
Abstract
Fabry disease is a rare X-linked lysosomal disorder. Alpha-galactosidase A deficiency caused by mutation leads to accumulation of glycosphingolipids predominantly in endothelial cells, leading to impairment of vascular wall morphology and function. We assessed vascular wall hypertrophy (carotid artery intima-media thickness, cIMT), endothelial function (brachial artery flow-mediated dilation, FMD), presence of atherosclerotic plaques in the carotid and femoral arteries, and levels of endothelial adhesion and inflammatory biomarkers in 33 Fabry patients compared with 66 healthy matched controls. Fabry patients had thicker cIMT (0.07 ± 0.02 vs 0.06 ± 0.02 cm; P = .021), as well as dilated common carotid arteries (0.80 ± 0.12 vs 0.70 ± 0.06 cm; P < .001), and aortic annulus than controls (3.07 ± 0.48 vs 2.7 ± 0.48 cm; P = .001). Flow-mediated dilation was reduced (4.48 ± 8.80 vs 10.67 ± 8.72%; P = .001) and atherosclerotic plaques were less present in Fabry patients (9.10% vs 43.94%; P < .001). Vascular cell adhesion molecule-1, interleukin-6, tumor necrosis factor α, and high-sensitivity CRP were significantly higher and E-selectin lower in Fabry patients. Our results suggest that a complex vascular phenotype is present in Fabry patients. This represents a challenge for further research that could have important clinical applications.
Introduction
Fabry disease (FD) (OMIM # 301500), also known as Anderson-Fabry disease, is a panethnic X-linked lysosomal storage disorder with frequencies of the classic and later-onset phenotypes of up to 1 in 22 570 males and 1 in 1390 males, respectively. 1 The underlying cause of this disease is a mutation of the alpha-galactosidase A (α-Gal A, EC 3.2.1.22) gene (GLA) at Xq22. 2 –4 The gene defect results in absent or very low activity of the lysosomal enzyme α-Gal A that leads to a widespread accumulation of globotriaosylceramide (Gb3) and its deacylated derivate globotriaosylsphingosine (lyso Gb3) in arterial walls, primarily in endothelial and smooth muscle cells. 2
Patients with FD show a wide clinical spectrum, and the clinical findings are influenced by the specific GLA mutation and gender of a patient. Hemizygous males typically experience the most severe manifestations of FD. Heterozygous females exhibit heterogeneous disease expression which ranges from asymptomatic to severe, depending on random X-chromosomal inactivation, and typically present with symptoms later in life compared with males. 1 The most common presenting features in patients with classic FD are burning pain in extremities, hypo- or hyperhidrosis, gastrointestinal disorders, angiokeratoma, and significant renal (proteinuria and kidney failure), cardiac (hypertrophic cardiomyopathy and arrhythmia), and cerebrovascular (transient ischemic attacks, strokes) disease. 2 Patients with atypical (ie, later-onset) FD and residual enzyme activity have a milder phenotype and show symptoms which are limited to one or a few organs without any symptoms in childhood. 5,6
The underlying pathophysiological mechanisms of FD are still not well understood. Current evidence suggests that accumulation of glycosphingolipids represents an initial insult that triggers a cascade of secondary processes such as inflammation, oxidative stress, and altered immune response that play an important role in the development of the clinical phenotype. 7 Vascular involvement is evident and early changes are thought to predominantly involve small vessels but also large arteries. 8 Due to a variety of mechanisms for FD vasculopathy, structural and functional changes in various organs leads to infarction and ischemia. 3 Life-threatening multisystem conditions such as ischemic complications of the kidney, heart, and brain shortens the life expectancy of untreated males and females with FD by approximately 16.5 and 4.6 years, respectively. 9 Cardiovascular disease is the most common cause of death among both genders. 9 –11 Enzyme replacement therapy (ERT) can remove stored Gb3 in endothelial cells 12 and slow or halt the progression of cardiac and renal disease, 13 but not all patients with FD benefit from ERT. Patients with FD have the most benefit when ERT starts early, before major organ damage develops. 14
Fabry disease manifestation takes a slow but progressive course and efforts should be made to reduce late diagnoses and to improve our understanding of FD vasculopathy through identification of additional risk and predictive factors for progression. Accordingly, the aim of our study was to investigate the extent and associations among vascular wall hypertophy (carotid intima-media thickness, cIMT), endothelial function (brachial artery flow-mediated dilation, FMD), and atherosclerosis (plaques in carotid and femoral arteries) in a Slovene cohort of patients with FD compared with healthy age- and sex-matched controls. In addition, endothelial adhesion and inflammatory molecules were assessed.
Patients and Methods
Study Population
We recruited 33 Slovene patients (13 males and 20 females) older than 18 years of age with genetically and enzymatically confirmed classical forms of FD and 66 healthy controls (26 men and 40 women). The demographic characteristics of both populations are summarized in Table 1. The study patients were matched for age, sex, body mass index (BMI), and smoking status. All participants were administered a standardized questionnaire that provided information about demographic background, medical history, occupation, drug use, and personal habits such as cigarette smoking. In male patients, FD was confirmed on the basis of low residual α-Gal A activity in leukocytes and genetic analysis. In females, the diagnosis of FD was confirmed by genetic analysis. The classic form of FD was defined according to the literature. 15 Patients had the following mutations in the GLA gene (number of patients): N272S (13), R363P (5), R227X (3), I270M (2), R342Q (2), Glu358del (2), Glu87_Asp92del (2), R49P (2), IVS5+2T>C (1), and M42R (1). 21 patients were using angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) (63.6%), 9 (27.3%) of them were using statins, and 12 (36.4%) were on antithrombotic medication; 3 patients had end-stage renal disease. Nineteen (57.6%) of patients with FD (all 13 males and 6 females) were receiving ERT. The study protocol was approved by the National Medical Ethics Committee of Slovenia (No. 27/05/11), and informed consent was obtained from all participants.
Baseline Clinical Characteristics of the Study Population and Conventional Risk Factor Exposure for Vascular Disease.
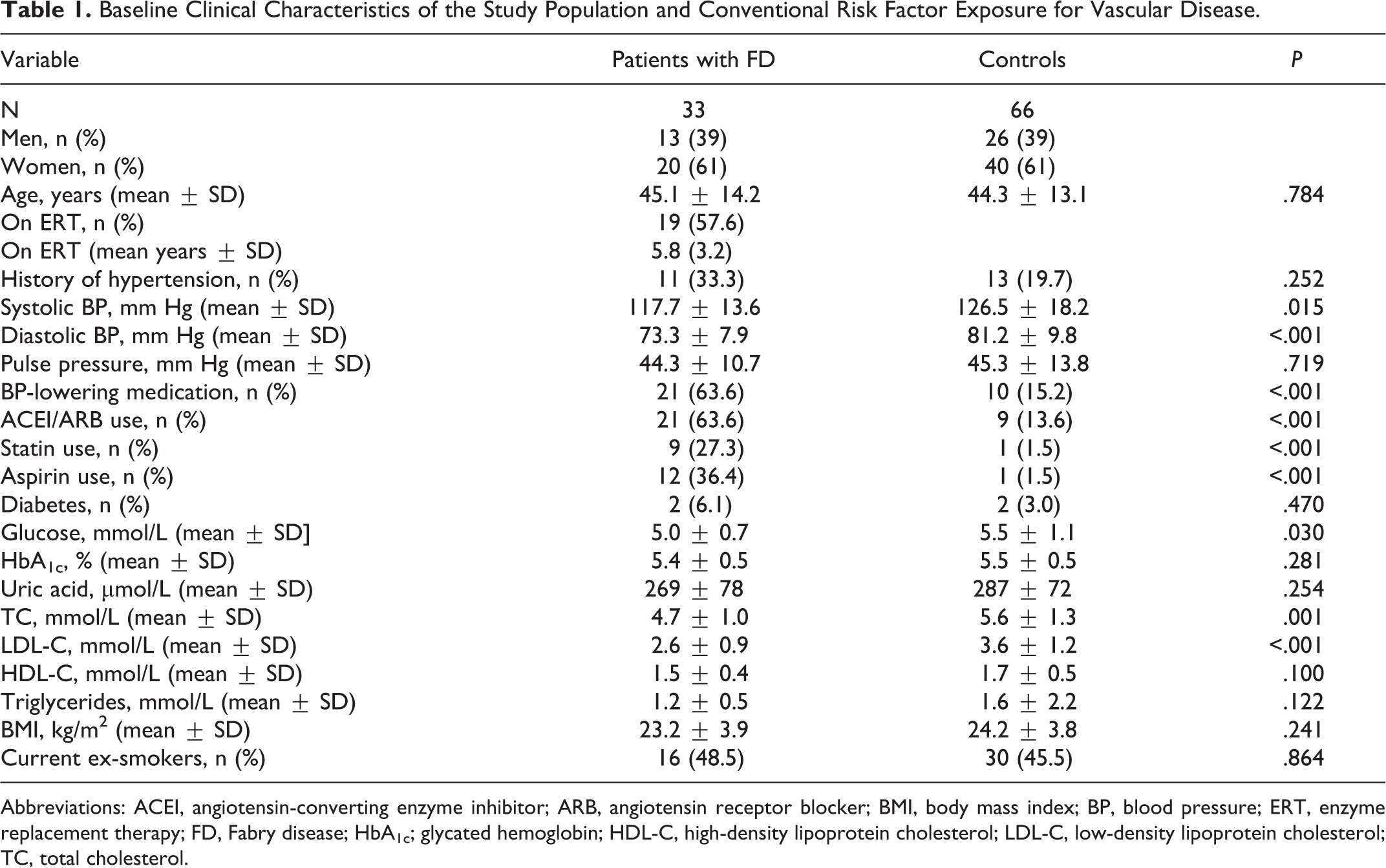
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BP, blood pressure; ERT, enzyme replacement therapy; FD, Fabry disease; HbA1c; glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol.
Patients with FD were analyzed for the presence of renal and heart disease by assessing renal function (estimated glomerular filtration rate, eGFR), level of proteinuria, high-sensitivity troponin-T (hsTnT) serum levels, and the presence of diastolic dysfunction and left ventricular hypertrophy (LVH). Those parameters were compared between treated and nontreated group of patients with FD.
Laboratory Assessments
Participants were instructed to fast overnight (10-12 hours). To minimize the effects of ERT on plasma, blood samples from patients with FD on ERT were collected immediately before enzyme infusion and on the 14th day after the previous infusion. Biochemical parameters (lipids, blood glucose, HbA1c, homocysteine, uric acid, hsTnT, creatinine, and urea), inflammatory and endothelial markers (high-sensitivity CRP [hsCRP], mg/L), lipoprotein a (Lp(a), g/L), interleukin-6 (IL-6, ng/L), vascular cell adhesion molecule-1 (VCAM-1, µg/L), E-selectin (µg/L), and tumor necrosis factor α (TNF-α, ng/L) were measured in all participants according to standard laboratory protocols.
Renal function was evaluated using the Chronic Kidney Disease Epidemiology Collaboration equation. 16 Proteinuria was assessed using a 24-hour collection of urine.
Study Protocol
Blood pressure (BP) was measured using the nondominant arm and a validated automatic oscillometric device (Datascope Duo, Mindray Electronics Co., Ltd). Pulse pressure (mm Hg) was calculated as the differences between the systolic and diastolic BP. Hypertension was defined as a systolic BP ≥140 mm Hg and/or a diastolic BP ≥90 mm Hg as a mean of 3 consecutive measurements or use of medication to lower the BP. Before the examination, patients lay quietly for 10 to 15 minutes in a dark, temperature-controlled room. Body mass index was calculated as weight in kg measured in light clothing, divided by the height in m2.
Ultrasound examinations were performed by a sonographer trained and certified in vascular echography. Before the examination, patients lay quietly for 10 to 15 minutes in a dark, temperature-controlled room. The internal lumen diameter and cIMT were measured with high-resolution imagers (ProSound Alpha 7, Hitachi Aloka, Medical Ltd.), with a 13.3 to 3.61 MHz probe. The carotid bulb was identified on both sides, and the segments of the common carotid arteries 1.5 to 2 cm proximal to the bifurcation were scanned. The resolution box function was adjusted to visualize the lumen-intimal and media-adventitial interfaces and the arterial posterior (far) wall along 1 cm of length was magnified. Two angles were used for common carotid IMT and lumen diameter measurements on both sides: anterior oblique and lateral. Vessel images in telediastole were analyzed. The cIMT was measured at a site free of any discrete plaques. Six measurements of far-wall cIMT were obtained manually using ultrasound calipers for each image, and the per-subject cIMT was defined as the average of the 6 cIMT measurements. The largest measurement of IMT on both the left and the right side was used for analysis.
A plaque in carotid arteries was defined as a focal wall thickening that was ≥50% greater than the thickening of relative to the adjacent wall segment or as a focal region with a IMT of >1.2 mm. 17 The participant was considered to be without a plaque if the morphology of the arteries was reported to be normal with homogenous IMT thickness. The number and thickness of artery plaques was measured from carotid arteries. For each artery, at least 2 optimal images were stored.
We estimated endothelial function by performing the postischemic brachial FMD which was expressed as the percentage of dilation in 60 seconds according to published guidelines. 18
Standard cardiac ultrasound was performed to assess parameters of heart involvement according to international recommendations. 19 Presence of LVH was defined as diastolic left ventricular wall thickness <12 mm. 14
Statistical Analyses
Statistical analyses were performed using IBM SPSS Statistics, ver. 22 (IBM Corp). The Shapiro-Wilk test was applied to assess the data distribution. Normally distributed values are presented as mean ± SD, and non-normally distributed variables as median (range). The t test was used to analyze normally distributed variables, and the Mann-Whitney U test was used to analyze data with nonparametric data to identify significant differences between the FD and control groups. Categorical variables were analyzed by χ2 test and expressed as percentage. A 2-sided P < .05 was considered significant.
Results
The age of participants (mean age ± SD) was 45.1 ± 14.2 years for the patients with FD and 44.3 ± 13.1 years for the controls. The patients with FD had significantly lower blood sugar, but there were no differences in HbA1c. Measured BP, but not pulse pressure, was significantly lower in patients with FD, where the majority were taking ARBs or ACEIs as antiproteinuric drugs and not because of proven hypertension. Total cholesterol and low-density lipoprotein cholesterol were significantly lower in the patients with FD, but 9 of the patients with FD were on hypolipidemic treatment. There was no difference in BMI between patients and controls (Table 1).
Endothelial Dysfunction and Vascular Remodeling in FD
When comparing the total cohort of classic patients with FD with matched controls, cIMT was significantly increased (0.07 vs 0.06 cm; P = .021; Table 2). Flow-mediated dilation was significantly lower than in controls (4.48% vs 10.67%; P = .001). The radius of common carotid arteries (0.80 ± 0.12 cm in patients with FD, 0.70 ± 0.06 cm in controls; P < .001; Table 2) and aortic bulb diameter (3.07 ± 0.48 cm in patients with FD and 2.72 ± 0.48 cm in controls; P = .001; Table 2) were significantly higher in all patients with FD relative to the healthy controls. Atherosclerotic plaques were found in the carotid arteries of only 3 older FD women, and their abundance was significantly lower compared with controls (Table 2).
Parameters of Systemic Endothelial Function and Cardiovascular Remodeling in FD Patients (for Total Cohort and for Men and Women Separately) Relative to Healthy Controls.
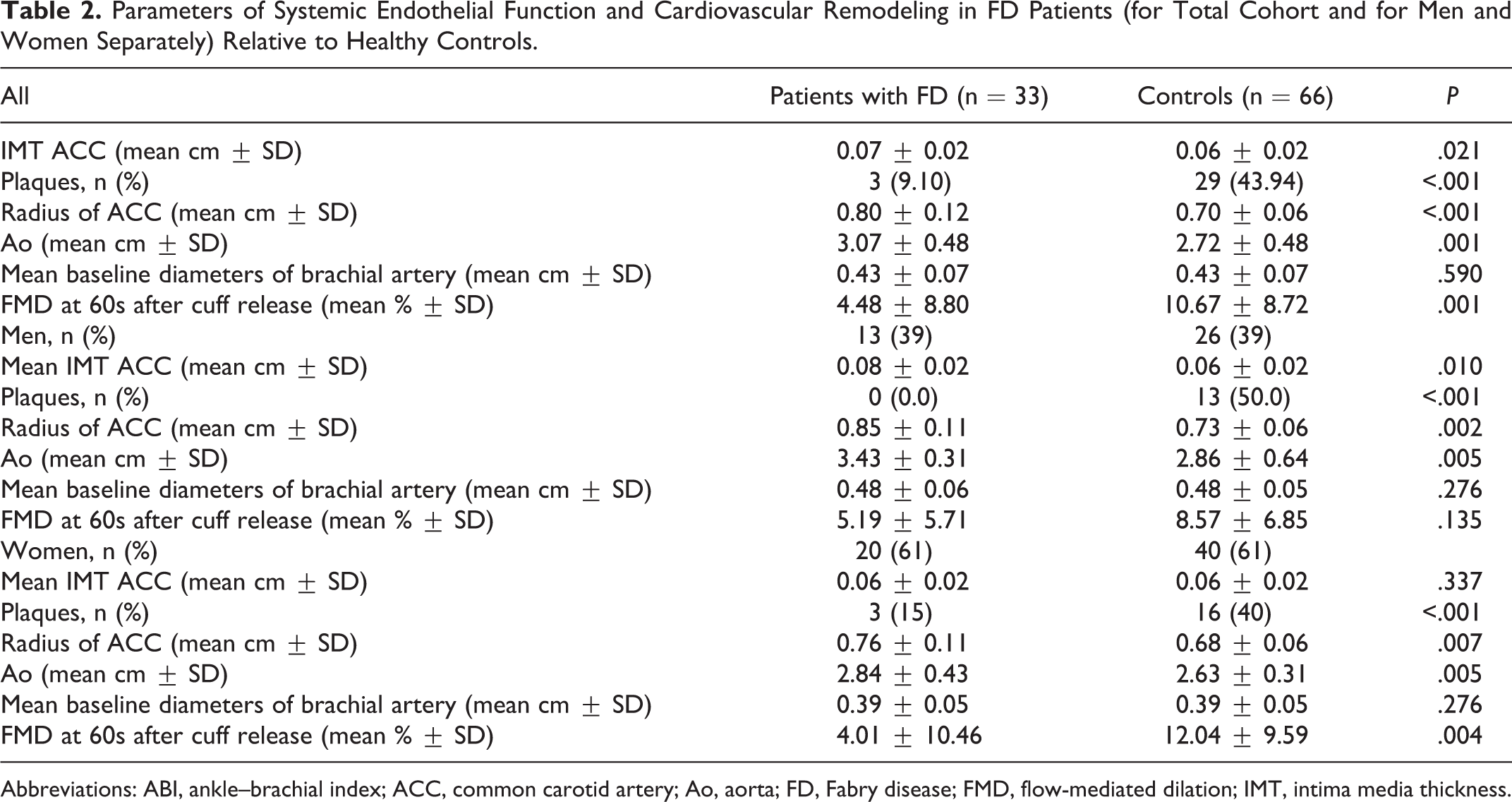
Abbreviations: ABI, ankle–brachial index; ACC, common carotid artery; Ao, aorta; FD, Fabry disease; FMD, flow-mediated dilation; IMT, intima media thickness.
Analysis by sex revealed that cIMT, radius of carotid arteries, and aortic bulb diameter were increased, and FMD was comparable in males relative to matched controls. In women with FD, cIMT was comparable with matched controls, FMD was significantly decreased, and the radius of carotid arteries and aortic bulb diameter were significantly increased.
For serum biomarkers of endothelial dysfunction and inflammation, the plasma concentrations of VCAM-1, IL-6, and hsCRP were significantly elevated, and TNF-α also showed a trend for elevated levels in patients with FD compared with control patients. E-selectin was significantly lower in patients with FD compared with control patients. No differences were observed for homocysteine and Lp(a) in patients with FD versus healthy volunteers (Table 3).
Serum Levels of Biomarkers for Endothelial Dysfunction and Inflammation of FD Patients and Control Patients (Total Patients and for Men and Women Separately).
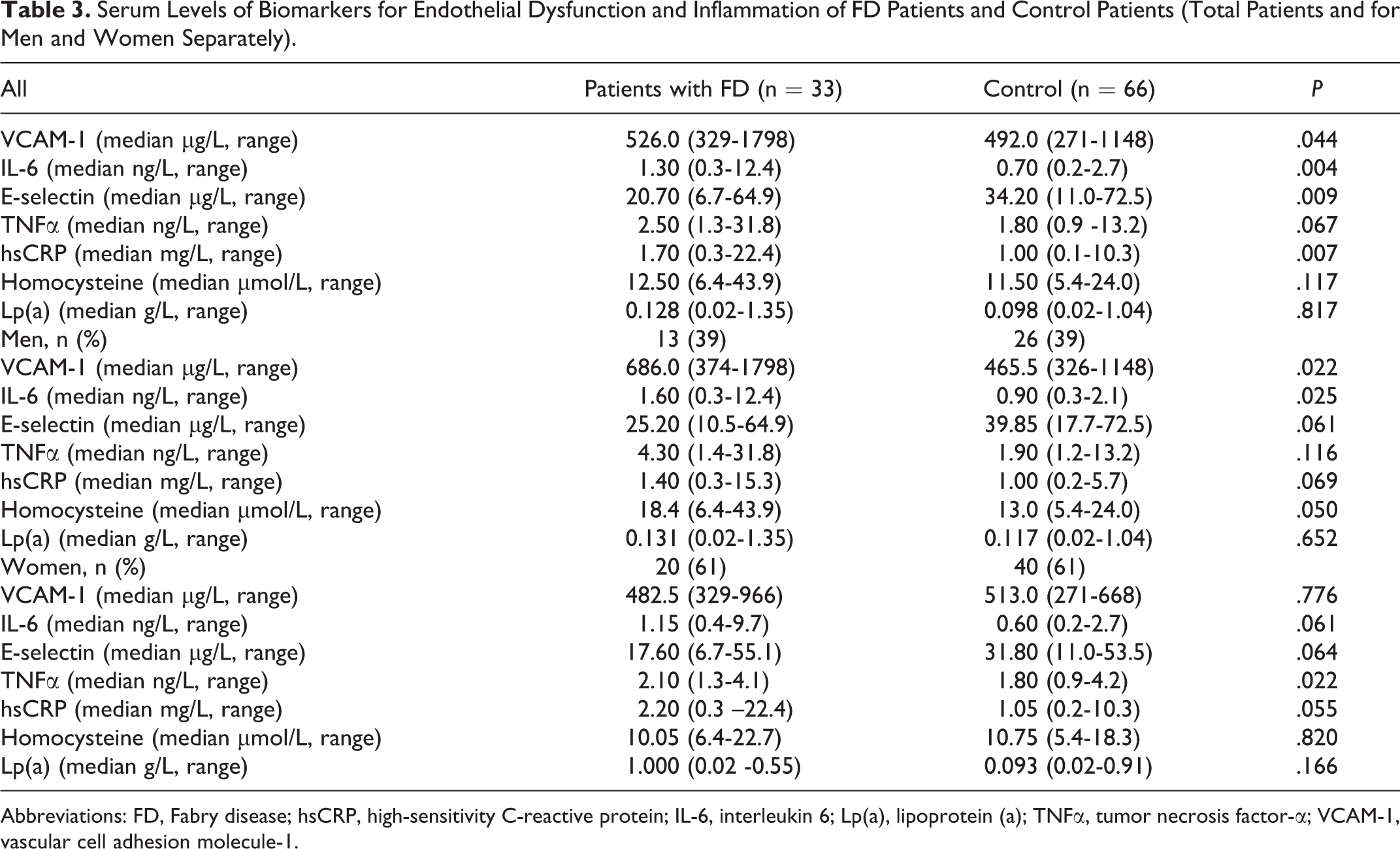
Abbreviations: FD, Fabry disease; hsCRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; Lp(a), lipoprotein (a); TNFα, tumor necrosis factor-α; VCAM-1, vascular cell adhesion molecule-1.
When results were differentiated according to sex, female patients with FD did not differ significantly in VCAM-1 (P = .39) relative to healthy females, whereas male patients with FD had relatively higher VCAM-1 levels compared with matched controls (P = .022). Tumor necrosis factor-α was not significantly elevated in male patients with FD (P = .116), but homocysteine concentrations were elevated (P = .005; Table 3).
Patients with FD were assessed for renal and cardiac disease in the treated group versus the nontreated patients. Patients in the treated group were older and mainly males, while in nontreated there were only females, who were younger (P = .088). Clearly patients on treatment were more affected by the disease since all analyzed parameters of renal (eGFR, P = .033), proteinuria (P = .048), and cardiac involvement (hsTnT [P = .015], the presence of diastolic dysfunction [P = .003], and LVH [P = .003]) differed significantly (Table 4).
Differences Between Fabry Patients Regarding ERT.
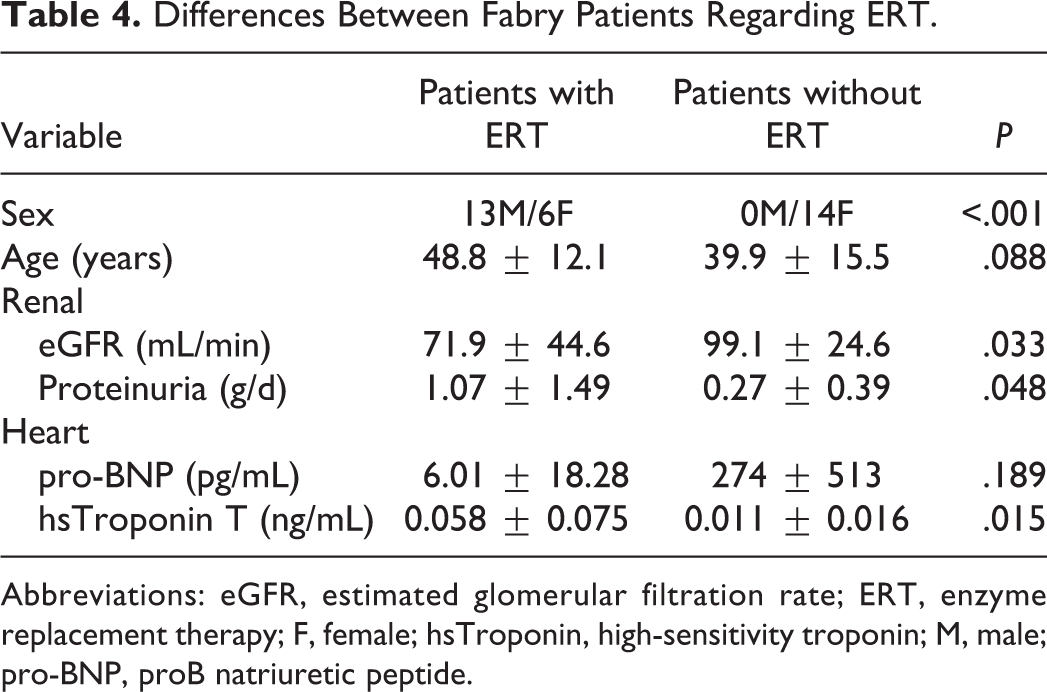
Abbreviations: eGFR, estimated glomerular filtration rate; ERT, enzyme replacement therapy; F, female; hsTroponin, high-sensitivity troponin; M, male; pro-BNP, proB natriuretic peptide.
Discussion
Fabry disease is predominantly a systemic vascular disorder with defined vasculopathy of small as well as large vessels. 8,20,21 The principal clinical manifestations are cerebrovascular, cardiac, and renal disease which limit life expectancy. 20 Before renal replacement therapy became available, male patients with FD died at about 40 years of age due to renal failure, but currently cardiovascular disease is the most frequent cause of death. 9,10 In this study, we investigated vascular remodeling, endothelial dysfunction, and atherosclerosis in a Slovene cohort of patients with FD.
We found moderately increased arterial wall thickness, substantially decreased endothelial function, reduction in atherosclerotic plaques, and increased plasma levels of adhesion molecules and inflammatory molecules.
The patients with FD in our cohort were already old and their treatment (ERT), at least for males, probably started too late and they had been on ERT for only about 5 years. Therefore, it was difficult to evaluate the possible role of ERT and aging on vascular changes, since in addition the initial data at ERT initiation were not available. The sole effect of ERT would be best evaluated in a prospective study involving young males (eg, boys age 10-15 years) who started ERT early before the development of significant vascular changes. However, there is no such study available.
The differences between patients with FD and controls were more pronounced in men. This certainly reflects the fact that males were more affected and mainly treated with ERT, whereas most females were not seriously affected and did not need treatment. This was confirmed by subanalysis that showed important difference between the treated and nontreated groups. Treated patients were older, with lower eGFR, higher level of proteinuria, higher serum concentration of hsTnT, and higher frequency of diastolic dysfunction and LVH (Table 4). These differences indicate that treated patients were more affected and with frequent renal and heart involvement. On the other hand, nontreated females were mainly asymptomatic or oligosymptomatic with only 3 females having mild LVH and only 1 having renal involvement (proteinuria >0.5 g/d).
The exact mechanism of vascular dysfunction, which is the main pathophysiological disorder in FD, remains unclear. Progressive accumulation of glycolipids, primarily Gb3 and lyso-Gb3, in vascular endothelial cells represents the most well-characterized pathological event. 8 The cascade of secondary pathophysiological outcomes includes inflammation and oxidative stress which can result in structural abnormalities in vessel walls, activated endothelium, and presence of a prothrombotic state. 7,22 -24 Vascular structural and functional changes, particularly in the microcirculation, lead to tissue infarction and ischemia resulting in many of the late complications of classical FD. 20 The development of irreversible tissue fibrosis ultimately leads to severe end-organ damage. 14,20 Several studies have reported that the removal of stored glycosphingolipids from endothelial cells via disease-specific therapy is of limited impact in the prevention of cardiovascular complications in FD. 25,26
Endothelial dysfunction, which interferes with the contractile status of the vascular smooth muscle, induces the increased expression of adhesion molecules and inflammatory cells. 27 Excess intracellular accumulation of Gb3-induced oxidative stress in in vitro studies 28 and upregulated the expression of cellular adhesion molecules in vascular endothelial cells of patients with FD. 24 Treatment of cells in vitro with α-Gal A led to reduction of endogenous Gb3 and decreased expression of adhesion molecules. 29 Previous studies reported increased biomarker levels for endothelial activation, such as soluble VCAM-1, soluble intercellular adhesion molecule, P-selectin, E-selectin, plasminogen activator inhibitor, 22,30,31 and endothelium-derived microparticles. 32 We measured circulating markers of inflammation and endothelial activation, and our findings also confirmed a significant increase in the levels of VCAM-1, IL-6, TNF-α, and hsCRP in patients with FD.
Flow-mediated dilation is widely used to assess endothelial function in conduit arteries. 33 Increased blood flow in conduit arteries causes an increase in shear stress and thus, by increasing nitric oxide (NO) production, leads to vasodilation. 33 Others showed that abnormal vascular responses in patients with FD were endothelium dependent and NO independent. 34 Endothelial function assessed by FMD has been shown to be affected by cardiovascular risk factors such as smoking, hypertension, hypercholesterolemia, obesity, diabetes mellitus, physical inactivity, hyperhomocysteinemia, and the aging process. 33 Our study participants were matched for age, sex, BMI, history of hypertension, and smoking status. Risk factors in patients with FD were very strictly controlled and treated (significantly higher percentage of patients with FD were on antihypertensive medications, acetylsalicylic acid, and statins). Nevertheless, the patients with FD exhibited significantly impaired FMD compared with controls. Our observations are in agreement with other studies 35,36 and show that endothelial function, as measured by brachial FMD, is significantly impaired/lower in patients with FD compared with healthy controls. When the FMD results were differentiated by sex, we found a significant decrease in FD females and a nonsignificant decrease in FD males. The impairment of endothelial function in females may be explained by a lower rate of prescribed medical therapies (acetylsalicylic acid, statins, ACEIs) and ERT compared with males.
The major structural change observed in the arterial walls of normotensive adult patients with FD is increased IMT due to the combination of smooth muscle cell proliferation in the media and enhanced vascular endothelial Gb3 storage. An increased IMT has been demonstrated in medium and large muscular arteries (eg, radial, carotid, and brachial and abdominal aorta) of patients with FD. 35,37 –39 Although cIMT measurements in patients with FD were still within normal limits, our data show significantly higher IMT of common the carotid arteries in patients with FD relative to healthy controls. In affected men, cIMT was increased compared with controls; however, in classically affected women, cIMT was comparable to healthy controls, which is in accordance with another report. 35 The variability of FD manifestation in heterozygous females is expected to be much higher than in males due to X-chromosome inactivation (XCI). X-chromosome inactivation is the process by which gene dosage equivalence is achieved between female with 2 X chromosomes and male with a single X chromosome. This happens at random within females resulting in inactivation of 1 X chromosome. There is a different course of illness for female patients with skewed XCI profiles, which depends on the predominantly expressed allele. 40 It would be of interest to include X-inactivation analysis in comparison and correlation with vascular parameters, but at the present time this methodology is not generally available and is available in only very few centers. Therefore, in general, symptoms usually occur later in life and disease progression is slower in females. 41
A number of genetic factors may modulate the interaction between α-D-galactosyl glycolipid accumulation and atherosclerotic plaque formation. Bodary et al observed that α-Gal A deficiency accelerates atherosclerosis in mice in the context of another genetic defect, apolipoprotein E deficiency. 42 The Altarescu group has shown that polymorphisms of genes known to be risk factors for stroke modify the likelihood of developing cerebral ischemic lesions in FD. 43 Collectively, these findings support the importance of genetic modification for the phenotypic expression in this single gene disorder. The process of atherosclerosis may thus be superimposed on FD vasculopathy, but this hypothesis requires systematic investigation. 44
Macroangiopathy changes have been repeatedly observed in patients with FD. Arterial remodeling is characterized by progressive vascular dilation and elongation of the conduits. 21 The vascular tortuosity observed in FD is likely to cause turbulent blood flow, which may contribute to the formation of focally distributed incipient atherosclerotic lesions. 45 Endothelial function is affected by risk factors, whereas occurrence of plaques at bifurcations of large arteries is predominantly affected by hemodynamic factors. 45 Therefore, it may be speculated that patients with FD possess different susceptibilities to hemodynamic stress at bifurcations due to different arterial wall characteristics. Aortic bulb diameter and radius of common carotid arteries were significantly greater in all patients with FD relative to healthy controls in our study. Patients with classic FD had a high prevalence of ascending aorta dilation 46,47 ; therefore, FD should be included in the differential diagnoses of genetic diseases leading to premature ascending aortic dilation/aneurysm. 48 Dilation appeared to be independent from cardiovascular risk factors and appears at a younger age in patients with FD compared with the general population. 49
According to observed vascular changes (particularly impaired endothelial function), a high rate of atherosclerotic changes is expected in patients with FD. However, differing reports regarding atherosclerosis in FD. Thus, in a histological study, there were no signs of atherosclerosis. 50 The Barbey group reported the absence of atherosclerotic plaques in the common carotid artery of patients with FD and suggested that the conduit arteries may be protected from atherosclerosis in FD. 37 On the other hand, others found atherosclerosis changes. 41,51 However, no study investigated the relation between arterial wall remodeling typical for FD and susceptibility/occurrence of atherosclerotic plaques.
Fabry disease can be conceived as a multidomain disease phenotype. The clinical phenotype is modulated by the effects of variation in other genetic loci (polygenic inheritance) and environmental stressors. 7 It is critically dependent on patient age and gender. 20 With advancing age, patients with FD, along with the general population, accumulate multiple atherosclerosis risk factors for the development of widespread atherosclerosis and vascular impairment, such as renal insufficiency, diabetes, and hypertension. Therefore, it would be expected that these risk factors for atherosclerosis, in combination with α-Gal A deficiency, would make patients with FD more susceptible to atherosclerosis. Indeed, we found the opposite with significant less plaques in patients with FD. Definitively, arterial wall is changed due to vascular smooth cell hypertrophy, increased extracellular matrix expression and consequent wall fibrosis, whereas the intima also undergoes fibrotic changes due to accumulation of α-D-galactosyl glycolipids. Consequently, the less compliant arterial wall, along with hyperdynamic circulation, is exposed to continuous hemodynamic load with resulting increased expression of adhesion molecules (as found in our study), cytokines and chemokines that collectively induce a prothrombotic milieu leading to vascular complications. These predictions are partially confirmed by assumptions from others. 21 We speculate that fibrotic processes in intima and media are opposing cholesterol penetration and formation of atherosclerotic plaques (as observed in our study). Of course, the wide use of statins in our patients with FD could play an additional role in the low rate of atherosclerotic plaques.
A major limitation of this single center study is the small sample size, which is an unavoidable consequence of the rarity of FD. The differences in disease stage, pooled analysis of data from both heterozygous female and hemizygous male patients with FD, and from patients receiving ERT may play a role in variability of the findings.
Conclusions
In our cohort, the following vascular phenotype was observed in patients with FD: moderately increased arterial wall thickness, substantially impaired endothelial function, reduction in atherosclerotic plaques, and increased plasma levels of adhesion and inflammatory mediators. A very low incidence of atherosclerotic plaques in arteries with substantial endothelial dysfunction is difficult to rationalize based on current pathophysiological paradigms. This is a challenge for further research that could have important clinical applications.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published. The authors confirm that content of the manuscript has not been published or submitted for publication elsewhere.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.C.V. received speaker honoraria and travel support from Sanofi Genzyme and Takeda. B.V. received speaker honoraria and travel support from Sanofi Genzyme, Takeda, and Greenovation and is a member of the European Fabry Registry Board of Advisors, sponsored by Sanofi Genzyme.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.