
Abstract
Data regarding angiographic characteristics, clinical profile, and inhospital outcomes of patients with coronavirus disease 2019 (COVID-19) referred for coronary angiography (CAG) are scarce. This is an observational study analyzing confirmed patients with COVID-19 referred for CAG from 10 European centers. We included 57 patients (mean age: 66 ± 15 years, 82% male) , of whom 18% had previous myocardial infarction (MI) and 29% had renal insufficiency and chronic pulmonary disease. ST-segment elevation myocardial infarction (STEMI) was the most frequent indication for CAG (58%). Coronavirus disease 2019 was confirmed after CAG in 86% and classified as mild in 49%, with 21% fully asymptomatic. A culprit lesion was identified in 79% and high thrombus burden in 42%; 7% had stent thrombosis. At 40 days follow-up, 16 (28%) patients experienced a major adverse cardiovascular event (MACE): 12 deaths (92% noncardiac), 1 MI, 2 stent thrombosis, and 1 stroke. In an European multicenter registry, patients with confirmed COVID-19 infection referred for CAG during the first wave of the severe acute respiratory syndrome coronavirus 2 pandemic presented mostly with STEMI and were predominantly males with comorbidities. Severity of COVID-19 was in general noncritical and 21% were asymptomatic at the time of CAG. Culprit coronary lesions with high thrombus burden were frequently identified, with a rate of stent thrombosis of 7%. The incidence of MACE at 40 days was high (28%), mostly due to noncardiac death.
Keywords
Introduction
The pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) has led to the onset of a new disease denominated coronavirus disease 2019 (COVID-19). Although in the majority of patients, COVID-19 manifests as a mild upper respiratory tract infection, a significant proportion of patients may present with severe forms of the disease, characterized by a systemic inflammation, cytokine storm, and hypercoagulability. Cardiac injury is frequent in critically ill patients with COVID-19, especially in those with pre-existent cardiovascular conditions and has been associated with a worse prognosis.1–3 Several pathophysiological mechanisms leading to myocardial damage in patients with COVID-19 have been described. Ischemic cardiac injury can result from type I myocardial infarction (MI) derived from a prothrombotic state or type 2 MI as a result of an imbalance of oxygen supply/demand in patients with respiratory distress or severe hypoxemia, shock, or coronary artery dissection. 4 Nonischemic cardiac injury may result as well from myocarditis, 5 stress-cardiomyopathy, 6 acute heart failure, pulmonary embolism, sepsis, or direct viral myocardial injury. In addition, patients with suspected or confirmed COVID-19 may present with an acute coronary syndrome (ACS) as the first clinical manifestation of the disease, even in the absence of respiratory symptoms. The role of invasive coronary angiography (CAG) may be thus crucial in defining the underlying mechanism and establishing the subsequent treatment in patients with COVID-19 presenting with cardiac injury. The potentially associated risks for health care workers and the particular institutional logistics during the pandemic led to development of clinical algorithms to identify patients with COVID-19 who would benefit from an invasive strategy. Current recommendations advise restricting invasive CAG to patients with COVID-19 in whom type I MI is suspected. 7 However, lack of understanding of the pathophysiological mechanisms of cardiac injury, especially in early phases of the pandemic, resulted in a heterogeneous COVID-19 population referred for CAG.
We aimed to describe the clinical and angiographic characteristics, related to each particular clinical context, in a cohort of confirmed patients with COVID-19 referred for invasive CAG in 9 different centers in 2 European countries. In addition, we evaluated the occurrence of major adverse cardiac events (MACEs) at 40 days of follow-up.
Methods
Study Population
Patients with confirmed COVID-19 (polymerase chain reaction [PCR] positive) referred for invasive CAG, irrespective of the clinical setting, between February 15, 2020, and April 30, 2020, in 9 hospitals with 24/7 available cardiac catheterization laboratory in 2 European countries (Spain and the Netherlands) conformed the study cohort. We included both patients with COVID-19 confirmed by reverse transcription PCR assays prior to invasive CAG and persons under investigation with subsequently PCR-confirmed COVID-19 diagnosis during hospitalization.
The institutional review board approved this retrospective analysis of clinically acquired data and waived the need for patient written informed consent.
Interventional Procedure Analysis
Coronary angiograms were retrospectively analyzed by an experienced interventional cardiologist at each center. The procedure was performed in a standard fashion according to current recommendations. Safety measures and protection of health care workers during the invasive procedures were applied according to local protocols at each participating center. 8 Vascular access, use of intravascular imaging, and stent type were left at operator’s discretion. Coronary artery flow at baseline and at the end of the procedure was assessed by using the Thrombolysis In Myocardial Infarction (TIMI) frame count method. 9 The presence of coronary thrombus was reported and thrombus burden was graded from 0 to 5 according to the TIMI-thrombus scale. 10 High thrombus burden was defined as a TIMI-thrombus scale grade ≥4. Multivessel disease was defined as the presence of >1 vessel with luminal narrowing ≥50%. The use of thrombus aspiration was left at operator’s discretion. Both TIMI-flow and TIMI-thrombus scales were reassessed after thrombus aspiration. Angiographic no-reflow phenomenon was defined as a TIMI flow <3 without evidence of mechanical obstruction. 11 Angiographic success of the procedure was defined as a final TIMI 3 flow with residual stenosis <20% and no immediate mechanical complications. SYNTAX score calculations were performed by an experienced interventional cardiologist at each site using the predefined SYNTAX score calculation definitions and algorithm. SYNTAX scores were calculated at baseline coronary angiograms before primary percutaneous coronary interventions (PCI), when performed. In patients presenting with ST-segment elevation myocardial infarction (STEMI), time points were defined according to current MI guidelines. 12 Patient delay was specified as the time interval from the onset of symptoms until the emergency service number was dialed. Door-to-balloon times were collected when appropriate, defining “door” time as the time of arrival at the PCI center and balloon time as the first intracoronary balloon inflation or reperfusion obtained by another device.
Data Collection and Follow-Up
Demographic, clinical, and laboratory data during admission were collected by study investigators from electronic medical records. Severity of COVID-19 at admission was graded according to the definitions proposed by the China Centers for Disease Control and Prevention: mild (non-pneumonia and mild pneumonia), severe (dyspnea, respiratory frequency ≥30 breaths per minute, SpO2 ≤93%, PaO2/FiO2 <300, or lung infiltrates >50%), and critical (respiratory failure, septic shock, or multiple organ dysfunction or failure. 13 Data regarding COVID-19 pharmacological therapy during hospitalization were obtained. Outcome data at 30 days were collected from electronic clinical records. The primary end point of the study was the occurrence of MACE at 40 days, defined as a composite of all-cause mortality, nonfatal MI, stent thrombosis, target vessel revascularization, or stroke. All deaths were considered cardiac unless another specific cause was documented. Myocardial infarction was defined according to current guidelines. 14 Target vessel revascularization and stent thrombosis were defined according to the Academic Research Consortium criteria. 15 If cases with stent thrombosis were subsequently complicated by an MI, the event was defined as stent thrombosis.
Statistical Analysis
Continuous variables are presented as either means ± standard deviation or medians with interquartile range as appropriate. Categorical variables were reported as frequencies and percentages. Kaplan-Meier analysis was performed to show the cumulative probability of MACE. Statistical analysis was performed with SPSS Version 23.0 (IBM).
Results
A total of 57 patients with PCR-confirmed COVID-19 referred for invasive CAG during the study period and were included in the registry. Of them, 49 (94%) patients were referred to Spanish centers and 5 (6%) to Dutch centers. Baseline clinical characteristics are depicted in Table 1. The mean age was 66 ± 15 years and 47 (82%) patients were males. Comorbidities were often present: 18% had a previous MI and 29% had renal insufficiency and chronic obstructive pulmonary disease (COPD). ST-segment elevation was the most common electrocardiographic finding (58%). Overall, echocardiography prior to CAG was available in 42 (74%) patients. A reduced left ventricular ejection fraction (LVEF) with regional wall motion abnormalities was often observed (33%). No echocardiographic abnormalities were observed in up to 19% of the cases. Of note, a Takotsubo cardiomyopathy diagnosis was established in one case presenting with left ventricular apical ballooning with normal coronary arteries. Regarding laboratory findings, elevated cardiac injury markers (troponin, creatine kinase) and inflammatory parameters (C-reactive protein; ferritin; interleukin 6) were observed. Additionally, elevated levels of D-dimers and lymphopenia were present. Coronavirus disease 2019-related clinical characteristics are presented in Table 2. Diagnosis of COVID-19 was confirmed after CAG in the majority of cases (86%). Severity of COVID-19 was classified as mild in 28 (49%) patients; severe in 12 (23%), and critical in 16 (28%). Only 12 (21%) patients were did not have typical COVID-19 symptoms at the time of CAG. The most common COVID-19-related symptoms at hospital admission were fever (51%), fatigue (27%), and dyspnea (27%). Of note, in 29 (81%) of 32 patients who presented with STEMI, this one was the first documented clinical manifestation of COVID-19. Three (5%) patients developed distributive shock during hospitalization. Eight (14%) patients were admitted to the intensive care unit with a median stay of 2 (0-5) days. Median length of hospital stay of the entire cohort was 9.5 (4-17) days. The COVID-19 pharmacological treatment was started in 43 (75%) patients, being combinations of several agents used in up to 26 (46%), with a significant heterogeneity of therapeutical regimes as shown in Table 2. Hydroxychloroquine was widely used (61%) as well as lopinavir-ritonavir (30%). Only 2% of patients were treated with remdesivir or tocilizumab. Concomitant antibiotic therapy was prescribed in 17 (30%) patients. Chest radiographic imaging was available in 44 (77%) patients. Bilateral pulmonary infiltration was the most common radiological pattern observed in 21 (38%) patients. Unilateral consolidations were detected in 19 (34%) patients, whereas diffuse ground-glass opacity was described in only 3 (5%) patients.
Baseline Clinical Characteristics.
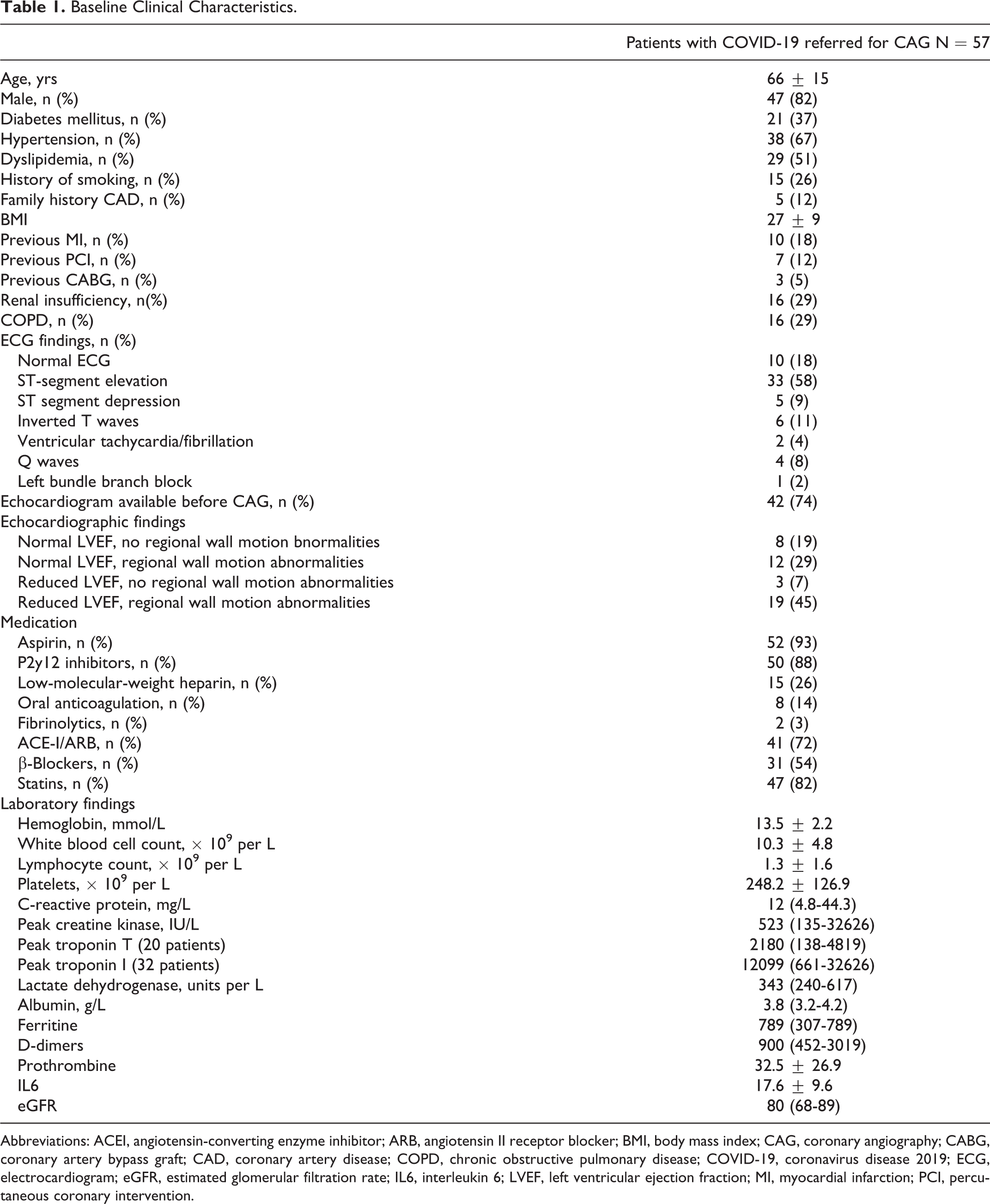
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index; CAG, coronary angiography; CABG, coronary artery bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; ECG, electrocardiogram; eGFR, estimated glomerular filtration rate; IL6, interleukin 6; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Coronavirus Disease 2019-Related Clinical Characteristics.
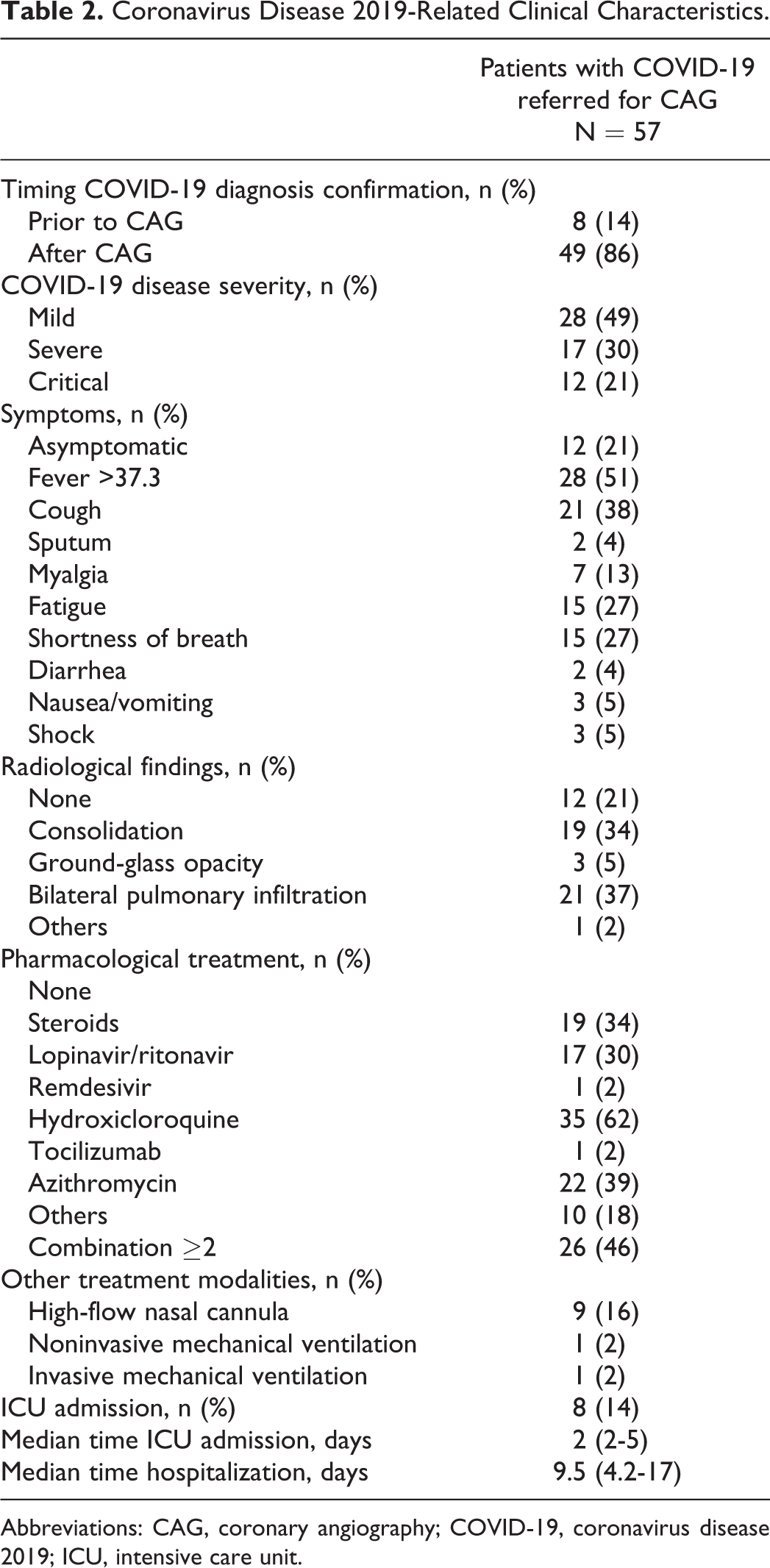
Abbreviations: CAG, coronary angiography; COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Invasive CAG findings and procedural characteristics are presented in Table 3. The indication of CAG was widely established in the context of a suspected ACS, with STEMI being the most frequent indication (58%). A culprit lesion was identified in 45 (79%) patients, including 3 patients with >1 culprit lesion (Figure 1). Of them, 35 (78%) of 45 patients showed obvious angiographic thrombus, with high thrombus burden (defined as TIMI-thrombus scale grade ≥4) present in 19 (42%) of 45 patients. Importantly, in 3 (7%) of 45 patients, a stent thrombosis was identified as the culprit lesion. Thrombus aspiration was performed in 11 (24%) of 45 patients, being used in the majority of cases (7/11) as the initial strategy. All patients treated with thrombus aspiration showed high thrombus burden. Thrombus aspiration resulted in an improvement of 2.2 ± 1.6 TIMI-thrombus scale grades and 2.2 ± 1.6 TIMI-flow scale grades. Multivessel coronary disease was observed in 26 (46%) patients. Median SYNTAX score before and after revascularization was 13 (9-24) and 5 (0-17), respectively, reflecting the presence of low complexity coronary artery disease. Two major procedural complications were documented: a femoral bleeding requiring surgical repair and a coronary perforation treated with prolonged balloon inflation.
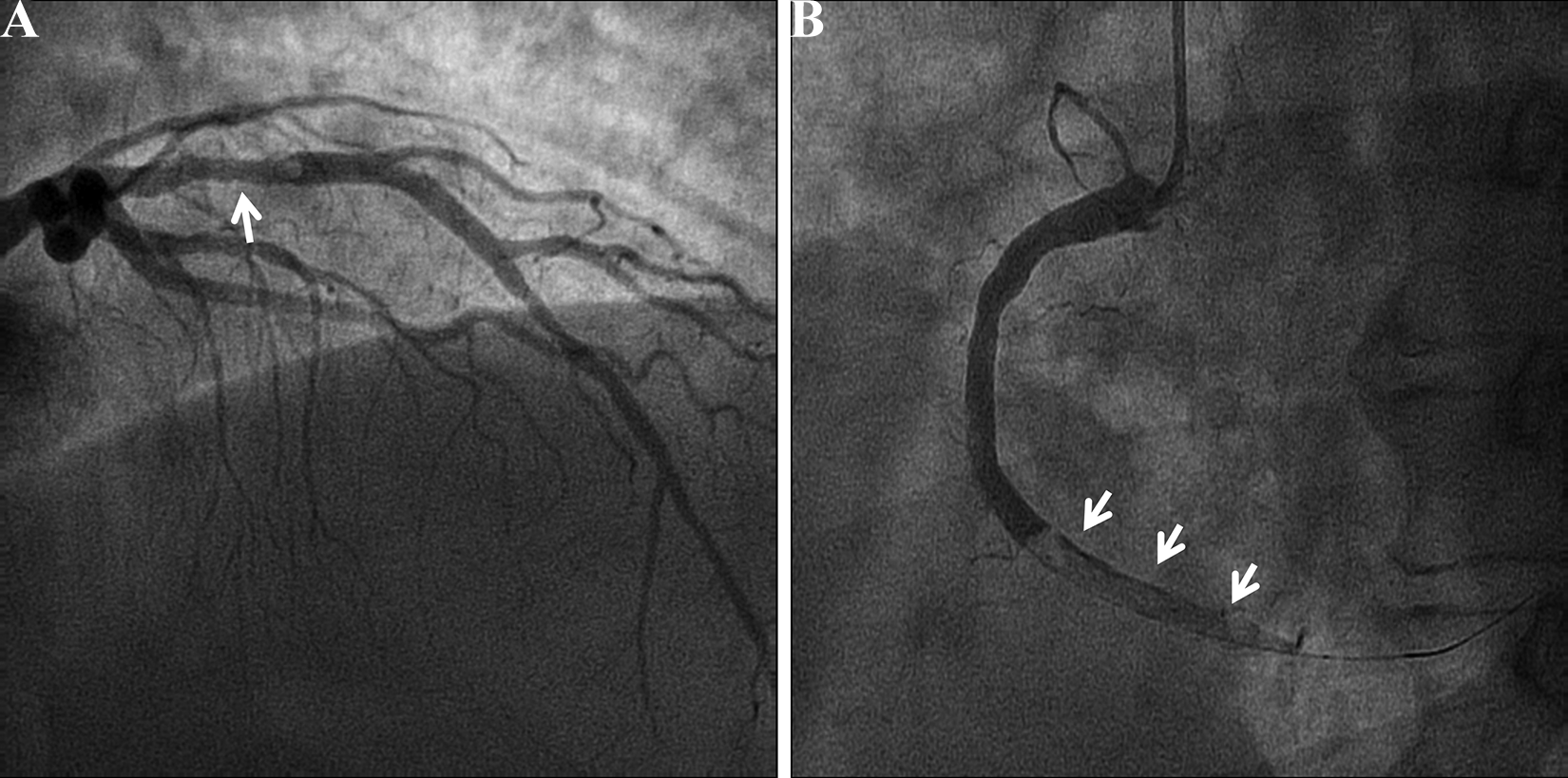
Example of patient with COVID-19 presenting with ST-elevation myocardial infarction, in whom 2 culprit lesions with high thrombus burden were identified on coronary angiography, located at the proximal left anterior descending artery (panel A, arrow) and distal right coronary artery (panel B, arrows). COVID-19 indicates coronavirus disease 2019.
Procedural and Angiographic Characteristics.
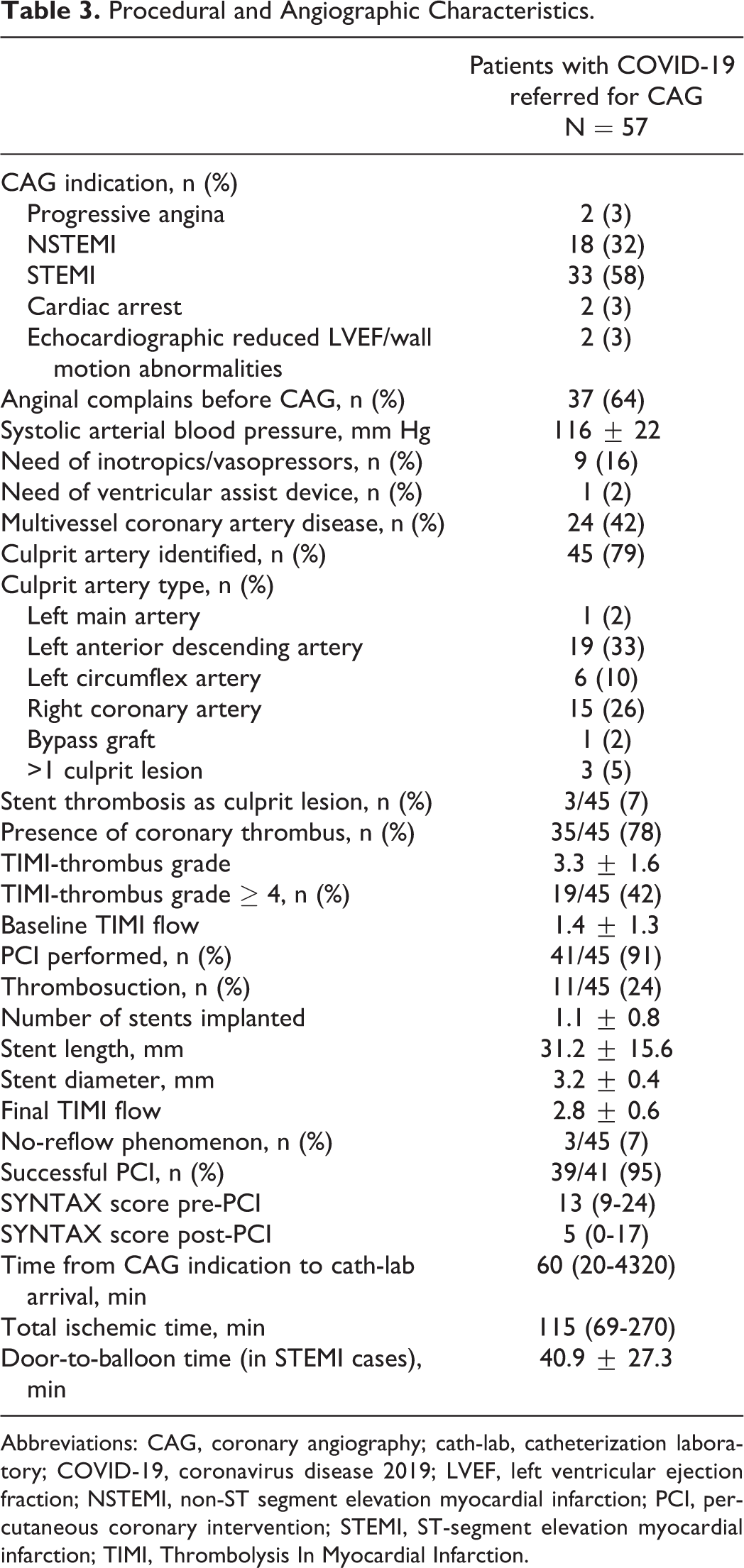
Abbreviations: CAG, coronary angiography; cath-lab, catheterization laboratory; COVID-19, coronavirus disease 2019; LVEF, left ventricular ejection fraction; NSTEMI, non-ST segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; TIMI, Thrombolysis In Myocardial Infarction.
After a follow-up of 40 days, 16 (28%) patients experienced an MACE (Table 4). A total of 12 patients died, predominantly due to noncardiac causes (11 patients, 92%), all of them during hospitalization; 1 patient suffered a non-fatal MI, treated conservatively; 2 presented stent thrombosis (1 intraprocedural in a stent implanted in the left anterior descending artery; 1 in the proximal left circumflex 30 minutes after PCI requiring percutaneous treatment) with subsequent MI. Finally, 1 patient experienced a stroke (Figure 2).
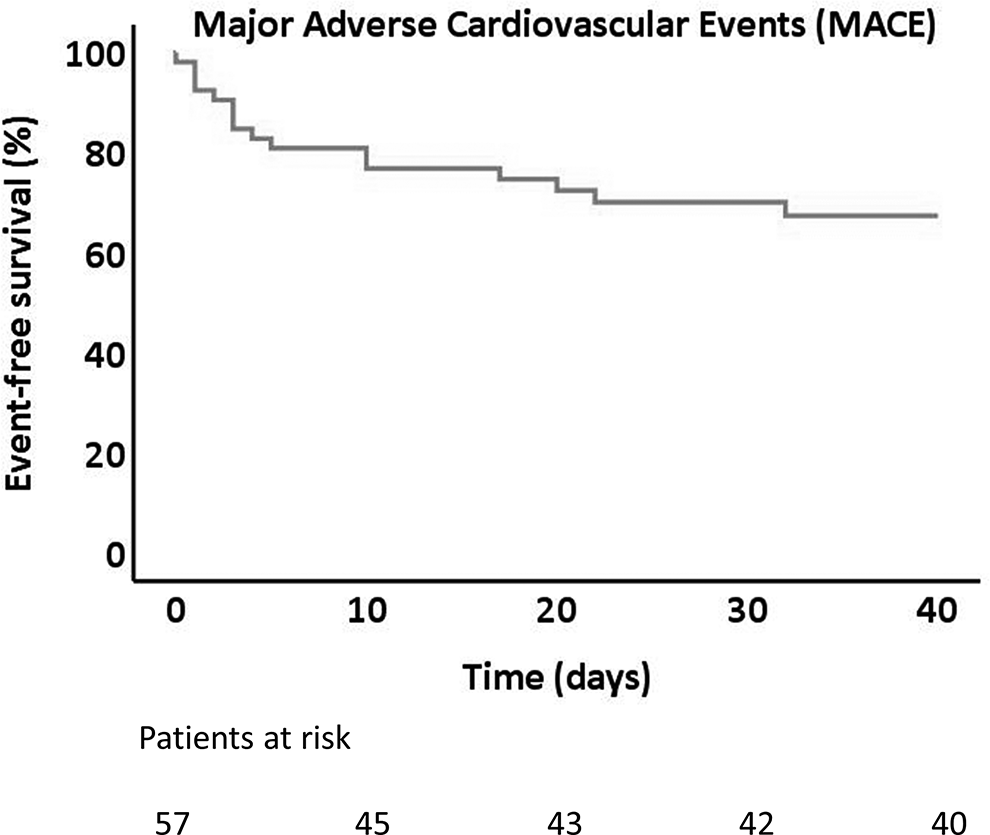
Kaplan-Meier cumulative incidence of MACE of patients with COVID-19 from invasive coronary angiography performance.
Clinical Outcomes.
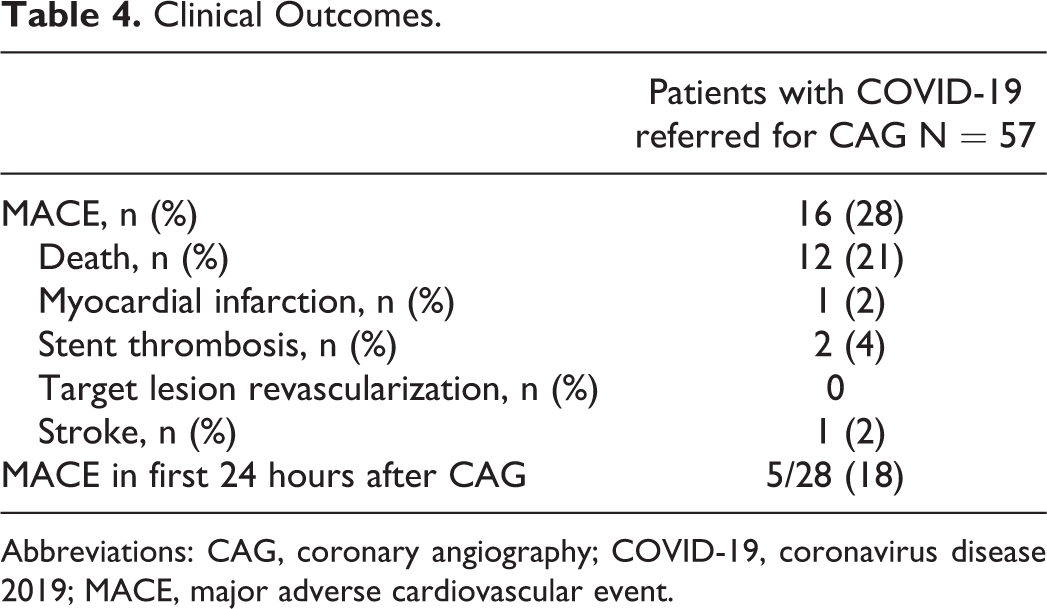
Abbreviations: CAG, coronary angiography; COVID-19, coronavirus disease 2019; MACE, major adverse cardiovascular event.
Discussion
The main findings of the present descriptive study are: (1) the most common indication for CAG in patients with COVID-19 during outbreak’s first wave was STEMI, representing 58% of the cases. (2) Patients referred for CAG were predominantly males and had often comorbidities (previous MI 18%, renal insufficiency 29%, COPD 29%). (3) Diagnosis of COVID-19 was confirmed prior to CAG only in 14% of the cases. (4) Severity of COVID-19 was predominantly noncritical, being 21% of patients asymptomatic at the time of CAG. (5) A culprit lesion was identified in the majority of cases (79%; often associated with a high thrombus load), being stent thrombosis detected in 7%; however, the complexity of coronary artery disease assessed by SYNTAX score was low (13 [9-24]). (5) The incidence of MACE at 40 days of follow-up was very high (28%), mostly due to noncardiac death (11 patients, 85%); of note, 3 patients presented with thrombotic events (2 stent thrombosis and 1 stroke).
The decrease of STEMIs worldwide during the COVID-19 pandemic has been extensively reported, showing up to a 42% to 48% reduction in hospitalizations for ACS and a 38% to 40% reduction in primary PCI for STEMI in areas with high COVID-19 prevalence.16,17 Nevertheless, STEMI remained the main indication for invasive CAG in our study. Despite the observed heterogenicity of CAG indication, CAG was ultimately indicated due to a suspected acute coronary event in the majority of patients regardless of the clinical presentation. However, in 21% of patients no evident culprit coronary lesion was observed. Interestingly, 17% of patients referred for CAG because of STEMI did not show an evident culprit lesion. In those patients presenting with an indication other than STEMI, no culprit lesion was identified in 27%. In a study comprising 28 patients having COVID-19 with STEMI referred for CAG, Stefanini et al reported the absence of a culprit coronary lesion in 39.3%. 18 This illustrates the particular challenges of ACS diagnosis in patients with COVID-19. As observed in our study, elevated cardiac biomarkers and electrocardiographic changes suggesting ischemia and/or echocardiographic abnormalities (reduced LVEF and/or regional wall motion abnormalities) are often present and may not necessarily be linked to a coronary event. Elevated cardiac troponins are frequently detected in patients with COVID-19, often secondary to a broad spectrum of noncoronary etiologies, such as nonspecific myocardial injury, myocarditis, pulmonary embolism, 19 or Takotsubo syndrome (which was found in 1 patient of our cohort). 6 Myocardial injury is more frequent in critically ill patients with COVID-19, especially in those with previous comorbidities, and is independently associated with a high mortality.1,2 Indeed, comorbidities were frequently present in our study cohort (previous MI 18%, renal insufficiency 29%, COPD 29%). However, almost 50% showed mild COVID-19 severity. It has been shown that ACS in patients with COVID-19 may occur in the absence of a severe systemic inflammation status. STEMI has been previously reported as the first clinical manifestation of COVID-19.18,20
Importantly, up to 21% of patients of the study cohort were completely asymptomatic for COVID-19 at the time of CAG. Furthermore, only 14% of the patients had a confirmed COVID-19 diagnosis before being referred to the catheterization laboratory. This highlights the need of establishing strategies to effectively identify patients who may benefit from an invasive approach and avoid unnecessary procedures with subsequent risk of contagion among catheterization laboratory personnel.
Coronavirus 2019 is linked to a multifactorial prothrombotic state, resulting from the hyperinflammatory state, endothelial dysfunction, and hemostatic abnormalities. 21 A high rate of both venous and arterial thrombotic events has been described.22,23 Similarly to other viral infections, COVID-19 may trigger an ACS by different mechanisms, such as plaque rupture, coronary spasm, or microthrombi. 3 Direct viral endothelial injury may trigger as well thrombus formation and subsequently ACS. 24 This prothrombotic state is translated angiographically in a high thrombus burden (42% TIMI thrombus grade ≥4), stent thrombosis as culprit lesion (7%), and even involvement of several coronary vessels (5%, Figure 1), typically associated with a low complex underlying coronary artery disease phenotype (SYNTAX pre-PCI 13 [9-24]). Similarly, Choudry et al reported a high rate of intracoronary thrombus burden (grade 4-5, 84%), multivessel thrombosis (17.9%), and stent thrombosis (10%) in a cohort of 39 patients with COVID-19 presenting exclusively with STEMI. 23
Finally, it is important to elucidate the high incidence of MACE at 40 days of follow-up (28%, Figure 2) in spite of having performed a successful PCI in 95% of patients without significant delays. The most frequent adverse event was noncardiac death (11 patients, 85%), mostly due to respiratory and systemic involvement. Of note, 3 patients presented thrombotic events: 2 stent thrombosis (4.8%), a higher stent thrombosis rate than recent reports (reference), and 1 stroke (1.7%).
Limitations
The main limitations of this study are its observational and retrospective design and its small sample size. Lack of control group of non-COVID-19 individuals prevents drawing definitive conclusions from this study, and therefore the observed results cannot be generalized. However, the present study presents information regarding angiographic and clinical features of patients with COVID-19 referred for CAG irrespective of the indication, which provides a useful overview of the potential value of an invasive approach in this clinical scenario.
Conclusion
In a European multicenter registry, patients with confirmed COVID-19 infection referred for CAG during the first wave of the SARS-CoV2 pandemic presented mostly with STEMI and were predominantly male, often with comorbidities. Severity of COVID-19 was in general noncritical, with 21% of asymptomatic patients at the time of CAG. Culprit coronary lesions with high thrombus burden were frequently identified, with a rate of stent thrombosis of 7%. The incidence of MACE at 40 days of follow-up was high (28%), mostly due to noncardiac death.
Footnotes
Authors’ Note
The content of this article has not been presented orally at a professional meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.