
Abstract
The relative superiority of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) on long-term clinical outcomes in patients with non-ST-segment elevation myocardial infarction (NSTEMI) with preserved left ventricular systolic function in the era of new generation drug-eluting stents is not well established. A total of 6436 patients with NSTEMI (ACEIs group: n = 3965 vs ARBs group: n = 2471) were enrolled. The major clinical end point was the occurrences of major adverse cardiac events (MACEs), defined as all-cause death, recurrent myocardial infarction (re-MI), and any repeat revascularization. After propensity score matching analysis, the cumulative incidences of MACEs (hazard ratio, 1.334; 95% confidence interval, 1.045-1.703; P = .021), any repeat revascularization, and target vessel revascularization (TVR) in the ARB group were significantly higher than that in the ACEI group. However, the cumulative incidences of all-cause death, cardiac death, re-MI, target lesion revascularization, and non-TVR were similar between the 2 groups. Hence, although the mortality and re-MI reduction benefits were similar between the 2 groups, the ACEIs group showed more prominent ability to decrease the occurrences of MACEs, any repeat revascularization, and TVR compared to the ARBs group in these patients during a 2-year follow-up period.
Introduction
Angiotensin-converting enzyme (ACE) catalyzes the breakdown of bradykinin into inactive peptides that play very important roles including vasodilation and stimulation of nitric oxide, prostacyclin, endothelium-derived hyperpolarizing factor, and tissue plasminogen activator production. 1 Angiotensin-converting enzyme inhibitors (ACEIs) enhance endothelial function and cardiovascular remodeling and reduce the progression of atherosclerosis. 2 Although angiotensin II type 1 (AT1) receptor blockers (ARBs) are indicated for patients who are intolerant to ACEIs, they can cause unwanted elevations in circulating angiotensin II level by stimulating the angiotensin II type 2 (AT2) receptor; this increased level of AT2 receptor is the main cause of cardiac myocyte hypertrophy, apoptosis, inflammation, plaque instability, and thrombus formation. 3 In the European guideline of non-ST-segment elevation myocardial infarction (NSTEMI), both ACEIs and ARBs are recommended in patients with systolic left ventricular dysfunction or heart failure (HF). 4 The American NSTEMI guideline also recommends that ACEIs be started and continued indefinitely in all patients with decreased left ventricular ejection fraction (LVEF <40%) unless contraindicated, while ARBs are recommended in patients with HF or myocardial infarction (MI) with LVEF <40% who are ACEIs intolerant. 5 Additionally, González-Cambeiro et al 6 demonstrated that the mortality rate was significantly lower in patients who were prescribed ACEIs/ARBs than in those for who these were not prescribed after propensity score matching (PSM) analysis (n = 813 in each group) with a hazard ratio (HR) of 0.77 (range: 0.63-0.94; absolute risk reduction, 3.8%; P = .03) as expected. However, there are limited data concerning the beneficial role of ACEIs and ARBs in patients with NSTEMI with a preserved LVEF. 7,8 Therefore, here we investigated the 2-year major clinical outcomes between ACEIs and ARBs therapy in patients with NSTEMI who underwent successful percutaneous coronary intervention (PCI) using new generation drug-eluting stents (DESs) to reflect current “real-world” practice.
Methods
Study Population
This nonrandomized, multicenter, observational, retrospective cohort study included data from the Korea Acute MI Registry (KAMIR), 9 a nationwide, prospective, multicenter registry in South Korea that was established in November 2005. The details of the registry can be found at the KAMIR website (http://www.kamir.or.kr). A total of 20 391 patients with NSTEMI in the KAMIR from November 2005 to June 2015 were evaluated. Patients with the following conditions were excluded: (1) lost to follow-up or did not participate (n = 1020, 5.0%), (2) incomplete laboratory results (n = 3901, 19.1%), (3) first-generation DESs deployment (n = 4466, 21.9%), (4) ACEIs or ARBs not prescribed (n = 3791, 18.6%), and, (5) concomitant use of ACEIs and ARBs (n = 164, 0.8%). After exclusion, a total of 7079 patients with NSTEMI who underwent successful new-generation DESs implantation and had been prescribed ACEIs or ARBs were considered for inclusion. Those patients with a decreased LVEF (<40%; n = 643, 9.1%) were also excluded. Finally, a total of 6436 patients with NSTEMI (ACEIs group, n = 3965 [61.6%] vs ARBs group, n = 2471 [38.4%]) with preserved left ventricular (LV) systolic function who underwent successful new-generation DESs implantation and who had been prescribed ACEIs or ARBs were enrolled (Figure 1).
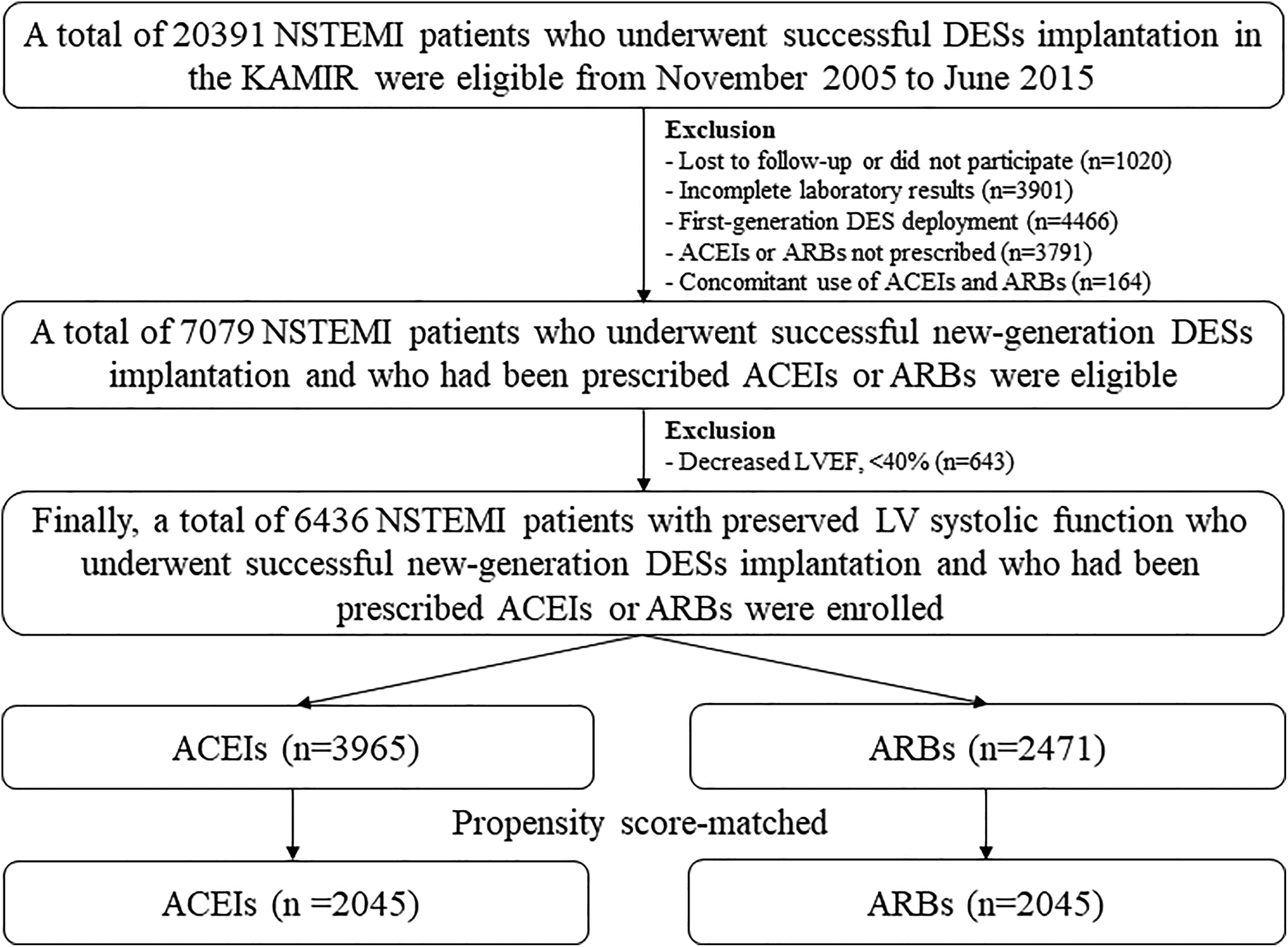
Flow chart. ACEIs indicates angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; DESs, drug-eluting stents; KAMIR, Korea Acute MI Registry; NSTEMI, non-ST-segment elevation myocardial infarction.
All data collection was carried out using a web-based case report form at each participating center. This study protocol was approved by the ethics committee at each participating center according to the ethical guidelines of the 1975 Declaration of Helsinki. All patients provided written informed consent prior to enrollment. In this study, all 6436 patients completed a 2-year clinical follow-up by face-to-face interviews, phone calls, or chart review.
Percutaneous Coronary Intervention Procedure and Medical Treatment
Diagnostic coronary angiography and PCI were performed through the femoral and the radial artery approach according to standard technique. 10 Loading doses of 200 to 300 mg aspirin and 300 to 600 mg clopidogrel (when available) or, alternatively, 180 mg ticagrelor or 60 mg prasugrel were administered to patients who were scheduled for PCI. The total duration of dual antiplatelet therapy (DAPT; combination of aspirin 100 mg/d with clopidogrel 75 mg/d or ticagrelor 90 mg twice a day or prasugrel 5-10 mg/d) was recommended for >12 months to patients who had undergone PCI. Triple antiplatelet therapy (100 mg cilostazol twice daily added to DAPT) was left to the discretion of the individual operators.
Study Definitions and Clinical Outcomes
Non ST-segment myocardial infarction was defined as prolonged (>20 minutes) acute chest pain but no persistent ST-segment elevation with increased cardiac biomarkers and a clinical context that was appropriate to the current diagnostic criteria. 4,5 The major clinical end point was the occurrence of major adverse cardiac events (MACEs) defined as all-cause death, recurrent myocardial infarction (re-MI), and any repeat coronary revascularization. All-cause death was classified as cardiac death (CD) or non-CD. Recurrent MI was defined as the presence of clinical symptoms, electrocardiographic changes, or abnormal imaging findings of MI combined with an increase in the creatine kinase myocardial band (CK-MB) fraction above the upper normal limits or an increase in troponin-T/troponin-I to greater than the 99th percentile of the upper normal limit during the follow-up period. 11 Target lesion revascularization (TLR) was defined as revascularization of the target lesion due to restenosis or reocclusion within the stent or 5 mm in and adjacent of the distal or proximal segment. Target vessel revascularization (TVR) was defined as a revascularization of the target vessel or any segment of the coronary artery containing the target lesion. Non-TVR was defined as a revascularization of any segment of the non-target coronary artery.
Statistical Analysis
For continuous variables, intergroup differences were evaluated with the unpaired t test, and data are expressed as mean ± standard deviation. For categorical variables, intergroup differences were analyzed using the χ2 test or, if not applicable, Fisher exact test, and the data are expressed as count and percentage. Various clinical outcomes were estimated with the Kaplan-Meier method, and intergroup differences were compared using the log-rank test. To adjust for potential confounders, a PSM analysis was performed using a logistic regression model. We tested all available variables listed in Table 1 that could be of potential relevance. The C-statistics for PSM was .707 in the current study. Patients in the ACEIs group were then one-to-one matched to those in the ARBs group according to propensity scores with the nearest available pair matching method. Patients were matched with a caliper width equal to .01. The procedure yielded 2045 matched pairs. Additionally, we performed a multivariable analysis to strengthen our results. The baseline confounding covariates were selected if they were significantly different (P < .001) between the 2 groups or had predictive values, as follows: age, men, LVEF, hypertension, diabetes mellitus (DM), previous history of MI, PCI, current smoker, cardiogenic shock, cardiopulmonary resuscitation (CPR) on admission, and serum level of CK-MB, N-terminal pro-brain natriuretic peptide (NT-ProBNP), creatinine, total cholesterol, high-density lipoprotein cholesterol, low-density cholesterol, clopidogrel, ticagrelor, prasugrel, β-blockers (BBs), calcium channel blockers, lipid-lowering agents, American College of Cardiology/American Heart Association (ACC/AHA) type B2 and C lesions, use of intravascular ultrasound (IVUS), DESs types (zotarolimus-eluting stents [ZES], biolimus-eluting stents [BES]), and PCI within 24 hours. For all analyses, a 2-sided P < .05 was considered significant. All statistical analyses were performed using SPSS software, version 20 (IBM, Armonk, New York).
Baseline Clinical, Laboratory, Angiographic, and Procedural Characteristics.a
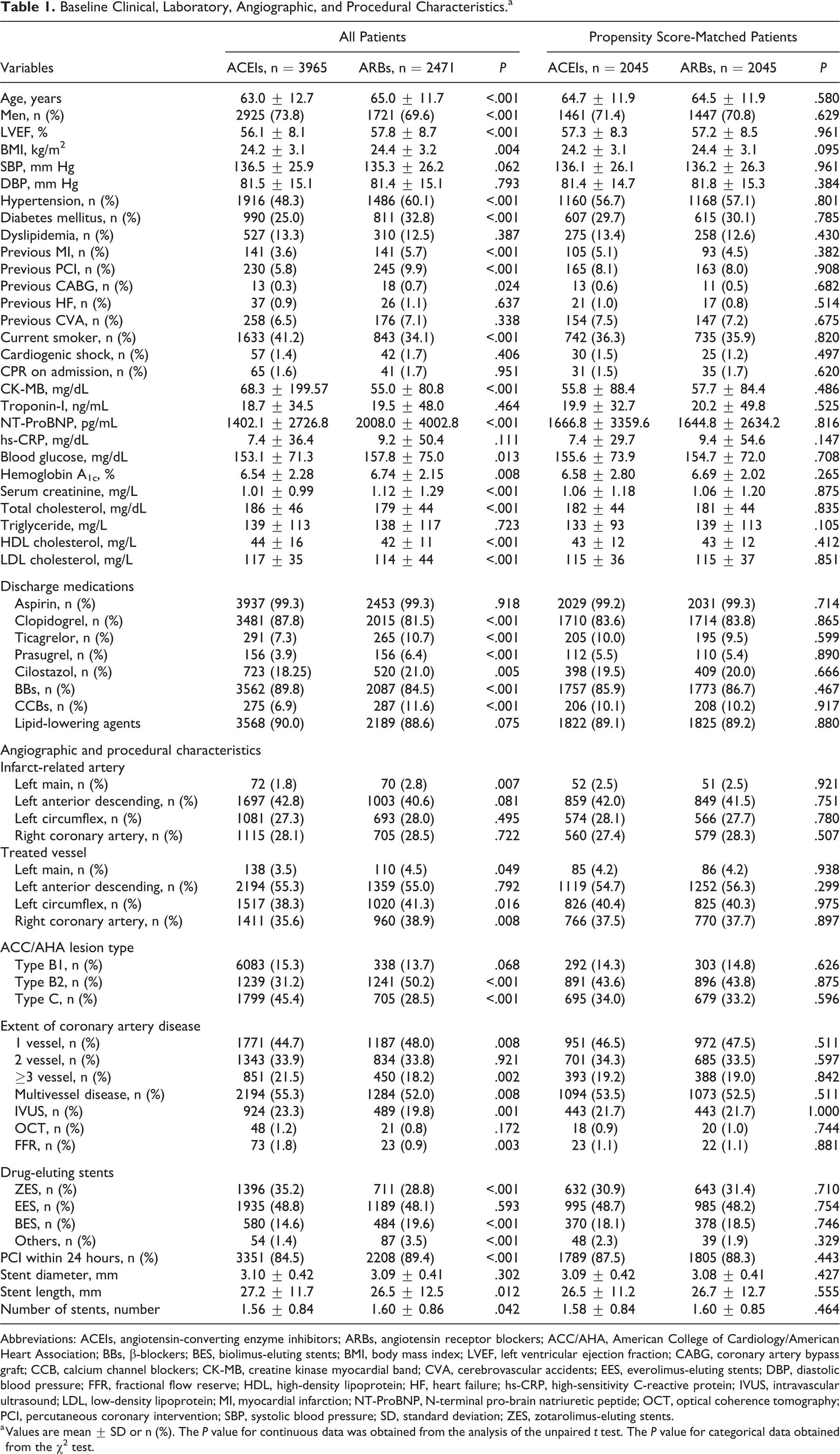
Abbreviations: ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; ACC/AHA, American College of Cardiology/American Heart Association; BBs, β-blockers; BES, biolimus-eluting stents; BMI, body mass index; LVEF, left ventricular ejection fraction; CABG, coronary artery bypass graft; CCB, calcium channel blockers; CK-MB, creatine kinase myocardial band; CVA, cerebrovascular accidents; EES, everolimus-eluting stents; DBP, diastolic blood pressure; FFR, fractional flow reserve; HDL, high-density lipoprotein; HF, heart failure; hs-CRP, high-sensitivity C-reactive protein; IVUS, intravascular ultrasound; LDL, low-density lipoprotein; MI, myocardial infarction; NT-ProBNP, N-terminal pro-brain natriuretic peptide; OCT, optical coherence tomography; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; SD, standard deviation; ZES, zotarolimus-eluting stents.
a Values are mean ± SD or n (%). The P value for continuous data was obtained from the analysis of the unpaired t test. The P value for categorical data obtained from the χ2 test.
Results
Baseline Characteristics
As shown in Table 1, the mean age of the ARBs group was older than that of the ACEIs group (65.0 ± 11.7 vs 63.0 ± 12.7 years; P < .001). The mean value of LVEF (57.8 ± 8.7 vs 56.1 ± 8.1%; P < .001) and body mass index were higher in the ARBs group. The number of patients with cardiogenic shock (1.7% vs 1.4%; P = .406) and CPR on admission (1.7% vs 1.6%; P = .951) were similar between the 2 groups. The number of PCI within 24 hours was higher in the ARBs group (89.4% vs 84.5%; P < .001). The number of patients with multivessel disease (MVD) and using IVUS, optical coherence tomography, and fractional flow reserve were higher in the ACEIs group than in the ARBs group. In contrast, the ARBs group showed higher numbers of patients with hypertension, DM, or a previous history of heart disease (MI, PCI, and coronary artery bypass graft); higher levels of blood NT-ProBNP, glucose, hemoglobin A1c, serum creatinine; higher prescription rates of ticagrelor, prasugrel, and cilostazol; and a higher incidence of left main coronary artery as the infarct-related artery (2.8% vs 1.8%; P = .007) and the treated vessel (4.5% vs 3.5%; P = .049), and ACC/AHA type B2/C lesions than the ACEIs group. The everolimus-eluting stent was deployed similarly in the 2 groups. However, ZES was more frequently deployed in the ACEs group and BES was more frequently deployed in the ARBs group. Despite this, the mean diameter of the deployed stents was similar between the 2 groups (3.10 ± 0.42 vs 3.09 ± 3.09 ± 0.41 mm; P = .302), the deployed stents were longer in the ACEIs group (27.2 ± 11.7 vs 26.5 ± 12.5 mm; P = .012), and the mean number of deployed stents was higher in the ARBs group (1.60 ± 0.86 vs 1.56 ± 0.84; P = .042). However, these intergroup differences in baseline characteristics were well balanced after PSM adjustment.
Clinical Outcomes
Table 2 and Figure 2 show the cumulative incidences of major clinical outcomes during the 2-year follow-up period. Before the adjustment, the cumulative incidences of MACEs, all-cause death, CD, re-MI, any repeat revascularization, and TVR were significantly higher in the ARBs group than in the ACEIs group. After PSM analysis, the cumulative incidence of MACEs (HR, 1.334; 95% confidence interval [CI], 1.045-1.703; P = .021), any repeat revascularization (HR, 1.848; 95% CI, 1.272-2.683; P = .001), and TVR (HR, 2.139; 95% CI, 1.340-3.415; P = .001) were significantly higher in the ARBs group than in the ACEIs. Additionally, the cumulative incidences of MACEs (adjusted HR [aHR], 1.297; 95% CI, 1.057-1.593; P = .013), any repeat revascularization (aHR, 1.480; 95% CI, 1.104-1.984; P = .009), and TVR (aHR, 1.830; 95% CI, 1.261-2.656; P = .001) of the ARBs group were significantly higher than the ACEIs group after multivariable analysis. However, the cumulative incidences of all-cause death, CD, re-MI, TLR, and non-TVR were similar between the 2 groups after PSM and multivariable analysis.
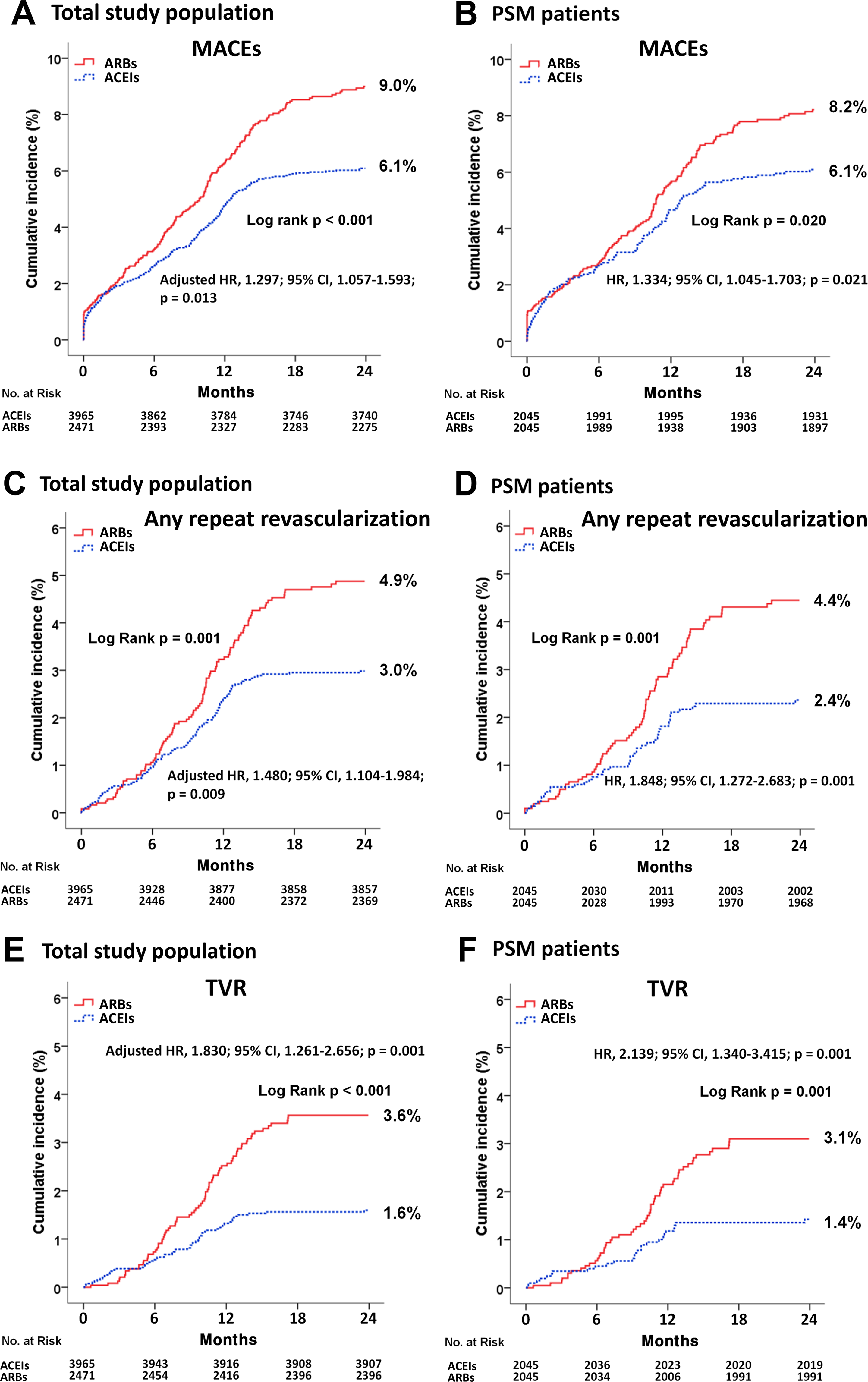
Kaplan-Meier curved analysis for major adverse cardiac events (MACEs; A and B), total repeat revascularization (C and D), and target vessel revascularization (TVR; E and F) in the total study population (A, C, and E) and propensity score matched (PSM) patients (B, D, and E) at 2 years. ACEIs indicates angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; MACEs, major adverse cardiac events; TVR, target vessel revascularization.
Clinical Outcomes by Kaplan-Meier Analysis and Cox Proportional Hazard Ratio Analysis Up to 2 Years.
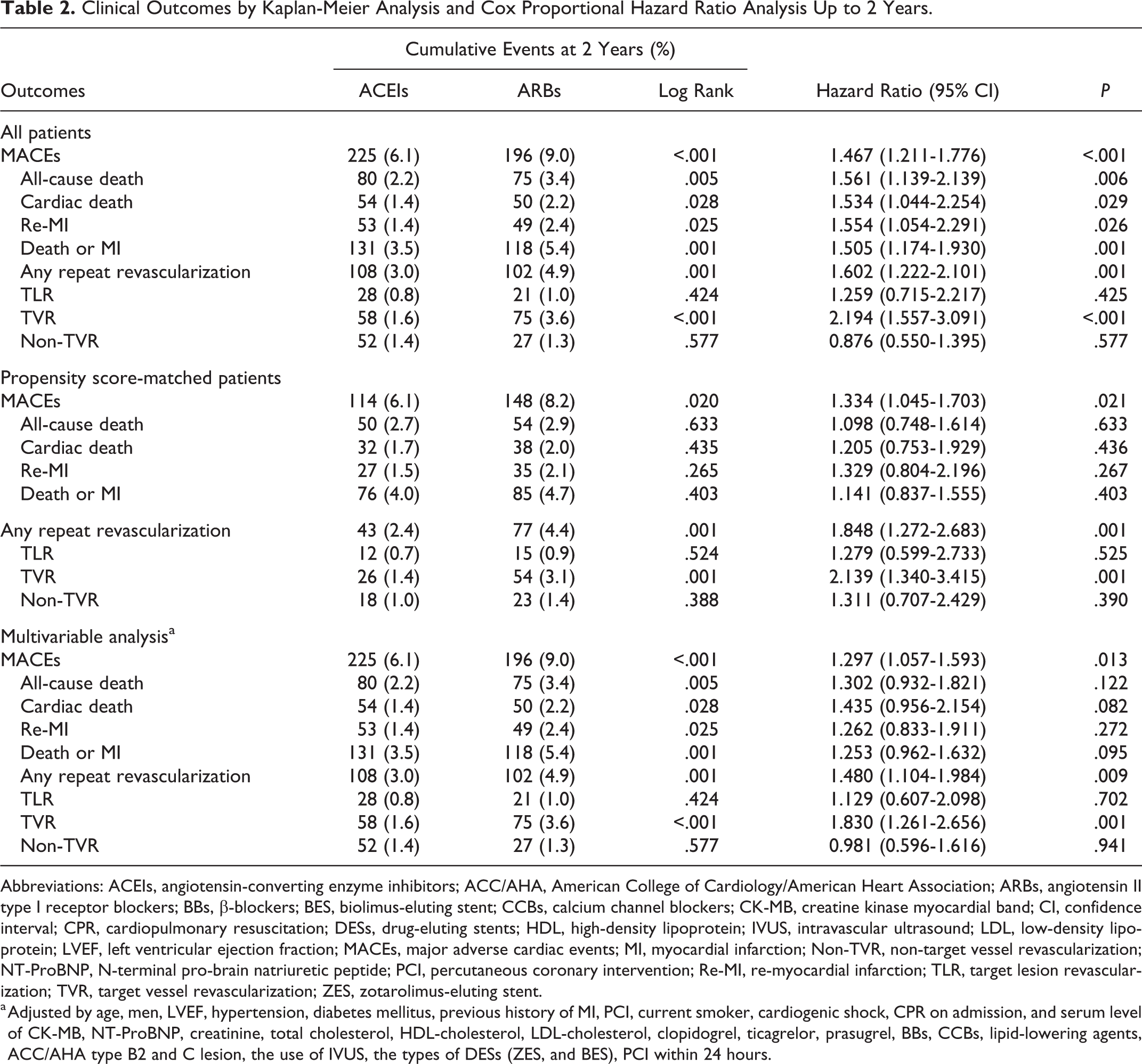
Abbreviations: ACEIs, angiotensin-converting enzyme inhibitors; ACC/AHA, American College of Cardiology/American Heart Association; ARBs, angiotensin II type I receptor blockers; BBs, β-blockers; BES, biolimus-eluting stent; CCBs, calcium channel blockers; CK-MB, creatine kinase myocardial band; CI, confidence interval; CPR, cardiopulmonary resuscitation; DESs, drug-eluting stents; HDL, high-density lipoprotein; IVUS, intravascular ultrasound; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; MACEs, major adverse cardiac events; MI, myocardial infarction; Non-TVR, non-target vessel revascularization; NT-ProBNP, N-terminal pro-brain natriuretic peptide; PCI, percutaneous coronary intervention; Re-MI, re-myocardial infarction; TLR, target lesion revascularization; TVR, target vessel revascularization; ZES, zotarolimus-eluting stent.
a Adjusted by age, men, LVEF, hypertension, diabetes mellitus, previous history of MI, PCI, current smoker, cardiogenic shock, CPR on admission, and serum level of CK-MB, NT-ProBNP, creatinine, total cholesterol, HDL-cholesterol, LDL-cholesterol, clopidogrel, ticagrelor, prasugrel, BBs, CCBs, lipid-lowering agents, ACC/AHA type B2 and C lesion, the use of IVUS, the types of DESs (ZES, and BES), PCI within 24 hours.
Table 3 shows the independent predictors for MACEs and TVR at 2 years in PSM patients. Old age (≥ 65 years, HR, 1.701; 95% CI, 1.322-2.188; P < .001), male (HR, 1.359; 95% CI, 1.055-1.751; P = .017), hypertension (HR, 1.288; 95% CI, 1.003-1.655; P = .048), DM (HR, 1.528; 95% CI, 1.192-1.958; P = .001), CPR on admission (HR, 2.288; 95% CI, 1.177-4.449; P = .015), ACC/AHA type B2/C lesions (HR, 1.444; 95% CI, 1.053-1.979; P = .023), MVD (HR, 1.576; 95% CI, 1.224-2.030; P < .001), and the use of IVUS (HR, 1.368; 95% CI, 1.037-1.803; P = .026) were meaningful independent predictors for MACEs. Diabetes mellitus (HR, 1.732; 95% CI, 1.112-2.699; P = .015), ACC/AHA type B2/C lesions (HR, 2.012; 95% CI, 1.065-3.802; P = .031), and MVD (HR, 1.594; 95% CI, 1.007-2.523; P = .047) were significant independent predictors for TVR. Figure 3A shows that in cases of old age and ZES, ACEIs may be preferred to ARBs to reduce MACEs after new-generation DESs implantation. In cases of ACC/AHA type B2/C lesions, ACEIs may be preferred to ARBs to reduce TVR (Figure 3B).
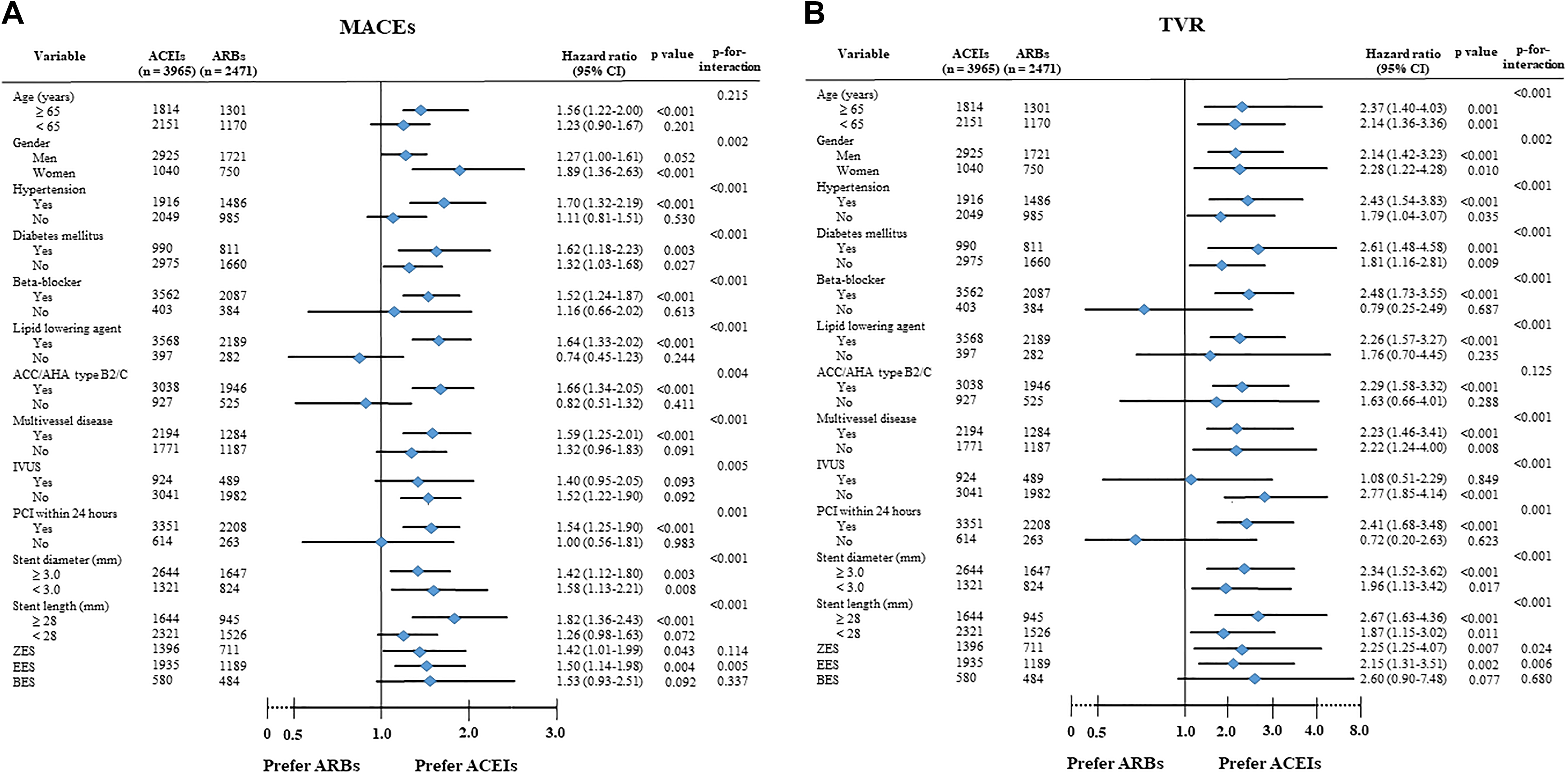
Subgroup analysis for major adverse cardiac events (MACEs; A) and target vessel revascularization (TVR; B). ACC/AHA indicates American College of Cardiology/American Heart Association; ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; BES, biolimus-eluting stents; CI, confidence interval; EES, everolimus-eluting stents; IVUS, intravascular ultrasound; MACEs, major adverse cardiac events; PCI, percutaneous coronary intervention; TVR, target vessel revascularization; ZES, zotarolimus-eluting stent.
Discussion
The main findings of this study are: (1) the cumulative incidences of all-cause death, CD, re-MI, TLR, and non-TVR were similar between the 2 groups; (2) the cumulative incidences of MACEs, any repeat revascularization, and TVR were significantly higher in the ARBs group than in the ACEIs group; and (3) DM, ACC/AHA type B2/C lesions, and MVD were common independent predictors for both MACEs and TVR in PSM patients.
Both ACEIs and ARBs are recommended in patients with NSTEMI with decreased LVEF (<40%). 4,5 However, the relative superiority on the long-term clinical outcomes between ACEIs and ARBs is still debatable. 2,12 The HOPE 13 and EUROPA 14 trial showed a significant benefit of ACEIs versus placebo regarding the risk of cardiovascular events. The PEACE, 15 CAMELOT, 16 and IMAGINE 17 studies did not show a benefit of ACEIs compared to placebo. The main cause of these results was related to lower event rates due to intensive treatment, including revascularization and lipid-lowering agents compared to the HOPE and EUROPA trials. 18 One head-to-head comparison trial of ACEIs versus ARBs in patients with versus without HF exhibited no difference in any outcomes, including all-cause death, CD, and MI (relative risk [RR] = 1.07, 95% CI, 0.94-1.22). 19 Another meta-analysis showed no significant difference in MI between ACEIs and ARBs. 18 In addition, the ONTARGET trial 20 showed no difference in MI between ARBs and ACEIs. In this study, the cumulative incidences of all-cause death (HR, 1.098; 95% CI, 0.748-1.614; P = .633), CD (HR, 1.205; 95% CI, 0.753-1.929; P = .436), and re-MI (HR, 1.329; 95% CI, 0.804-2.196; P = .267) were similar between the ACEIs and the ARBs groups after PSM analysis. Therefore, the results of the current study are consistent with the above published meta-analysis results. However, the study populations of these previous studies 18,19 were not confined to patients with NSTEMI. Regarding this characteristic of the included study populations, Yang et al 21 reported no significant difference in the rate of CD or MI between the ACEIs and ARBs groups (1.7% vs 1.8%; aHR, 0.94; 95% CI, 0.58-1.53; P = .79) in patients with STEMI with preserved LVEF. Hence, we cautiously suggest that the mortality- and MI-reducing capability of ACEIs and ARBs may be comparable between patients with NSTEMI and those with STEMI and a preserved LVEF.
Despite similar cumulative incidences of all-cause death, CD, and re-MI between the 2 groups, the cumulative incidences of MACEs, total revascularization, and TVR were significantly higher in the ARBs group. In the current study, the main cause of the intergroup difference in the cumulative incidence of MACEs is related to a higher cumulative incidence of TVR in the ARBs group. Up to date, acute coronary syndromes account for 20% to 70% of in-stent restenosis (ISR) cases, according to the patient population, lesion characteristics, and stent type. 22 After PCI, restenosis occurs mainly from excessive neointimal formation. 23,24 In an animal model, ACEIs blocked neointimal formation after vascular experimental balloon angioplasty 25 ; this effect could be related to the role of ACE in the formation of angiotensin II 26 and in the degradation of bradykinin. 27 Deftereos et al 28 demonstrated that the ACEI quinapril inhibited ISR by stimulating apoptosis after PCI in 86 patients who required stent implantation in the left anterior descending artery or a major branch. In the VALVACE trial, 29 ARBs were more effective than ACEIs in preventing ISR after PCI. However, the exact role of ARBs in ISR remains uncertain. 30 In our study, the cumulative incidence of TLR was similar between ACEIs and ARBs (HR, 1.297; 95% CI, 0.599-2.733; P = .525).
Byun et al 31 reported that the use of ACEIs was associated with a lower incidence of TVR (risk ratio = 0.47; 95% CI, 0.28-0.76; P = .47), total revascularization, and MACEs than the ARBs use in patients with NSTEMI and DM after PCI with DESs. Kim et al 32 also demonstrated that the combination of BBs with ACEIs was beneficial for reducing the cumulative incidence of TVR compared to BBs with ARBs in patients with NSTEMI who underwent PCI with DESs. In the total population of the current study, the numbers of patients with DM (32.8% vs 25.0%; P < .001), ACC/AHA type B2/C lesions (78.7% vs 76.6%; P < .001) occurred significantly more frequently in the ARBs group (Table 1), and these factors were linked with independent predictors of TVR in this study (Table 3). Therefore, we think that although we adopted PSM analysis or multivariable analysis for adjusting numerous confounding factors, these baseline characteristics may be related to the higher cumulative incidence of TVR in the ARBs versus ACEIs group.
Multivariate Cox-Proportional Regression Analysis for Independent Predictors of MACEs and TVR in PSM Patients.
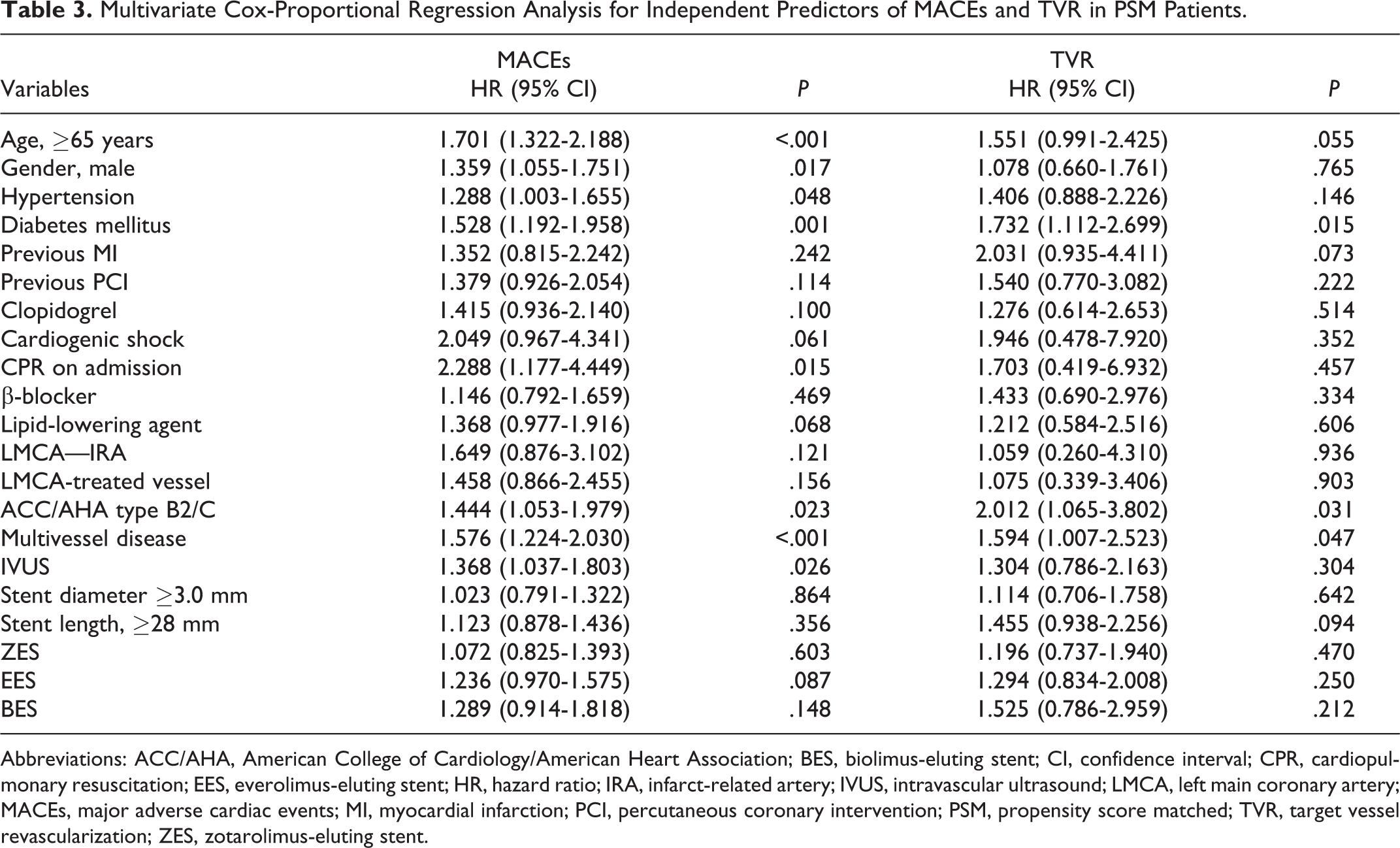
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; BES, biolimus-eluting stent; CI, confidence interval; CPR, cardiopulmonary resuscitation; EES, everolimus-eluting stent; HR, hazard ratio; IRA, infarct-related artery; IVUS, intravascular ultrasound; LMCA, left main coronary artery; MACEs, major adverse cardiac events; MI, myocardial infarction; PCI, percutaneous coronary intervention; PSM, propensity score matched; TVR, target vessel revascularization; ZES, zotarolimus-eluting stent.
In this study, we performed PSM and multivariable analysis to strengthen our results, and >50 high-volume university or community hospitals in South Korea participated in this study. Additionally, this registry reflects the results of “real-world” clinical practice, especially in the era of new-generation DESs. The current guidelines do not clearly define the usefulness of ACEIs and ARBs in patients having NSTEMI with a preserved LVEF. Therefore, we think that our study may provide meaningful message to interventional cardiologists during PCI with new-generation DESs regarding ACEIs or ARBs use in those patients. However, this result may be more precisely defined by other well-designed prospective randomized studies in the future.
Conclusions
In conclusion, in the current study, the mortality and re-MI reduction benefits were similar between the ACEIs and the ARBs groups. However, the ACEIs group showed a more prominent ability to reduce the occurrences of MACEs, any repeat revascularization, and TVR than the ARBs group in patients with NSTEMI and preserved LV systolic function after new-generation DESs implantation during a 2-year follow-up period.
Study Limitations
This study had several limitations. First, there may be some underreporting or missed data because this was a nonrandomized study. Second, this study was based on medications at discharge, and these registry data do not contain the full information regarding the continuation of drugs, potential crossover, drug dosing, and concomitant medication during the 2-year follow-up period. Likewise, adherence to therapy was not reported. All of these factors might have substantially affected the outcomes. Third, the selection of treatment strategies of ACEIs versus ARBs after PCI was left to physician discretion, which may be another important selection bias. Fourth, although we performed a PSM and multivariable analysis to strengthen our results, variables not included in this registry may have affected the study outcomes.
Footnotes
Authors’ Note
Yong Hoon Kim and Ae-Young Her contributed equally to this work.
Acknowledgments
The authors thank Korea Acute Myocardial infarction Registry (KAMIR) investigators: Myung Ho Jeong, MD, Youngkeun Ahn, MD, Sung Chul Chae, MD, Jong Hyun Kim, MD, Seung-Ho Hur, MD, Young Jo Kim, MD, In Whan Seong, MD, Donghoon Choi, MD, Jei Keon Chae, MD, Taek Jong Hong, MD, Jae Young Rhew, MD, Doo-Il Kim, MD, In-Ho Chae, MD, Junghan Yoon, MD, Bon-Kwon Koo, MD, Byung-Ok Kim, MD, Myoung Yong Lee, MD, Kee-Sik Kim, MD, Jin-Yong Hwang, MD, Myeong Chan Cho, MD, Seok Kyu Oh, MD, Nae-Hee Lee, MD, Kyoung Tae Jeong, MD, Seung-Jea Tahk, MD, Jang-Ho Bae, MD, Seung-Woon Rha, MD, Keum-Soo Park, MD, Chong Jin Kim, MD, Kyoo-Rok Han, MD, Tae Hoon Ahn, MD, Moo-Hyun Kim, MD, Ki Bae Seung, MD, Wook Sung Chung, MD, Ju-Young Yang, MD, Chong Yun Rhim, MD, Hyeon-Cheol Gwon, MD, Seong-Wook Park, MD, Young-Youp Koh, MD, Seung Jae Joo, MD, Soo-Joong Kim, MD, Dong Kyu Jin, MD, Jin Man Cho, MD, Sang-Wook Kim, MD, Jeong Kyung Kim, MD, Tae Ik Kim, MD, Deug Young Nah, MD, Si Hoon Park, MD, Sang Hyun Lee, MD, Seung Uk Lee, MD, Hang-Jae Chung, MD, Jang-Hyun Cho, MD, Seung Won Jin, MD, Myeong-Ki Hong, MD, Yangsoo Jang, MD, Jeong Gwan Cho, MD, Hyo-Soo Kim, MD, and Seung Jung Park, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by a fund (2016-ER6304-02) from the Research of Korea Centers for Disease Control and Prevention.