
Abstract
The prognostic value of high-sensitivity C-reactive protein (hsCRP) in complex coronary artery disease has not been fully established. We aimed to determine the association between hsCRP and long-term outcomes in elderly patients with 3-vessel disease (TVD). From April 2004 to February 2011, 3069 patients aged ≥65 years with TVD were consecutively enrolled and received medical treatment alone, percutaneous coronary intervention, or coronary artery bypass grafting. The patients were divided into 2 groups according to their hsCRP levels: <3.00 mg/L (62.1%) and ≥3.00 mg/L (37.9%). The mean age was 71 ± 4 years. The high hsCRP group had more risk factors and more frequently received conservative treatment than the low hsCRP group. During a median follow-up period of 6.2 years, elevated hsCRP was significantly associated with increased all-cause death (19.5% vs 29.6%, P < .001), cardiac death (9.4% vs 15.2%, P = .001), and major adverse cardiovascular and cerebrovascular events (34.1% vs 42.5%, P = .001). Multivariable Cox regression analyses revealed that hsCRP was an independent predictor for all of these events. Combining hsCRP with Synergy between PCI with TAXUS and Cardiac Surgery score II further improved the predictive power of the score. The relationship between hsCRP and mortality was relatively consistent across subgroups. Overall, hsCRP could prove useful for risk prediction in elderly patients.
Keywords
Introduction
Coronary artery disease (CAD) is a leading threat to public health, and 3-vessel disease (TVD) accounts for approximately one-third of all cases in this era of population aging.1,2 Revascularization is important, and guidelines recommend that timely scoring models like the SYNTAX score (SS) should be applied for anatomical evaluation and decision-making during hospitalization.3,4 However, various factors besides anatomical severity are involved in decision-making. Thus, the updated SS II, which integrates the original SS with clinical characteristics such as age and comorbidities, has emerged as a promising tool for management.5,6 Rencuzogullari et al 7 evaluated 6 risk scores for outcomes in octogenarians with ST-elevated myocardial infarction (STEMI) and provided sound evidence for the superiority of SS II.
Systemic inflammation is associated with multiple chronic diseases that often coexist in patients with advanced age.8–11 In particular, inflammation is considered to play an essential role in the initiation and chronic development of CAD as well as in an acute ischemic event.12–14
High-sensitivity C-reactive protein (hsCRP) is a widely used inflammatory biomarker in clinical practice. 15 However, there is a paucity of evidence concerning the relationship between inflammatory status and prognosis of TVD, especially in elderly adults. To fill this gap, the present study aimed to determine whether hsCRP can be useful for predicting long-term outcomes and consequently improve the predictive ability of SS II in elderly Chinese patients with TVD.
Materials and Methods
Subjects and Study Design
We conducted a single-center, prospective cohort study on 8943 consecutively enrolled patients from April 2004 to February 2011. Three-vessel disease was defined as angiographic stenosis ≥50% in all 3 main coronary arteries, including the left anterior descending, circumflex, and right coronary artery, with or without involvement of the left main artery. A total of 3593 patients aged ≥65 years were eligible for the study. Patients with missing records for hsCRP were excluded. The institutional review board approved the study protocol in accordance with the Declaration of Helsinki, and all patients provided written informed consent.
Results of blood tests at admission and imaging examinations as well as clinical baseline data were recorded. A plasma hsCRP ≥3 mg/L was considered positive.
Patients received medical therapy (MT) alone, percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG) according to contemporary practice guidelines, heart team judgment, and patient preference. Baseline and procedural data for all participants were collected into a database by independent clinical research coordinators.
The SS was calculated using an online calculator (http://www.syntaxscore.com) by 2 of the 3 experienced cardiologists participating in this study in an independent angiographic core laboratory; they were blinded to the clinical data. 16 A lesion with ≥1.5 mm in diameter and ≥50% stenosis was scored using the digital videos of angiography. When disagreement occurred, the opinion of the third observer was obtained, and the final decision was made by consensus. Intraobserver variability for calculation of the SS (tertile partitioning), based on reanalyzing 50 cases at a 3-month interval, indicated a high level of agreement (j statistic 0.879; 95% CI, 0.81-0.94; P < .001). The SS II was calculated when combining anatomical SS with the clinical variables as previously described. 5
Follow-Up and Definitions of End Points
After enrollment, outcome data were obtained by telephone interview, follow-up letter, or clinic visit. The last follow-up was completed in 2016. The primary end point was all-cause death. Secondary end points included cardiac death and major adverse cardiovascular and cerebrovascular events (MACCEs), a composite of all-cause death, myocardial infarction (MI), stroke, and/or unplanned revascularization. All deaths were considered cardiac unless an unequivocal noncardiac cause could be established.
Statistical Analysis
Continuous variables were summarized as mean ± SD or median (interquartile range) and were compared by Student t test or the Mann-Whitney U test as appropriate. Categorical variables were expressed as percentage and were compared by the χ2 test or Fisher exact test as appropriate. Propensity score (PS) matching was performed to adjust for baseline differences between the groups with a matching ratio of 1:1 and a caliper of 0.2.
Kaplan-Meier curves were created to compare the event risks between the groups. Variables with statistical significance in univariable Cox proportional hazards regression analyses were subsequently incorporated in multivariable models to screen for independent predictors of adverse events. The effect of combining of hsCRP and SS II was estimated by the C-index, net reclassification index (NRI), and integrated discrimination improvement compared with SS II alone as previously described.17,18
A 2-tailed P < .05 was considered significant. Analyses were performed using 2 statistical software packages, SPSS Statistics version 20.0 and R software version 3.4.3.
Results
Baseline Characteristics
After excluding patients who lacked records for hsCRP (n = 524), 3069 patients were enrolled in the study. The mean age was 71 ± 4 years, 2195 (71.5%) were male, and 1927 (62.8%) presented with acute coronary syndrome (ACS; including acute MI and unstable angina). Among all patients, 34% received MT, 38% received PCI, and 28% received CABG. The patients were divided into 2 groups according to their hsCRP levels: <3.0 mg/L (n = 1905, 62.1%) and ≥3.0 mg/L (n = 1064, 37.9%).
The baseline characteristics are detailed in Table 1. The patients with elevated hsCRP were older and more likely to be female. No significant differences were found for comorbidities, except for chronic kidney disease (P = .03). However, high hsCRP was correlated with abnormalities in lipid and glucose metabolism as well as cardiac and renal function. Moreover, the proportions of ACS onset and MT choice were significantly increased following elevation of hsCRP.
Baseline Characteristics Between Normal and High hsCRP Groups.a
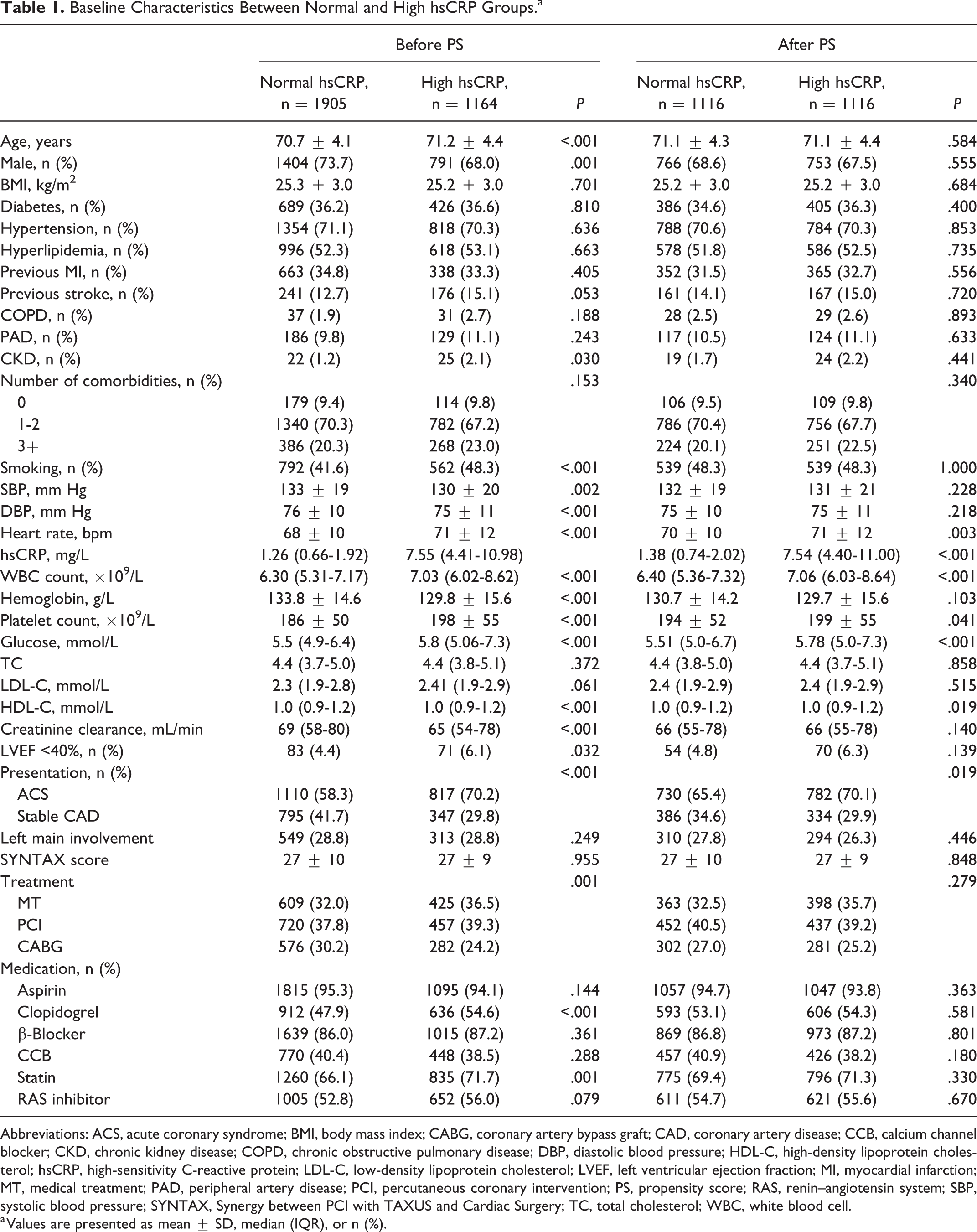
Abbreviations: ACS, acute coronary syndrome; BMI, body mass index; CABG, coronary artery bypass graft; CAD, coronary artery disease; CCB, calcium channel blocker; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; MI, myocardial infarction; MT, medical treatment; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; PS, propensity score; RAS, renin–angiotensin system; SBP, systolic blood pressure; SYNTAX, Synergy between PCI with TAXUS and Cardiac Surgery; TC, total cholesterol; WBC, white blood cell.
a Values are presented as mean ± SD, median (IQR), or n (%).
Outcomes
The median follow-up period was 6.2 (4.7-8.2) years. All patients achieved ≥1 year of follow-up. The last follow-up was completed in March 2016, and the response rate was 78%. Overall, 716 (23.3%) patients died, in whom half had a cardiac cause. A total of 1145 (37.3%) patients experienced MACCE.
Compared with the low hsCRP group, an elevated hsCRP was strongly related to increases in all-cause death (19.5% vs 29.6%, P < .001), cardiac death (9.4% vs 15.2%, P = .001), and MACCE (34.1% vs 42.5%, P = .001; Figure 1). The Kaplan-Meier curves (Figure 2) illustrated an ongoing divergence in the cumulative occurrences of these events (all log rank, P < .001). Furthermore, although attenuated, hsCRP remained independently predictive of both the primary and secondary end points in multivariable Cox analyses as well as after PS matching (Table 2, Supplementary Table 1). The hazards for death, cardiac death, and MACCE were increased by 39%, 50%, and 24%, respectively, with hsCRP elevation in the multivariable Cox models.
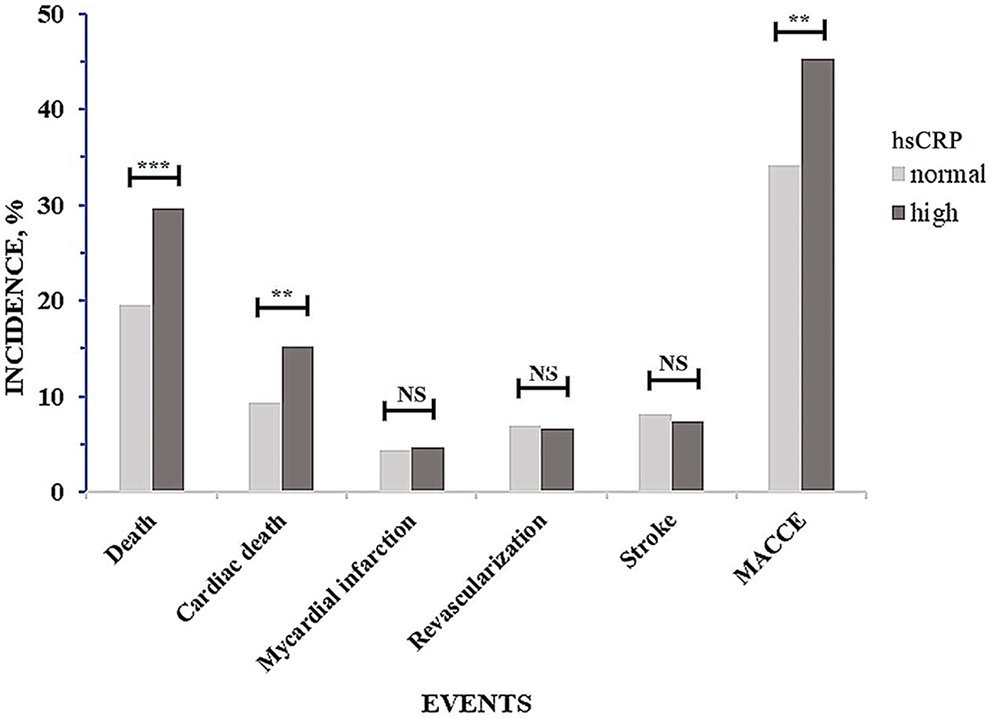
Clinical outcomes between normal and high high-sensitivity C-reactive protein groups.
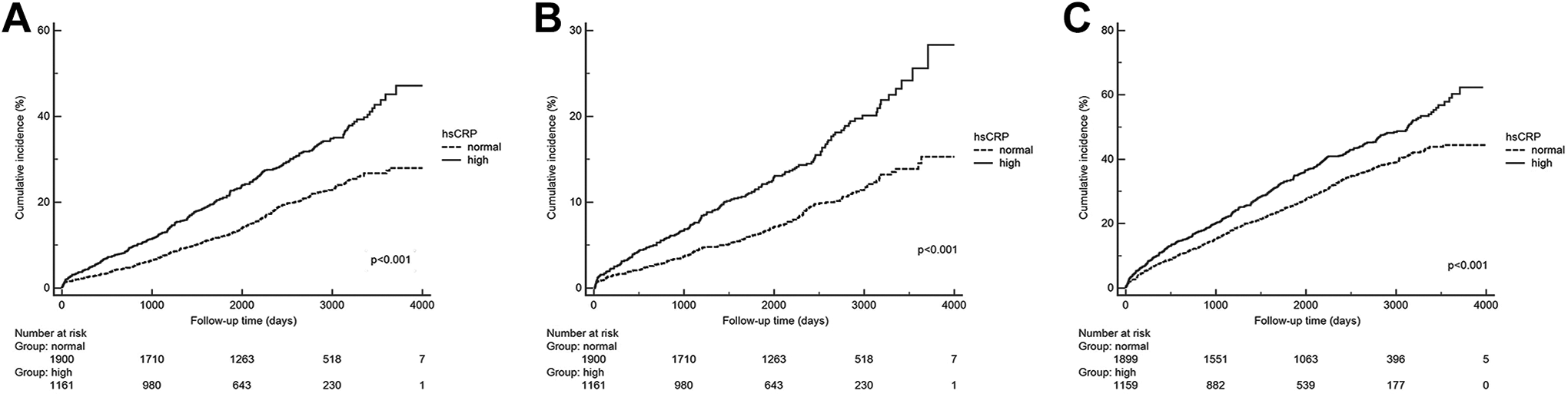
Kaplan-Meier curves for all-cause death (A), cardiac death (B), and major adverse cardiovascular and cerebrovascular events (C). hsCRP indicates high-sensitivity C-reactive protein.
Relationship Between hsCRP and Outcomes in Cox Regression Analysis.a
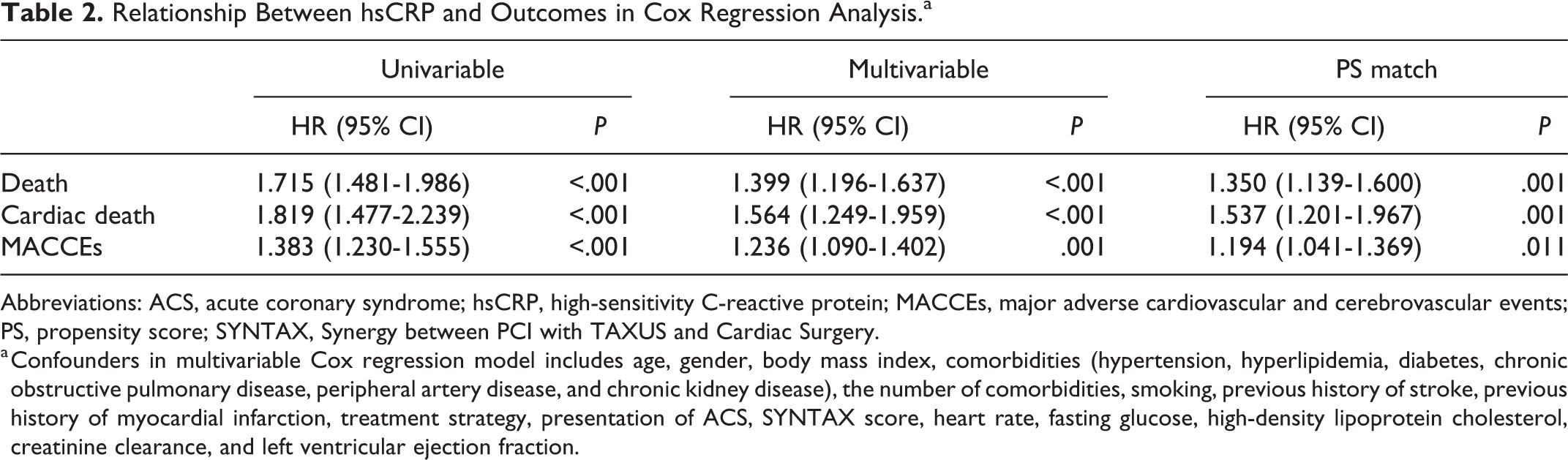
Abbreviations: ACS, acute coronary syndrome; hsCRP, high-sensitivity C-reactive protein; MACCEs, major adverse cardiovascular and cerebrovascular events; PS, propensity score; SYNTAX, Synergy between PCI with TAXUS and Cardiac Surgery.
a Confounders in multivariable Cox regression model includes age, gender, body mass index, comorbidities (hypertension, hyperlipidemia, diabetes, chronic obstructive pulmonary disease, peripheral artery disease, and chronic kidney disease), the number of comorbidities, smoking, previous history of stroke, previous history of myocardial infarction, treatment strategy, presentation of ACS, SYNTAX score, heart rate, fasting glucose, high-density lipoprotein cholesterol, creatinine clearance, and left ventricular ejection fraction.
Combination of hsCRP With SS II
On combining hsCRP level with the SS II score, the resulting reclassification of all-cause death, cardiac death, and MACCE yielded significant improvements described by NRI and integrated discrimination improvement (Ps < .01; Table 3). More specifically, the combination of hsCRP with SS II produced a categorical NRI of 0.049 (0.006-0.091) with P = .026, indicating a 4.9% improved classification (Supplementary Table 2). Regarding discrimination, both all-cause death and cardiac death reached statistical significance in the C-index combining hsCRP with SS II, while MACCE showed a nonsignificant change (P = .069).
Additional Predictive Value Provided by hsCRP Beyond the SYNTAX Score II.
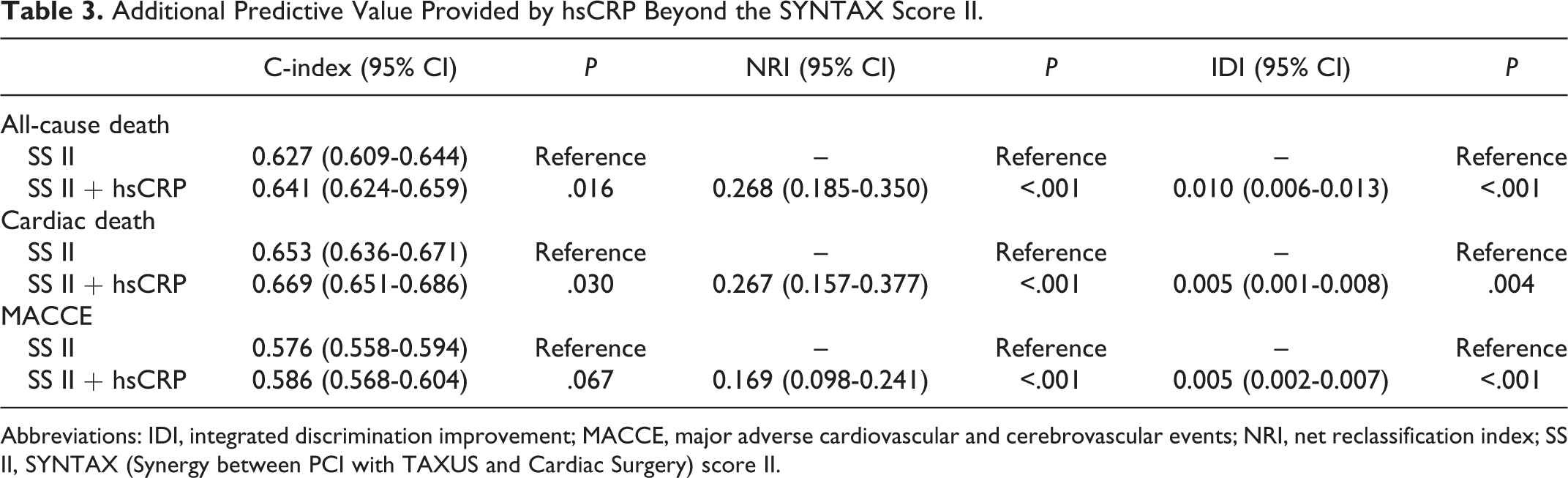
Abbreviations: IDI, integrated discrimination improvement; MACCE, major adverse cardiovascular and cerebrovascular events; NRI, net reclassification index; SS II, SYNTAX (Synergy between PCI with TAXUS and Cardiac Surgery) score II.
Subgroup Analyses
We conducted further analyses regarding survival or nonsurvival in the major subgroups (Figure 3). There were no interactions between hsCRP and the majority of covariates (age, sex, hypertension, CAD types, and treatment strategies), while the interactions with diabetes and hyperlipidemia reached statistical significance. After adjustment for confounders, hsCRP remained independently predictive for long-term mortality in the subgroups (HR ranging from 1.30 and 1.55), with the exception of female sex, STEMI onset, and CABG group.
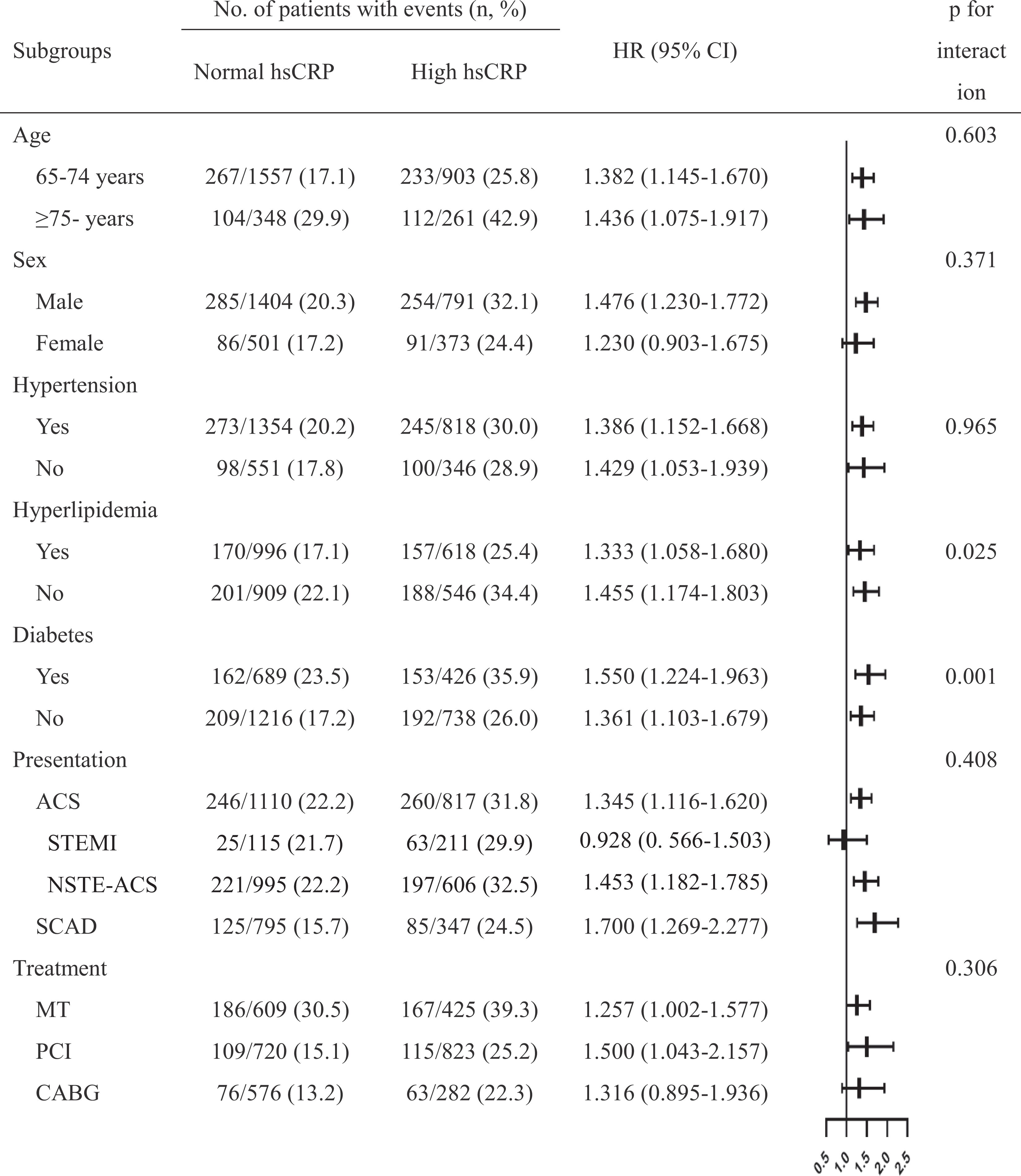
Subgroup analyses of outcomes. ACS indicates acute coronary syndrome; CABG, coronary artery bypass grafting; CAD, coronary artery disease; hsCRP, high-sensitivity C-reactive protein; MT, medical treatment; PCI, percutaneous coronary intervention; SCAD, stable coronary artery disease.
Discussion
To the best of our knowledge, the present study is the first to specifically investigate the role of hsCRP in predicting long-term outcomes in a large cohort of elderly patients with TVD. The major findings were (1) patients with elevated hsCRP on admission had more risk factors such as advancing age, smoking, and deteriorated renal or cardiac function; (2) baseline hsCRP was an independent predictor of all-cause death, cardiac death, and MACCE; (3) hsCRP provided increased accuracy for risk prediction beyond SS II; and (4) the positive correlation between hsCRP and mortality rate remained consistent in various subgroups.
Evidence supports that baseline hsCRP levels can predict poor prognosis in patients with established CAD.19–21 Wada et al 19 recruited all-comer patients aged 66 ± 10 years and demonstrated a significant relationship between hsCRP and long-term outcomes after PCI. Similarly, Eldrup et al 20 found that hsCRP > 3 mg/L predicted a 40% increase in adverse events under stable atherosclerotic conditions with 15 years of follow-up. Meanwhile, in patients requiring CABG (mean age: 67 years), preoperative hsCRP had predictive power for mortality with a median follow-up of 89 months. 22 However, these previous reports provided either limited or no information on the predictive value of hsCRP for TVD in elderly patients.
The present study extended the above findings by evaluating this very high-risk population from several aspects. First, we enrolled a large cohort of elderly patients with TVD who received different management strategies in almost equivalent numbers. The data were relatively representative of the characteristics and management strategies in real-world practice at the time of the study, and the large cohort increased the statistical confidence of the results. Second, although hsCRP is a nonspecific biomarker linked with multiple clinical conditions, various adjustments performed in the present study confirmed the constant association between hsCRP and prognosis. Third, ACS presents with more intense inflammation than stable CAD. As noted in previous studies, hsCRP shows distinct fluctuation after an acute ischemic attack. 21 A few studies provided inconclusive results that baseline, peak, or on-treatment hsCRP was associated with cardiac rehabilitation.11,21,23,24 The present data partly supported that the prognostic value of hsCRP pertained to both stable angina and non–ST-elevated ACS subtypes when assessed separately. However, for STEMI, the performance of baseline hsCRP could be inferior. Fourth, in the present study, hsCRP appeared to have additive effects beyond SS II. These findings suggest that hsCRP may have potential as a candidate biomarker to refine this risk scoring system.
The mechanisms underlying the influence of hsCRP in the cardiovascular system remain inconclusive. Accumulating laboratory findings support an etiological role of CRP in atherogenesis, with plaque instability arising through various pathways involving the interplay of CRP with other cytokines and cells, including platelet activation, endothelium inflammation, smooth muscle cell proliferation, microphage polarization, lipid uptake, and lipid deposition.25–28 Nevertheless, in recent years, Mendelian randomization studies failed to prove the causality of CRP for CAD.29,30
Regardless of the debate on whether CRP acts as a mediator or a marker, hsCRP, implying low-grade systemic inflammation, has promising potential for clinical application. The recent Canakinumab Anti-Inflammatory Thrombosis Outcomes Study trial tested the benefit of canakinumab, a monoclonal interleukin-1β antibody, in patients with MI and defined hsCRP as a treatment target for routine monitoring.31,32 The findings indicated that patients aged ≥60 years could benefit from the anti-inflammatory treatment. Nevertheless, more evidence is needed for the application of canakinumab in elderly patients because of a disturbing complication involving fatal infections. 31
In this study, revascularization (PCI or CABG) continued to manifest significant long-term event-free benefits over MT alone in patients with 3-vessel CAD after adjusting for confounding effects. Furthermore, although the patients with CABG and PCI had comparable overall survival rates, CABG provided significant benefits for cardiac death and MACCE over PCI (data not shown). These results conform with previous clinical practice that favored guideline-based aggressive management of TVD and CABG for elderly patients in particular.33–35 Nevertheless, advanced age complicates the management of patients through concerns regarding multimorbid illnesses, complications, and frailty. These factors usually lead to selecting conservative treatment. Notably, in this cohort study, patients with ≥3 comorbidities had a 42% increased mortality risk relative to nonmultimorbid counterparts (HR 1.422, 95% CI, 1.052-1.922, P = .022), irrespective of treatment choice. Similar with prior research, it calls for more emphasis concerning that multimorbidity challenged the postdischarge health care and life expectancy.36,37 The present study revealed a nonsignificant trend toward a correlation between hsCRP and mortality in the CABG arm. The most likely explanation may be an overall improvement in myocardial perfusion with complete revascularization. 38 This could, to some extent, offset the impact of inflammation in long-term severe and diffuse lesions.
This study has several limitations. First, the observational nature of the study leaves an inherent concern regarding selection bias and confounding. In particular, frailty and cognitive function are characteristic influencers in elderly patients, but neither of these factors was recorded. Second, the study did not describe the completeness of the revascularization treatments. This may be important because a previous study concluded that CABG conferred reduced mortality rates relative to incomplete revascularization of PCI. 39 Untreated stenosis or occlusion of the coronary artery may be a factor in patients with chronic inflammatory status, providing a reason why hsCRP could predict long-term outcomes, especially in the MT and PCI subgroups. Third, because lipid-lowering therapy exerts an anti-inflammatory effect, 40 a reduction in hsCRP after discharge (residual inflammatory risk) may have confounded the results.
Conclusions
The presence of hsCRP > 3 mg/L on admission appeared to be independently predictive of worse outcomes in elderly patients with TVD in the long-term and hsCRP could improve the discrimination and reclassification of SS II for risk stratification.
Supplemental Material
Supplemental Material, sj-docx-1-ang-10.1177_00033197211021195 - Relationship Between High-Sensitivity C-Reactive Protein and Long-Term Outcomes in Elderly Patients With 3-Vessel Disease
Supplemental Material, sj-docx-1-ang-10.1177_00033197211021195 for Relationship Between High-Sensitivity C-Reactive Protein and Long-Term Outcomes in Elderly Patients With 3-Vessel Disease by Yue Liu, Ce Zhang, Lin Jiang, Lianjun Xu, Jian Tian, Xueyan Zhao, Xinxing Feng, Dong Wang, Yin Zhang, Kai Sun, Jingjing Xu, Ru Liu, Bo Xu, Wei Zhao, Rutai Hui, Runlin Gao, Zhan Gao, Lei Song and Jinqing Yuan in Angiology
Footnotes
Authors’ Note
LS, JY, RH, and RG contributed to the conception or design of the work. LJ, LX, JT, XZ, XF, DW, YZ, KS, JX, RL, BX, WZ, and ZG contributed to the data acquisition, analysis, or interpretation of data of the work. YL, CZ, and LJ drafted the manuscript. LS and JY critically revised the manuscript. All authors have reviewed and agreed with the content of the article for publication.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CAMS Innovation Fund for Medical Sciences (CAMS-I2M, 2016-I2M-1-002), the National Science and Technology Support Program of China (no. 2016YFC1301301), and the National Natural Science Foundation of China (81770365).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.