
Abstract
The differential impact of young age and female gender on transradial access (TRA) outcomes remains to be confirmed. The primary objective was to assess the impact of young age and female gender on in-hospital net adverse cardiovascular events (NACE). Among 12 346 patients from the Coronary Angiogram Database of South Australia (CADOSA) Registry, the impact of gender; men (transfemoral access [TFA] 1995, TRA 6168) and women (TFA 1249, TRA 2934), and a median split of age, ≤63 years (TFA 1617, TRA 4727) and >63 years (TFA 1627, TRA 4375) were analyzed on in-hospital outcomes by creating 5 separate propensity-matched cohorts (entire cohort, men, women, ≤63 and > 63 years). Net adverse cardiovascular event reduction with TRA was limited to the >63 years old cohort (odds ratio [OR] = 0.56, 95% CI: 0.34-0.93, P = .02) and women (OR = 0.37, 95% CI: 0.18-0.76, P = .007). In both the age groups and genders, TRA was associated with a lower risk of bleeding and all-cause mortality. On multivariate logistic regression, TRA was associated with a significant reduction in NACE, major bleeding, and mortality in the overall cohort. In conclusion, a reduction in bleeding and mortality was noted with TRA in all the subgroups in this observational study.
Introduction
Coronary angiography and angioplasty reduce major adverse cardiovascular events (MACE) but with an associated risk of increased bleeding, which may result in worse short- and long-term clinical outcomes. 1 Therefore, while reducing MACE, efforts to reduce of bleeding events have the potential to further reduce morbidity, mortality, and costs. A common source of bleeding following coronary angiography is access site bleeding which remains a major cause of morbidity and prolonged hospital stay. In this context, transradial access (TRA) has been found to be superior to transfemoral access (TFA) in reducing access site bleeding events. 2 Compared with the femoral artery, the radial artery is more superficial and has a smaller caliber, therefore making access site hemostasis more achievable. Studies comparing TRA with TFA have shown mixed results when analyses have been performed in specific acute coronary syndrome (ACS) groups. 3 –6 However, there is a strong trend toward fewer adverse outcomes with TRA. 7,8
One factor, which makes TFA procedures challenging, is the advanced age of the patients. 9 Compared with the young, elderly patients have many factors that increase the risk of access site bleeding, including multiple comorbidities, worsening renal function, presence of complex coronary disease, and calcified femoral vessels. 10,11 Therefore, it can be anticipated that the benefits of TRA over TFA are most evident in an elderly population and possibly not present in young patients, who have a lower risk of access site bleeding. We hypothesized that patients under 63 years old (median age of the cohort) would not achieve benefits from TRA, and in young patients, in-hospital net adverse cardiovascular events (NACE) will be similar when using TFA or TRA.
Like age, the outcomes of TRA and TFA are also influenced by gender. The data suggest that female sex is an independent risk factor for major bleeding and that the use of TRA for percutaneous coronary interventions (PCI) is likely reduces this risk. 12,13 The impact of sex on comparative outcomes was analyzed in the Minimizing Adverse Haemorrhagic Events by TRansradial Access Site and Systemic Implementation of angioX (MATRIX) trial showing that women were at higher risk of bleeding, access site complications, and requirement of transfusion. 14 There was no significant interaction for NACE stratified by sex. 14 However, there are concerns that TRA may be technically more challenging in women due to smaller radial arteries and increased rates of radial artery spasm, potentially leading to lower procedural success rates. 15 Most randomized trials comparing TRA with TFA have enrolled more men than women. 8 Our second hypothesis was that a major benefit in the reduction in NACE with the TRA is limited to women compared with men.
The primary aim of the present study was to evaluate the impact of young age and female gender on NACE. The secondary aims were to assess the impact of young age and female gender on all-cause mortality at discharge and major bleeding among patients undergoing TRA or TFA cardiac catheterization.
Methods
Data Collection
The Coronary Angiogram Database of South Australia (CADOSA) is a registry of cardiac catheterization procedures performed in the 4 public tertiary hospitals of South Australia (SA). The CADOSA Registry collects a standardized 8-page case report form (CRF) for all public coronary angiograms and PCI performed in the state. The CRF is compatible with the American College of Cardiology National Cardiovascular Data Registry. The CADOSA Registry is compatible with the American College of Cardiology (Registered Trademark) CathPCI (Registered Trademark) Registry, sharing common data elements and data specifications. The CADOSA Registry captures all the in-hospital data by prospective data collection.
We included consecutive patients who underwent coronary angiography for an indication of stable angina/chronic coronary disease or ACS between January 1, 2012, and December 31, 2016 in the 4 major teaching hospitals in SA. Patients presenting with cardiogenic shock, <18 years of age, known peripheral artery disease, a history of coronary artery bypass grafting (CABG), and inability to provide consent for data collection were excluded. For patients with multiple procedures, only the index visit was used and patients with multiple successful access sites were excluded. Demographic, angiographic procedural data, and clinical outcome data were collected prospectively in each center according to the prespecified definitions. The independent clinical research coordinators of the CADOSA Registry collected data.
Definitions
To assess the impact of age and gender on the outcomes, we divided patients into subgroups according to median age (≤63 vs >63 years) and gender. We also performed subgroup analysis on patients presenting with ACS. Furthermore, multivariate logistic regressions were performed to find independent predictors of worse and improved outcomes. In-hospital NACE was defined as a composite of death, myocardial infarction (MI), stroke, or major bleeding. In-hospital MACE was defined as a composite of death, MI, or stroke. All-cause mortality was recorded within 24 h of the procedure and at discharge. Major bleeding was defined as a hemoglobin drop of ≥30 g/L; or transfusion of whole blood or packed red blood cells; or procedural intervention/surgery at the bleeding site to reverse/stop or correct the bleeding (such as surgical closures/exploration of the arteriotomy site, balloon angioplasty to seal an arterial tear, endoscopy with cautery of a gastrointestinal bleed).
In the majority of patient, intravenous heparin was the main anticoagulant during PCI, and bivalirudin use was limited to only 122 (0.9%) patients. The dose of heparin was adjusted according to the body weight of the patient with an aim to keep activated clotting time (ACT) between 250 and 300 seconds for the PCI cases.
Statistical Methods
Gender- and age-specific baseline characteristics were compared across access sites. We used t tests to compare continuous covariates and χ2 tests to compare categorical data. Two-sided P values <.05 were considered significant. Logistic regressions were then performed on the entire cohort.
For propensity score matching, cohorts were created for the entire cohort and for each subgroup analysis. Matching on subgroup-specific propensity scores (PS) was performed and as it has been demonstrated to improve balance and bias reduction when there are true differences across subgroups. 16,17 The 5 propensity-matched cohorts created were entire cohort, men, women, ≤63 years, and >63 years. Propensity scores were calculated using a multivariable logistic regression. The PS was the conditional probability that a patient will receive TRA, given the covariates in Table 1. After obtaining the PS, we then utilized inverse probability of treatment weighting (IPTW) approaches to create stabilized weights. As simple IPTW can result in large weights that are not normally distributed, stabilized weights marginalizing the probability of TRA were used to reduce variability and improve the precision of the estimates. The marginal probability of TRA was calculated for this purpose also using logistic regression. Thus, for TRA patients, stabilized IPTW weights were calculated by dividing the marginal probability of TRA by the individual patient’s propensity score. For TFA patients, stabilized IPTW weights were calculated by dividing (1 minus the marginal probability of TRA) by (1 minus the individual patient’s propensity score). The adequacy of the stabilized IPTW weighting was assessed by checking the distribution of PS by treatment for reasonable overlap and the pre- and post-IPTW balance of the covariates. Finally, IPTW-adjusted logistic regression models were used to evaluate whether access site was an independent predictor of in-hospital outcomes (bleeding, NACE, MACE, death within 24 hours, and death on discharge). Figure 1 shows the reduction in bias across the confounders after adjustment of confounders.
Gender-Specific Demographics, Risk Factors, and Clinical Features by Access Site in the Overall Cohort.
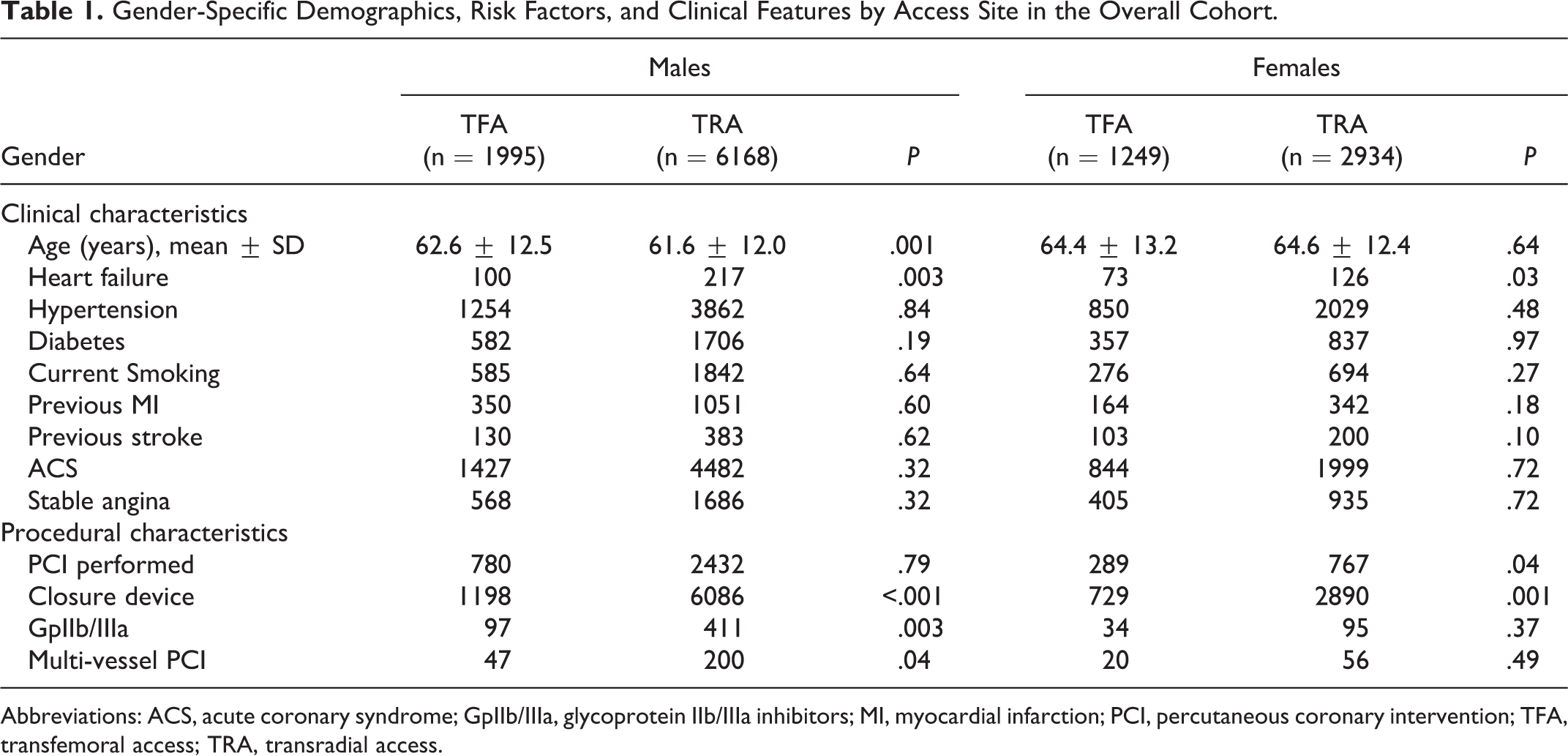
Abbreviations: ACS, acute coronary syndrome; GpIIb/IIIa, glycoprotein IIb/IIIa inhibitors; MI, myocardial infarction; PCI, percutaneous coronary intervention; TFA, transfemoral access; TRA, transradial access.
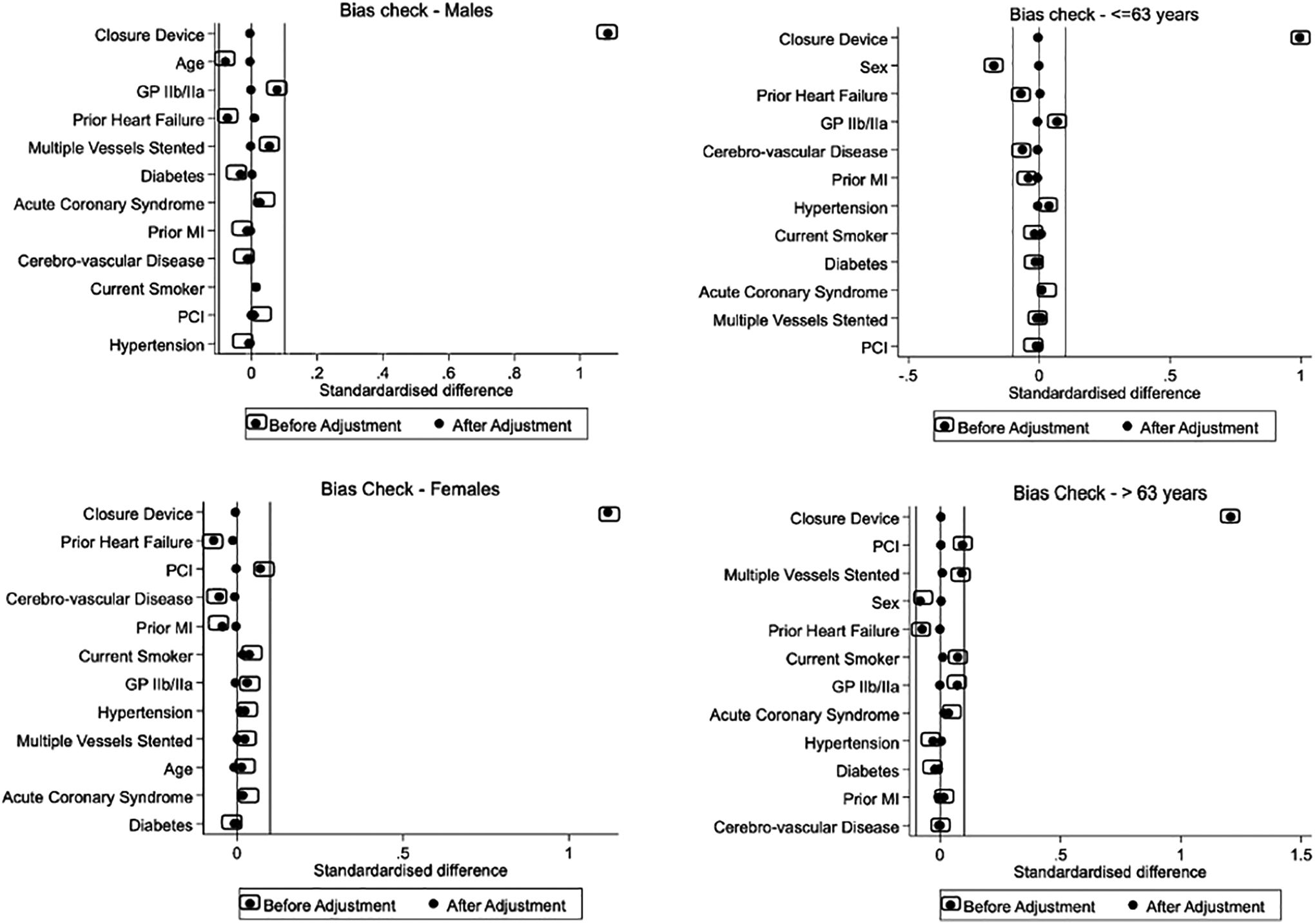
Bias before and bias after for the propensity samples. GpIIb/IIIa indicates glycoprotein IIb/IIIa inhibitors; MI, myocardial infarction, PCI, percutaneous coronary intervention.
Results
Baseline Characteristics
A total of 12 346 patients (TFA 3244, TRA 9102) were included in the analysis. The entire cohort of the patients were divided into 4 subgroups according to the gender; men (TFA 1995, TRA 6168) and women (TFA 1249, TRA 2934), and 2 quartiles of age; and ≤63 years (TFA 1617, TRA 4727) and >63 years (TFA 1627, TRA 4375).
Tables 1 and 2 depicts the differences in baseline characteristics across 2 access sites by the gender and age-group. Among men, the TRA cohort was younger. In both genders, patients with heart failure were more likely to undergo TFA. As expected, the closure device was more likely in the TRA cohort in both the genders. In both the age groups, women were more likely to undergo TFA. The use of GpIIb/IIIa inhibitors was greater in the TRA group.
Age-Specific Demographics, Risk Factors, and Clinical Features by Access Site in Overall Cohort.

Abbreviations: ACS, acute coronary syndrome; GpIIb/IIIa, glycoprotein IIb/IIIa inhibitors; MI, myocardial Infarction; PCI, percutaneous coronary intervention; TFA, transfemoral access; TRA, transradial access.
In the overall cohort, the unadjusted rates for NACE, MACE, and major bleeding events were 1.38%, 0.87%, and 0.59%, respectively. The unadjusted all-cause mortality rate in the first 24 hours of procedure was 0.13%, while the unadjusted overall in-hospital all-cause mortality rate was 0.65% (Supplementary Table 1). In the total cohort, 73 (0.59%) patients had a post-procedural MI and 26 (0.21%) had a post-procedural stroke.
Effect of Young Age on Clinical Outcomes of TRA Compared With TFA
In young patient group (≤63 years), there was no difference in NACE between the TRA and TFA (odds ratio [OR] = 0.64, 95% CI 0.35-1.16, P = .14) compared with >63 years old where TRA reduced NACE (OR = 0.56, 95% CI: 0.34-0.93, P = .02). In both the age groups, TRA was associated with lowered risk of major bleeding ([≤63 years age-group, OR = 0.20, 95% CI: 0.08-0.53, P = .001], [>63 years age-group, OR = 0.26, 95% CI: 0.13-0.53, P < .001]) and all-cause mortality on discharge ([≤63 years age-group, OR = 0.39, 95% CI: 0.15-0.99, P = .049], [>63 years age-group OR = 0.45, 95% CI: 0.23-0.87, P = .02]). Figure 2 shows the forest plots for the ORs for the propensity-matched age groups.
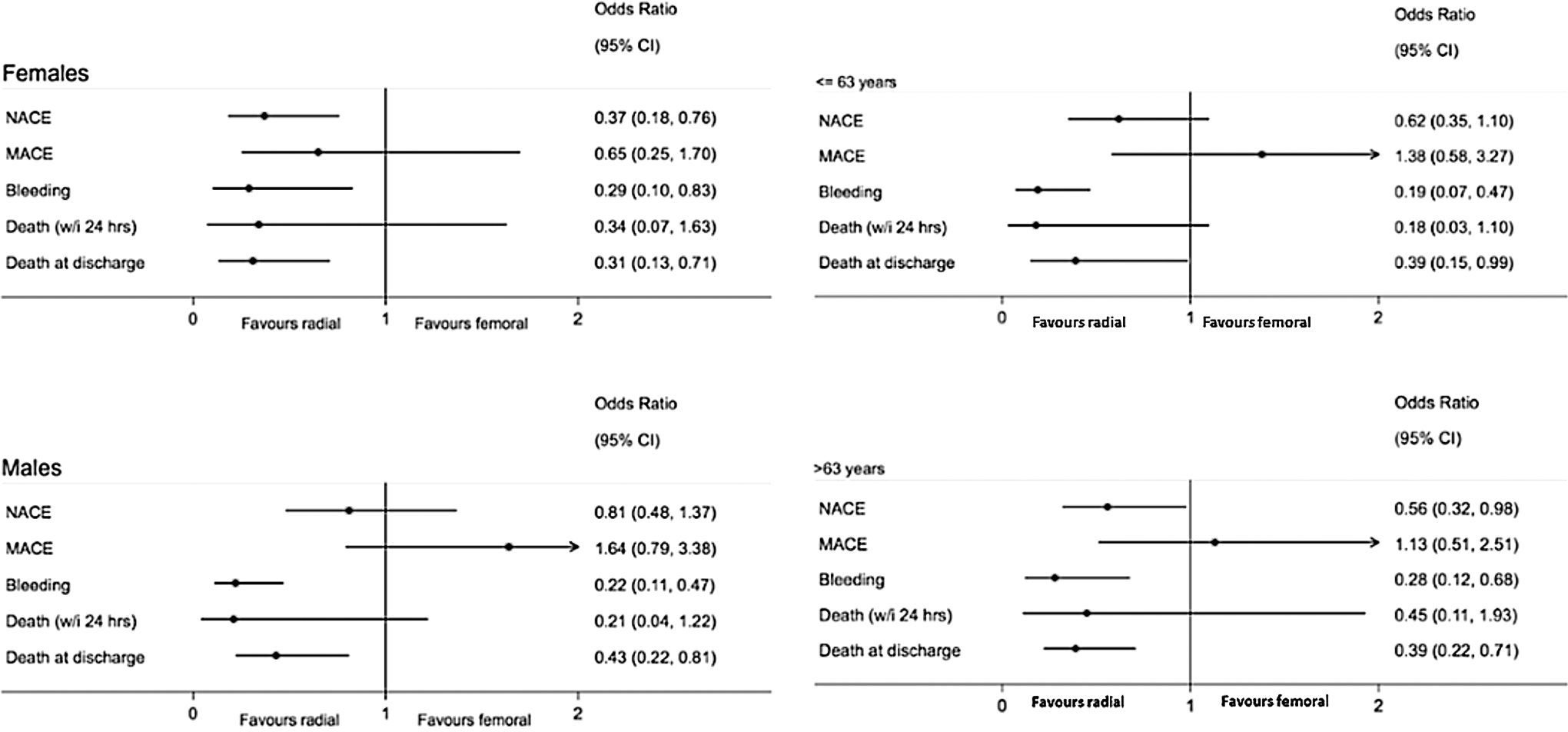
Forest plots for the odds ratios for the propensity-matched male and female cohorts and propensity-matched age groups for the in-hospital outcomes. MACE indicates major adverse cardiovascular events; NACE, net adverse cardiovascular events; OR, odds ratio.
On subgroup analysis of patients with ACS, TRA was associated with a reduction in NACE ([≤63 years age-group, OR = 0.47, 95% CI: 0.26-0.86, P = .02], [>63 years age-group, OR = 0.5, 95% CI: 0.28-0.90, P = .02]), major bleeding ([≤63 years age-group, OR = 0.18, 95% CI: 0.07-0.46, P < .001], [>63 years age-group, OR = 0.28, 95% CI: 0.11-0.72, P = .009]), and all-cause mortality at discharge ([≤63 years age-group, OR = 0.36, 95% CI: 0.14-0.95, P = .04], [>63 years age-group, OR = 0.41, 95% CI: 0.22-0.77, P = .005]) in both the age groups (Supplementary Table 8).
Effect of Gender on Clinical Outcomes of TRA Compared With TFA
In the propensity-matched cohort, TRA was associated with a lower risk of NACE in women (OR = 0.37, 95% CI: 0.18-0.76, P = .007), while there was no difference in NACE between access sites in men (OR = 0.81, 95% CI: 0.48-0.137, P = .43). Transradial access was associated with reduced major bleeding ([women, OR = 0.29, 95% CI: 0.10-0.83, P = .02], [men, OR = 0.22, 95% CI: 0.10-0.46, P < .001]), and all-cause mortality at discharge ([women, OR = 0.31, 95% CI: 0.13-0.71, P = .006], [men, OR = 0.43, 95% CI: 0.22-0.81, P < .001]) in both genders. Figure 2 shows the forest plots for the ORs for the propensity-matched male and female cohorts.
On subgroup analysis of patients with ACS, TRA was associated with a reduction in NACE in women (OR = 0.33, 95% CI: 0.16-0.69, P = .003), but not in men (OR = 0.65, 95% CI: 0.38-1.12, P = .48). Transradial access led to a reduction in major bleeding ([women, OR = 0.27, 95% CI: 0.09-0.76, P = .01], [men, OR = 0.20, 95% CI: 0.10-0.43, P < .001]) and all-cause mortality at discharge ([women, OR = 0.33, 95% CI: 0.14-0.77, P = .01], [men, OR = 0.45, 95% CI: 0.23-0.87, P = .02]) in both genders (Supplementary Table 9). Age- and gender-based basic characteristics and propensity score–matched outcomes for ACS and PCI subcohort are shown in Supplementary Tables 2 to 9.
Clinical Outcomes of TRA Compared With TFA in the Entire Cohort
The in-hospital outcomes comparing TRA and TFA in the overall cohort using propensity matching are shown in Table 3. Transradial access was associated with lower risk of in-hospital NACE (OR = 0.62, 95% CI: 0.41-0.93, P = .02), major bleeding complications (OR = 0.28, 95% CI: 0.13-0.60, P = .001), reduction in all-cause mortality within 24 hours of the procedure (OR = 0.29, 95% CI: 0.09-0.91, P = .04), and all-cause mortality on discharge (OR = 0.39, 95% CI: 0.24-0.65, P < .001).
In-Hospital Outcomes by Access Site in the Entire Cohort With and Without Propensity Matching.
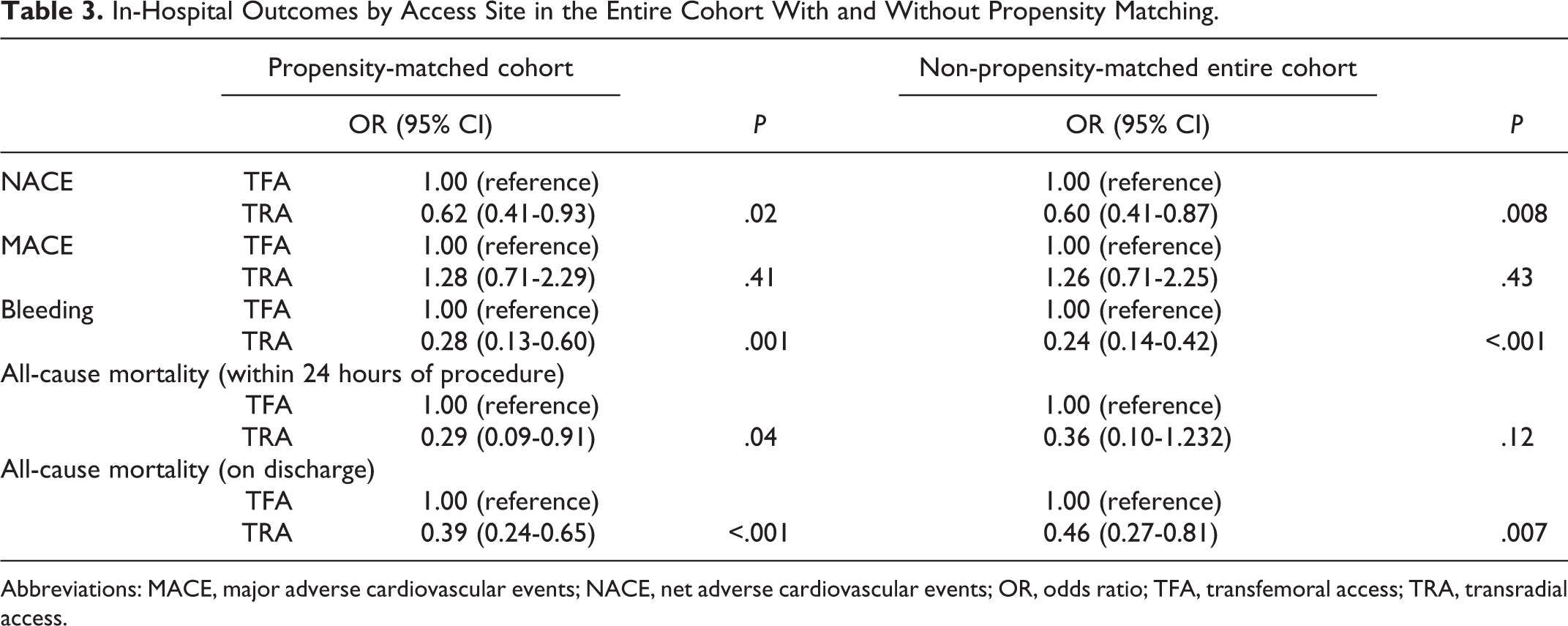
Abbreviations: MACE, major adverse cardiovascular events; NACE, net adverse cardiovascular events; OR, odds ratio; TFA, transfemoral access; TRA, transradial access.
Table 4 displays the multivariate logistic regressions in the overall cohort for each of the in-hospital complication and mortality rates. Transradial access was independently associated with decreased NACE. Transradial access was independently associated with a reduction in major bleeding, while age, female gender, current smoking, ACS, PCI, and administration of GpIIb/IIIa inhibitors were independently associated with an increase in major bleeding. Transradial access was independently associated with decreased all-cause mortality on discharge, while age, ACS, and administration of GpIIb/IIIa inhibitors were independently associated with an increase in in-hospital mortality.
Multivariate Logistic Regressions of in-Hospital Complications in Overall Cohort.a
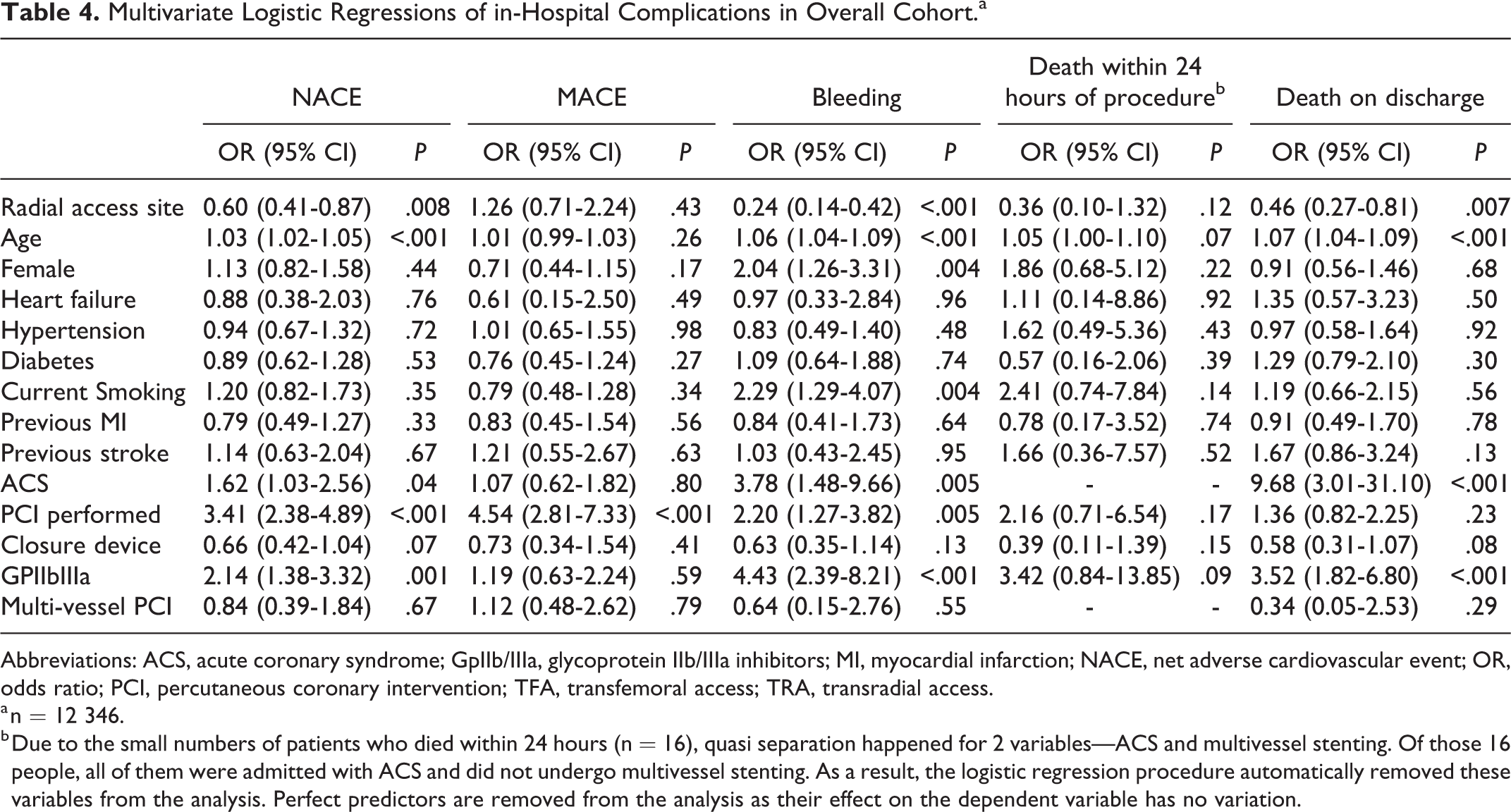
Abbreviations: ACS, acute coronary syndrome; GpIIb/IIIa, glycoprotein IIb/IIIa inhibitors; MI, myocardial infarction; NACE, net adverse cardiovascular event; OR, odds ratio; PCI, percutaneous coronary intervention; TFA, transfemoral access; TRA, transradial access.
a n = 12 346.
b Due to the small numbers of patients who died within 24 hours (n = 16), quasi separation happened for 2 variables—ACS and multivessel stenting. Of those 16 people, all of them were admitted with ACS and did not undergo multivessel stenting. As a result, the logistic regression procedure automatically removed these variables from the analysis. Perfect predictors are removed from the analysis as their effect on the dependent variable has no variation.
Discussion
The main findings of the present analysis of the real-world large-scale registry data (CADOSA) collected prospectively were: Among patient undergoing coronary angiography/PCI, the benefits of TRA to reduce NACE varied according to age and gender despite a significant reduction in bleeding in each group. This was most likely related to a high MACE in men and younger age cohort. The impact of TRA in reducing the major bleeding events and reducing all-cause mortality at discharge was independent of the age and gender of the patient group. In the overall population, TRA was independently associated with a lower risk of in-hospital NACE, major bleeding complications, and a reduction in all-cause mortality on discharge.
We noticed that the benefits of reduction in NACE were dependent upon the age and the gender of the patient. There was trend toward the benefit in NACE in both age groups and genders, but only because males and younger patients had a higher risk of MACEs, the NACE effect was diluted despite a significant reduction in bleeding. The reason for higher MACE in the younger group and in men is most likely related to the higher proportion of ACS and PCI in both of these subgroups. The number of men undergoing PCI in the whole cohort was 3 times that of women. Similarly, rate of PCI was much higher in the younger age cohort. There could be other explanations for this observation. Advanced age in itself is an independent predictor of mortality after ACS 18 and complex coronary anatomy. Complex coronary anatomy could impact clinician’s decision-making and favoring medical management over PCI. However, in the ACS subgroup, the benefits extended to both the age groups. This is probably related to an increased bleeding risk in the ACS population. (1) ACS as pathology has an independent association with increased bleeding, 19 and (2) the use of antithrombotic therapy in ACS patients increases the risk of bleeding through the TFA relatively more than the TRA. 8,19
Regarding sex-related differences in clinical outcomes, our results matched the previously published data in women undergoing TRA. The SAFE-PCI for Women trial (Study of Access Site for Enhancement of PCI for Women) evaluated the outcomes of TRA compared with TFA in women in a registry-based trial. The trial was stopped early, and even though the PCI group did not show a significant reduction in Bleeding Academic Research Consortium bleeding with TRA, there was a reduction in the bleeding and vascular complications in the overall population of which PCI cohort was a subgroup. 20 In our study, the maximum benefit in reduction in adverse outcomes with TRA was noted in women. Not only was there a reduction in all-cause mortality at discharge and bleeding, but there was also a reduction in overall NACE. Our study was different from the previously published studies such as SAFE PCI for Women and Radial versus femoral access for coronary angiography and intervention in patients with ACSs (RIVAL) in that we excluded all the patients who underwent access site crossover. Exclusion of failed TRA in our study could explain the difference in our study outcomes from SAFE PCI for women trial. Women tend to have a smaller radial artery, higher incidence of radial spasm and higher crossover. 21 At the same time, female gender is an independent predictor of higher access site bleeding. 19 Operator experience, use of smaller sheath size, medications to reduce spasm, and single right and left catheter have reduced spasm and increased success of TRA in women.
The beneficial effects of TRA over TFA noted in the current study are consistent with the results of some of the previous studies. 7,8 On the other hand, recent data from the SAFARI-STEMI (SAfety and Efficacy of Femoral Access vs RadIal Access in STEMI) study did not show any reduction in mortality at 30 days among patients undergoing primary PCI with TRA. 5 In our study, there was reduction in the all-cause mortality at discharge in all the subgroups.
The findings of our study once again confirm the superiority of TRA to TFA in overall outcomes. Our study, which involves an analysis of data from a large prospective registry, is representative of real-world practice. In most of the centers in SA, there was a progressive shift from the TFA to TRA from 2007 onward. These data were collected in the time period when most of the interventional cardiologists were very experienced with both routes for coronary angiography. Nearly 73% of the procedures in the current cohort were performed using the TRA. As per the classification used in the MATRIX trial, the CADOSA registry would fall in the intermediate volume centers of TRA. We believe that this is probably the best combination where bias from operators experience with either access route is minimal. 22
Stratification of patients according to their age and gender provides a better insight into how one approach compares with the other regarding benefits and challenges. Our study also confirms that TRA should be the access of choice in all ages and genders to benefit from reduced risk bleeding, mortality, and overall NACE.
The present study has several limitations. The patients were not randomly allocated, and hence analyses with propensity score were taken to account the differences in baseline characteristics and the potential selection bias. Despite performing propensity score matching, we cannot exclude the presence of selection bias. It is also possible that some operators preferred TFA for difficult and sicker patients. The impact of large sheath size on access site bleeding and the impact of complex PCI on periprocedural MI was also not assessed in the present study. Furthermore, information on body mass index (BMI) was not present in all the patients to be included as a factor in the propensity matching. We excluded patients with cardiogenic shock, peripheral artery disease, or previous CABG to reduce selection bias. We also did not have complete information on BMI, which could affect TFA site bleeding. 23 Despite these limitations, one of the important points of our study is that all the data were collected very meticulously and prospectively by the medical and research staff by reviewing the patients with prespecified definitions. Furthermore, the CADOSA registry captures every coronary angiogram and PCI in all the teaching hospitals of SA.
In conclusion, we demonstrated that a major reduction in bleeding and mortality was noted with TRA in all the subgroups in our observational study. This study consolidates the benefits of TRA in a real-world population.
Supplemental Material
Supplementary_files - Impact of Young Age and Gender on Outcomes of Transradial Versus Transfemoral Access Coronary Angiography
Supplementary_files for Impact of Young Age and Gender on Outcomes of Transradial Versus Transfemoral Access Coronary Angiography by Kuljit Singh, Rosanna Tavella, Tracy Air, Matthew Worthley, Ajay Sinhal, Margaret Arstall, Christopher Zeitz and John Beltrame in Angiology
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. KS has received speaker fees/education grant/research grants from Terumo Medical, Abbott medical, BioExcel, AstraZeneca, Bristol Myers Squibb and Bayer Australia
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.