
Abstract
The risk of sudden cardiac death (SCD) is high in heart failure (HF) patients. Sudden arrhythmic death (SAD) is a frequent cause of exit in HF patients at the lower end of the HF spectrum, and implantable cardioverter–defibrillators have been recommended to prevent these life-threatening rhythm disturbances in select patients. However, less is known regarding the cause of SCD in patients at the upper end of the HF spectrum, despite the fact that the majority of out-of-hospital SCD victims have unknown or near-normal/normal left ventricular ejection fraction (LVEF). In this review, we report the epidemiology, summarize the mechanisms, discuss the diagnostic challenges, and propose a stepwise approach for the prevention of SAD in HF with near-normal/normal LVEF.
Keywords
Introduction
The risk of death in heart failure (HF) is high, and in approximately 20% to 50% of HF patients, the mode of demise is sudden cardiac death (SCD). 1 Because many (but not all) of these events in patients with HF at the lower end of the HF spectrum (HF with low left ventricular [LV] ejection fraction [LVEF]) are related to a sustained ventricular tachyarrhythmia (sudden arrhythmic death [SAD]), implantable cardioverter–defibrillators (ICDs) have been recommended to prevent these serious rhythm disturbances in select patients with New York Heart Association (NYHA) class II-III HF with LVEF <35%. 2 In contrast, in patients with HF at the upper end of the HF spectrum (HF with near-normal/normal LVEF), the causes of SCD, which is a surprisingly frequent mode of exit, have not been delineated. 3 As a result, these patients have been virtually excluded from ICD clinical trials, despite the fact that the majority of out-of-hospital SCD victims have unknown or relatively preserved LVEF (>30%). 4 The purpose of this study is to review the epidemiology, summarize the mechanisms, and discuss potential prevention strategies of SAD in HF with near-normal/normal LVEF.
Sudden Cardiac Death Is Not Always Arrhythmic: The Problem of Sudden Arrhythmic Death Definition
According to the World Health Organization (WHO), SCD is defined as sudden unexpected death occurring either within 1 hour of symptom onset (witnessed) or within 24 hours of having been observed alive and symptom-free (unwitnessed). 5 The primary utility of such a definition would be to identify SAD. Without a complete autopsy, however, noncardiac, cardiac nonarrhythmic, and arrhythmic conditions leading to SCD often cannot be correctly identified (Figure 1). 6 In the San Francisco Postmortem Systematic Investigation of Sudden Cardiac Death study in which autopsy was systematically used to identify SAD, only 55.8% of WHO-defined SCD were actually autopsy defined as SAD after excluding nonarrhythmic and noncardiac causes identified by postmortem investigation, including intracranial hemorrhage, occult overdose, acute HF, tamponade, or pulmonary embolism. 6
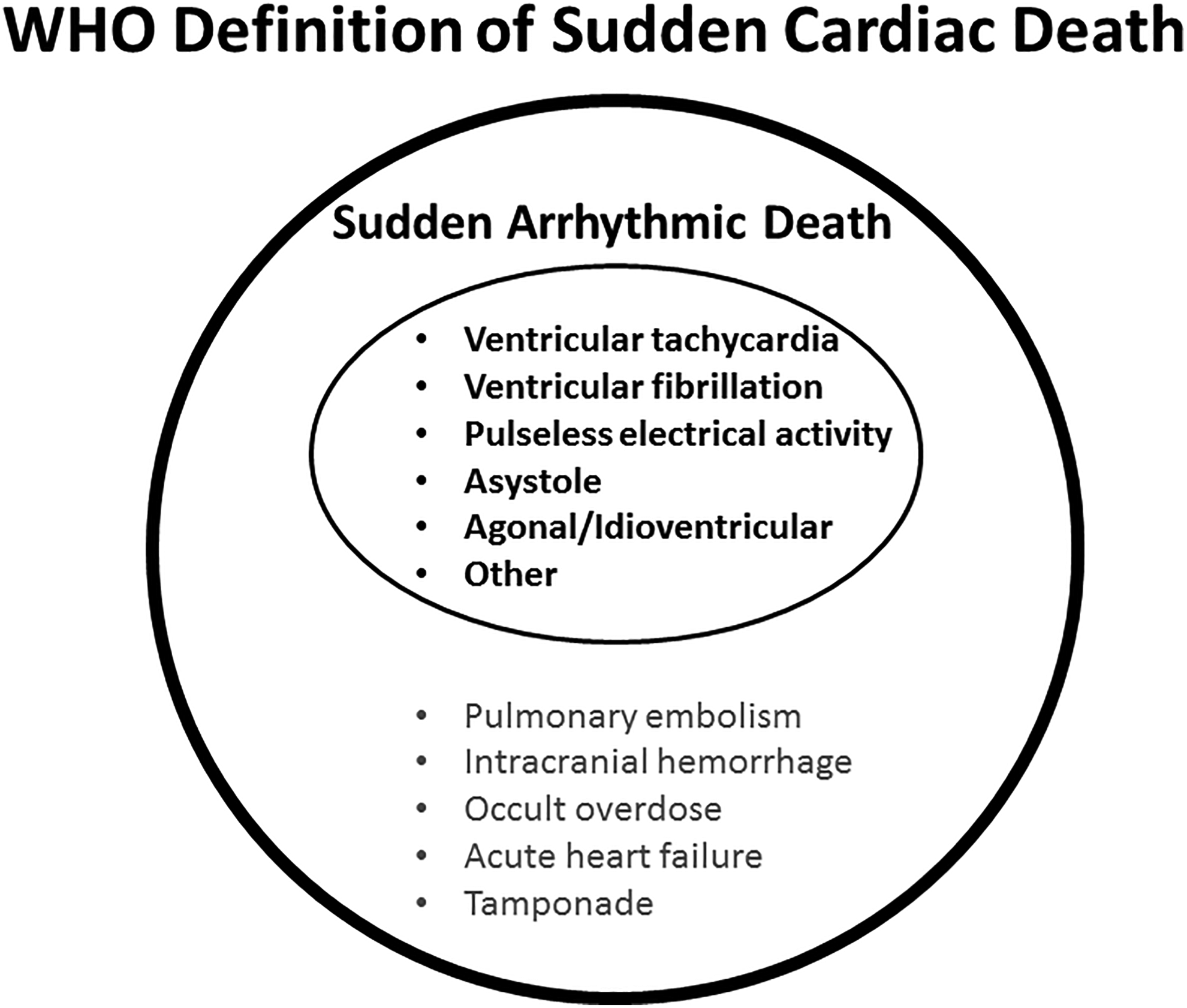
World Health Organization (WHO) definition of sudden cardiac death (SCD). Autopsy studies have demonstrated that, besides sudden arrhythmic death, it includes sudden cardiac nonarrhythmic and sudden noncardiac death. Based on data from Tseng et al. 6
As a result of the lack of a gold standard definition of SAD, several multidisciplinary working groups have sought to standardize the approach to SAD adjudication. 7 Proposed definitions generally integrate features of context (unexpected), timing (rapid witness collapse or occurring within 1 hour of onset of symptoms), inferred arrhythmic mechanism (abrupt collapse of circulation), and exclusion of noncardiovascular (non-CV) mechanism of death. 8 Moreover, models to identify premortem characteristics that can better specify autopsy-defined SAD among presumed SCD have been developed. 9
Sudden Cardiac Death Is Common in HF With Near-Normal/Normal LVEF
In the Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity-Preserved (CHARM-Preserved) trial (patients with HF having LVEF >40%), deaths were considered CV unless a specific non-CV cause was identified and were further categorized as sudden or as attributed to myocardial infarction (MI), HF, stroke, complications of a procedure, or another CV cause. Sudden cardiac death was defined as the unexpected death of a stable patient. 10 In this study, 134 SCD events occurred representing 28% of total deaths and 39% of CV deaths over a 37-month follow-up.
In the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE) trial (patients with HF having LVEF ≥45%), sudden death was defined as an unexpected death in a previously clinically stable patient. 11 Patients in this category had recent human contact before the event. This category included patients who after attempted resuscitation became comatose and then died. Patients who died and had been out of contact for prolonged (generally 1 week) or unknown periods of time were classified as unknown. When sufficient information was available, sudden death was subcategorized as with or without preceding CV symptoms. In the absence of such information, the sudden death event was subcategorized as unknown. In this study, 231 SCD events occurred representing 26% of total mortality and 43% of CV mortality over 50-month follow-up. 11
In the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial (patients with HF having LVEF ≥45%), sudden death was defined as a death event that occurred unexpectedly in an otherwise stable patient, and it was further subclassified as either witnessed (if death was observed) or last seen ≥1 and <24 hours and presumed sudden death (if last seen ≥24 hours with the clinical context suggestive of sudden death). In this study, 128 SCD events occurred representing 24% of total mortality and 38% of CV mortality over a 40-month follow-up. 12 In the TOPCAT Americas study, 72 sudden death events occurred, representing 19% of total mortality and 32% of CV mortality during a median follow-up of 3 years. 13
The higher estimates of SCD in CHARM-Preserved and I-PRESERVE than in TOPCAT may be due to the diverse definitions of SCD. Moreover, TOPCAT Americas enrolled higher proportions of patients ≥75 years (41%) than CHARM-Preserved (27%) and I-PRESERVE (34%), which might have contributed to higher global risk, including nonsudden modes of death.
A systematic review including 8 randomized controlled trials (RCTs) and 24 epidemiological studies collected information on mode of death in HF and near-normal/normal LVEF over a 30-year period (1985-2015) and highlighted 4 major points. 14 The majority of patients died of CV causes with significant variability between RCTs and epidemiological studies, and specific CV deaths (ie, SCD and death due to worsening HF) are infrequently adjudicated and poorly defined. Also, SCD, as currently reported, accounted for up to 30% to 40% of CV-related deaths, and non-CV modes of death accounted for up to 20% to 30% of deaths in HF and near-normal/normal LVEF studies. 14
Rates of SCD observed in epidemiological studies on HF with near-normal/normal LVEF were lower than that reported in large contemporary RCTs. This may be related to the higher rates of deaths related to noncardiac comorbidities in epidemiological studies and the more complete capture and ascertainment of events as well as the more liberal definitions applied in RCTs.
Sudden Cardiac Death in HF With Near-Normal/Normal LVEF
Experimental and clinical evidence suggest that a considerable proportion of SCDs in HF with near-normal/normal LVEF may be SAD.
Experimental Studies
Dahl salt-sensitive rats were fed a high-salt diet (8% NaCl) from 7 weeks of age to induce HF with near-normal LVEF (n = 38). Rats fed a normal salt diet (0.3% NaCl) served as controls (n = 13). 15 After 7 weeks of a high-salt diet, 31 of 38 rats showed diastolic dysfunction and near-normal LVEF along with signs of HF. Susceptibility to ventricular arrhythmias was markedly increased in rats with HF and near-normal LVEF. Underlying abnormalities included QT prolongation, delayed repolarization from downregulation of potassium currents, and multiple reentry circuits during ventricular arrhythmias.
In another study, Dahl salt-sensitive rats (7 weeks of age) were fed a high-salt diet to induce HF with near-normal LVEF (n = 13) or a normal salt diet (controls, n = 9). 16 Telemetric electrocardiographic (ECG) recordings were analyzed for QT interval duration, burden of premature ventricular contractions, spontaneous ventricular arrhythmias, and heart rate variability. Sudden death was common and generally associated with ventricular arrhythmias.
Clinical Studies
The proportion of SAD among SCD is virtually unknown in HF with near-normal/normal LVEF. There are signals, however, suggestive that SAD may be associated both with the risk factors (obesity, hypertension, coronary artery disease [CAD]) of HF and near-normal/normal LVEF itself.
Sudden arrhythmic death in risk factors for HF and near-normal/normal LVEF
Obesity increases the risk of SCD. In a recent meta-analysis, there was a 16% increase in the relative risk per 5-unit increase in body mass index (BMI) and an 82% increase in relative risk per 0.1-unit increase in waist to hip ratio. There was also evidence of a nonlinear J-shaped association between BMI and SCD, with a slight increase in risk in the underweight categories and a 14%, 60%, and 2- to 3-fold increase in risk in the overweight, obese, and severely obese categories. 17 Ventricular arrhythmias, long QT syndrome, frequent premature ventricular contractions, and left ventricular hypertrophy (LVH) with diastolic dysfunction are commonly observed in obese humans. 18 Moreover, several mechanisms link adipocytes to increased arrhythmogenicity. 19
Hypertension is associated with increased arrhythmogenesis, especially in the presence of LVH. A study followed for an average of 10.3 years a cohort of 3242 initially untreated patients with hypertension without evidence of coronary or cerebrovascular heart disease at entry. 20 During follow-up, SCD occurred in 33 patients at a rate of 0.10 per 100 patient-years (95% confidence interval [CI], 0.07-0.14). The rate of SCD was 0.07 and 0.30 per 100 patient-years, respectively, in the cohort of patients without and with ECG LVH (P < .01). LVH almost tripled the risk of SCD (adjusted hazard ratio, 2.99; 95% CI, 1.47-6.09; P = .002) after adjustment for age, sex, diabetes mellitus, and 24-hour ambulatory pulse pressure. For each 10 mm Hg increase in 24-hour ambulatory pulse pressure, the risk of SCD increased by 35%. The LVH may increase the risk of arrhythmias through electrophysiological disturbances, including QT-interval prolongation and dispersion, and may be associated with myocardial fibrosis and activation of sympathetic nervous system and renin–angiotensin system. 21 –23 LVH may also predispose to atrial fibrillation, which has been associated with a higher risk of SAD. 24
Coronary artery disease is the most common cause of SCD. 25 Acute ischemia is often responsible for SCD in patients without a prior history of CAD, in whom an SAD due to a ventricular arrhythmia may be the first manifestation of coronary atherosclerosis. Although in this setting ventricular fibrillation is the most common terminal rhythm, it is at times preceded by polymorphic ventricular tachycardia. 26 On the other hand, what is frequently termed substrate-related or nonischemic SAD occurs more frequently in patients with low LVEF, in whom acute ischemia is usually less important for the development of a lethal ventricular arrhythmia than is the presence of a myocardial scar from a previous infarction. Nevertheless, autopsy results from 171 HF patients with low LVEF enrolled in the Assessment of Treatment with Lisinopril and Survival (ATLAS) study who died suddenly suggested that acute coronary findings (ie, coronary thrombus, ruptured plaque, or MI) was a frequent cause of sudden death that usually eluded the clinical diagnosis in HF patients with CAD. 27
Sudden arrhythmic death in established HF with near-normal/normal LVEF
There are limited data, predominantly in patients with CAD. The PRE-DETERMINE Biologic Markers and Sudden Cardiac Death Study was a prospective observational multicenter cohort study of 5761 North American patients with CAD and LVEF >30% followed up for a median of 3.9 years. 28 The cumulative incidence of SAD and non-SAD was 2.1% and 7.7%, respectively. Sudden and/or arrhythmic death was the most common mode of CV death accounting for 114 (56%) of 202 cardiac deaths, although noncardiac death was the primary mode of death in this population. The 4-year cumulative incidence of SAD was lowest in those with an LVEF >60% (1.0%) and highest among those with LVEF of 30% to 40% (4.9%) and class III/IV HF (5.1%); however, the cumulative incidence of non-SAD was similarly elevated in these latter high-risk subgroups. Patients with a moderately reduced LVEF (40%-49%) were more likely to die of SAD, whereas those with class II HF and advancing age were more likely to die of non-SAD.
The Post Myocardial Infarction Risk Stratification for Sudden Cardiac Death in Patients With Preserved Ejection Fraction (PRESERVE EF) enrolled 575 consecutive patients with MI, at least 40 days after the event (90 days after surgery if they underwent coronary artery bypass grafting), with LVEF ≥40% (also assessed after 40 or 90 days, respectively from the index event), either revascularized or not—but without any evidence of active ischemia on optimal tolerated medical therapy. 29 After a mean follow-up of 32 months, no SCDs were observed, while 9 implanted ICDs (1.57% of total screened population) were appropriately activated.
Presumed Mechanisms of SAD in HF With Near-Normal/Normal LVEF
Worsening congestion, myocardial overstretch, adrenergic overactivity, myocardial denervation, and ischemia may all increase the risk of fatal ventricular arrhythmias. 30 –32 LVH, one of the structural hallmarks of HF with near-normal/normal LVEF, is associated with excess fibrosis, collagen deposition, and increased risk of SAD. 33 Areas of fibrosis alter regional conduction patterns and serve as islands of reentry, which is the commonest underlying mechanism of sustained ventricular tachyarrhythmias. The risk of SAD in patients with ECG evidence of LVH and intraventricular conduction delay has been reported to be comparable with that of patients with established symptomatic CAD. 34 In the Oregon Sudden Unexpected Death Study, SCD cases with archived echocardiographic data available were prospectively identified during 2002 to 2015 and compared to geographical controls. 35 Analysis was restricted to patients with LVEF >35%. Cases with SCD (n = 307) and controls (n = 280) did not differ in age, sex, or LVEF, but increased LV mass was more common in cases. Twenty-nine percent of cases with SCD presented with normal LV geometry, 35% had concentric remodeling, 25% concentric hypertrophy, and 11% eccentric hypertrophy. In multivariate model, concentric remodeling (odds ratio [OR]: 1.76; 95% CI: 1.18-2.63; P = .005), concentric hypertrophy (OR: 3.20; 95% CI: 1.90-5.39; P < .001), and eccentric hypertrophy (OR: 2.47; 95% CI: 1.30-4.66; P = .006) were associated with increased risk of SCD.
Mineralocorticoid receptor activation has been shown to promote arrhythmia, both by increasing tissue remodeling and fibrosis and through electrophysiological alterations that lead to the formation of the arrhythmogenic substrate of reentry of triggered activity. 36 In TOPCAT Americas, SCD was numerically lower but not statistically reduced in those randomized to spironolactone. 13
On the molecular level, calcium overload in the cardiomyocytes in HF with near-normal/normal LVEF may result in arrhythmogenic regional repolarization heterogeneity. 37 Downregulation of enzymes involved in calcium reuptake into the sarcoplasmic reticulum (governed by the SERCA2a gene) may be responsible for cytoplasmic calcium overload, leading to prolongation of action potential, a known trigger for reentry. 38 Moreover, T-tubule disorganization and the resulting disruption of intracellular calcium cycling have been implicated in the development of cardiac fibrosis and dysfunction in HF with near-normal/normal LVEF. 39 Altered calcium handling and increased oxidative stress in the mitochondria may be central to the development of HF and SAD. 40,41 Electrolyte deficits and proarrhythmic drugs may also play a role in SAD. 42 Finally, an important determinant of SAD in HF could be an underlying genetic predisposition to electrical instability. 43
Identifying Patients With HF and Near-Normal/Normal LVEF at Higher Risk of SAD
The public health challenge of preventing SCD and especially SAD which may be countered by ICD implantation is significant. A reasonable approach would be first to identify patients at increased risk of SCD and subsequently the subgroup at increased risk for SAD.
Prediction of SCD
In the I-PRESERVE trial, a multivariable model including age, gender, history of diabetes and MI, LBBB on ECG, and the natural logarithm of N-terminal-pro-B-type natriuretic peptide (NT-proBNP) identified a subgroup of 837 (24%) patients with ≥10% cumulative incidence of SCD over 5 years. 44 This risk is equivalent to that of patients with HF and low LVEF enrolled in the Sudden Cardiac Death in Heart Failure (SCD-Heft). 45 In addition, from another analysis of the I-PRESERVE trial, it was concluded that patients with CAD are at higher risk of all-cause mortality and SCD (almost double) when compared with those without CAD. 46
In TOPCAT Americas after accounting for competing risks of non-SCD, male sex and insulin-treated diabetes mellitus were independently predictive of SCD (C-statistic = 0.65). 13 Sex and diabetes mellitus status remained independent predictors in sensitivity analyses, excluding patients with ICDs and when predicting SCD alone. 13
Aro et al, utilizing the community-based Oregon Sudden Unexpected Death Study (population ∼1 million), analyzed data from 522 cases with SCD with available 12-lead ECG and compared those with 736 geographical controls to investigate the incremental value of multiple ECG parameters in prediction of SCD. 47 These researchers developed the ECG risk score (heart rate, LV hypertrophy, QRS transition zone, QRS-T angle, QTc, and Tpeak-to-Tend interval), which was externally validated in the Atherosclerosis Risk in Communities Study. The ECG risk score proved to be highly predictive of SCD among patients with normal or near-normal LVEF. 47
Prediction of SAD
Several studies have shown microvolt T-wave alternans (MTWA) to be an accurate predictor of ventricular tachyarrhythmic events in patients with near-normal/normal LV function. From the largest trial of MTWA 48 in 1041 post-MI patients with LVEF >40%, a multivariate analysis showed that those with a positive MTWA result were almost 20 times more likely to have an arrhythmic event (ArE) than those with a negative test result (P < .0001). Likewise, in the Risk Estimation Following Infraction Non-invasive Evaluation (REFINE) study, 49 MTWA was a strong independent predictor factor for SCD in post-MI patients with an average LVEF of 49%.
In the previously mentioned PRESERVE EF, 29 a combined noninvasive/invasive risk stratification approach in post-MI, ischemia-free patients, with LVEF ≥40%, was introduced. Patients with at least 1 positive ECG noninvasive risk factor (NIRF): premature ventricular complexes, nonsustained ventricular tachycardia, late potentials, prolonged QTc, increased T-wave alternans, reduced heart rate variability, and abnormal deceleration capacity with abnormal turbulence, were referred for programmed ventricular stimulation (PVS), with ICDs offered to those with inducible ventricular arrhythmias (monomorphic ventricular tachycardia or ventricular flutter or polymorphic ventricular tachycardia). The primary end point was the occurrence of a major ArE, namely, sustained ventricular tachycardia/fibrillation, appropriate ICD activation, or SCD. Of 575 consecutive patients, 204 (35.5%) had at least 1 positive NIRF. Forty-one (27%) of 152 patients undergoing PVS exhibited inducible ventricular tachycardia. Thirty-seven (90.2%) of them received an ICD. Mean follow-up was 32 months and no SCDs were observed, while 9 ICDs were appropriately activated. No patient without NIRFs or with NIRFs but negative PVS met the primary end point. The algorithm yielded the following: sensitivity 100%, specificity 93.8%, positive predictive value 22%, and negative predictive value 100%. There is limited information regarding the usefulness of electrophysiological study and PVS for risk stratification of SCD in HF patients with near-normal/normal LVEF. 50 However, it proved useful in the PRESERVE EF study. 29 One reasonable approach for preventing SAD in HF with near-normal/normal LVEF based on the above is presented in Figure 2. 13,29,44
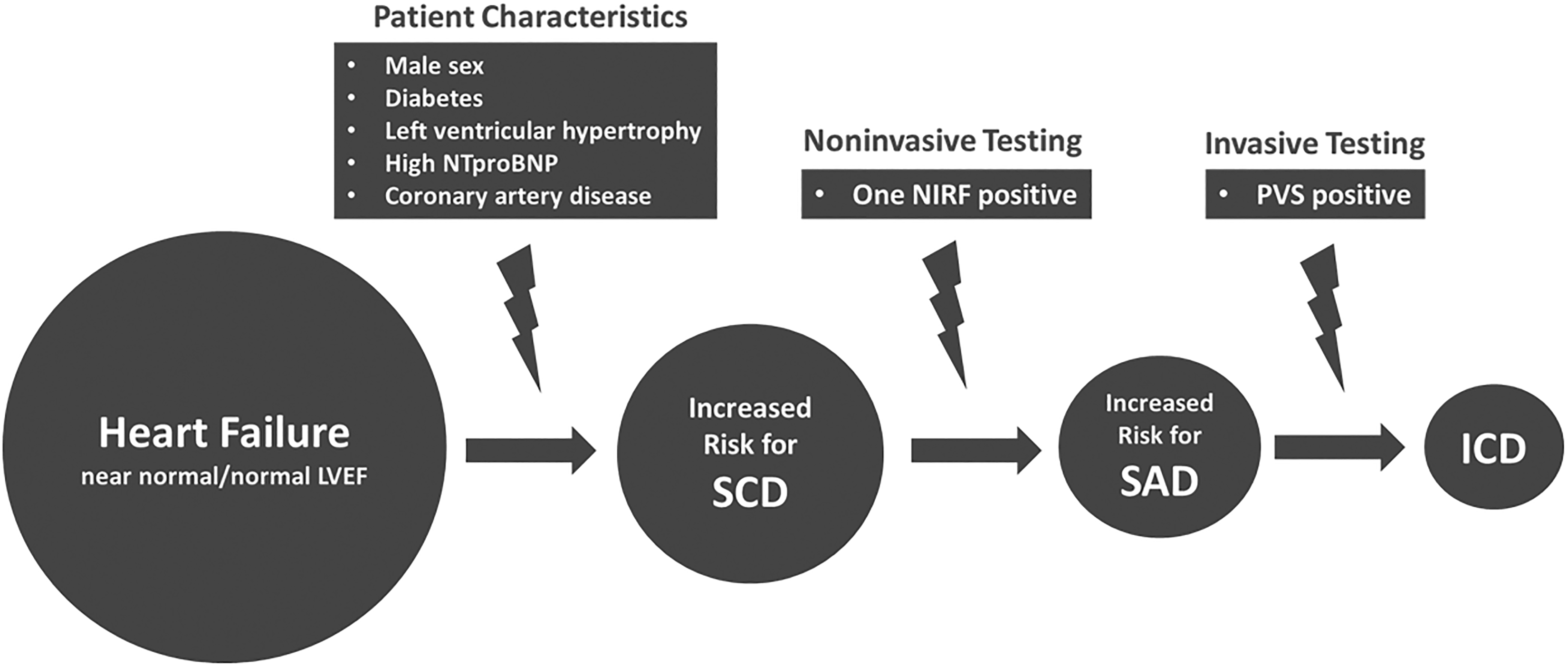
Proposed stepwise approach for the prevention of sudden arrhythmic death (SAD) in heart failure with near-normal/normal left ventricular ejection fraction (LVEF). Patients with characteristics indicative of high risk for sudden cardiac death (SCD) should undergo noninvasive testing. Those with electrocardiographic noninvasive risk factor (NIRF) positive (premature ventricular complexes, nonsustained ventricular tachycardia, late potentials, prolonged QTc, increased T-wave alternans, reduced heart rate variability, abnormal deceleration capacity, or abnormal turbulence) should be referred for programmed ventricular stimulation (PVS). In patients with positive PVS, an implantable cardioverter defibrillator (ICD) should be offered. Based on data from Adabag et al. 44
Efficacy of ICDs in Patients With Recovered LVEF
A recent retrospective analysis from SCD-HeFT trial showed that patients with baseline LVEF <35% who improved their LVEF to >35% after trial enrollment benefited from ICD implantation for primary prevention similar to those whose LVEF remained below 35% (adjusted hazard ratio for the effect of ICD on mortality compared to placebo was 0.64; 95% CI, 0.48-0.85, in patients with a repeated LVEF of ≤35% and 0.62; 95% CI, 0.29-1.30, in those with a repeated LVEF >35%). 51 In a prospective cohort of patients (n = 538) undergoing primary prevention ICD implantation, changes in LVEF during a mean follow-up of 4.9 years were inversely related to all-cause mortality and appropriate ICD shock (ie, a shock for ventricular tachyarrhythmia). 52 In particular, patients with an improved LVEF demonstrated 67% and 71% lower risk of death and appropriate shock, respectively, compared to those with an unchanged LVEF. During follow-up, a quarter of patients exhibited improved LVEF to >35%. Interestingly, the risk of appropriate shock was decreased but not eliminated in these patients.
A retrospective chart review revealed that approximately 25% of patients who receive ICDs for primary prevention may no longer meet current guideline indications for ICD use at the time of generator replacement. 53 Moreover, it has been reported that the decision to replace the ICD generator should take into consideration both cardiac parameters, such as LVEF and prior history of ventricular arrhythmia and noncardiac comorbidities (ie, diabetes mellitus, chronic lung disease, peripheral artery disease, anemia, and chronic kidney disease), which may impact the duration as well as the quality of life. 54
Future Perspectives
The prevention of SCD, and especially SAD, in HF with near-normal/normal LVEF is a high goal, whose accomplishment requires accurate prediction. Current prediction models, however, are far from accurate and need improvement.
Artificial intelligence (AI), which broadly refers to analytical algorithms that iteratively learn from data, allowing computers to find hidden insights without being explicitly programmed where to look, might be extremely helpful. 55 Indeed, the initial results are encouraging. In a recent study, a multicenter database of HF (n = 529), in which 2-year outcomes were known, was used as the training database of AI. 56 The sudden ArE group consisted of arrhythmic death, SCD, and appropriate therapy by ICD. The model input was 8 variables of age, sex, NYHA functional class, LVEF, ischemic etiology, heart to mediastinum ratio, BNP, or NT-ProBNP, and estimated glomerular filtration rate. The area under the receiver–operating characteristic curve was 0.87 for predicting all events, and 0.91 and 0.74 for HF death and ArE, respectively. The role of magnetic resonance imaging (MRI) in the risk stratification for SCD is promising. 57,58 Several variables based on this technique (late gadolinium enhancement, T1 mapping, T2* relaxometry, deformation imaging) have been associated with ventricular arrhythmias and SCD risk. However, prospective, randomized trials and standardization of MRI techniques are needed before its implementation in HF with near-normal/normal LVEF. 58 In this regard, however, it is encouraging that MRI has already proved useful in hypertrophic cardiomyopathy (HCM), 57 a nonhypertensive form of HF with near-normal/normal LVEF. 59 Lastly, genetic testing in certain cases may contribute to a better risk stratification for SCD by identifying mutations (ie, MYBPC3) associated with lethal arrhythmias. 60
Conclusions
Improvements in managing SAD in HF with near-normal/normal LVEF will require a concerted effort across scientific disciplines, clinician groups, and industry to combine technological innovation and rigorous scientific studies. Advances can be considered in the categories of understanding and better managing the underlying pathology and developing accurate SAD prediction algorithms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.