
Abstract
We assessed sex-related differences in the association of pericardial fat volume (PFV) and obesity measured by body mass index (BMI) with coronary atherosclerotic markers (coronary artery calcium score [CAC], coronary luminal stenosis severity, and coronary plaque) in young patients. Patients (n = 174; age <50 years) with suspected coronary artery disease who underwent 64-slice multidetector computed tomography angiography were enrolled. Females tended to have a younger age and increased BMI, normal coronary arteries (free from luminal stenosis), and increased percentage of absent coronary plaque compared with males. There was a significant independent association between PFV with coronary luminal stenosis and between PFV and BMI with coronary noncalcified plaque presence after adjustment for conventional cardiac risk factors. On the other hand, males showed a more increment in PFV, CAC, percentage of calcified plaque, and percentage of significant coronary luminal stenosis compared with females. There was a significant independent association of PFV with CAC, significant coronary stenosis, and calcified plaque presence, while no association was observed between BMI with coronary markers in young males. In conclusion, PFV, but not BMI, showed a significant independent association with advanced coronary atherosclerosis in young male patients.
Introduction
There is has been an increased prevalence of coronary artery disease (CAD) among young age-group. 1,2 Acute coronary syndrome prevalence rates have increased among young adults age 35 to 54 years, particularly in females. 2
Coronary artery disease initiates at a very early stage in life as a rapidly progressive process of atherosclerosis and carries a poor long-term prognosis in most studies. 1 –4 Therefore, the early identification of coronary atherosclerosis presence in the young is of paramount importance. A significant sex difference in risk factor profiles, morbidity, and mortality from CAD among the young have been reported in previous studies. 4,5 Females have different risk factors profile and are less likely to be investigated and receive primary prevention or intervention in the setting of coronary atherosclerosis and its related complications. 4,5
Several studies have reported that due to direct effects, local body fat accumulation, including pericardial fat, may affect the development of coronary atherosclerosis and adverse outcomes more than increased general adiposity measured by body mass index (BMI). 6 –8 Indeed, pericardial fat volume (PFV) is reported to be associated with coronary atherosclerosis progression and unfavorable cardiovascular (CV) prognosis independent of other risk factors and beyond general body adiposity. 6 –9 Although the distribution of PFV in males and females has been assessed, 8 investigation of sex disparity in pericardial fat deposition and its impact on the relationship of PFV with different coronary atherosclerotic markers relative to general adiposity measured by BMI in the young is largely unexplored in the literature.
The main aim of the present study was to assess the sex-related differences in the association of PFV and obesity (measured by BMI) with coronary atherosclerotic markers (coronary artery calcium score [CAC], coronary luminal stenosis severity, and coronary plaque) in young symptomatic patients (<50 years) with suspected CAD assessed by multidetector computed tomography (MDCT) angiography.
Patients and Methods
This was a retrospective study conducted at the Cardiology Center at Al-Sader Teaching Hospital, Najaf, Iraq, between January 2013 and December 2018.
The inclusion criteria were (1) patients with stable chest pain with intermediate pretest probability of CAD referred for MDCT examination to exclude occlusive CAD, (2) complete clinical and MDCT interpretation data, and, (3) age <50 years. Exclusion criteria were age ≥50 years or incomplete clinical data.
Among 496 Iraqi patients with stable chest pain and suspected CAD who underwent 64-slice MDCT angiography to exclude occlusive CAD, 174 patients (age <50 years) were eligible to participate in the present study.
A history of conventional cardiac risk factors for CAD was obtained from each patient at the time of coronary MDCT including a positive family history of premature CAD (occurring before the age of 55 years in men and before 65 years in women), current smoking history (>10 cigarettes/day in the past year), diabetes mellitus defined as fasting blood glucose of ≥126 mg/dL or glycated hemoglobin ≥6.5% or the use of diabetes lowering drugs or insulin, dyslipidemia (defined as fasting levels of total cholesterol ≥200 mg/dL or triglyceride ≥150 mg/dL) or use of lipid-lowering medications and measurement of body weight and height to calculate BMI. Body mass index calculated as weight (kg)/height (m2) . 6
Informed verbal consent was obtained from all patients enrolled in the study. The study was approved by our medical college.
Multidetector Computed Tomography Scan Protocol
Computed tomography coronary angiography was performed with a 64-slice scanner (Aquilon 64, v. 4.51 ER 010; Toshiba Medical Systems). Pericardial fat volume was defined as any fat tissue located within the pericardial sac and measured 3-dimensionally in the contrast-enhanced phase. The layer of the pericardium was manually traced, and a 3-dimensional image of the heart was constructed. Then, the PFV was quantified by calculating the total volume of the tissue whose CT density ranged from −250 to −20 HU within the pericardium by using a 3-dimensional workstation statistical analysis. For coronary CT analysis, a plaque was defined as a structure of >1 mm within and/or adjacent to the vessel lumen. Plaques were classified into calcified (plaque consisting of only calcium), noncalcified plaque (plaque that was free of calcium). 6
The severity of coronary artery stenosis was visually graded as normal (normally appearing lumen), nonsignificant with a mean lumen diameter reduction of <50%) and significant with a mean lumen diameter reduction of ≥50% in a single vessel by comparing the lumen diameter of the narrowest segment with that of a more proximal or distal normal segment in 2 orthogonal projections. The CAC score was assessed as per our previous study. 6
The analyses of MDCT images were performed by 2 independent radiologists with >5 years’ experience in coronary MDCT angiography data interpretation.
Statistical Analysis
Data were presented as mean ± standard deviation or as numbers with percentages, as appropriate. Pericardial fat volume and CAC score values were non-normally distributed and presented as median (interquartile range [IQR]). The independent t test or nonparametric test (Mann-Whitney U test) was used to assess the relationships of PFV and BMI with coronary stenosis and plaque presence, as appropriate. The association between PFV and BMI with CAC was assessed by using Spearman rank correlation for nonparametric data. Binary logistic regression analysis was used to analyze the association of coronary atherosclerotic markers with PFV, BMI, age, hypertension, smoking, diabetes mellitus, dyslipidemia, and family history of premature CAD. For the purpose of binary regression analysis, CAC was classified into 2 groups as the CAC = 0 group and CAC >0 group. Also, coronary stenosis severity was categorized into 2 groups as normal nonsignificant stenosis (<50%) group and significant stenosis (≥50%) group. Odds ratios and CIs were calculated for each variable of the regression analysis. A P < .05 was considered significant. SPSS ver. 13.0 (SPSS Inc) was used for statistical analysis.
Results
A total of 174 young age patients (mean age: 42.8 ± 6 years, 49.5% males) with stable chest pain of suspected CAD were enrolled in the study. The median (IQR) PFV was 83.6 cm3 (43-125) and CAC score was 0 (0-6) in the total study sample. Patients’ characteristics are shown in Table 1.
Patient Characteristics.
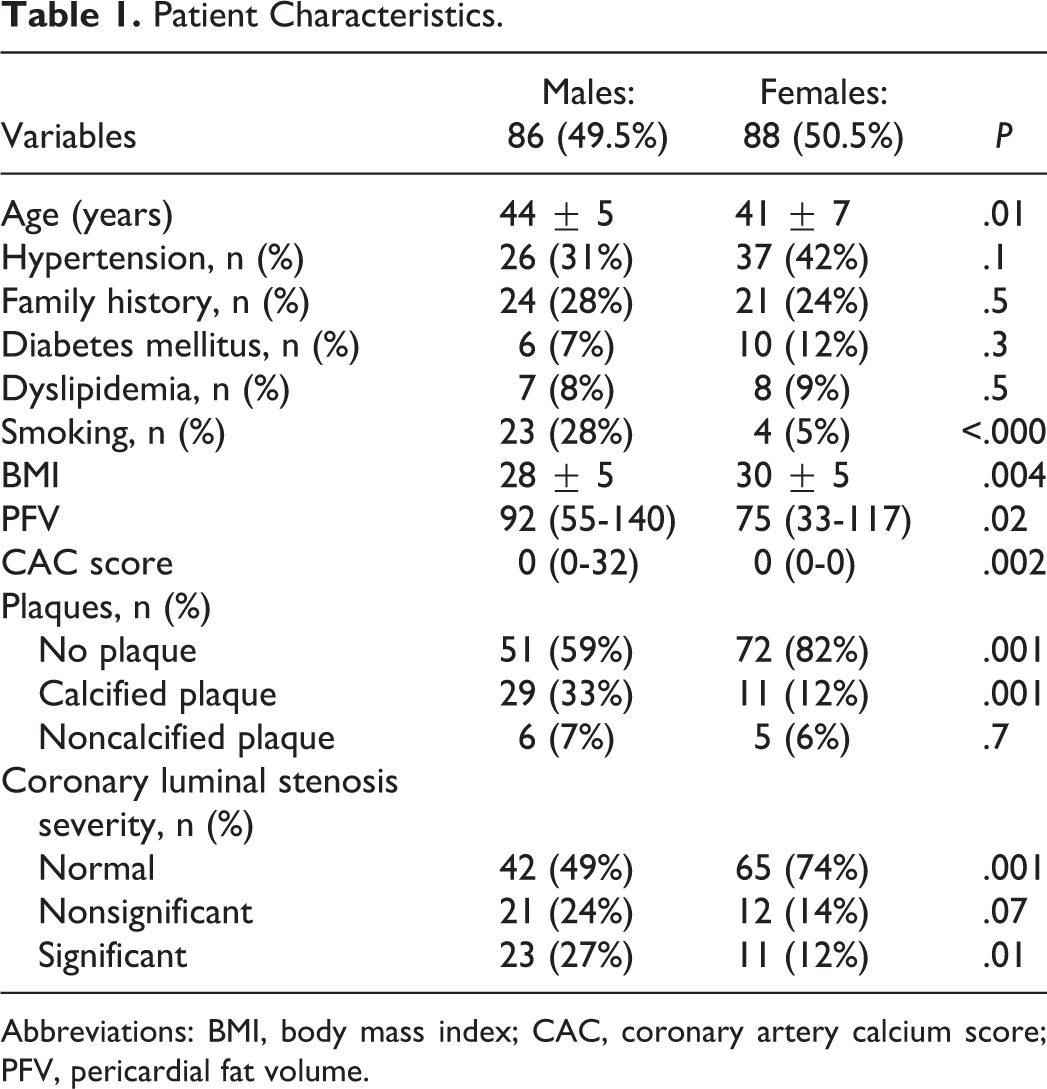
Abbreviations: BMI, body mass index; CAC, coronary artery calcium score; PFV, pericardial fat volume.
Females
Females tended to have increased BMI, normal coronary arteries (free from luminal stenosis) and increased percentage of absent coronary plaque compared with males (Table 1).
Pericardial fat volume showed a significant association with coronary luminal stenosis and noncalcified plaque presence, while there was no significant association between PFV with CAC (Table 2).
PFV Versus BMI Association With Coronary Atherosclerotic Markers.
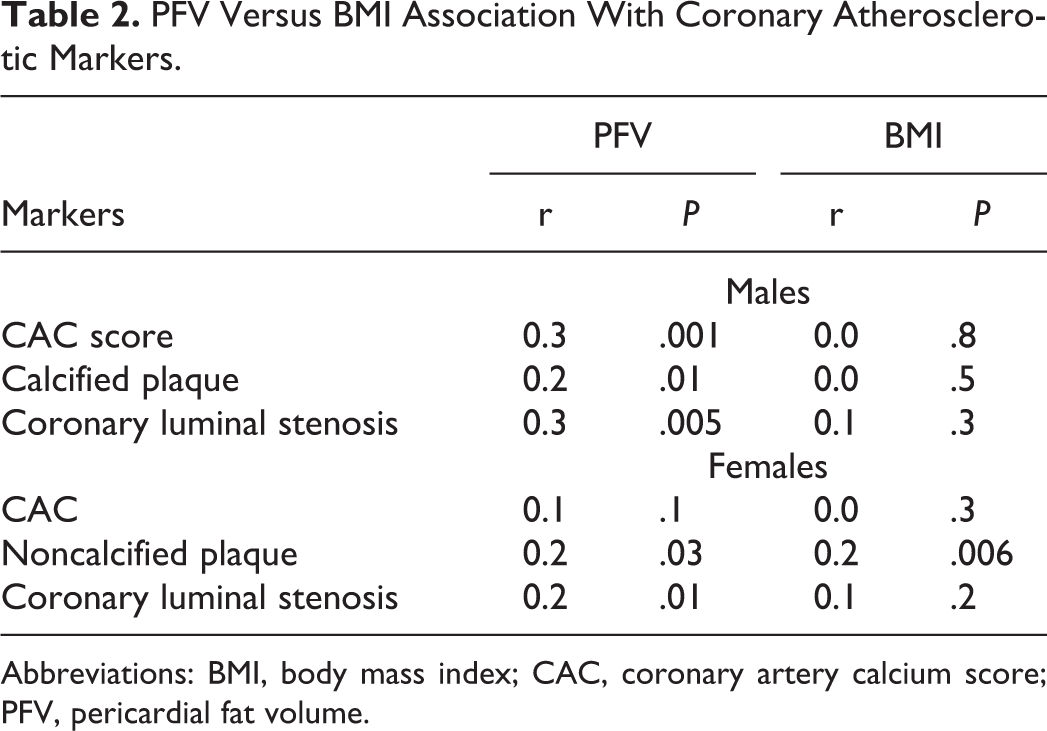
Abbreviations: BMI, body mass index; CAC, coronary artery calcium score; PFV, pericardial fat volume.
On the other hand, BMI showed a significant association with coronary noncalcified plaque presence, while there was no significant association between BMI with CAC score and coronary luminal stenosis (Table 2).
After adjustment for conventional cardiac risk factors, the association of PFV with coronary luminal stenosis and the association of BMI with coronary noncalcified plaque presence persisted (Table 3).
Regression Analysis.
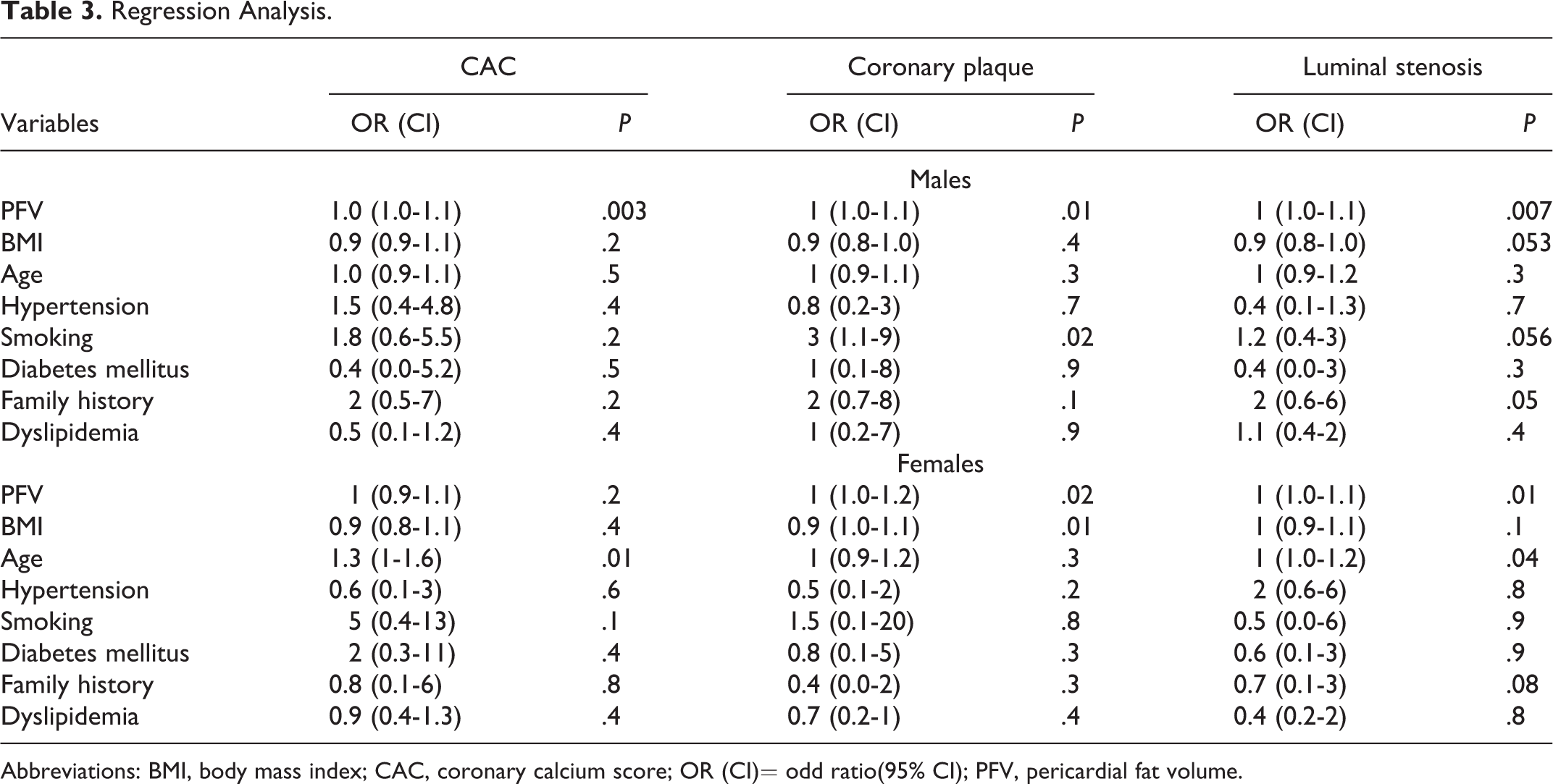
Abbreviations: BMI, body mass index; CAC, coronary calcium score; OR (CI)= odd ratio(95% CI); PFV, pericardial fat volume.
Males
The prevalence of smoking was greater in males than in females. Males showed a significant increment in PFV, CAC score, percentage of calcified plaque, and significant coronary luminal stenosis compared with females (Table 1).
Pericardial fat volume showed a significant association with coronary atherosclerotic markers (CAC score, calcified plaque, and luminal stenosis; P < .05), while BMI showed no significant association with any of these coronary atherosclerotic markers (P > .05; Table 2).
The association of PFV with CAC score, significant coronary stenosis and calcified plaque presence persisted (P < .05) even after adjustment for conventional cardiac risk factors (Table 3).
Discussion
There is evidence that overall adiposity measured by BMI has a significant limitation as an anthropometric marker to assess metabolic and CV risk because BMI does not provide information on body fat distribution, such as visceral and subcutaneous fat. 6 –10
On the other hand, fat in the pericardial sac, owing to its proximity to the myocardium and coronary vasculature with no barriers, has been reported to play an important role in the pathogenesis and progression of coronary atherosclerosis through local paracrine and endocrine release of different substances. 6 –10,11
In the literature, pericardial fat assessed by echocardiography, MDCT, and cardiac magnetic resonance imaging showed a significant association with coronary atherosclerosis, heart failure, atrial fibrillation, and metabolic syndrome. 11
Moreover, the assessment of PFV may allow better CV and metabolic risk stratification independent of BMI and beyond conventional cardiac risk factors. 11,12
Regarding sex-related differences in coronary atherosclerosis in the young, necropsy studies have shown that coronary atherosclerosis appears to start in asymptomatic individuals at a very early stage of life and some of these individuals later develop CAD as a result of plaque rupture. 13 Supporting this notion is that postmortem examination of coronaries of young American soldiers killed in the Korean and Vietnam wars reported atherosclerosis in 77% and 45% of autopsies, respectively. 13
Significant sex-related differences in coronary atherosclerosis incidence, presentation and prognosis have been reported, whereby females have a less favorable risk factor profile, rates of CAD events and revascularization, and higher mortality than males. 4
Similar to sex-related differences in CV disorders, there is a sex-specific deposition of fatty tissue. Males have more visceral fatty tissue and pericardial fat deposition than females, and this sexual dimorphism in visceral fatty deposition between males and females may be due to differences beyond the levels in sex hormones. 10,14
The relationship of pericardial fat and BMI with coronary atherosclerotic markers in the young was ambiguous and conflicting among previous clinical studies. 10,15 –17
Previous studies of obesity measured by BMI in young adults demonstrated positive associations between increased BMI and coronary atherosclerosis extent and progression. 10 –15
In disagreement with our result, the Cardiovascular Risk in Young Finns Study (557 patients assessed from 1980 to 2007) showed no significant independent association between increased cardiac fat and increased CAC. 16 In contrast, to the Cardiovascular Risk in Young Finns Study and in agreement with our result, young girls with Cushing syndrome showed a pronounced association between cardiac fat and markers of early coronary atherosclerosis and premature CV dysfunction, including carotid intimal media thickness. 17
Also, the association of pericardial fat with CAC has been confirmed by a study conducted by Mahabadi et al. 7 They showed that pericardial fat was associated with CAC progression in young persons (45-55 years of age) independent of BMI and other conventional cardiac risk factors. The authors suggested that increased pericardial fat deposition could promote atherosclerosis development at early stages. 17
In the present study, the significant association of PFV with noncalcified plaques, rather than calcified plaques, in females compared with males is interesting as noncalcified and nonobstructive plaques may be more prone to rapid progression and erosion. 2
In prior studies of symptomatic middle to older-aged adults undergoing MDCT examination, the presence of nonobstructive, noncalcified high-risk plaques were correlated with an increased risk of long-term mortality. 2 On the other hand, coronary calcified plaque might represent a late manifestation of atherosclerosis process which could be associated with less aggressive behavior compared with noncalcified plaque. 18
Although females may have less extensive coronary atherosclerosis than males, coronary plaques in females have less necrotic core volume, dense calcium volume, and fibrous and fibro-fatty tissue compared with males. 19 These high-risk plaque characteristics in females may be associated with a higher rate of plaque erosion and progressive coronary atherosclerosis in the postmenopausal period, independent of other comorbidities conventional cardiac risk factors. 19 Thus, females may develop symptoms even with smaller plaque burden or thrombus load. 20,21
It has been reported that increasing cardiac fat deposition, measured by volumetric analysis rather than linear thickness assessment, is significantly associated with the presence of high-risk plaque features in a systematic review and meta-analysis of 9 studies. This association may be mediated via cellular cross-talk which may lead to the development of plaque characteristics considered to be “high risk” given their association with major adverse coronary events. 22
The significant association of PFV with calcified plaque and CAC in males versus a significant association of PFV with noncalcified plaque in females in the present study, suggests a sexual dimorphism of PFV influence on coronary atherosclerosis. Thus, PFV may be associated with more advanced and stabilized coronary atherosclerosis in young males compared with young females. 4
The present study has several limitations. It was a single-center study and did not include long-term follow-up. A causal relationship between atherosclerotic markers with PFV and BMI cannot be established because of the cross-sectional nature of the study. Because of some limitations in statistical analysis and low coefficient r value, the results need to be interpreted with caution. However, the findings of the present study may provide new insight, which could be used in prospective studies to establish a prognostic role of PFV in the young. This would facilitate better risk stratification of coronary atherosclerosis burden.
Conclusion
Pericardial fat volume, but not BMI, showed a significant independent association with advanced coronary atherosclerosis in young male patients. Pericardial fat volume and BMI showed a significant independent association with the noncalcified plaque in young female patients. These findings suggest that PFV is significantly associated with advanced but stable and late phase of coronary atherosclerosis in young males with suspected CAD. While in young females, PFV was associated with the early phase of atherosclerosis which is vulnerable for acute coronary events.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Acknowledgments
The author acknowledges Dr Hasan Alnafakh for his valuable contribution to the analysis of MDCT images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.