approval of the version to be published. Clinical Trial Registration: URL: ![]() . Unique identifiers: NCT03583411.
. Unique identifiers: NCT03583411.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.