
Abstract
Angiotensin-converting enzyme inhibitor (ACEi) and angiotensin II receptor blockers (ARB) showed comparable survival results in patients with heart failure (HF) and reduced left ventricular ejection fraction (LVEF). However, there is lack of evidence of the comparative effectiveness in preserved LVEF patients after an acute coronary syndrome (ACS). The aim of this study was to evaluate whether the selection between ACEi and ARB in preserved LVEF after an ACS confers a prognostic benefit, based on real life results. We analyzed a cohort of 3006 contemporary patients with LVEF ≥40% after an ACS. A propensity score matching and Cox regression analysis were performed to assess the association between treatment and events (death, acute myocardial infarction [AMI], HF, and combined event) for a mean follow-up of 3.6 ± 2.1 years. We found no significant differences between ACEi/ARB for all-cause mortality (hazard ratio [HR] for ARB: 0.95, 95% CI: 0.70-1.29), AMI (HR for ARB: 1.34, 95% CI: 0.95-1.89), HF (HR for ARB: 1.11, 95% CI: 0.85-1.45), or combined end point (death, AMI and HF: HR for ARB: 1.14, 95% CI: 0.92-1.40). In conclusion, there are no prognostic differences between the use of ACEi and ARB in patients with LVEF ≥40% after ACS. Further prospective studies are needed to confirm our results.
Keywords
Introduction
The inhibition of the renin–angiotensin–aldosterone system (RAAS) after an acute coronary syndrome (ACS) has been associated with a clear benefit in terms of mortality. 1 Furthermore, the prognostic impact of neurohormonal blockade varies depending on the left ventricular ejection fraction (LVEF).2–5 However, this evidence comes from older studies in which percutaneous coronary intervention (PCI) was not the standard of care.
Recent studies, based on contemporaneous data (with high rates of PCI and optimal medical treatment), have reported the results of a real-world population analysis. It was observed that while the benefit is clear for patients with depressed LVEF, there are only some subgroups of patients with preserved LVEF that would benefit from the use of angiotensin-converting enzyme inhibitor (ACEi) and angiotensin II receptor blockers (ARB; essentially, those with ST-elevation myocardial infarction [STEMI]).6,7
International clinical practice guidelines for the management of ACS establish ACEi as a drug of first choice over ARB for treating all ACS patients in the absence of contraindications.8,9 Those guidelines propose the use of ARB as an alternative for patients who are intolerant to ACEi without setting any efficacy criteria between both therapies (ACEi vs ARB). However, there is no comparison between both drugs to support this recommendation. In our study, we aim to analyze the long-term prognostic impact of ACEi versus ARB in ACS patients with preserved LVEF.
Material and Methods
The data analyzed in this study were obtained from the CardioCHUVI registry (ClinicalTrials.gov Identifier: NCT03664388). This is a retrospective clinical registry that included all consecutive patients admitted for ACS to the University Hospital of Vigo (Spain) between 2010 and 2016. For the purpose of the present study, we excluded patients who had died during hospitalization, those with LVEF ≤ 40% and also those who had not been treated with ACEi/ARB at hospital discharge. The final study cohort included 3006 patients (Figure 1). We performed the study in accordance with the principles of the Declaration of Helsinki, and the local ethics committee provided approval before the start of the study.
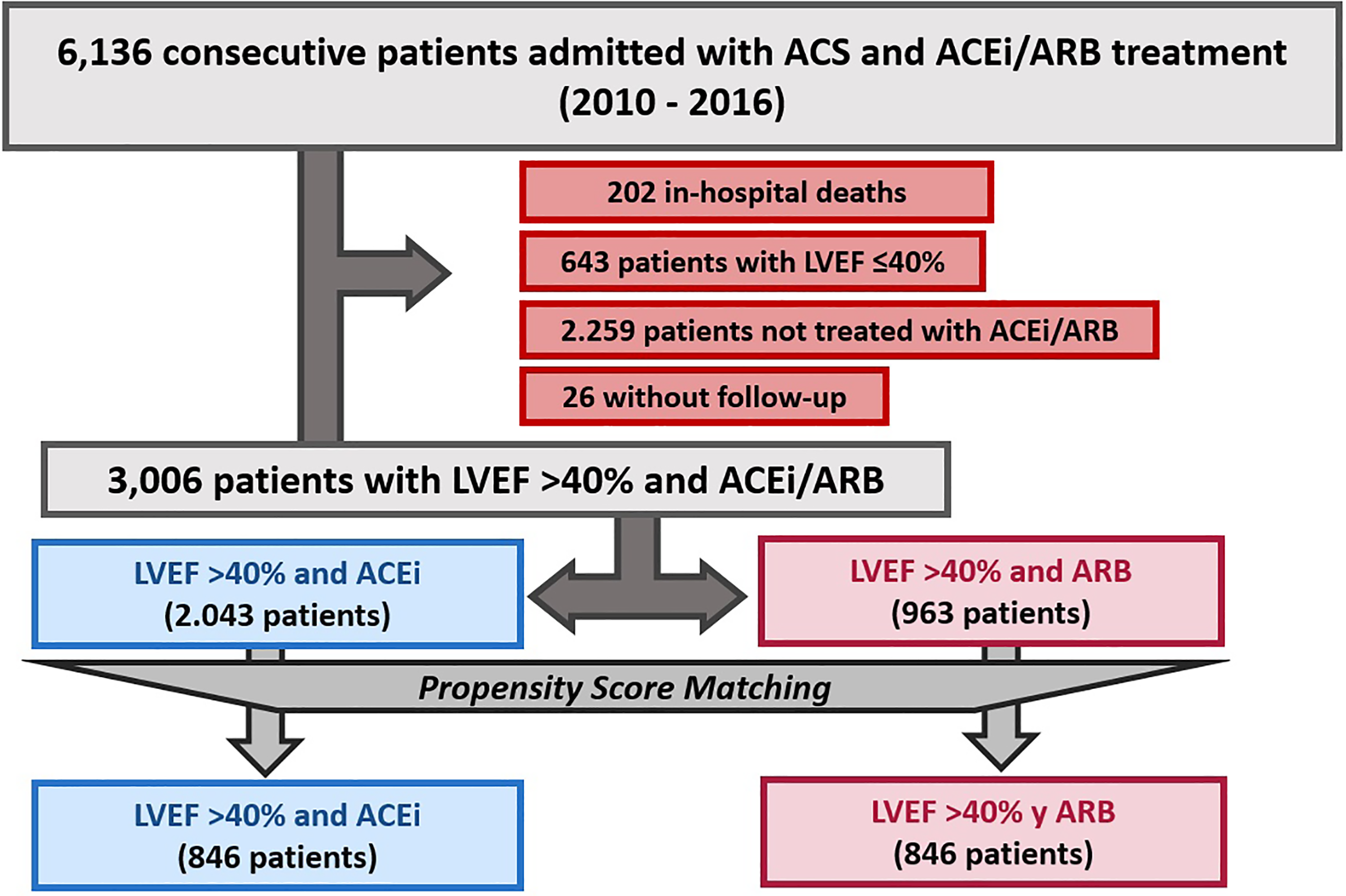
Flowchart of study population. ACEi indicates angiotensin-converting enzyme inhibitor; ACS, acute coronary syndrome; ARB, angiotensin II-receptor blocker; LVEF, left ventricular ejection fraction.
The primary end point was a combination of all-cause death, acute myocardial infarction (AMI) and heart failure (HF) during follow-up. As secondary end points, we separately analyzed mortality from any cause, AMI and HF for each of the treatment groups. Diagnosis of AMI was based on the universal definition of AMI. 10 Diagnosis of HF was based on the definition recommended in the current European HF guidelines. 11 For this purpose, we considered all hospitalizations after hospital discharge for ACS in which HF was a primary diagnosis.
Statistical Analysis
This was performed with SPSS version 25.0, R version 3.2.2, and Stata MP64 version 14.1. Baseline characteristics according to treatment with ACEi or ARB were described by using number and percentage for categorical data and standardized mean difference for continuous data, respectively. Differences in characteristics were assessed by using χ2 tests and 2-sample Student t tests. The association between ACEi or ARB exposure and events was studied in robust Cox proportional hazards models with adjustment for potential confounders at baseline. The multivariable model risk adjustment was performed with all variables associated with postdischarge major cardiovascular events based on clinical plausibility or P < .05 in the univariate Cox analyses. Because of important differences in key baseline characteristics depending on prescription of ACEi or ARB therapy (Table 1), we assessed the association between ACEi or ARB exposure and cardiovascular events using a propensity score matching (PSM) analysis. Propensity scores (PS) were estimated using a nonparsimonious multivariable logistic regression model, with ACEi therapy as the dependent variable and those characteristics that differed between patients treated and not treated with ACEi or ARB (Table 1) as covariates. We applied a greedy 1:1 matching algorithm without replacement and defined optimal matching as a SD of 0.2. Subsequent PSM was performed to assemble a cohort in which all the measured covariates would be well balanced across both groups (ACEi and ARB, Table 1). In the PS-matched population (constituted by 2 groups of 846 patients with similar characteristics according to prescription of ACEi or ARB), the reduction in the rate of death, reinfarction, and HF was compared using a robust stratified Cox regression model. Results were expressed as hazard ratio (HR) with its 95% CI. The effect of ACEi versus ARB was graphically represented in Kaplan-Meier curves. A 2-sided P < .05 was considered significant.
Baseline Characteristics Before and After PSM According to ACEi/ARB Prescription.
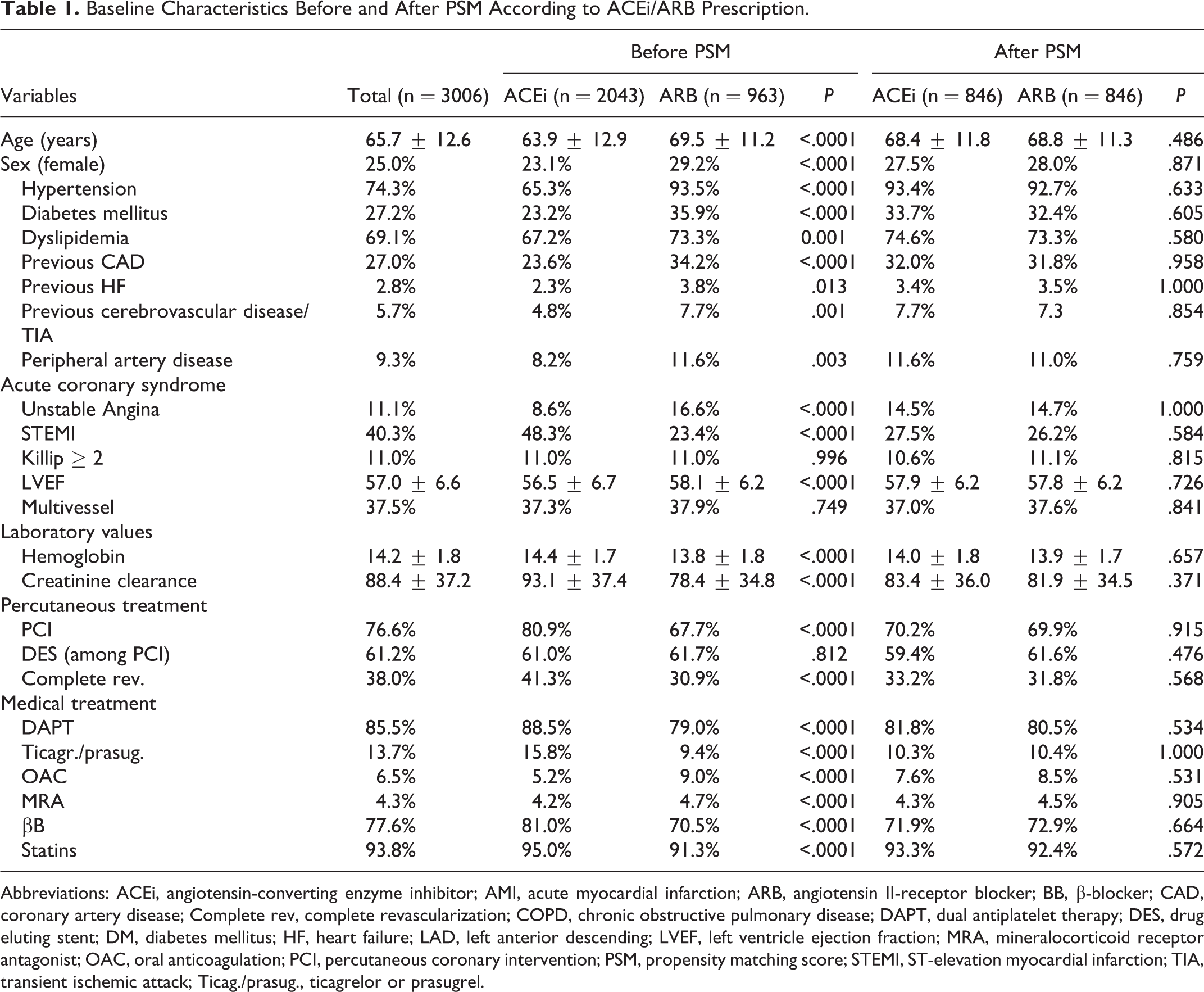
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin II-receptor blocker; BB, β-blocker; CAD, coronary artery disease; Complete rev, complete revascularization; COPD, chronic obstructive pulmonary disease; DAPT, dual antiplatelet therapy; DES, drug eluting stent; DM, diabetes mellitus; HF, heart failure; LAD, left anterior descending; LVEF, left ventricle ejection fraction; MRA, mineralocorticoid receptor antagonist; OAC, oral anticoagulation; PCI, percutaneous coronary intervention; PSM, propensity matching score; STEMI, ST-elevation myocardial infarction; TIA, transient ischemic attack; Ticag./prasug., ticagrelor or prasugrel.
Results
Among 3006 ACS patients with preserved LVEF, 2043 (68%) were discharged on ACEi treatment and 963 (34.4%) on ARBs. Table 1 shows the baseline characteristics stratified by each drug.
Patients who were prescribed ACEi were younger, were at lower cardiovascular risk (with lower prevalence of diabetes mellitus, dyslipidemia, and hypertension), and had lower rates of previous cardiovascular disease (previous coronary disease, HF, peripheral, or cerebrovascular disease). Angiotensin-converting enzyme inhibitor was mainly prescribed for patients with ST-segment elevation ACS (STE-ACS), while ARB prescription was significantly higher in non-ST-segment elevation ACS (NSTE-ACS).
In relation to absolute values of clinical outcomes, we observed that during mean follow-up of 3.6 ± 2.1 years, within the overall population, 392 (13.0%) patients died, 274 had an AMI (9.1%), and 442 were admitted for HF (14.7%).
The non-adjusted incidence rate for mortality was 3.03 cases/100 person-year for ACEi and 4.85 cases/100 person-year ARB. The incidence rates for re-AMI were 2.31 events/100 person-year for ACEi and 3.50 events/100 person-year for ARB and for HF were 3.63 events/100 person-year for ACEi and 6.12 events/100 person-year for ARB.
We performed a PSM and obtained 2 groups of 846 patients of comparable baseline characteristics. We did not find differences in postdischarge outcomes (Table 2) or survival analysis (Figures 2 and 3): death from any cause (HR for ARB: 0.952, 95% CI: 0.70-1.29), AMI (HR for ARB: 1.34, 95% CI: 0.95-1.89), HF (HR for ARB: 1.11, 95% CI: 0.85-1.45), and combined event of the 3 previous end points (HR for ARB: 1.14, 95% CI: 0.92-1.40).
Clinical Outcomes Before and After PSM According to ACEi/ARB Prescription.
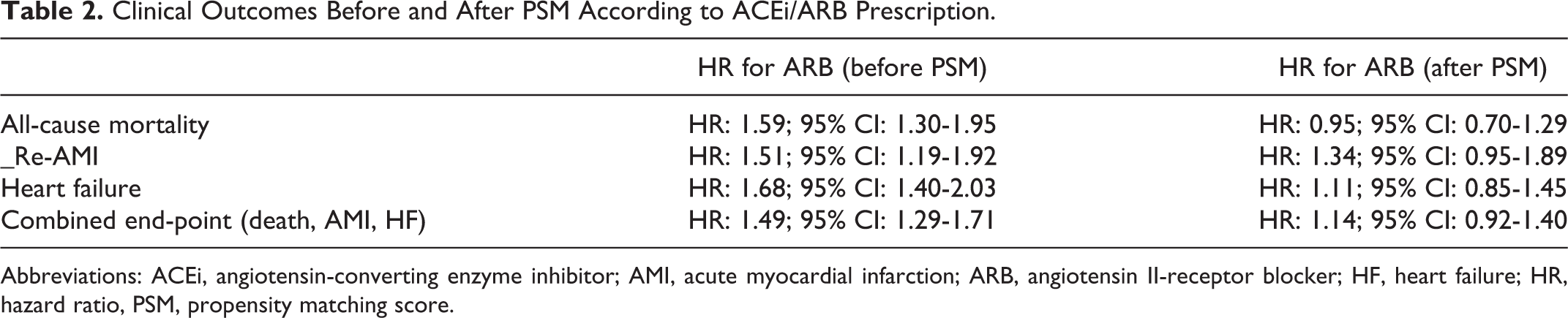
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin II-receptor blocker; HF, heart failure; HR, hazard ratio, PSM, propensity matching score.
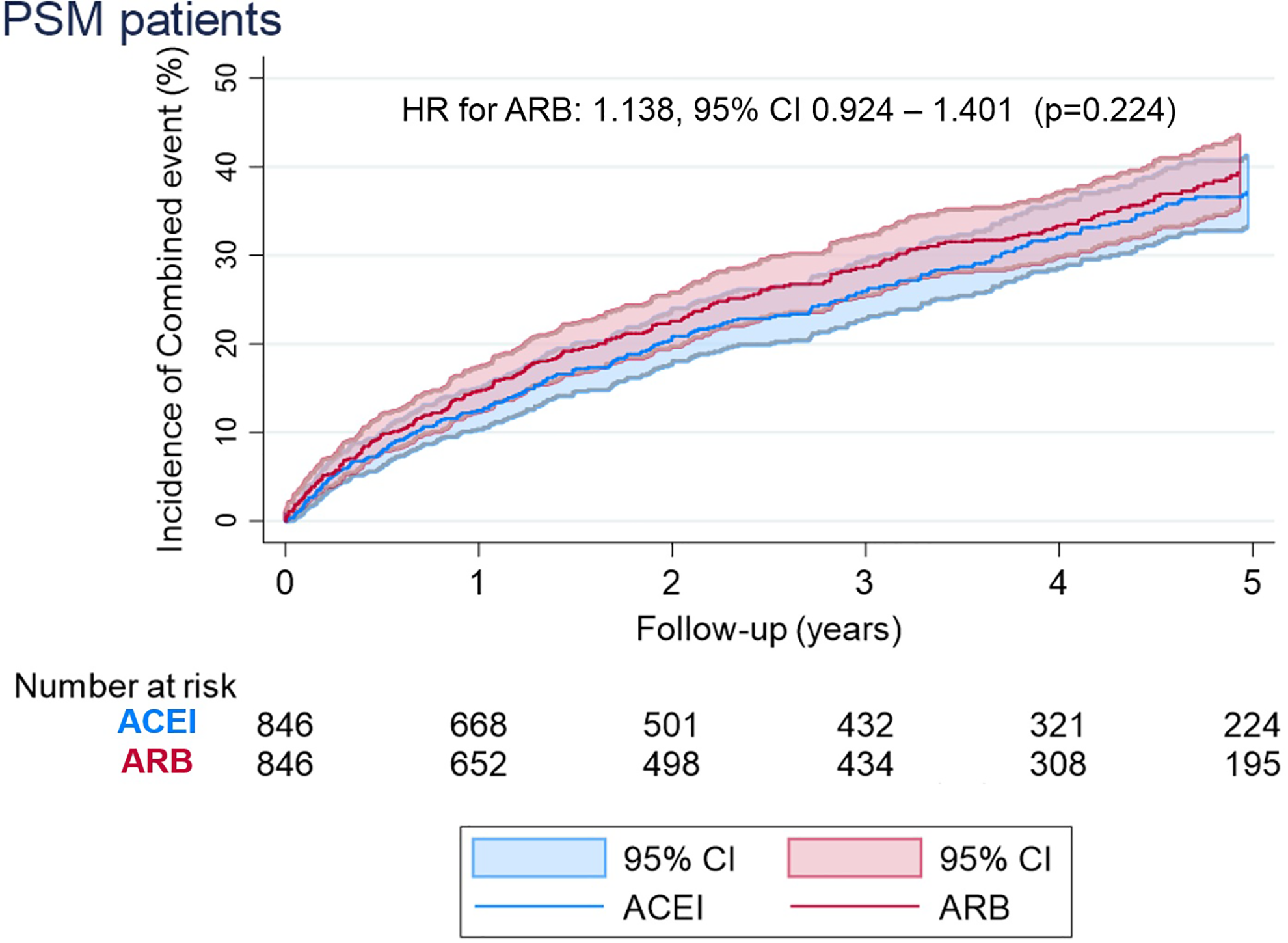
Incidences of combined event (all-cause death, acute myocardial infarction, and heart failure) according to treatment with ACEi or ARB. ACEi indicates angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin II-receptor blocker; HR, hazard ratio; PSM, propensity score matching.
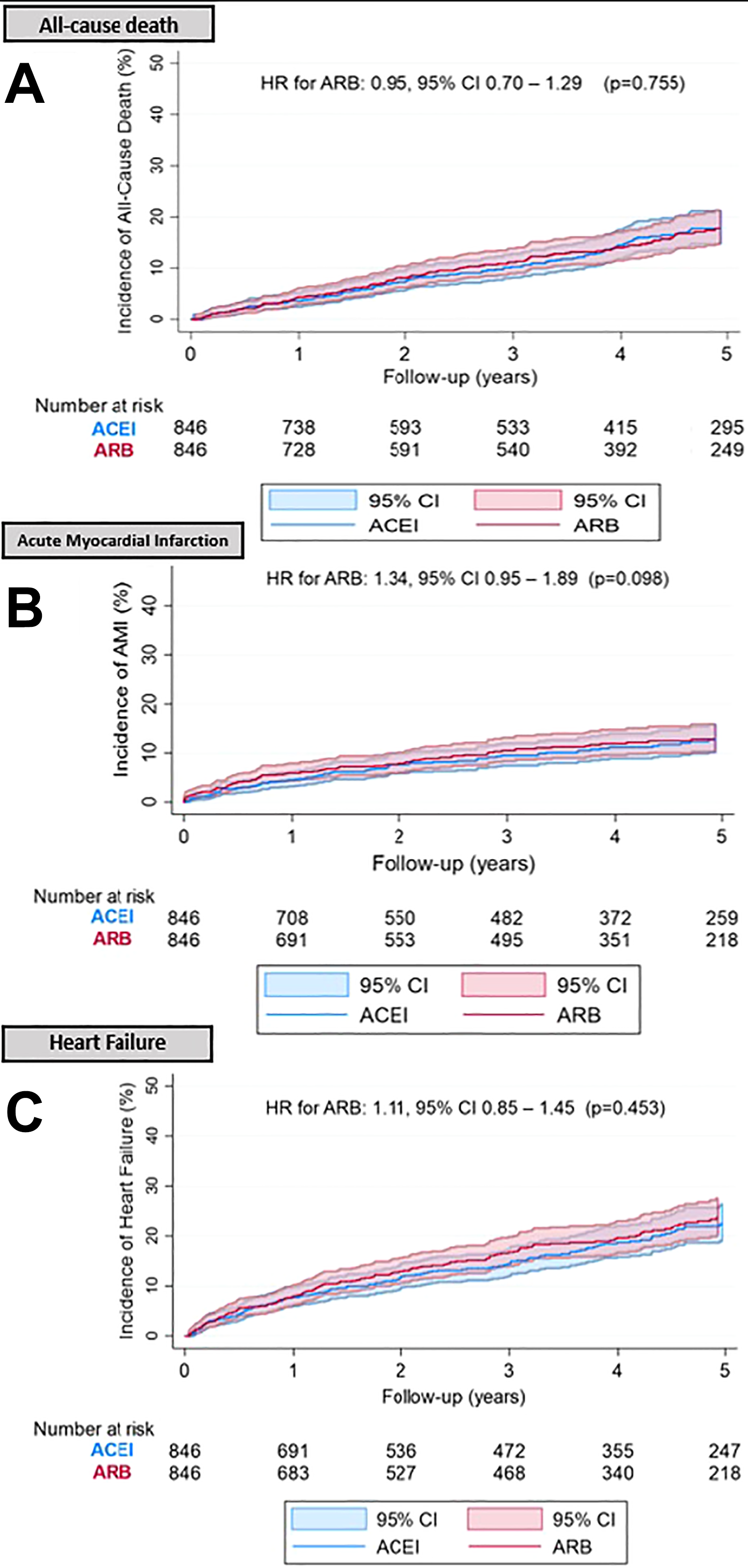
Incidence of all-cause death (A), acute myocardial infarction (B), and heart failure (C) according to treatment with ACEi or ARB. ACEi indicates angiotensin-converting enzyme inhibitor, AMI, acute myocardial infarction; ARB, angiotensin II-receptor blocker; HR, hazard ratio; PSM, propensity score matching.
In addition, we compared the prognostic benefit between ACEi and ARB in patients with ST-elevation ACS (STE-ACS) and patients without ST-elevation ACS (NSTE-ACS). We did not observe differences between both drug classes regarding the incidence of the combined event (HR for ARB: 1.03, 95% CI: 0.85-1.24; P = .796 for NSTE-ACS vs HR for ARB: 1.82, 95% CI: 0.82-1.70; P = .366 for STE-ACS), AMI (HR for ARB: 1.03, 95% CI: 0.75-1.43; P = .839 for NSTE-ACS vs HR for ARB: 1.36, 95% CI: 0.65-2.83; P = .409 for STE-ACS), or HF (HR for ARB: 1.04, 95% CI: 0.81-1.34; P = .768 for NSTE-ACS vs HR for ARB: 1.02, 95% CI: 0.63-1.65; P = .936 for STE-ACS; Figure 4).
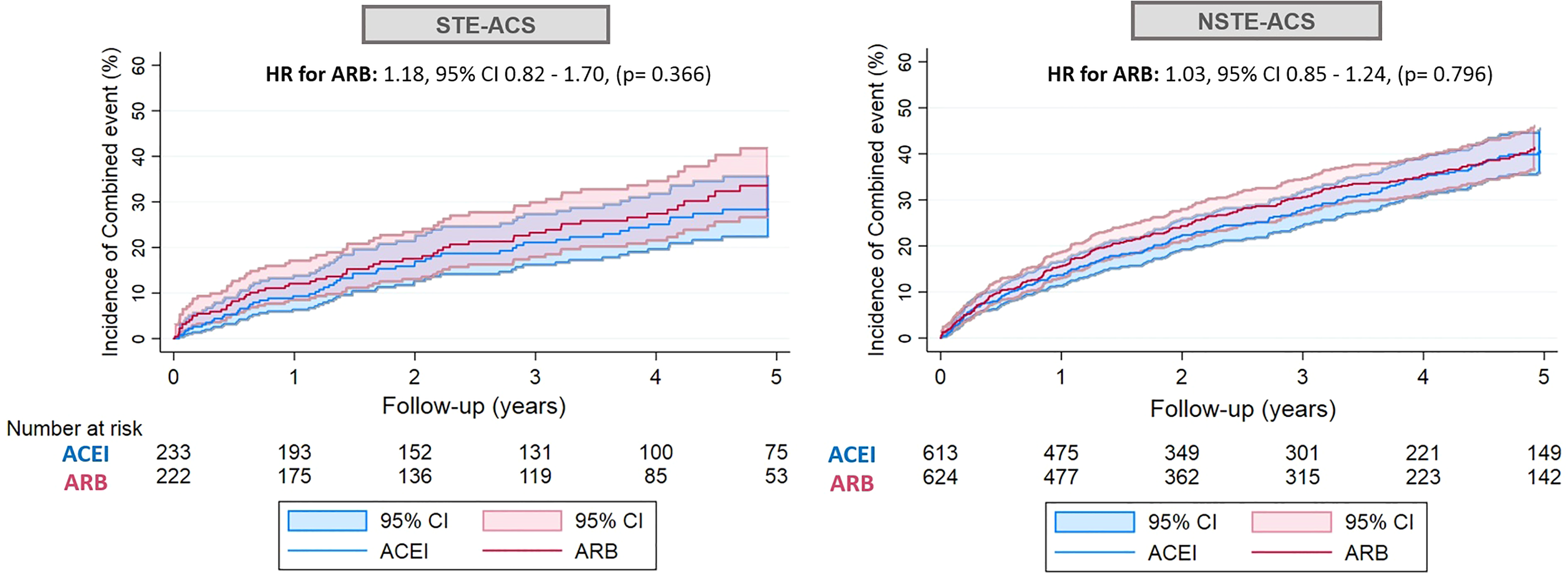
Incidences of combined event (all-cause death, acute myocardial infarction, and heart failure) according to treatment with ACEi or ARB by groups (NSTE-ACS vs STE-ACS). ACEi indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin II-receptor blocker; HR, hazard ratio; NSTE-ACS, non-ST elevation acute coronary syndrome; STE-ACS, ST elevation acute coronary syndrome.
A subgroup analysis was also performed in a multivariate Cox regression analysis without prognostic differences between ACEi and ARB (Figure 5).
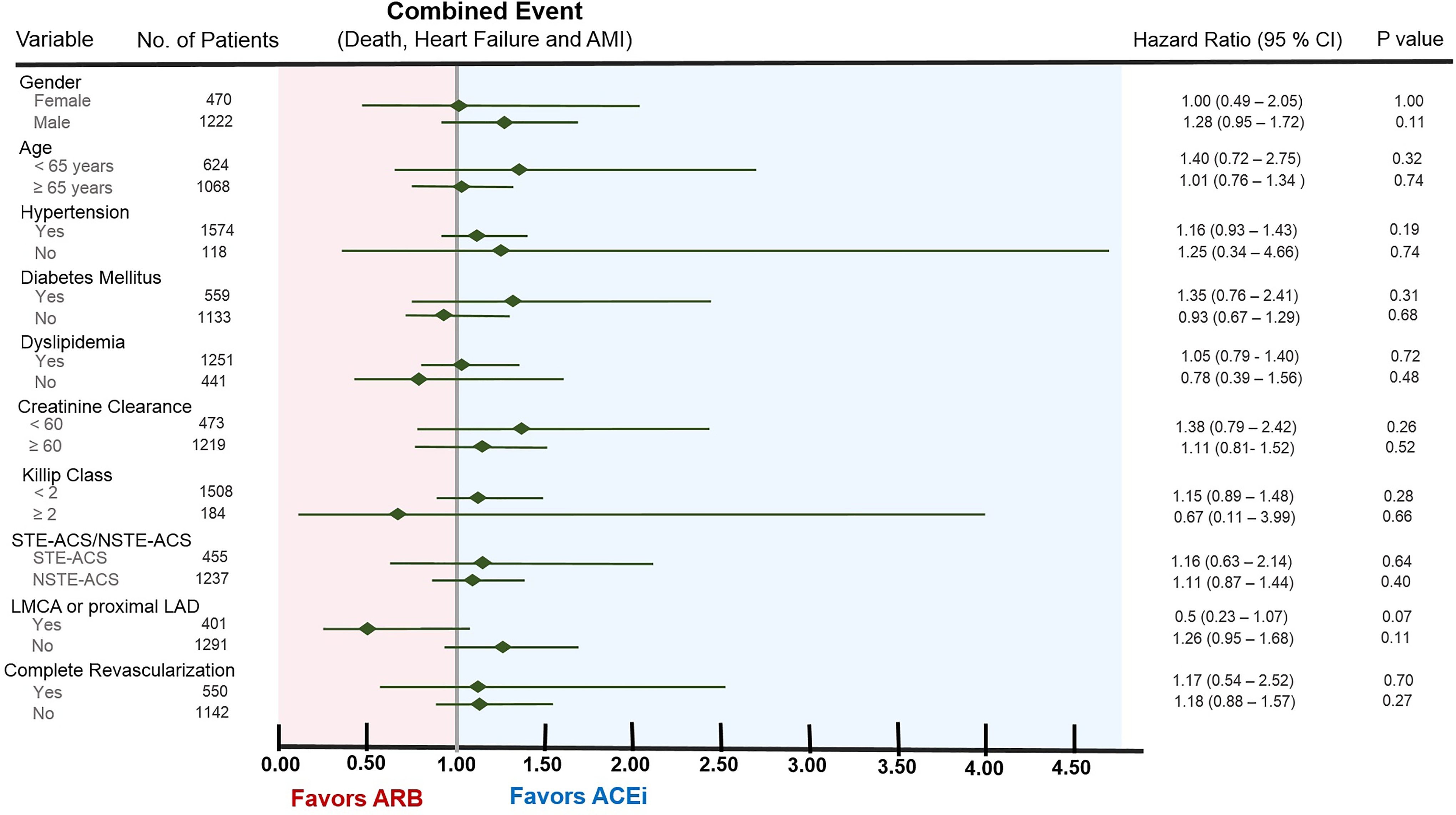
Multivariate Cox regression analysis for primary end point (all-cause death, AMI, and/or HF) between treatments groups (ACEi vs ARB), adjusting by clinical characteristics and cardiovascular risk factors. ACEi indicates angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin II-receptor blocker; HF, heart failure; LAD, left anterior descending; LMCA, left main coronary artery; NSTE-ACS, non-ST elevation acute coronary syndrome; STE-ACS, ST elevation acute coronary syndrome.
Discussion
Our study compared the effectiveness of ACEi versus ARB in patients with preserved LVEF after an ACS, based on contemporaneous and real-world data. We found that there are no differences between both therapies in terms of mortality, re-AMI, or HF development. We found no differences in the effectiveness of these drugs in the subgroup analysis according to clinical characteristics at admission (ACS type, proximal vessel disease, Killip class, or renal impairment) and cardiovascular risk factors (DM, dyslipidemia, or hypertension).
The absence of benefit of one therapy over the other is consistent with other clinical trials and observational studies.12,13 However, the small percentage of patients with preserved LVEF and without HF included in their cohorts make the results not completely valid for our target population: patients with preserved LVEF after an ACS.
In recent years, several studies have been published that point toward the possible prognostic difference between ACEi and ARB given their distinct pharmacological mechanisms of action and different target in the neurohormonal cascade.14–17 Specifically in patients with history of ischemic heart disease, a recent meta-analysis shows that ACEi provide a potentially important blood pressure–independent clinical benefit, which is not present in ARB treatment. 16 There are defined pathophysiological bases that explain the different pharmacological properties and effects of both therapies. Angiotensin-converting enzyme inhibitor act by decreasing angiotensin II synthesis and inhibiting the bradykinin degradation to inactive peptides whereas ARB directly prevent the activation of AT1 receptor, which could lead to a significantly increase in angiotensin II levels and upregulation of AT2 receptors. AT2 receptors are involved in hypertrophy, proatherogenic, and pro-inflammatory effects as well as in angiogenesis inhibition. 17
However, the real benefit of one drug over the other in patients with preserved LVEF has not been fully evaluated in contemporary populations of patients with ischemic heart disease. VALIANT trial demonstrated that ARBs are a clinically effective alternative for ACEis in improving survival and reducing cardiovascular morbidity after an AMI. Nevertheless, this study only included patients with reduced LVEF (<35%), which does not allow validating these results to patients with preserved ventricular function. 12
OPTIMAAL trial was also carried out in patients after an AMI to compare ACEi and ARB. They found that ARB was associated with a significant increase in CV mortality after 2.7 years of follow-up, but this trend in favor of ACEi did not satisfy the trial’s noninferiority criteria. However, PCI was performed in very few patients (15%) and they only included patients with preserved LVEF when presenting along with acute HF at admission. 13
In recent years, several studies aimed to assess whether there are prognostic differences between ACEi and ARB depending on the type of ACS. In non-STEMI (NSTEMI)-ACS patients, Kim et al 18 showed that ACEi was related to a decrease in the occurrences of MACE (major adverse cardiac events), any repeat revascularization and target vessel revascularization compared with ARB, during a 2-year follow-up period. The authors state that the differences observed could be related to the intimal neoformation blocking capacity that ACEi have in animal-model assays. Nevertheless, they found similar mortality cumulative incidences and re-MI incidence between the 2 groups and this corresponds to our findings on the absence of significant clinical differential benefit.
On the other hand, in STEMI-ACS patients, Yang et al recently reported similar beneficial effects between ACEi and ARB in terms of mortality and MI, reaffirming that both drugs can be used interchangeably in the context of ACS. 7
In relation to comparative effectiveness in different subgroups, some recent observational studies reported comparable effectiveness between ACEi and ARB post-ACS even in some special population as DM patients.19,20 However, they did not segregate patients by LVEF, which does not allow drawing valid specific conclusions for these subgroups among preserved LVEF population. In our study, we did not find relevant differences between subgroups of patients based on clinical features and risk factors, as shown in Figure 5.
Regarding clinical outcomes, we have presented our results in absolute value for complete follow-up period (3.6 ± 2.1 years), relative value, and incidence rate. We are concerned about high mortality, re-AMI, and HF rates in post-ACS patients. Without a doubt, the high average age of our patients is one of the plausible explanations of these results. On the other hand, our results are comparable with those of other recently published observational studies and clinical trials.21,22 Nevertheless, we consider that they are suboptimal results and this constitutes a real challenge for improvement in contemporary cardiology.
Concerning follow-up time of the study, there are some studies that showed that prognostic differences between ACEi and ARB in post-AMI patients in the recent PCI-era were only evident after the second year from discharge, being equivalent before that period. 23 In this context, our study includes a broad follow-up period, which adds value to the obtained results: the long-term equivalence between both therapies.
Several recent observational studies have also compared the effectiveness of ACEi and ARB in combination with other drugs of proven efficacy in patients with chronic heart disease. The variety and the different direction of the results are surprising. It has been reported that ARBs offer better results if they are combined with statins. 24 However, including data about LVEF in these analyses could change the conclusions. Kim et al showed that in the group of patients with preserved LVEF and NSTEMI, although the mortality and re-MI reduction benefits were similar between the use of ACEi and ARB, the ACEi group showed more prominent ability to decrease the occurrences of MACE, any repeat revascularization, and target vessel revascularization compared with the ARB group during a 2-year follow-up period. 18
According to international clinical practice recommendations, ACEi should be the first choice drug over ARB. Angiotensin II receptor blockers are proposed as an alternative only in case of intolerance of ACEi, without setting an efficacy criteria. This recommendation is based on several studies and clinical trials whose conclusions are not completely applicable to the contemporary population of patients treated for AMI and, specifically, to those with preserved LVEF.16,25,26 On the one hand, most of these studies were developed in a non-AMI scenario, in which the majority of patients had depressed LVEF or acute HF at admission. On the other hand, the current cohorts of patients with ischemic heart disease have significantly different baseline characteristics compared to those included in the studies. Nowadays, patients with ACS undergo a higher rate of percutaneous revascularization and optimal medical treatment (BB, dual antiplatelet treatment, statins, etc). These conditions suppose an intrinsic improvement in survival and do not allow a complete extrapolation of former results.
To our knowledge, our study is the first to compare ACEi versus ARB in a non-Asiatic population of patients with ACS and preserved LVEF. Based on our results, the use of both drugs could be equivalent in these patients. This could encourage the development of further investigation and, potentially, upgrade the indication for treatment with ARBs, at least, at the same level as ACEis in the context of ACS with preserved LVEF.
Our study has several limitations. Firstly, this was a retrospective observational study. Although we performed a PS adjusting analysis, our study was not randomized sample, and had the usual limitations and biases inherent to retrospective study designs. Second, the survival and prognosis benefits of ACEi or ARB were analyzed based on the principle of intention-to-treat since it is not possible to assess adherence or changes in treatment during follow-up. However, it should be noted that, according to previous studies, only a minority of patients undergo changes in RAAS inhibitors therapies in the first 3 years after an ACS.27,28 We do not have either data about the treatment strategies performed (primary PCI or within 48 hours) nor information related to the infarct-related artery. This would be interesting to know whether ACEi offer some differential benefit compared with ARB based on earlier revascularization or depending on the affected coronary territory. Despite these limitations, the results of the present study, showing the equivalent effectiveness of ACEi and ARB in patients with preserved LVEF after an ACS, are consistent with other recently published studies (in Korean population).18,19 This finding could constitute the basis for developing and guiding future clinical trial design that may have clinical impact on medical practice.
Conclusions
Angiotensin-converting enzyme inhibitor and ARB effectiveness in ACS patients with preserved LVEF is equivalent in terms of survival and strong cardiovascular end points, such as AMI or HF. This equality is maintained throughout the follow-up, even after statistical adjustments and subgroup analyses.
Footnotes
Author’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.