
Abstract
We analyzed data from 4 nationwide prospective registries of consecutive patients with acute coronary syndromes (ACS) admitted to the Italian Intensive Cardiac Care Unit network between 2005 and 2014. Out of 26 315 patients with ACS enrolled, 13 073 (49.7%) presented a diagnosis of non-ST elevation (NSTE)-ACS and had creatinine levels available at hospital admission: 1207 (9.2%) had severe chronic kidney disease (CKD) (estimated glomerular filtration rate [eGFR] <30), 3803 (29.1%) mild to moderate CKD (eGFR 31-59), and 8063 (61.7%) no CKD (eGFR > 60 mL/min/1.73 m2). Patients with severe CKD had worse clinical characteristics compared with those with mild-moderate or no kidney dysfunction, including all the key predictors of mortality (P < .0001) which became worse over time (all P < .0001). Over the decade of observation, a significant increase in percutaneous coronary intervention rates was observed in patients without CKD (P for trend = .0001), but not in those with any level of CKD. After corrections for significant mortality predictors, severe CKD (odds ratio, OR: 5.49; 95% CI: 3.24-9.29; P < .0001) and mild-moderate CKD (OR: 2.33; 95% CI: 1.52-3.59; P < .0001) remained strongly associated with higher in-hospital mortality. The clinical characteristics of patients with NSTE-ACS and CKD remain challenging and their mortality rate is still higher compared with patients without CKD.
Keywords
Introduction
Chronic kidney disease (CKD) is a strong independent predictor of mortality in patients with acute coronary syndrome (ACS), especially for those with non-ST elevation ACS (NSTE-ACS). 1 –6 The mechanisms by which renal dysfunction adversely impact clinical outcomes in ACS are multifactorial, but may also be partially explained by differences in medical management. 5 Several studies have demonstrated that, compared with patients with preserved renal function, patients with ACS with CKD are less likely to be treated using an early interventional approach. 1,3
There are very limited data available, particularly from a representative, population-based perspective, to describe contemporary and changing trends in the epidemiology, treatments, and event rates for patients with ACS and concomitant renal dysfunction. 7,8 In the present study, we describe the evolution of in-hospital management and outcome for patients with NSTE-ACS with CKD admitted to Italian intensive cardiac care units (ICCUs) network from 2005 to 2014.
Methods
Four prospective registries in patients with ACS were conducted in Italy between 2005 and 2014 by the Italian Association of Hospital Cardiologists (ANMCO): IN-ACS Outcome (Italian Network on Acute Coronary Syndromes Outcome) in 2005 to 2008 9 ; BLITZ-4 in 2009 to 2010 10 ; MANTRA (Management of patients with ACS in the real world practice in Italy: an outcome research study focused on the use of ANTithRombotic Agents) in 2009 to 2010, 11 and EYESHOT (EmploYEd antithrombotic therapies in patients with acute coronary Syndromes HOspitalized in iTalian cardiac care units) in 2013 to 2014. 12 All surveys were nationwide and included patients with ACS consecutively admitted to the participating ICCUs during a prespecified period (few weeks for the BLITZ-4 and EYESHOT registries and 1 year for IN-ACS Outcome and MANTRA) (Supplemental Table 1).
The methods used for each registry have been described. 9 –12 Briefly, their primary objectives were to assess the clinical characteristics, management, and outcomes of patients with ACS, using a catchment method broad enough to provide data representative of the entire country. Participation in the various registries had been offered to all institutions in BLITZ-4 and EYESHOT and to a representative sample of CCUs (balanced by geographical region and hospital complexity) in IN-ACS Outcome and MANTRA.
Physicians were instructed that participation in the registries should not affect clinical care or management. Informed consent was obtained from all patients who were aware of the nature and aims of the registries. Local Institutional Review Boards were informed of the study according to the Italian rules and approved the protocol.
Data Collection
Data on baseline characteristics, including demographics, risk factors, and medical history were collected, as previously described. 9 –12 Information on the use of cardiac procedures, including coronary angiography, type of revascularization (if any), and in-hospital major clinical events, were recorded.
For the present analysis, we focused on patients with CKD according to estimated glomerular filtration rates (eGFR) calculated from serum creatinine values recorded on admission. The eGFR was calculated using the Cockcroft-Gault equation 13 and the population was divided into 3 groups accordingly: eGFR ≤30 (severe CKD), eGFR ranging from 31 to 59 (mild to moderate CKD), and eGFR ≥60 mL/min/1.73 m2 (no CKD). 8 Among patients with severe CKD, those with end-stage renal disease or on dialysis were included.
The definitions of inclusion criteria and outcome events were consistent throughout the surveys. With the exclusion of patients presenting with chest pain and ST-segment elevation lasting >30 minutes (or new-onset left bundle branch block), all cases with a clinical presentation suggestive of acute myocardial ischemia, with or without acute ischemic changes on the electrocardiogram (ECG) were defined as NSTE-ACS. 14 Reinfarction during initial hospitalization was diagnosed in the presence of new ischemic symptoms and a re-elevation of biochemical myocardial necrosis markers with or without concurrent ECG changes. Major bleeding was classified according to the thrombolysis in myocardial infarction criteria. 15 Stroke was identified as an acute neurologic deficit lasting >24 hours and affecting the ability to perform daily activities with or without confirmation by imaging techniques.
For the assessment of trends in revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass grafting [CABG]), we excluded patients enrolled in the BLITZ-4 registry since in this study only the indication to PCI or CABG, but not the actual revascularization, had been recorded.
All data were collected using a standardized case report form at the participating centers and entered in a central database located at the ANMCO Research Center (Florence, Italy). By using a validation plan integrated in the data entry software, data were checked with data queries for missing or contradictory entries and values out of the normal range. The data were also centrally audited at the coordinating center.
Statistical Analysis
Categorical variables are reported as numbers and percentages and compared by χ2 test, whereas continuous variables are reported as means and standard deviations and compared by t test or analysis of variance, if normally distributed, or by Mann-Whitney U test and Kruskal-Wallis test, if not. Temporal trends were tested using the Cochran-Armitage test for binary variables and the Kendall Tau rank correlation coefficient with the Jonckheere-Terpstra test for continuous variables. A multivariable analysis (logistic regression) was performed to identify the independent predictors of coronary angiography during hospital stay, considering CKD, study cohort, the type of hospital (with cath-lab vs without cath-lab), age (as continuous), diabetes mellitus, peripheral artery disease (PAD), Killip IV, systolic blood pressure (as continuous), heart rate (as continuous), oral anticoagulants, antiplatelets, and positive troponin levels at entry, as covariates. Furthermore, a logistic regression on coronary angiography was performed considering CKD, and the propensity score to CKD as covariates; for each patient, the latter was estimated as the probability of presenting CKD, by a logistic regression, in which the variables mentioned above were inserted. Finally, another multivariable analysis was performed to estimate the risk of in-hospital mortality over time, adjusting for study cohort, atrial fibrillation at entry, coronary angiography, geographic area, and for risk factors and baseline characteristics considered of clinical interest. Also, female sex, age (as continuous), smoking, diabetes mellitus, prior myocardial infarction (MI), prior revascularization (PCI or CABG), prior heart failure (HF), PAD, prior stroke/transient ischemic attack (TIA), prior renal dysfunction, Killip IV class at entry, atrial fibrillation at entry, hemoglobin levels at entry, body mass index, ECG changes, systolic blood pressure at entry (as continuous), heart rate at entry (as continuous), and coronary angiography were considered. When more than 2 categories were present, dummy variables were introduced to define a reference group (ie, year 2005 for study cohort, and north for geographic area). Factors that remained significant at the 0.05 level in the multivariable models comprised the final models. The estimates of the association between predictors and end points are presented as odds ratios (ORs) with 95% CIs. The Wald χ2 for all factors in the models are summed. The percent for each χ2 relative to this total is used as an estimate of the percent of the predictive information (% PI) in the model accounted for by that variable. All tests were 2-sided; a P < .05 was considered significant. All analyses were conducted with SAS system software version 9.4 (SAS Institute Inc).
Results
Patient Characteristics
Out of 26 315 patients with ACS enrolled in the 4 registries, 14 454 (54.9%) were classified as NSTE-ACS and, of these, 13 073 (90.4%) had serum creatinine levels available on admission. Among these patients, 1207 (9.2%) had severe CKD, 3803 (29.1%) mild to moderate CKD, and 8063 (61.7%) no CKD. Significant trends for increasing prevalence were observed for patients with severe CKD and with mild/moderate CKD (all P = .02), whereas the prevalence of patients without CKD remained fairly stable (Supplemental Table 1).
Apart from impaired kidney function, patients with severe CKD had worse clinical characteristics compared with those with mild-moderate kidney dysfunction or preserved function. They were much older and had significantly more risk factors such as diabetes mellitus and hypertension. Patients with severe CKD also presented more often a history of cardiovascular disease, including prior MI, PCI, and CABG, as well as prior cerebrovascular and PAD. The hemodynamic condition on admission was worse in patients with severe CKD with lower systolic blood pressure, higher heart rate, lower ejection fraction (at entry/during hospital stay), and a higher rate of Killip class IV (Table 1).
Baseline Clinical Characteristics and Hemodynamic Variables of Patients With NSTE-ACS With and Without CKD at Admission.
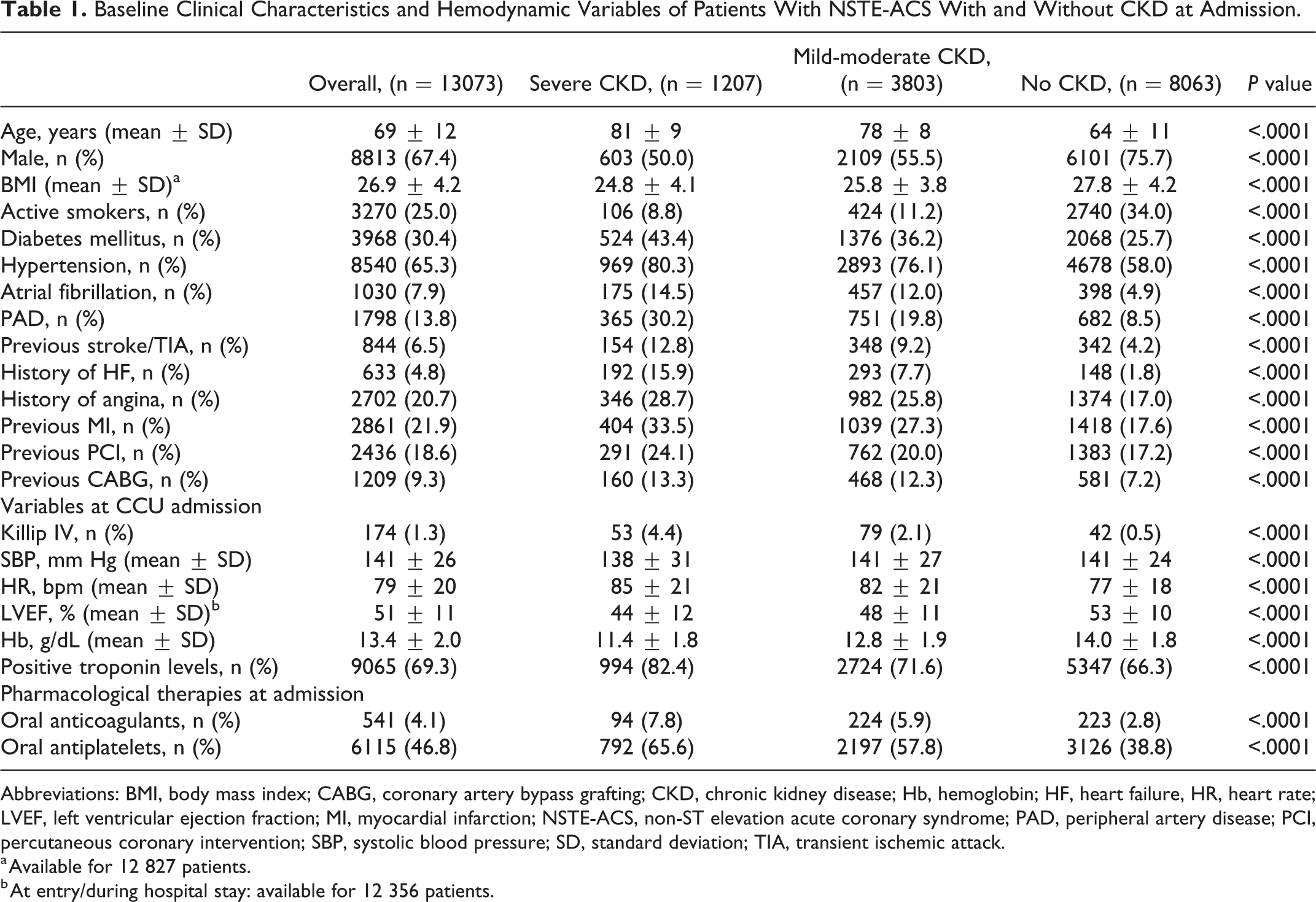
Abbreviations: BMI, body mass index; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; Hb, hemoglobin; HF, heart failure, HR, heart rate; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NSTE-ACS, non-ST elevation acute coronary syndrome; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; SD, standard deviation; TIA, transient ischemic attack.
a Available for 12 827 patients.
b At entry/during hospital stay: available for 12 356 patients.
Clinical Characteristics of Patients With CKD Over Time
Among patients with severe CKD, the rates of patients with diabetes mellitus, PAD, prior HF, MI and revascularization, as well as the rates of Killip class IV on admission, significantly increased during the 10-year period (Supplemental Table 2). A similar worsening trend of clinical characteristics and prior cardiovascular events were observed in patients with mild to moderate CKD (Supplemental Table 2). Among patients without CKD, only the rates of women, history of stroke/TIA, HF, and prior revascularizations increased over time. The prevalence of prior angina significantly decreased for all the 3 groups of patients.
Coronary Angiography and Revascularization
During the 10-year observation period, a coronary angiography was performed, respectively, in 610 (50.5%), 2855 (75.1%), and 7187 (89.1%) patients with severe, mild to moderate and, no CKD (P < .0001). As shown in Figure 1, the rates of coronary angiography remained stable over time in all groups. Admission to a hospital with onsite cath-lab was by far the most powerful independent predictor of undergoing coronary angiography (χ2 1220 out of a total χ2 of 2007; P < .0001; PI: 61%), followed by age ( χ2 221; P < .0001; PI: 11%) and CKD (χ2 157; P < .0001; PI: 8%). At logistic regression using propensity score to CKD as covariates, the presence of any CKD resulted an independent predictor of coronary angiography (OR: 0.52; 95% CI: 0.46-0.58; P < .0001). Among the 10 010 patients with data available, multivessel coronary artery disease (CAD) was found in 72% of patients with severe CKD, 60% of those with mild to moderate CKD, and 48% of those without CKD (P < .0001). The extent of CAD at coronary angiography in the 3 groups is shown in Figure 2.
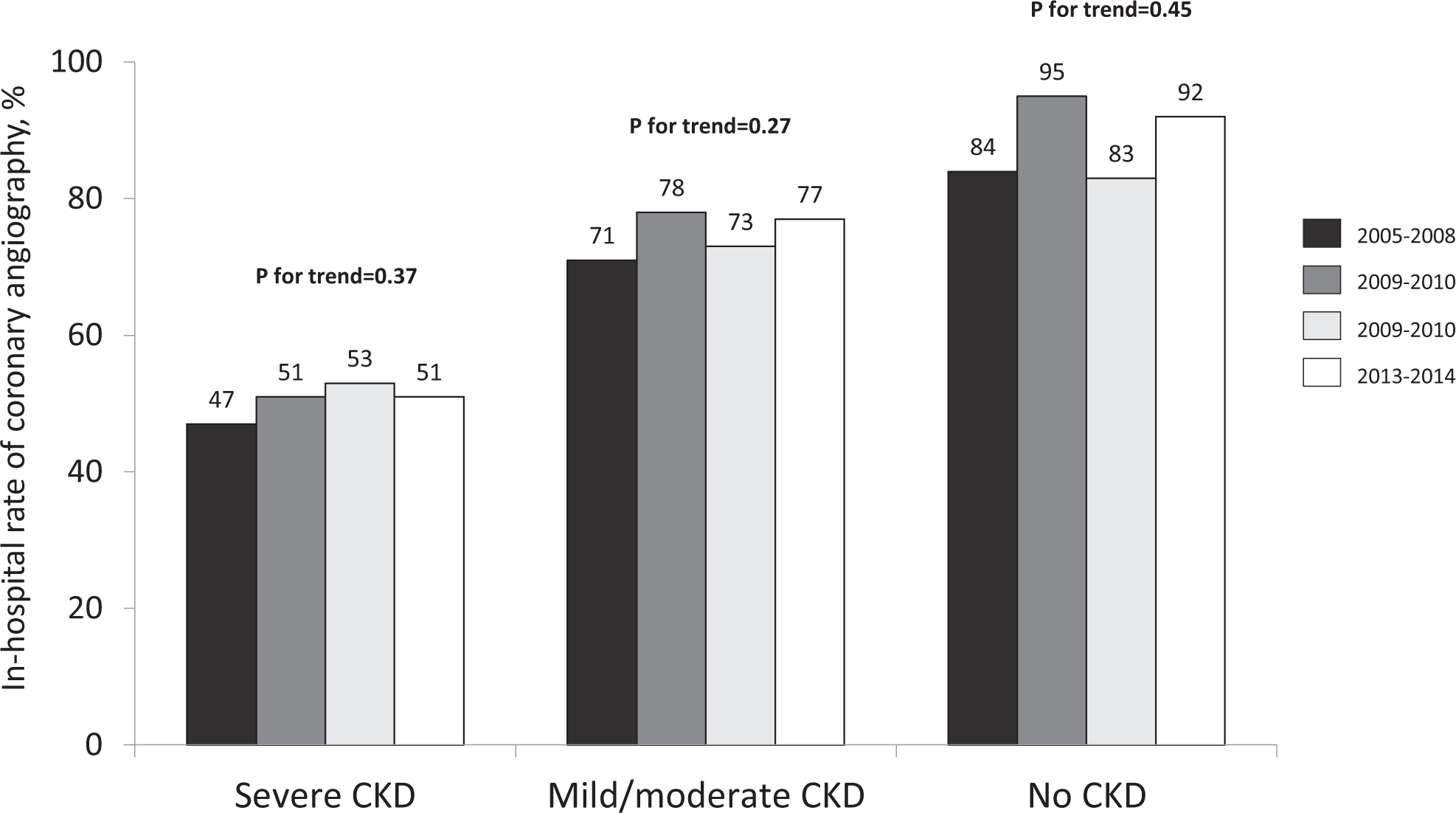
In-hospital rates of coronary angiography over time among patients with non-ST elevation acute coronary syndromes with no-chronic kidney disease (CKD) or with different degrees of CKD.
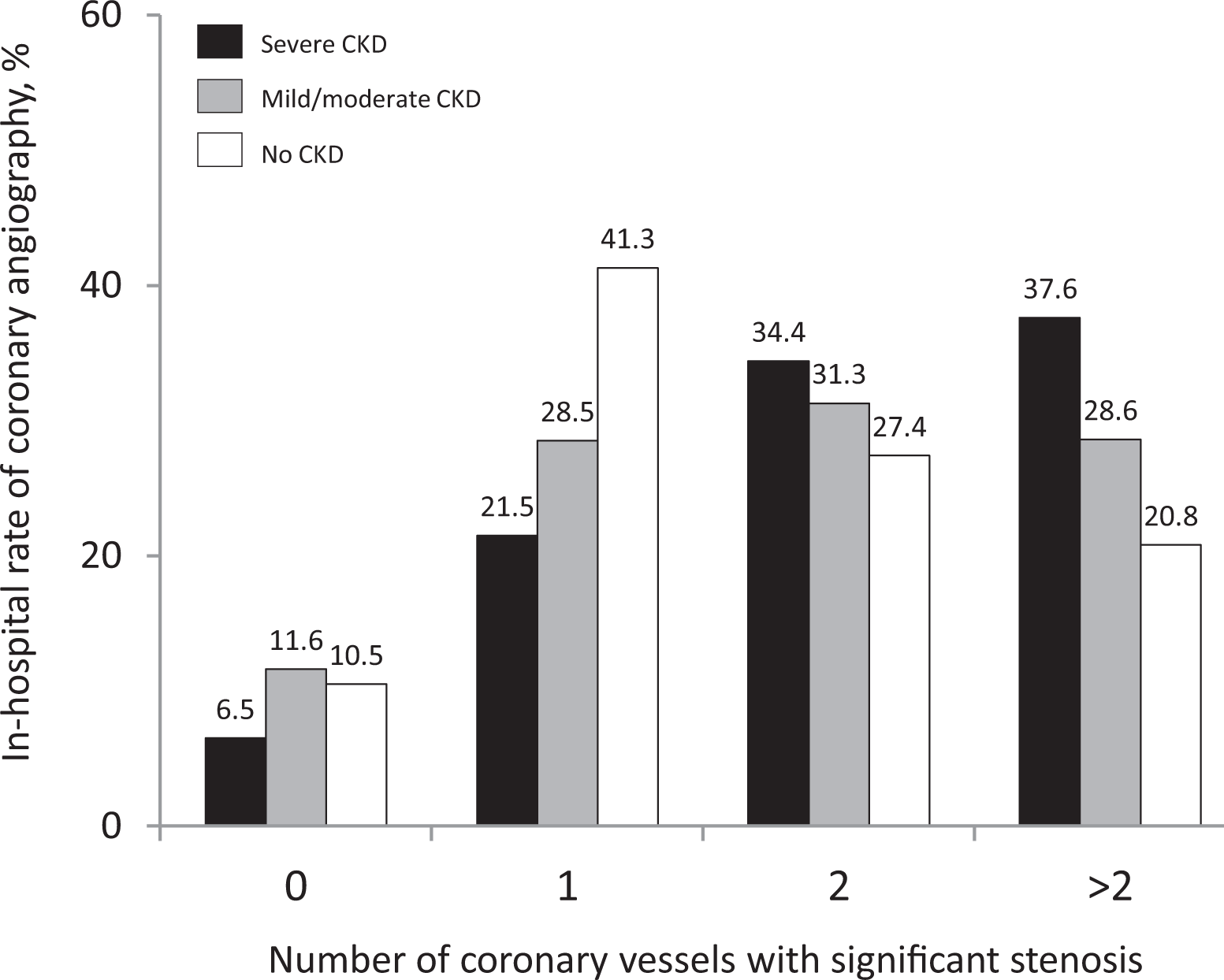
Extent of coronary artery disease at coronary angiography.
Among the 7334 patients with available data on revascularization, 3846 (52%) underwent PCI and 377 (5.1%) CABG. Percutaneous coronary intervention was performed in 201 (32%), 952 (46%), and 2693 (58%) (P < .0001), and CABG in 23 (3.6%), 101 (4.9%), and 253 (5.5%) (P = .12) of patients with severe, mild to moderate, and no CKD, respectively. Over the decade, there was a significant increase in the rate of PCI (P for trend = .0001), with a concomitant decrease in CABG (P for trend = .003), only for patients without CKD (Figure 3).
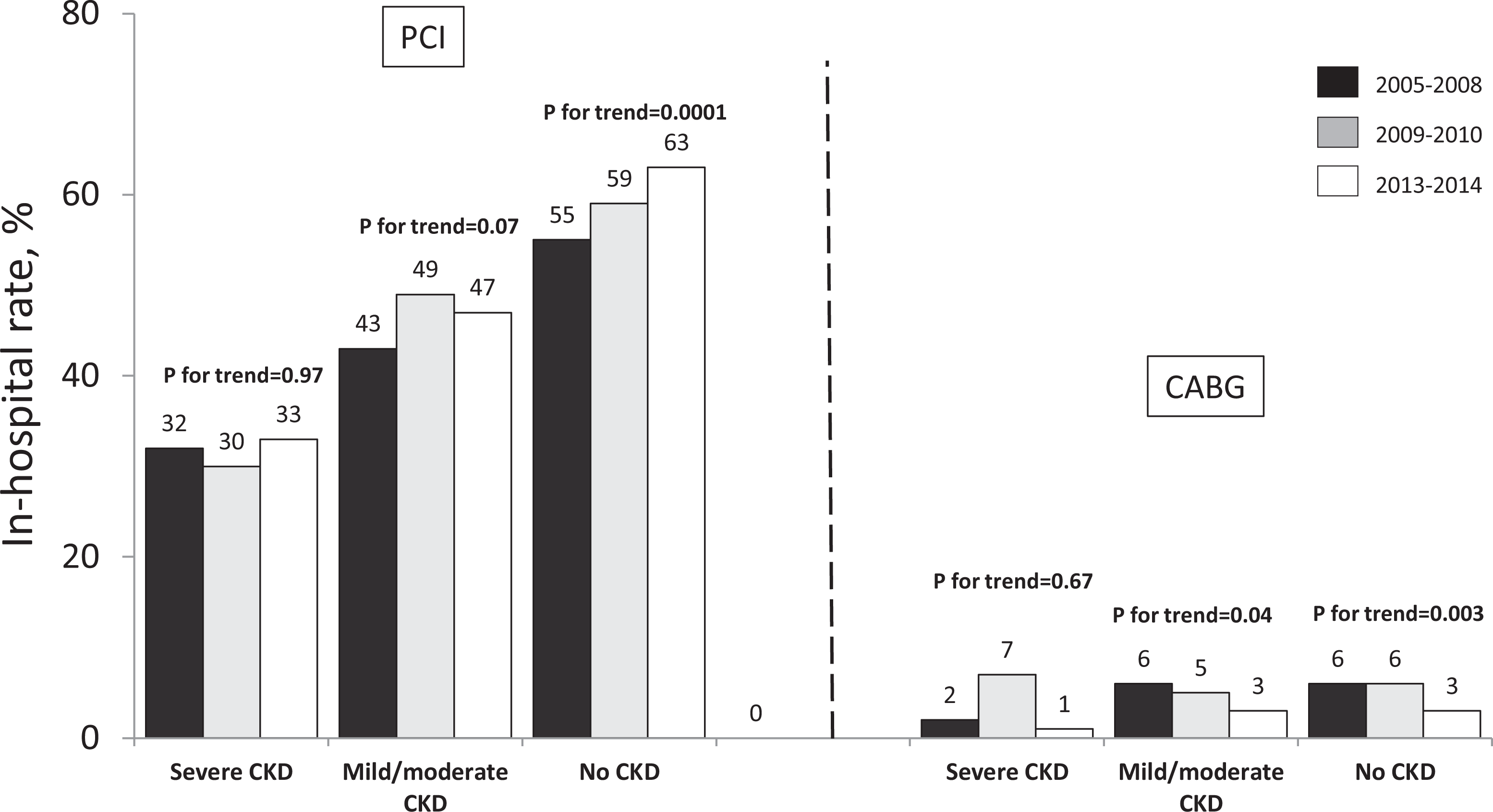
In-hospital rates of myocardial revascularization over time among patients with non-ST elevation acute coronary syndromes with no-chronic kidney disease (CKD) or with different degrees of CKD. CABG indicates coronary artery by-pass grafting; PCI, percutaneous coronary intervention.
In-Hospital Outcomes
Compared with patients without CKD, crude in-hospital mortality rates were almost 10 times and 3 times higher in patients with severe and mild to moderate CKD, respectively, and changed significantly over time, only in patients without CKD (P = .04; Table 2). Nonsignificant trends were observed for reinfarction, stroke, and major bleeding in CKD groups.
In-Hospital Major Clinical Events of NSTE-ACS Patients With and Without CKD at Admission.
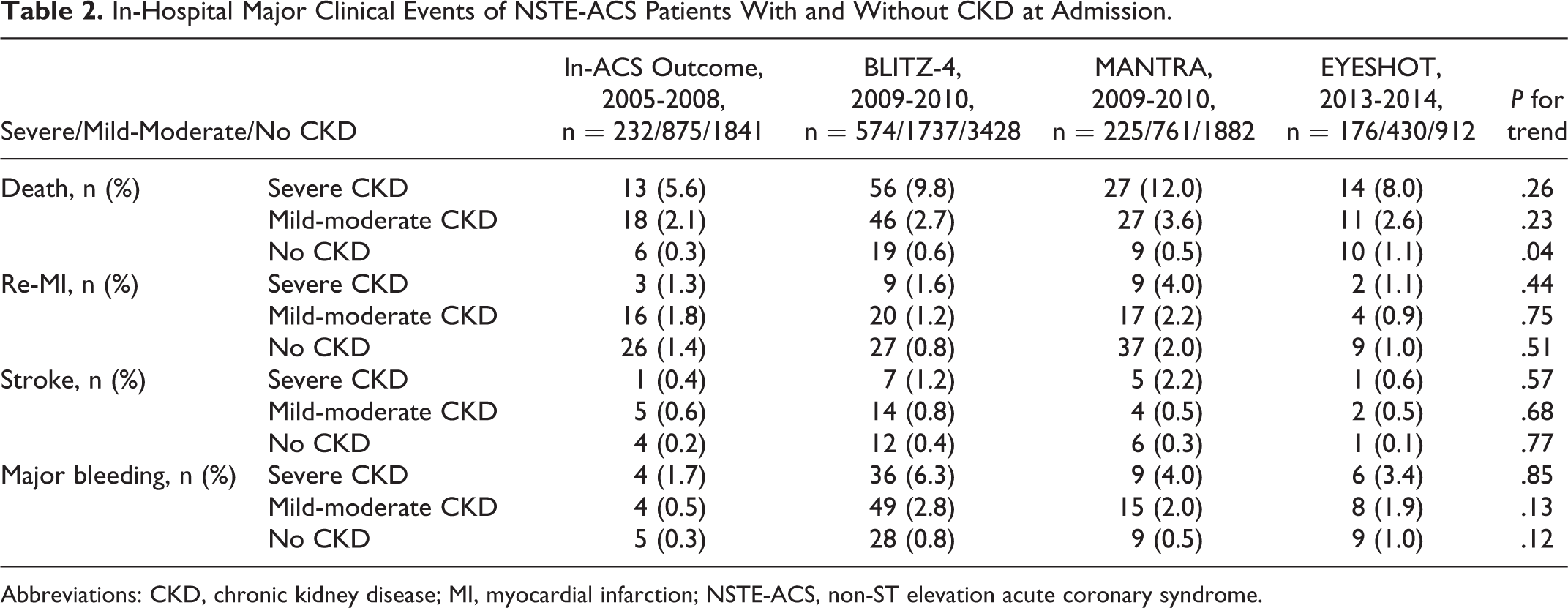
Abbreviations: CKD, chronic kidney disease; MI, myocardial infarction; NSTE-ACS, non-ST elevation acute coronary syndrome.
At multivariable analysis, CKD, either severe (OR 5.49; 95% CI: 3.24-9.29; P < .0001) or mild to moderate CKD (OR 2.33; 95% CI: 1.5-3.59; P < .0001), was among the strongest independent predictors of in-hospital mortality (Figure 4). On the other hand, invasive management (OR 0.34; 95% CI: 0.25-0.45; P < .0001) was associated with reduced in-hospital mortality.
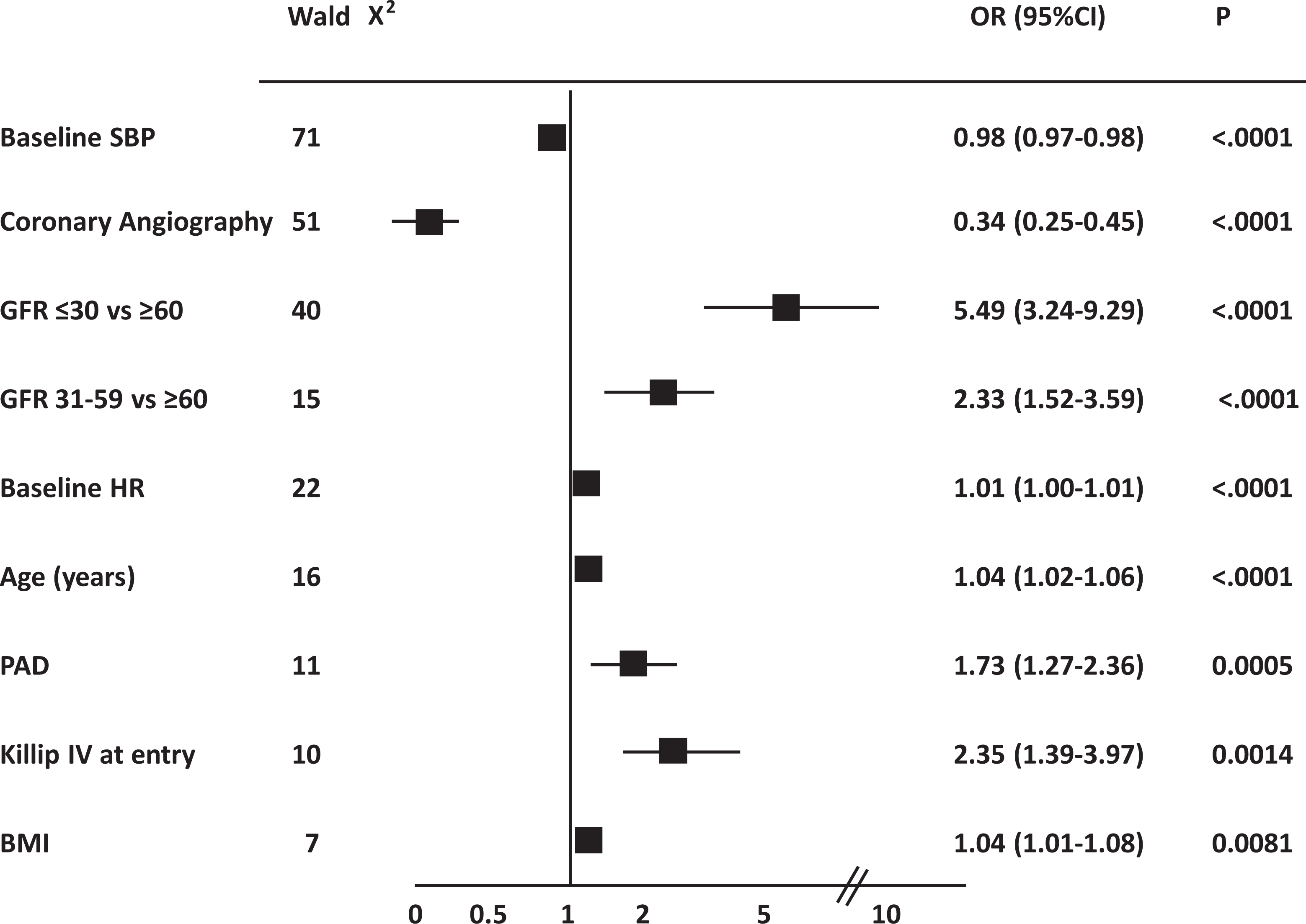
Multivariable logistic regression analysis on in-hospital mortality over time in the overall population with non-ST elevation acute coronary syndromes. CABG indicates coronary artery by-pass grafting; PCI, percutaneous coronary intervention.
Discussion
The main findings of the present analysis of consecutive, nationwide, real-world registries covering a decade of observation are: (1) About 40% of patients with NSTE-ACS admitted to ICCUs have CKD with this rate increasing over time; (2) compared with patients without CKD, those with CKD are much older and have significantly worse clinical characteristics, including all the key predictors of mortality. The prevalence of mortality predictors in the CKD population increased over time; (3) patients with CKD less frequently underwent coronary angiography and PCI compared with those without CKD, and the rate of invasive management did not change over time in patients with CKD; (4) After adjustment for other key mortality predictors, patients with CKD continue to show significantly higher in-hospital mortality risk compared with those with preserved renal function.
Although several studies have analyzed the impact of CKD on outcomes of patients with ACS, 1,3 the present study is the first to assess contemporary and changing trends in the epidemiology and management of these high-risk patients. Our data gathered between 2005 and 2014 must be considered in the time context of the evolution of the Italian ICCU network, which under many aspects is similar in other Western countries. As described in previous papers, 16,17 the “great leap forward” in ACS management in our country happened between 2000 and 2004, with the organization of the STEMI networks and the dramatic increase of early invasive management in NSTE-ACS following the recommendations of international Guidelines based on solid evidence. 18 Therefore, the prevalent approach to NSTE-ACS was early invasive already at the beginning of the decade described in the present paper, though more frequent in the low-risk patients, such as those with preserved renal function. The approach was progressively more conservative as renal function decreased. In the subsequent period, as depicted in the present analysis, whereas the rates of coronary angiography further increased and became almost systematic in patients with preserved renal function, the overall angiography and revascularization rates remained stable in patients with CKD.
Another trend did happen at the same time, with a dramatic worsening of the patient characteristics in the ICCUs, particularly in the CKD population: over the decade, increasing numbers of patients with prior cardiovascular events and multisite vascular involvement joined the NSTE-ACS ICCU population, a trend clearly shown in the present study, and this change was especially striking among patients with CKD. The present data show that key mortality predictors in the NSTE-ACS population, such as diabetes mellitus, PAD, and Killip class IV on admission, which are all typical of CKD, have increased over the decade among patients with CKD with NSTE-ACS. This worsening of the CKD population characteristics was not associated with increased mortality over the decade, but neither with a more aggressive approach toward revascularization which, however, increased progressively in lower risk patients, such as those with preserved renal function.
In ACS, CKD represents a potent and independent risk factor for recurrent ischemic events, sudden and non-sudden cardiac death. Although the mechanisms underlying the poor prognosis of this vulnerable population are not fully understood, it is plausible that the interplay between extensive comorbidities, more severe disease on presentation with ACS, underutilization of known cardioprotective therapies, extensive CAD, contrast-induced acute kidney injury (CI-AKI), more frequent errors in dosing with excess toxicity from conventional therapies, unique pathobiology of CKD, and less aggressive treatment, have a considerable role. 19,20
Several studies have demonstrated that patients with ACS with CKD are more commonly treated conservatively, rather than using an invasive strategy, compared with patients with preserved renal function. 1 –5 Also in our series, patients with CKD, especially those with severe renal dysfunction, underwent coronary angiography and PCI less frequently compared with patients without CKD. Notably, the invasive approach to ACS has steadily increased in Italy over the years and was associated with improved outcomes in most patient categories, irrespective of age and sex, 16,17 cardiogenic shock status, 21 presence of atrial fibrillation, 22 or concomitant vascular disease. 23 Older age, per se, has not precluded invasive management in our ICCU network 16 whereas, as shown in the present paper, CKD did. The most likely reason seems to be the presence of cardiovascular comorbidity, as well as the fear of increased susceptibility to procedural complications following coronary revascularization. We have observed a similar trend among patients with ACS with complicated diabetes, where the progressive increase in invasive treatment was less pronounced compared with the systematic invasive approach observed in patient without diabetes. 24 Notably, the by far most powerful positive predictor of undergoing coronary angiography was admission to a hospital with onsite cath-lab, a finding that supports the recommendation that ICCUs should work within a hospital network, linking fully equipped medical centers with smaller hospitals with more limited capabilities. 25
The present study has limitations. First, previous serum creatinine levels were not available and therefore some patients may have presented with acute rather than chronic renal failure. Second, all the equations that are used for GFR estimation (including the Cockroft-Gault formula) are based on serum creatinine levels and may overestimate the measured GFR. Nevertheless, creatinine-based estimated GFR is still the most common mode for renal function assessment in clinical practice, especially in complex populations 26 in whom, a dose-adjustment of antithrombotic drugs based on the Cockroft-Gault formula is preferable. Additionally, data from large nationwide registry found that the Cockcroft-Gault formula is better than other equations in predicting mortality after myocardial infarction. 27 However, it is unlikely that using different estimates would lead to different patient classification among classes of renal dysfunction. Third, the pharmacological treatment used during the hospitalization has not been collected in detail in all studies and therefore not considered in the present analysis. Fourth, our database did not include data regarding medication and procedural side effects or complications such as the incidence of CI-AKI. In addition, since no follow-up was available for all the registries, we could not assess how changes in in-hospital treatment affected long-term outcomes.
Conclusions
Non-ST elevation ACS is associated with a wide spectrum of risk. Patients with CKD, particularly those with severe dysfunction, have a high and increasing burden of cardiovascular comorbidities. At a national level, an early invasive approach to NSTE-ACS has been implemented in lower risk patients and has led to an overall improvement in outcome, but high-risk patients, such as those with severe CKD, remain undertreated and have not improved their outcome so far. The need for cardiac intensive care for patients with severe renal dysfunction is becoming increasingly important in most advanced health care systems and still faces a high mortality rate. 28 To improve outcomes for these patients will require a higher level of clinical competence in the ICCU system 25,29 and convincing data from dedicated trials which have been lacking so far. 5
Supplemental Material
Supplement_material_PDF - Temporal Trends in Invasive Management and In-Hospital Mortality of Patients With Non-ST Elevation Acute Coronary Syndromes and Chronic Kidney Disease
Supplement_material_PDF for Temporal Trends in Invasive Management and In-Hospital Mortality of Patients With Non-ST Elevation Acute Coronary Syndromes and Chronic Kidney Disease by Leonardo De Luca, Giuseppe Di Pasquale, Lucio Gonzini, Massimo Uguccioni, Zoran Olivari, Gianni Casella, Alessandro Boccanelli, Stefano De Servi, Stefano Urbinati, Furio Colivicchi, Domenico Gabrielli and Stefano Savonitto in Angiology
Footnotes
Authors’ Note
All authors substantial contributed to: (1) conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The studies included in this manuscript were funded, by unrestricted grants, as follows: IN-ACS Outcome (Sanofi-Aventis and Bristol-Myers Squibb, Italy), BLITZ-4 (Merck, Sharp & Dohme, Italy), MANTRA (GlaxoSmithKline, Italy), and EYESHOT (AstraZeneca, Italy). The sponsor of the studies was the Heart Care Foundation, a nonprofit independent institution which is also the owner of the databases. Database management and quality control of the data were under the responsibility of the Research Centre of the Italian Association of Hospital Cardiologists (ANMCO). The Steering Committees of the studies had full access to all of the data in the studies and took complete responsibility for the integrity of the data and the accuracy of data analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.